Thyroid Pathology in End-Stage Renal Disease Patients on Hemodialysis

 , ,
, ,  , and
, and 
Abstract
:1. Introduction
2. Material and Methods
Statistical Analysis
3. Results
4. Discussions
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ESRD | end-stage renal disease |
| RRT | renal replacement therapy |
| CKD | chronic kidney disease |
| TSH | thyroid-stimulating hormone |
| FT3 | free triiodothyronine |
| FT4 | free thyroxin |
| US | ultrasonography |
| CKD-MBD | chronic kidney disease mineral bone disorder |
| GFR | glomerular filtration rate |
| RPF | renal plasma flow |
| TG Ab | thyroglobulin antibodies |
| TPO Ab | thyroperoxidase antibodies |
References
- Rhee, C.M.; You, A.S.; Nguyen, D.V.; Brunelli, S.M.; Budoff, M.J.; Streja, E.; Nakata, T.; Kovesdy, C.P.; Brent, G.A.; Kalantar-Zadeh, K. Thyroid status and mortality in a prospective hemodialysis cohort. J. Clin. Endocrinol. Metab. 2017, 102, 1568–1577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korosi, A. Practice guidelines for chronic kidney disease. Ann. Intern. Med. 2004, 140, 934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wheeler, D.; Winkelmayer, W.C. Kidney Disease: Improving Global Outcomes. KDIGO clinical practice guidelines for the prevention, diagnosis, evaluation, and treatment of Hepatitis C in chronic kidney disease. Kidney Int. 2008, 73, S1–S99. [Google Scholar]
- Ketteler, M.; Block, G.A.; Evenepoel, P.; Fukagawa, M.; Herzog, C.A.; McCann, L.; Moe, S.M.; Shroff, R.; Tonelli, M.A.; Toussaint, N.D.; et al. Executive summary of the 2017 KDIGO Chronic Kidney Disease–Mineral and Bone Disorder (CKD-MBD) Guideline Update: What’s changed and why it matters. Kidney Int. 2017, 92, 26–36. [Google Scholar] [CrossRef] [Green Version]
- Fleming, G.M. Renal replacement therapy review: Past, present and future. Organogenesis 2011, 7, 2–12. [Google Scholar] [CrossRef]
- Cotoi, L.; Stoian, D.; Borlea, A.; Varcus, F. Ultrasonographic and elastographic diagnostic of parathyroid lesions–a literature review. Austin J. Endocrinol. Diab 2019, 6, 1–9. [Google Scholar]
- Kaptein, E.M.; Quion-Verde, H.; Chooljian, C.J.; Tang, W.W.; Friedman, P.E.; Rodriquez, H.J.; Massry, S.G. The thyroid in end-stage renal disease. Medicine (United States) 1988, 67, 187–197. [Google Scholar] [CrossRef] [PubMed]
- Kaptein, E.M. Thyroid hormone metabolism and thyroid diseases in chronic renal failure. Endocr Rev. 1996, 17, 45–63. [Google Scholar] [CrossRef]
