Subacute Changes in N-Acetylaspartate (NAA) Following Ischemic Stroke: A Serial MR Spectroscopy Pilot Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Imaging Techniques
2.3. Clinical Assessments
2.4. Data Analysis
3. Results
3.1. Patient Characteristics
3.2. Temporal Evolution of NAA and Other Metabolites
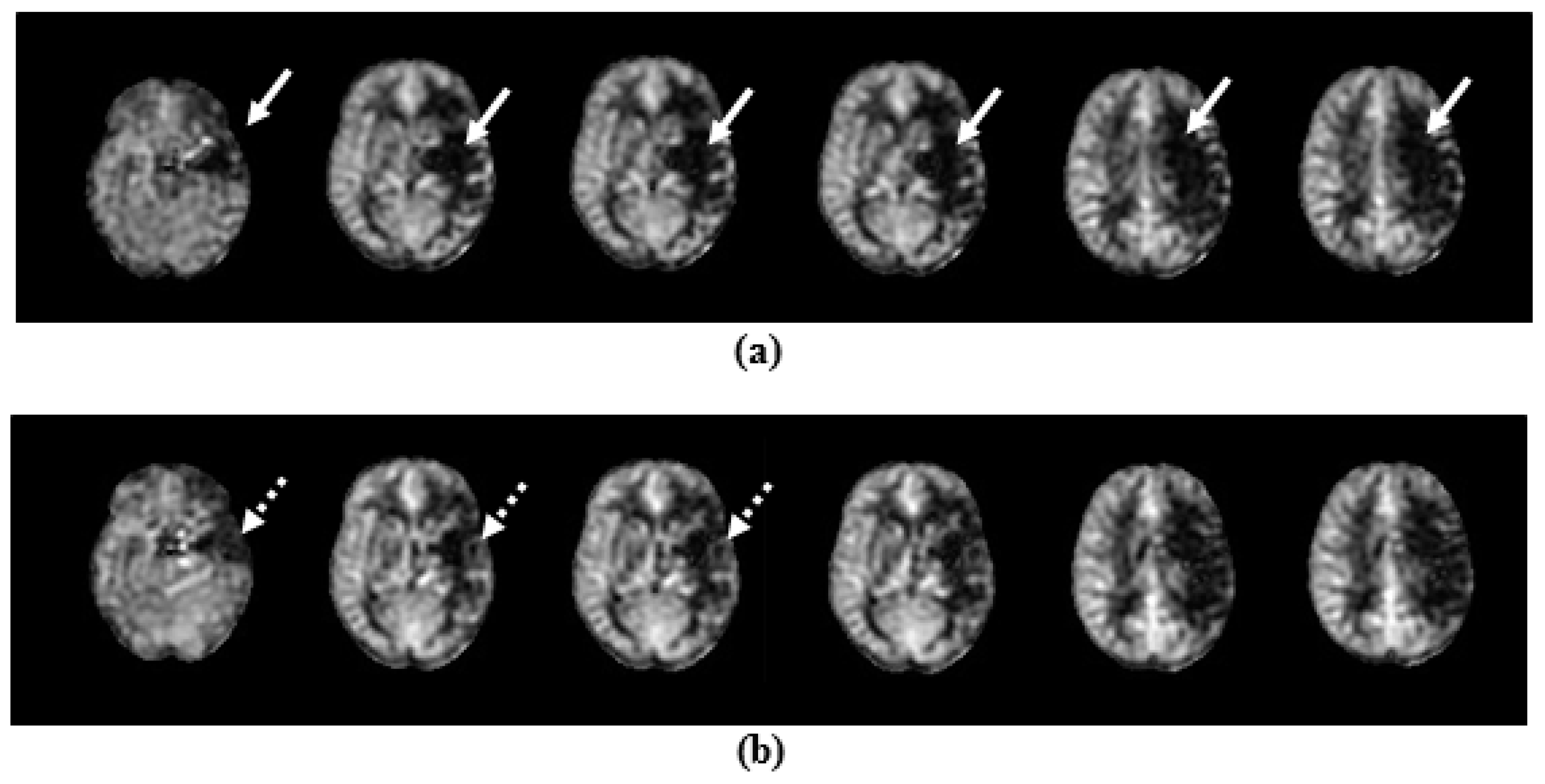
3.3. Temporal Evolution of CBF
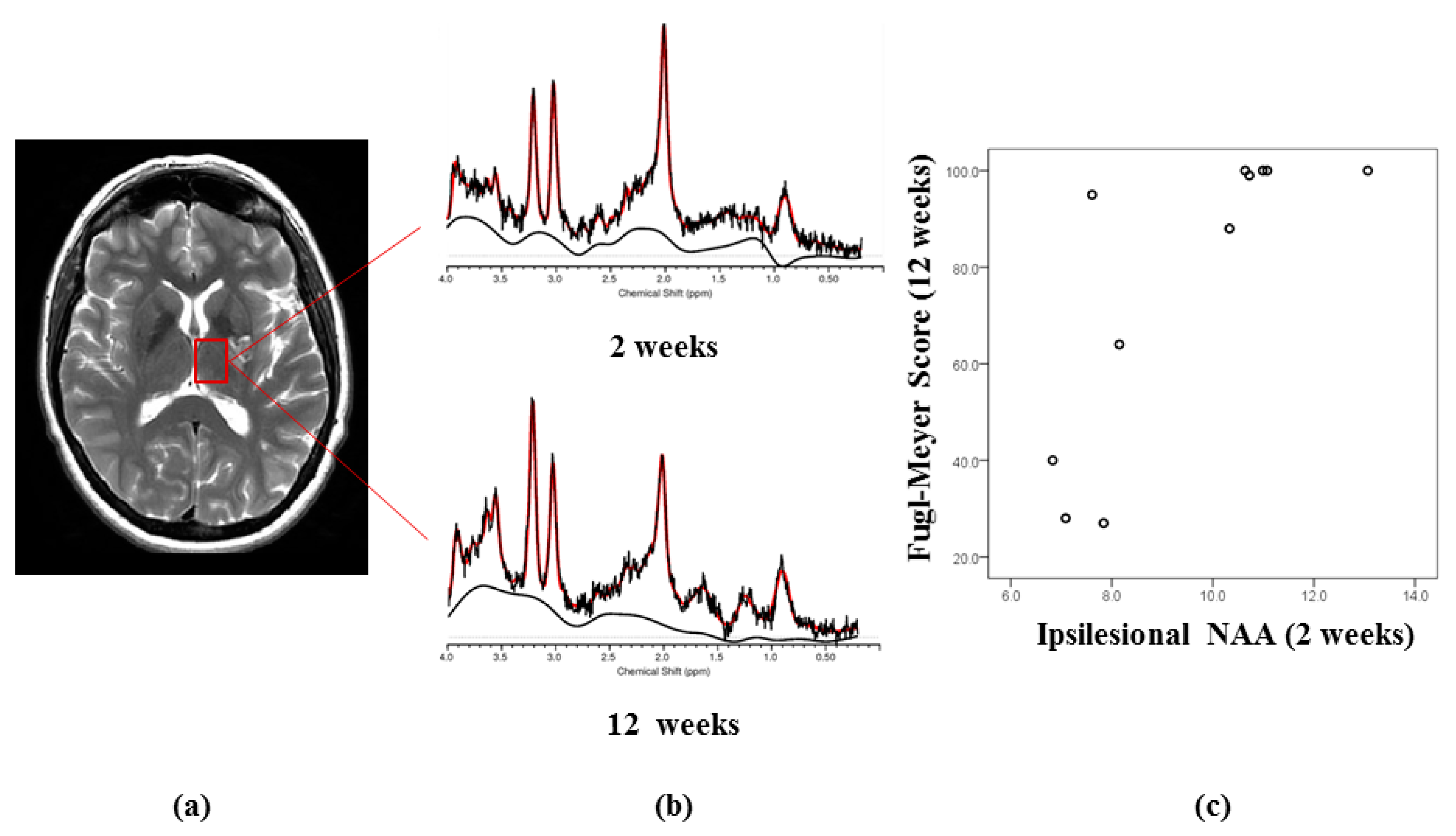
3.4. Relationship of MRS and ASL Measures with Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Duncan, P.W.; Zorowitz, R.; Bates, B.; Choi, J.Y.; Glasberg, J.J.; Graham, G.D.; Katz, R.C.; Lamberty, K.; Reker, D. Management of Adult Stroke Rehabilitation Care: A clinical practice guideline. Stroke 2005, 36, e100–e143. [Google Scholar] [CrossRef]
- Cramer, S.C. Repairing the human brain after stroke: I. Mechanisms of spontaneous recovery. Ann. Neurol. 2008, 63, 272–287. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.G.; Chopp, M. Neurorestorative therapies for stroke: Underlying mechanisms and translation to the clinic. Lancet Neurol. 2009, 8, 491–500. [Google Scholar] [CrossRef] [Green Version]
- Sztriha, L.K.; O’Gorman, R.L.; Modo, M.; Barker, G.J.; Williams, S.C.R.; Kalra, L. Monitoring brain repair in stroke using advanced magnetic resonance imaging. Stroke 2012, 43, 3124–3131. [Google Scholar] [CrossRef] [Green Version]
- Hervé, D.; Molko, N.; Pappata, S.; Buffon, F.; LeBihan, D.; Bousser, M.G.; Chabriat, H. Longitudinal thalamic diffusion changes after middle cerebral artery infarcts. J. Neurol. Neurosurg. Psychiatry 2005, 76, 200–205. [Google Scholar] [CrossRef]
