
Medullary Carcinoma of the Gastrointestinal Tract: Report on Two Cases with Immunohistochemical and Molecular Features

 , ,
, , {kind=link}
{kind=link}
Abstract
:1. Introduction
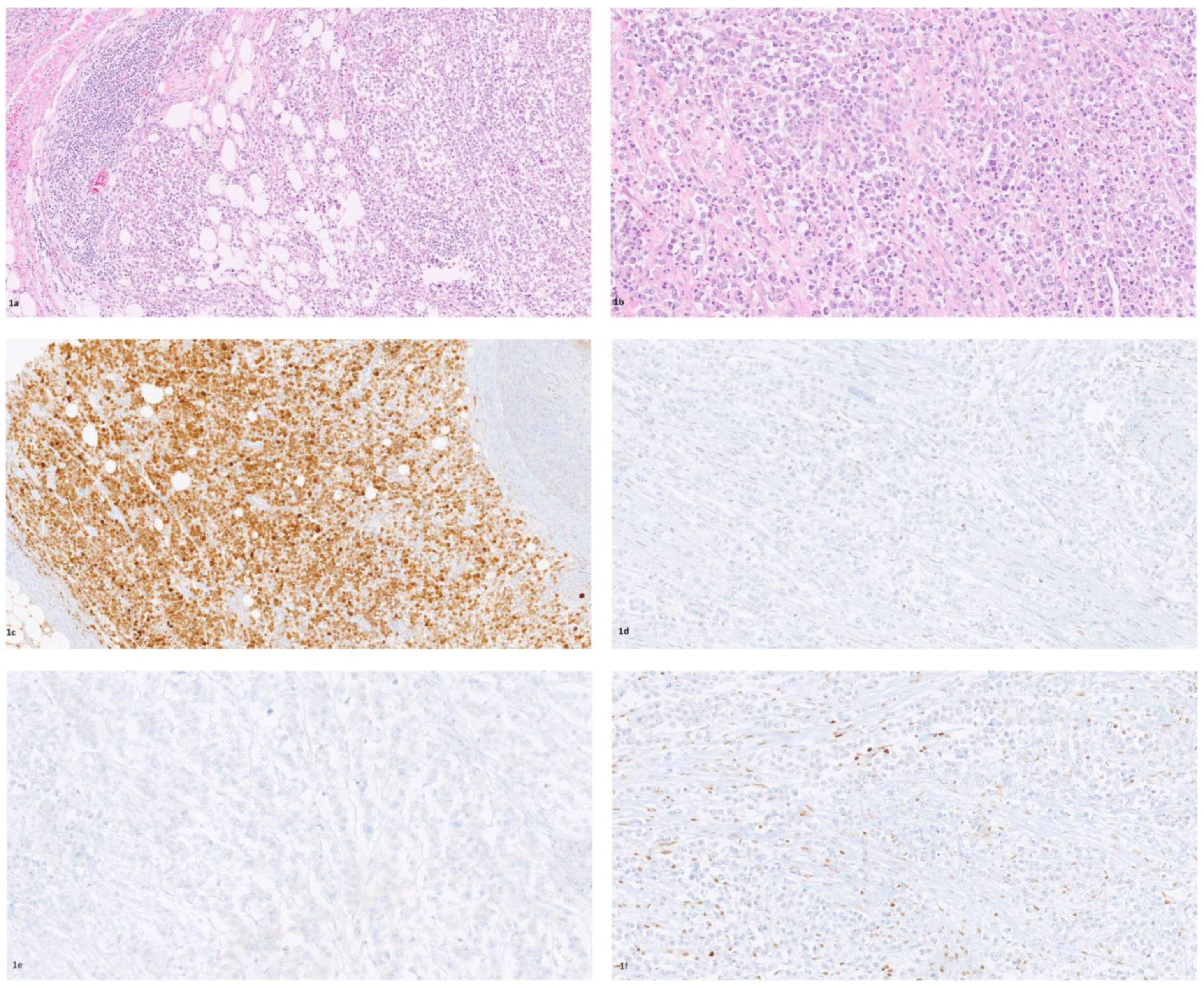
2. Case Report 1
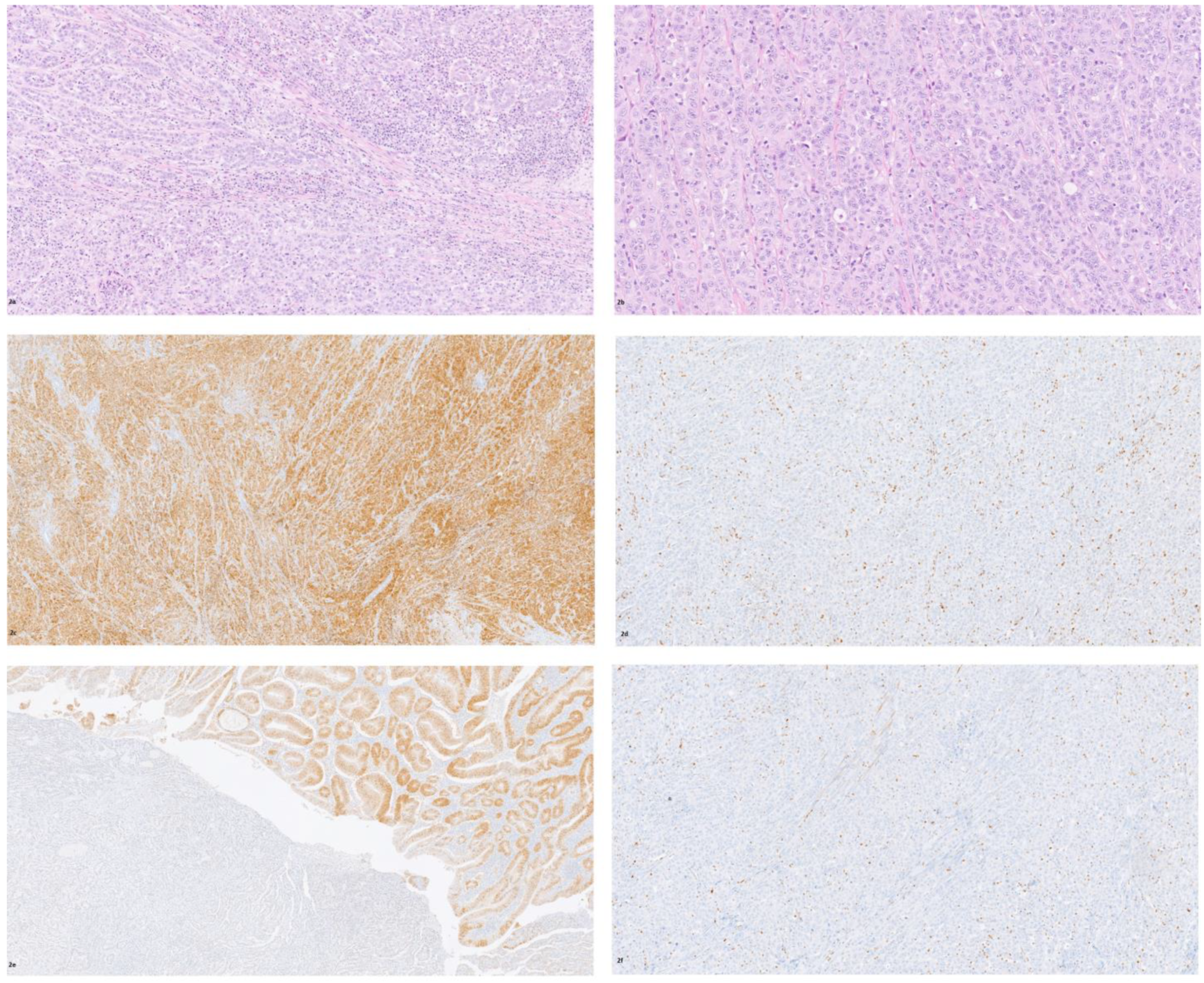
3. Case Report 2
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Argilés, G.; Tabernero, J.; Labianca, R.; Hochhauser, D.; Salazar, R.; Iveson, T.; Laurent-Puig, P.; Quirke, P.; Yoshino, T.; Taieb, J.; et al. ESMO guidelines committee. Localised colon cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 1291–1305. [Google Scholar] [CrossRef]
- Fleming, M.; Ravula, S.; Tatishchev, S.; Wang, H.L. Colorectal carcinoma: Pathologic aspects. Gastrointest. Oncol. 2012, 3, 153. [Google Scholar]
- Samadder, N.J.; Jasperson, K.; Burt, R.W. Hereditary and common familial colorectal cancer: Evidence for colorectal screening. Dig. Dis. Sci. 2015, 60, 734–747. [Google Scholar] [CrossRef]
- Guinney, J.; Dienstmann, R.; Wang, X.; de Reyniès, A.; Schlicker, A.; Soneson, C.; Marisa, L.; Roepman, P.; Nyamundanda, G.; Angelino, P.; et al. The consensus molecular subtypes of colorectal cancer. Nat. Med. 2015, 21, 1350–1356. [Google Scholar] [CrossRef]
- Sammarco, G.; Gallo, G.; Vescio, G.; Picciariello, A.; De Paola, G.; Trompetto, M.; Currò, G.; Ammendola, M. Mast cells, microRNAs and others: The role of translational research on colorectal cancer in the forthcoming era of precision medicine. J. Clin. Med. 2020, 9, 2852. [Google Scholar] [CrossRef]
- Vakil, N.; Ciezki, K.; Singh, M. Colorectal cancer in 18 to 49-year-olds: Rising rates, presentation, and outcome in a large integrated health system. Gastrointest. Endosc. 2021, 94, 618–626. [Google Scholar] [CrossRef]
- Knox, R.D.; Luey, N.; Sioson, L.; Kedziora, A.; Clarkson, A.; Watson, N.; Toon, C.W.; Cussigh, C.; Pincott, S.; Pillinger, S.; et al. Medullary colorectal carcinoma revisited: A clinical and pathological study of 102 cases. Ann. Surg. Oncol. 2015, 22, 2988–2996. [Google Scholar] [CrossRef]