- Rhee, C.M.; Alexander, E.K.; Bhan, I.; Brunelli, S.M. Hypothyroidism and mortality among dialysis patients. Clin. J. Am. Soc. Nephrol. 2013, 8, 593–601. [Google Scholar] [CrossRef] [Green Version]
- Rhee, C.M.; Kim, S.; Gillen, D.L.; Oztan, T.; Wang, J.; Mehrotra, R.; Kuttykrishnan, S.; Nguyen, D.V.; Brunelli, S.M.; Kovesdy, C.P.; et al. Association of thyroid functional disease with mortality in a national cohort of incident hemodialysis patients. J. Clin. Endocrinol. Metab. 2015, 100, 1386–1395. [Google Scholar] [CrossRef] [Green Version]
- Rhee, C.M.; Chen, Y.; You, A.S.; Brunelli, S.M.; Kovesdy, C.P.; Budoff, M.J.; Brent, G.A.; Kalantar-Zadeh, K.; Nguyen, D.V. Thyroid status, quality of life, and mental health in patients on hemodialysis. Clin. J. Am. Soc. Nephrol. 2017, 12, 1274–1283. [Google Scholar] [CrossRef] [Green Version]
- Iglesias, P.; Díez, J.J. Thyroid dysfunction and kidney disease. Eur. J. Endocrinol. 2009, 160, 503–515. [Google Scholar] [CrossRef]
- Kar, P.M.; Hirani, A.; Allen, M.J. Acute renal failure in a hypothyroid patient with rhabdomyolysis. Clin. Nephrol. 2003, 60, 428–429. [Google Scholar] [CrossRef] [PubMed]
- Sekine, N.; Yamamoto, M.; Hayashi, M.; Michikawa, M.; Enomoto, T.; Ozawa, E.; Kobayashi, T. Rhabdomyolysis and acute renal failure in a patient with hypothyroidism. Intern. Med. 1993, 32, 269–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, P.A.; Bobby, Z.; Selvaraj, N.; Vinayagamoorthi, R. An evaluation of thyroid hormone status and oxidative stress in undialyzed chronic renal failure patients. Indian J. Physiol. Pharmacol. 2006, 50, 279. [Google Scholar] [PubMed]
- Kutlay, S.; Atli, T.; Koseogullari, O.; Nergizoglu, G.; Duman, N.; Gullu, S. Thyroid disorders in hemodialysis patients in an iodine-deficient community. Artif. Organs. 2005, 29, 329–332. [Google Scholar] [CrossRef] [PubMed]
- Miki, H.; Oshimo, K.; Inoue, H.; Kawano, M.; Tanaka, K.; Komaki, K.; Uyama, T.; Kawauchi, M.; Minakuchi, J.; Monden, Y. Thyroid nodules in female uremic patients on maintenance hemodialysis. J. Surg. Oncol. 1993, 54, 216–218. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, G.; Bittle, P.; Sanders, H.; Bercu, B. Hypothalamo-Hypophyseal Function before and after Dialysis Patients. J. Clin. Endocrinol. Metab. 1992, 74, 517–524. [Google Scholar]
- Farag, S.E.S. Functional and Morphological Thyroid Disorders in Hemodialysis Patients. J. Thyroid Disord Ther. 2013, 2, 2–5. [Google Scholar] [CrossRef] [Green Version]