- Munoz Maniega, S.; Cvoro, V.; Chappell, F.M.; Armitage, P.A.; Marshall, I.; Bastin, M.E.; Wardlaw, J.M. Changes in NAA and lactate following ischemic stroke: A serial MR spectroscopic imaging study. Neurology 2008, 71, 1993–1999. [Google Scholar] [CrossRef]
- Li, C.; Ling, X.; Liu, S.; Xu, A.; Zhang, Y.; Xing, S.; Pei, Z.; Zeng, J. Early detection of secondary damage in ipsilateral thalamus after acute infarction at unilateral corona radiata by diffusion tensor imaging and magnetic resonance spectroscopy. BMC Neurol. 2011, 11, 49. [Google Scholar] [CrossRef] [Green Version]
- Gerhard, A.; Schwarz, J.; Myers, R.; Wise, R.; Banati, R.B. Evolution of microglial activation in patients after ischemic stroke: A [11 C](R)-PK11195 PET study. Neuroimage 2005, 24, 591–595. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Barker, P.B. MR Spectroscopy and Spectroscopic Imaging of the Brain. Methods Mol. Biol. 2011, 711, 203–226. [Google Scholar] [PubMed] [Green Version]
- Rae, C.D. A Guide to the Metabolic Pathways and Function of Metabolites Observed in Human Brain 1H Magnetic Resonance Spectra. Neurochem. Res. 2014, 39, 1–36. [Google Scholar] [CrossRef] [PubMed]
- Rigotti, D.J.; Inglese, M.; Gonen, O. Whole-brain N-acetylaspartate as a surrogate marker of neuronal damage in diffuse neurologic disorders. Am. J. Neuroradiol. 2007, 28, 1843–1849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petroff, O.A.; Graham, G.D.; Blamire, A.M.; al-Rayess, M.; Rothman, D.L.; Fayad, P.B.; Brass, L.M.; Shulman, R.G.; Prichard, J.W. Spectroscopic imaging of stroke in humans: Histopathology correlates of spectral changes. Neurology 1992, 42, 1349–1354. [Google Scholar] [CrossRef] [PubMed]