- Martinotti, M.; Cirillo, F.; Ungari, M.; Tanzi, G.; Rolando, G.; Tarasconi, A.; Ranieri, V.; Aulisa, P.; Vismarra, M.; Rovatti, M.; et al. Microsatellite instability in medullary carcinoma of the colon. Rare Tumors 2017, 9, 6541. [Google Scholar] [CrossRef]
- Remo, A.; Fassan, M.; Vanoli, A.; Bonetti, L.R.; Barresi, V.; Tatangelo, F.; Gafà, R.; Giordano, G.; Pancione, M.; Grillo, F.; et al. Morphology and molecular features of rare colorectal carcinoma histotypes. Cancers 2019, 11, 1036. [Google Scholar] [CrossRef] [Green Version]
- Cunningham, J.; Kantekure, K.; Saif, M.W. Medullary carcinoma of the colon: A case series and review of the literature. Vivo 2014, 28, 311–314. [Google Scholar]
- Kasapidis, P.; Grivas, E.; Papamichail, V.; Alfaras, P. Medullary carcinoma of the colon: An adenocarcinoma with better prognosis. Ann. Gastroenterol. 2015, 28, 289. [Google Scholar]
- Brcic, I.; Cathomas, G.; Vanoli, A.; Jilek, K.; Giuffrida, P.; Langner, C. Medullary carcinoma of the small bowel. Histopathology 2016, 69, 136–140. [Google Scholar] [CrossRef] [PubMed]
- Rüschoff, J.; Dietmaier, W.; Lüttges, J.; Seitz, G.; Bocker, T.; Zirngibl, H.; Schlegel, J.; Schackert, H.K.; Jauch, K.W.; Hofstaedter, F. Poorly differentiated colonic adenocarcinoma, medullary type: Clinical, phenotypic, and molecular characteristics. Am. J. Pathol. 1997, 150, 1815–1825. [Google Scholar] [PubMed]
- Jessurun, J.; Romero-Guadarrama, M.; Manivel, L.C. Medullary adenocarcinoma of the colon: Clinicopathologic study of 11 cases. Hum. Pathol. 1999, 30, 843–848. [Google Scholar] [CrossRef]
- Thirunavukarusu, P.; Sathaiah, M.; Singla, S.; Sukumar, S.; Karunamurthy, A.; Pragatheeshwar, K.D.; Lee, K.K.W.; Zeh, H.; Kane, K.M.; Bartlett, D.L. Medullary carcinoma of the large intestine: A population based analysis. Int. J. Oncol. 2010, 37, 901–907. [Google Scholar]