- Wiederkehr, M.R.; Kalogiros, J.; Krapf, R. Correction of metabolic acidosis improves thyroid and growth hormone axes in haemodialysis patients. Nephrol. Dial. Transplant. 2004, 19, 1190–1197. [Google Scholar] [CrossRef] [Green Version]
- Mohamedali, M.; Reddy Maddika, S.; Vyas, A.; Iyer, V.; Cheriyath, P. Thyroid disorders and chronic kidney disease. Int. J. Nephrol. 2014, 2014, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, V.S.; Fang, V.S.; Katz, A.I.; Refetoff, S. Thyroid dysfunction in chronic renal failure. A study of the pituitary thyroid axis and peripheral turnover kinetics of thyroxine and triiodothyronine. J. Clin. Invest. 1977, 60, 522–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hardy, M.J.; Ragbeer, S.S.; Nascimento, L. Pituitary-thyroid function in chronic renal failure assessed by a highly sensitive thyrotropin assay. J. Clin. Endocrinol. Metab. 1988, 66, 233–236. [Google Scholar] [CrossRef] [PubMed]
- Åsvold, B.O.; Vatten, L.J.; Bjøro, T. Changes in the prevalence of hypothyroidism: The HUNT study in Norway. Eur. J. Endocrinol. 2013, 169, 613–620. [Google Scholar] [CrossRef] [PubMed]
- McGrogan, A.; Seaman, H.E.; Wright, J.W.; De Vries, C.S. The incidence of autoimmune thyroid disease: A systematic review of the literature. Clin. Endocrinol. 2008, 69, 687–696. [Google Scholar] [CrossRef] [PubMed]
- Stoian, D.; Ivan, V.; Sporea, I.; Florian, V.; Mozos, I.; Navolan, D.; Nemescu, D. Advanced ultrasound application – Impact on presurgical risk stratification of the thyroid nodules. Ther. Clin. Risk Manag. 2020, 16, 21–30. [Google Scholar] [CrossRef] [Green Version]
- Canaris, G.J.; Manowitz, N.R.; Mayor, G.; Ridgway, E.C. The colorado thyroid disease prevalence study. Arch. Intern. Med. 2000, 160, 526–534. [Google Scholar] [CrossRef] [Green Version]
- Taylor, P.N.; Albrecht, D.; Scholz, A.; Gutierrez-Buey, G.; Lazarus, J.H.; Dayan, C.M.; Okosieme, O.E. Global epidemiology of hyperthyroidism and hypothyroidism. Nat. Rev. Endocrinol. 2018, 14, 301–316. [Google Scholar] [CrossRef]
- Lo, J.C.; Chertow, G.M.; Go, A.S.; Hsu, C.Y. Increased prevalence of subclinical and clinical hypothyroidism in persons with chronic kidney disease. Kidney Int. 2005, 67, 1047–1052. [Google Scholar] [CrossRef] [Green Version]
- Da Costa, A.B.B.A.; Pellizzari, C.; Carvalho, G.A.; Sant’Anna, B.C.; Montenegro, R.L.; Zammar Filho, R.G.; Mesa Junior, C.O.; Hauck Prante, P.R.; Olandoski, M.; Carvalho, M. High prevalence of subclinical hypothyroidism and nodular thyroid disease in patients on hemodialysis. Hemodial. Int. 2016, 20, 31–37. [Google Scholar] [CrossRef]