- Font, M.A.; Arboix, A.; Krupinski, J. Angiogenesis, neurogenesis and neuroplasticity in ischemic stroke. Curr. Cardiol. Rev. 2010, 6, 238–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaharchuk, G. Arterial spin labeled perfusion imaging in acute ischemic stroke. Stroke 2014, 45, 1202–1207. [Google Scholar] [CrossRef] [Green Version]
- Walker, P.M.; Ben Salem, D.; Lalande, A.; Giroud, M.; Brunotte, F. Time course of NAA T2 and ADC(w) in ischaemic stroke patients: H-1 MRS imaging and diffusion weighted MRI. J. Neurol. Sci. 2004, 220, 23–28. [Google Scholar] [CrossRef]
- Wahlund, L.O.; Barkhof, F.; Fazekas, F.; Bronge, L.; Augustin, M.; Sjogren, M.; Wallin, A.; Adèr, H.; Leys, D.; Pantoni, L.; et al. A New Rating Scale for Age-Related White Matter Changes Applicable to MRI and CT. Stroke 2001, 32, 1318–1322. [Google Scholar] [CrossRef]
- Ward, N.S.; Brown, M.M.; Thompson, A.J.; Frackowiak, R.S. Neural correlates of motor recovery after stroke: A longitudinal FMRI study. Brain 2003, 126, 2476–2496. [Google Scholar] [CrossRef]
- Provencher, S.W. Automatic quantitation of localized in vivo 1H spectra with LC Model. NMR Biomed. 2001, 14, 260–264. [Google Scholar] [CrossRef]
- Dai, W.; Garcia, D.; de Bazelaire, C.; Alsop, D.C. Continuous flow-driven inversion for arterial spin labeling using pulsed radio frequency and gradient fields. Magn. Reason. Med. 2008, 60, 1488–1497. [Google Scholar] [CrossRef] [Green Version]
- Gladstone, D.J.; Danells, C.J.; Black, S.E. The fugl-meyer assessment of motor recovery after stroke: A critical review of its measurement properties. Neurorehabil. Neural Repair 2002, 16. [Google Scholar] [CrossRef]
- Rehabilitation Measures Database. Available online: http://www.rehabmeasures.org/Lists/RehabMeasures/DispForm.aspx?ID=889 (accessed on 5 July 2015).