- Scott, N.; West, N.P.; Cairns, A.; Rotimi, O. Is medullary carcinoma of the colon underdiagnosed? An audit of poorly differentiated colorectal carcinomas in a large NHS teaching hospital. Histopathology 2021, 78, 963–969. [Google Scholar] [CrossRef] [PubMed]
- WHO Classification of Tumours Editorial Board. Digestive System Tumours, 5th ed.; WHO Classification of Tumours Editorial Board: Lyon, France, 2019; p. 181. [Google Scholar]
- Lee, L.H.; Yantiss, R.K.; Sadot, E.; Ren, B.; Marcela, M.S.; Hechtman, J.F.; Ivelja, S.; Huynh, B.; Xue, Y.; Shitilbans, T.; et al. Diagnosing colorectal medullary carcinoma: Interobserver variability and clinicopathological implications. Hum. Pathol. 2017, 62, 74–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winn, B.; Tavares, R.; Faniona, J.; Noblea, L.; Gao, J.; Sabo, E.; Resnick, M.B. Differentiating the undifferentiated: Immunohistochemical profile of medullary carcinoma of the colon with an emphasis on intestinal differentiation. Hum. Pathol. 2009, 40, 398–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ye, J.; Zhou, Y.; Weiser, M.R.; Gönen, M.; Zhang, L.; Samdani, T.; Bacares, R.; De Lair, D.; Ivelja, S.; Vakiani, E.; et al. Immunohistochemical detection of ARID1A in colorectal carcinoma: Loss of staining is associated with sporadic microsatellite unstable tumors with medullary histology and high TNM stage. Hum. Pathol. 2014, 45, 2430–2436. [Google Scholar] [CrossRef] [PubMed]
- Cancer Genome Atlas Network. Comprehensive molecular characterization of human colon and rectal cancer. Nature 2012, 487, 330–337. [Google Scholar] [CrossRef] [Green Version]
- Chou, A.; Toon, C.W.; Clarkson, A.; Sioson, L.; Houang, M.; Watson, N.; DeSilva, K.; Gill, A.J. Loss of ARID1A expression in colorectal carcinoma is strongly associated with mismatch repair deficiency. Hum. Pathol. 2014, 45, 1697–1703. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, M.W.; Bledsoe, J.R.; Morales-Oyarvide, V.; Huynh, T.G.; Mino-Kenudson, M. PD-L1 expression in colorectal cancer is associated with microsatellite instability, BRAF mutation, medullary morphology and cytotoxic tumor-infiltrating lymphocytes. Mod. Pathol. 2016, 29, 1104–1112. [Google Scholar] [CrossRef] [PubMed]