- Chonchol, M.; Lippi, G.; Salvagno, G.; Zoppini, G.; Muggeo, M.; Targher, G. Prevalence of subclinical hypothyroidism in patients with chronic kidney disease. Clin. J. Am. Soc. Nephrol. 2008, 3, 1296–1300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allawi, A.A. Prevalence Of Hypothyroidism In Chronic Kidney Disease Among Sample Of Iraqi Patients. Clin. J. Am. Soc. Nephrol. 2013, 3, 1296–1300. [Google Scholar]
- Pakfetrat, M.; Dabbaghmanesh, M.H.; Karimi, Z.; Rasekhi, A.; Malekmakan, L.; Hossein Nikoo, M. Prevalence of hypothyroidism and thyroid nodule in chronic hemodialysis Iranian patients. Hemodial Int. 2017, 21, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, G.; O’Neill, W.; Jubiz, W.; Bloomer, H.A. Thyroid dysfunction in uremia: Evidence for thyroid and hypophyseal abnormalities. Ann. Intern. Med. 1976, 84, 672–676. [Google Scholar] [CrossRef]
- Gharib, H.; Papini, E.; Paschke, R.; Duick, D.S.; Valcavi, R.; Hegedus, L.; Vitti, P. American Association of Clinical Endocrinologists, Associazione Medici Endocrinologi, and European Thyroid Association medical guidelines for clinical practice for the diagnosis and management of thyroid nodules. J. Endocrinol. Invest. 2010, 33, 1–50. [Google Scholar] [CrossRef]
- Stoian, D.; Bogdan, T.; Craina, M.; Craciunescu, M.; Timar, R.; Schiller, A. Elastography: A New Ultrasound Technique in Nodular Thyroid Pathology. Thyroid Cancer Adv. Diagnosis Ther. 2016. [Google Scholar] [CrossRef] [Green Version]
- Demirer, A.N.; Kemal, Y.; Gursoy, A.; Sahin, M.; Tutuncu, N.B. Clinicopathological characteristics of thyroid cancer in patients on dialysis for end-stage renal disease. Thyroid 2008, 18, 45–50. [Google Scholar] [CrossRef]
- Karamchandani, D.; Arias-Amaya, R.; Donaldson, N.; Gilbert, J.; Schulte, K.M. Thyroid cancer and renal transplantation: A meta-analysis. Endocr. Relat. Cancer 2010, 17, 159. [Google Scholar] [CrossRef] [Green Version]
- Stoian, D.; Borcan, F.; Petre, I.; Mozos, I.; Varcus, F.; Ivan, V.; Cioca, A.; Apostol, A.; Dehelean, C.A. Strain elastography as a valuable diagnosis tool in intermediate cytology (Bethesda III) thyroid nodules. Diagnostics 2019, 9, 119. [Google Scholar] [CrossRef] [Green Version]
- Shabana, W.; Peeters, E.; De Maeseneer, M. Measuring Thyroid Gland Volume: Should We Change the Correction Factor? Am. J. Roentgenol. 2006, 186, 234–236. [Google Scholar] [CrossRef]