- White, I.R.; Royston, P.; Wood, A.M. Multiple imputation using chained equations: Issues and guidance for practice. Stat. Med. 2011, 30, 377–399. [Google Scholar] [CrossRef] [PubMed]
- Wardlaw, J.M.; Dennis, M.S.; Lindley, R.I.; Warlow, C.P.; Sandercock, P.A.G.; Sellar, R. Does early reperfusion of a cerebral infarct influence cerebral infarct swelling in the acute stage or the final clinical outcome? Cerebrovasc. Dis. 1993, 3, 86–93. [Google Scholar] [CrossRef]
- Sijens, P.E.; den Heijer, T.; de Leeuw, F.E.; de Groot, J.C.; Acheten, E.; Heijboer, R.J.; Hofman, A.; Breteler, M.M.; Oudkerk, M. MR spectroscopy detection of lactate and lipid signals in the brains of healthy elderly people. Eur. Radiol. 2001, 11, 1495–1501. [Google Scholar] [CrossRef]
- Walter, H.L.; Walberer, M.; Rueger, M.A.; Backes, H.; Wiedermann, D.; Hoehn, M.; Neumaier, B.; Graf, R.; Fink, G.R.; Schroeter, M. In vivo analysis of neuroinflammation in the late chronic phase after experimental stroke. Neuroscience 2015, 292, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Tsai, G.; Coyle, J.T. N-acetylaspartate in neuropsychiatric disorders. Prog. Neurobiol. 1995, 46, 531–540. [Google Scholar] [CrossRef]
- Kirov, I.I.; Tal, A.; Babb, J.S.; Herbert, J.; Gonen, O. Serial proton MR spectroscopy of gray and white matter in relapsing-remitting MS. Neurology 2013, 80, 39–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Gorman, R.L.; Siddiqui, A.; Alsop, D.C.; Jarosz, J.M. Perfusion MRI demonstrates crossed-cerebellar diaschisis in sickle cell disease. Pediatr. Neurol. 2010, 42, 437–440. [Google Scholar] [CrossRef] [Green Version]
- Chu, W.J.; Mason, G.F.; Pan, J.W.; Hetherington, H.P.; Liu, H.G.; San Pedro, E.C.; Mountz, J.M. Regional cerebral blood flow and magnetic resonance spectroscopic imaging findings in diaschisis from stroke. Stroke 2002, 33, 1243–1248. [Google Scholar] [CrossRef] [Green Version]
- Carrera, E.; Tononi, G. Diaschisis: Past, Present, Future. Brain 2014, 137, 2408–2422. [Google Scholar] [CrossRef] [Green Version]
- Craciunas, S.C.; Brooks, W.M.; Nudo, R.J.; Popescu, E.A.; Choi, I.Y.; Lee, P.; Yeh, H.W.; Savage, C.R.; Cirstea, C.M. Motor and premotor cortices in subcortical stroke: Proton magnetic resonance spectroscopy measures and arm motor impairment. Neurorehabil. Neural Repair 2013, 27, 411–420. [Google Scholar] [CrossRef] [Green Version]
- Bivard, A.; Krishnamurthy, V.; Stanwell, P.; Yassi, N.; Spratt, N.J.; Nilsson, M.; Levi, C.R.; Davis, S.; Parsons, M.W. Spectroscopy of reperfused tissue after stroke reveals heightened metabolism in patients with good clinical outcomes. J. Cereb. Blood Flow Metab. 2014, 34, 1944–1950. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Metabolite | Group | VOI Location | Baseline | 6 Weeks | 12 Weeks | p-Value (Longitudinal Change in Patients) | p-Value (Patients at Baseline vs. Controls) § |