- Raghav, K.; Michael, J. Overman small bowel adenocarcinomas—evolving paradigms and therapy options. Nat. Rev. Clin. Oncol. 2013, 10, 534–544. [Google Scholar] [CrossRef] [PubMed]
- Friedman, K.; Brodsky, A.S.; Lu, S.; Wood, S.; Gill, A.J.; Lombardo, K.; Yang, D.; Resnick, M.B. Medullary carcinoma of the colon: A distinct morphology reveals a distinctive immunoregulatory microenvironment. Mod. Pathol. 2016, 29, 528–541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nazemalhosseini-Mojarad, E.; Mohammadpour, S.; Esafahani, A.T.; Gharib, E.; Larki, P.; Moradi, A.; Porhoseingholi, M.A.; Aghdaei, H.A.; Kuppen, P.J.K.; Zali, M.R. Intratumoral infiltrating lymphocytes correlate with improved survival in colorectal cancer patients: Independent of oncogenetic features. J. Cell. Physiol. 2019, 234, 4768–4777. [Google Scholar] [CrossRef]
- Lanza, G.; Gafà, R.; Matteuzzi, M.; Santini, A. Medullary-type poorly differentiated adenocarcinoma of the large bowel: A distinct clinicopathologic entity characterized by microsatellite instability and improved survival. J. Clin. Oncol. 1999, 17, 2429–2438. [Google Scholar] [CrossRef]
- Pyo, J.S.; Sohn, J.H.; Kang, G. Medullary carcinoma in the colorectum: A systematic review and meta-analysis. Hum. Pathol. 2016, 53, 91–96. [Google Scholar] [CrossRef]
- Lin, C.C.; Lai, Y.L.; Lin, T.C.; Chen, W.S.; Jiang, J.K.; Yang, S.H.; Wang, H.S.; Lan, Y.T.; Liang, W.Y.; Hsu, H.M.; et al. Clinicopathologic features and prognostic analysis of MSI-high colon cancer. Int. J. Colorectal. Dis. 2012, 27, 277–286. [Google Scholar] [CrossRef] [PubMed]