- Cotoi, L.; Borcan, F.; Sporea, I.; Amzar, D.; Schiller, O.; Schiller, A.; Dehelean, C.A.; Pop, G.H.; Stoian, D. Shear wave elastography in diagnosing secondary hyperparathyroidism. Diagnostics 2019, 9, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Abdelwhab, S.; Foda, O. Relation Between Thyroid Hormones and Insulin Resistance in Hemodialysis Patients. Kidney 2010, 19, 66–72. [Google Scholar] [CrossRef]
- Amato, A.A.; Santos, G.M.; De Assis Rocha Neves, F. Thyroid hormone action in chronic kidney disease. Curr. Opin. Endocrinol. Diabetes Obes. 2008, 15, 459–465. [Google Scholar] [CrossRef] [PubMed]
- Schiller, A.; Timar, R.; Siriopol, D.; Timar, B.; Bob, F.; Schiller, O.; Drug, V.; Mihaescu, A.; Covic, A. Hepatitis B and C Virus Infection in the Hemodialysis Population from Three Romanian Regions. Nephron 2015, 129, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Elzakil, M.; Gareeballah, A.; Gameraddin, M.; Burai, M.; Alagab, F. Sonographic assessment of thyroid gland in patients with chronic kidney disease undergoing hemodialysis. Int. J. Diagnostic Imaging 2017, 5, 4. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, I.A.; Ramadan, Y.K.; Hassan, E.A.; Eissa, A.H. Abnormalities in Thyroid Function and Morphology in Chronic Hemodialysis Patients. Med. J. Cairo Univ. 2016, 84, 143–148. [Google Scholar]
- Lo, J.C.; Beck, G.J.; Kaysen, G.A.; Chan, C.T.; Kliger, A.S.; Rocco, M.V.; Li, M.; Chertow, G.M. Thyroid function in end stage renal disease and effects of frequent hemodialysis. Hemodial. Int. 2017, 21, 534–541. [Google Scholar] [CrossRef]
- Rhee, C.M.; Ravel, V.A.; Streja, E.; Mehrotra, R.; Kim, S.; Wang, J.; Nguyen, D.V.; Kovesdy, C.P.; Brent, G.A.; Kalantar-Zadeh, K. Thyroid functional disease and mortality in a national peritoneal dialysis cohort. J. Clin. Endocrinol. Metab. 2016, 101, 4054–4061. [Google Scholar] [CrossRef]
- Cuna, V.; Menghi, V.; Comai, G.; Cappuccilli, M.; Cianciolo, G.; Raimondi, C.; Grammatico, F.; Donati, G.; Baraldi, O.; Capelli, I.; et al. Functional abnormalities and thyroid nodules in patients with end-stage renal disease. In Vivo 2017, 31, 1203–1208. [Google Scholar]
- Cotoi, L.; Amzar, D.; Sporea, I.; Borlea, A.; Navolan, D.; Varcus, F.; Stoian, D. Shear Wave Elastography versus Strain Elastography in Diagnosing Parathyroid Adenomas. Int. J. Endocrinol. 2020, 2020, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Lin, S.Y.; Lin, W.M.; Lin, C.L.; Yang, T.Y.; Sung, F.C.; Wang, Y.H.; Kao, C.H. The relationship between secondary hyperparathyroidism and thyroid cancer in end stage renal disease: A population based cohort study. Eur. J. Intern. Med. 2014, 25, 276–280. [Google Scholar] [CrossRef] [PubMed]