|---|---|---|---|---|---|---|---|
| NAA (mmol/L) | Patient | Ipsilesional thalamus | 10.0 (2.03) | 6.85 (4.08) | 7.97 (1.69) | 0.003 ** | |
| Contralesional thalamus | 10.46 (1.94) | 12.18 (3.42) | 10.52 (0.92) | 0.19 | |||
| Control | Left thalamus | 11.17 (1.01) | 0.27 | ||||
| Right thalamus | 11.19 (0.59) | 0.23 | |||||
| Cho (mmol/L) | Patient | Ipsilesional | 2.33 (0.35) | 2.51 (1.17) | 2.82 (0.58) | 0.025 * | |
| Contralesional | 1.98 (0.28) | 2.40 (0.90) | 2.56 (1.18) | 0.22 | |||
| Control | left | 2.06 (0.33) | 0.009 ** | ||||
| right | 2.00 (0.21) | 0.87 | |||||
| mI (mmol/L) | Patient | Ipsilesional | 4.29 (2.06) | 4.07 (3.11) | 6.33 (3.21) | 0.031 * | |
| Contralesional | 4.38 (2.25) | 4.29 (1.54) | 4.32 (1.43) | 0.82 | |||
| Control | left | 4.07 (1.44) | 0.62 | ||||
| right | 3.97 (1.06) | 0.27 | |||||
| Creatinine (mmol/L) | Patient | Ipsilesional | 5.63 (0.36) | 6.31 (1.33) | 7.38 (1.75) | 0.003 ** | |
| Contralesional | 6.63 (2.19) | 6.86 (2.82) | 6.14 (3.20) | 0.44 | |||
| Control | left | 7.08 (0.66) | 0.0001 * | ||||
| right | 6.92 (2.14) | 0.43 | |||||
| Lactate (mmol/L) | Patient | Ipsilesional | 0.90 (1.11) | 1.77 (1.61) | 2.03 (1.49) | 0.001 ** | |
| Contralesional | 0.66 (1.13) | 0.70 (1.16) | 0.72 (0.67) | 0.79 | |||
| Control | left | 0.47 (0.70) | 0.27 | ||||
| right | 0.30 (0.40) | 0.32 | |||||
| CBF (mL/100 g/min) | Patient | Ipsilesional | 22.72 (8.18) | 31.84 (4.75) | 31.04 (4.18) | 0.004 ** | |
| Contralesional | 32.93 (8.47) | 36.10 (4.82) | 32.17 (8.32) | 0.58 | |||
| Control | left | 36.81 (6.77) | 0.004 ** | ||||
| right | 38.64 (7.95) | 0.25 | |||||
| Clinical assessments (patients only) | Baseline | 6 weeks | 12 weeks | p-value (longitudinal change in patients) | |||
| Fugl–Meyer | 43.3 (30.0) | 74.2 (32.2) | 78.3 (30.1) | 0.009 ** | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazibuko, N.; Tuura, R.O.; Sztriha, L.; O’Daly, O.; Barker, G.J.; Williams, S.C.R.; O'Sullivan, M.; Kalra, L. Subacute Changes in N-Acetylaspartate (NAA) Following Ischemic Stroke: A Serial MR Spectroscopy Pilot Study. Diagnostics 2020, 10, 482. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10070482
Mazibuko N, Tuura RO, Sztriha L, O’Daly O, Barker GJ, Williams SCR, O'Sullivan M, Kalra L. Subacute Changes in N-Acetylaspartate (NAA) Following Ischemic Stroke: A Serial MR Spectroscopy Pilot Study. Diagnostics. 2020; 10(7):482. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10070482
Chicago/Turabian StyleMazibuko, Ndaba, Ruth O’Gorman Tuura, Laszlo Sztriha, Owen O’Daly, Gareth J. Barker, Steven C. R. Williams, Michael O'Sullivan, and Lalit Kalra. 2020. "Subacute Changes in N-Acetylaspartate (NAA) Following Ischemic Stroke: A Serial MR Spectroscopy Pilot Study" Diagnostics 10, no. 7: 482. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10070482