- Ogino, S.; Shima, K.; Meyerhardt, J.A.; McCleary, N.J. Predictive and prognostic roles of BRAF mutation in stage III colon cancer: Results from intergroup trial CALGB 89803. Clin. Canc. Res. 2012, 18, 890–900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dalerba, P.; Sahoo, D.; Paik, S.; Guo, X.; Yothers, G.; Song, N.; Wilcox-Fogel, N.; Forgó, E.; Rajendran, P.S.; Miranda, S.P.; et al. CDX2 as a prognostic biomarker in stage II and stage III colon cancer. N. Engl. J. Med. 2016, 374, 211–222. [Google Scholar] [CrossRef]
- Colarossi, C.; Picardo, M.C.; Colarossi, L.; Deiana, E.; D’Agata, C.; Fichera, C.; Aiello, E.; Giannone, G.; Memeo, L. Clear cell carcinoma arising in abdominal wall cesarean section scar: A case report with description of pathological and molecular features. Front. Surg. 2021, 8, 735381. [Google Scholar] [CrossRef]
- Wei, X.L.; Wang, D.S.; Xi, S.Y.; Wu, W.J.; Chen, D.L.; Zeng, Z.L.; Wang, R.Y.; Huang, Y.X.; Jin, Y.; Wang, F.; et al. Clinicopathologic and prognostic relevance of ARID1A protein loss in colorectal cancer. World J. Gastroenterol. 2014, 20, 18404–18412. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colarossi, C.; Mare, M.; La Greca, G.; De Zuanni, M.; Colarossi, L.; Aiello, E.; Piombino, E.; Memeo, L. Medullary Carcinoma of the Gastrointestinal Tract: Report on Two Cases with Immunohistochemical and Molecular Features. Diagnostics 2021, 11, 1775. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11101775
Colarossi C, Mare M, La Greca G, De Zuanni M, Colarossi L, Aiello E, Piombino E, Memeo L. Medullary Carcinoma of the Gastrointestinal Tract: Report on Two Cases with Immunohistochemical and Molecular Features. Diagnostics. 2021; 11(10):1775. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11101775
Chicago/Turabian StyleColarossi, Cristina, Marzia Mare, Giorgio La Greca, Marco De Zuanni, Lorenzo Colarossi, Eleonora Aiello, Eliana Piombino, and Lorenzo Memeo. 2021. "Medullary Carcinoma of the Gastrointestinal Tract: Report on Two Cases with Immunohistochemical and Molecular Features" Diagnostics 11, no. 10: 1775. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11101775