- Cataldo, E.; Columbano, V.; Nielsen, L.; Gendrot, L.; Covella, B.; Piccoli, G.B. Phosphate binders as a cause of hypothyroidism in dialysis patients: Practical indications from a review of the literature. BMC Nephrol. 2018, 19, 1–7. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Study Group |
|---|---|
| Gender (F/M) | 53/70 |
| Age (years) | 62.2 ± 11.01 |
| BMI (kg/m2) | 28.3 ± 5.95 |
| Hemodialysis duration (years) | 5.6 ± 4.89 |
| Parathormone (pg/mL) | 609.4 ± 605.5 |
| Total serum calcium (mg/dL) | 8.6 ± 0.65 |
| Serum creatinine (mg/dL) | 8.9 ± 2.32 |
| Serum urea (mg/dL) | 122.2 ± 29.66 |
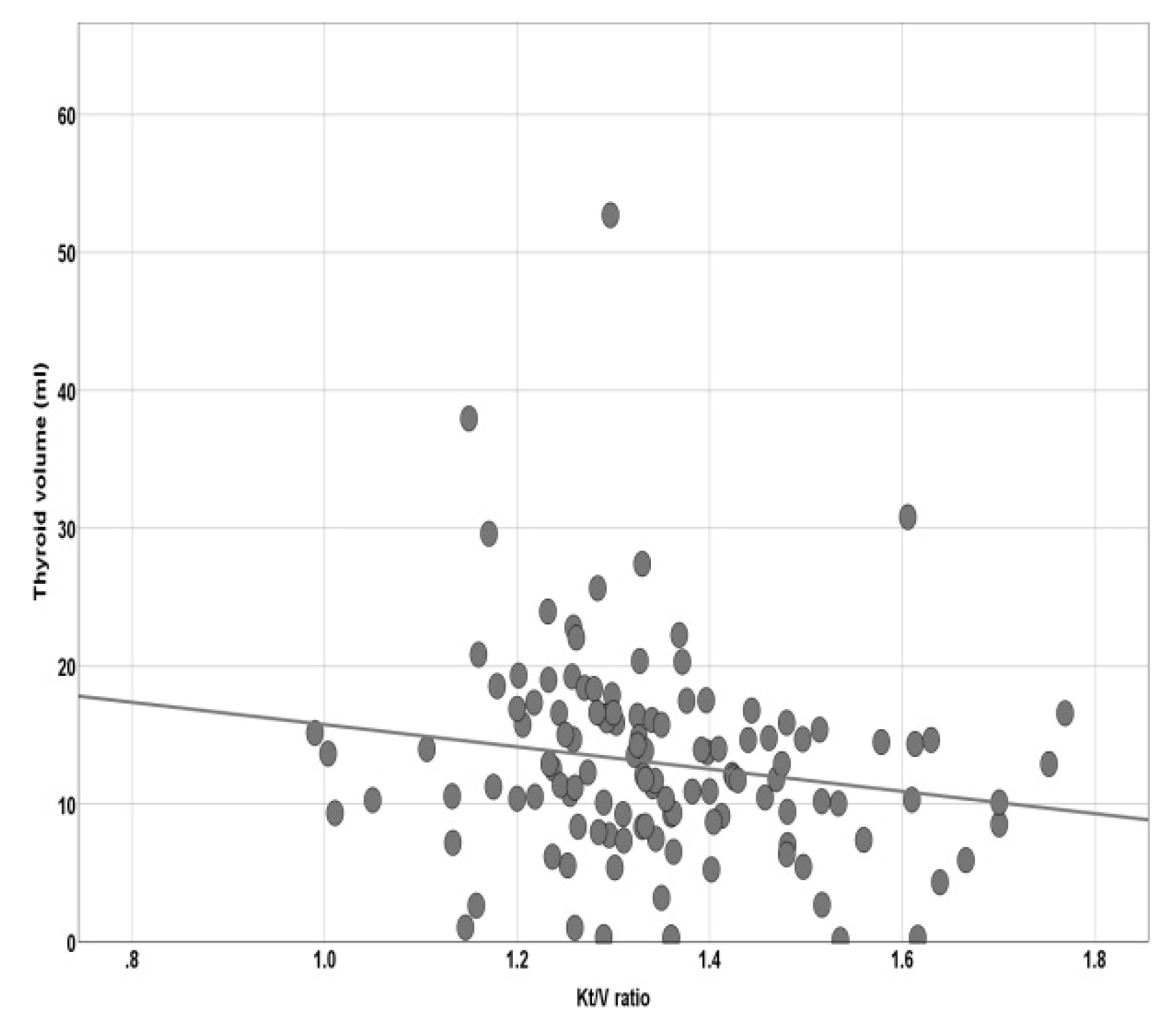
| Kt/v ratio | 1.3 ± 0.153 |
| Glomerular filtration rate (mL/min/1.73 m) | 5.5 ± 1.64 |
| TSH (µU/mL) | 3.36 ± 2.31 |
| FT4 (pmol/L) | 15.52 ± 2.92 |
| FT3 (pmol/L) | 3.2 ± 2.961 |
| TG Ab (IU/mL) | 16.0 ± 70.44 |
| TPO Ab (IU/mL) | 98.6 ± 295.8 |
| Thyroid volume (mL) | 13.3 ± 7.18 |
| Thyroid Disorders | Number of Patients | Percent Occurrence (%) |
|---|---|---|
| Euthyroid | 89 | 72.4 |
| Subclinical Hyperthyroidism | 4 | 3.3 |
| Hypothyroid | 30 | 24.4 |
| Morphology Disorders | Number of Patients | Percent Occurrence (%) |
|---|---|---|
| Without Goiter | 60 | 48.7 |
| Nodular goiter | 63 | 51.2 |
| Autoimmune thyroiditis | 22 | 17.8 |
| Papillary thyroid carcinoma | 3 | 2.4 |
| Variable | B | S.E. | p | OR | 95% OR | |
|---|---|---|---|---|---|---|
| Female gender | 1.276 | 0.416 | 0.002 | 3.581 | 1.585 | 8.092 |
| BMI | 0.90 | 0.038 | 0.015 | 1.083 | 1.005 | 1.168 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cotoi, L.; Borcan, F.; Sporea, I.; Amzar, D.; Schiller, O.; Schiller, A.; Dehelean, C.A.; Pop, G.N.; Borlea, A.; Stoian, D. Thyroid Pathology in End-Stage Renal Disease Patients on Hemodialysis. Diagnostics 2020, 10, 245. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10040245
Cotoi L, Borcan F, Sporea I, Amzar D, Schiller O, Schiller A, Dehelean CA, Pop GN, Borlea A, Stoian D. Thyroid Pathology in End-Stage Renal Disease Patients on Hemodialysis. Diagnostics. 2020; 10(4):245. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10040245
Chicago/Turabian StyleCotoi, Laura, Florin Borcan, Ioan Sporea, Daniela Amzar, Oana Schiller, Adalbert Schiller, Cristina A. Dehelean, Gheorghe Nicusor Pop, Andreea Borlea, and Dana Stoian. 2020. "Thyroid Pathology in End-Stage Renal Disease Patients on Hemodialysis" Diagnostics 10, no. 4: 245. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10040245