
CEA, EpCAM, αvβ6 and uPAR Expression in Rectal Cancer Patients with a Pathological Complete Response after Neoadjuvant Therapy

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Material and Methods
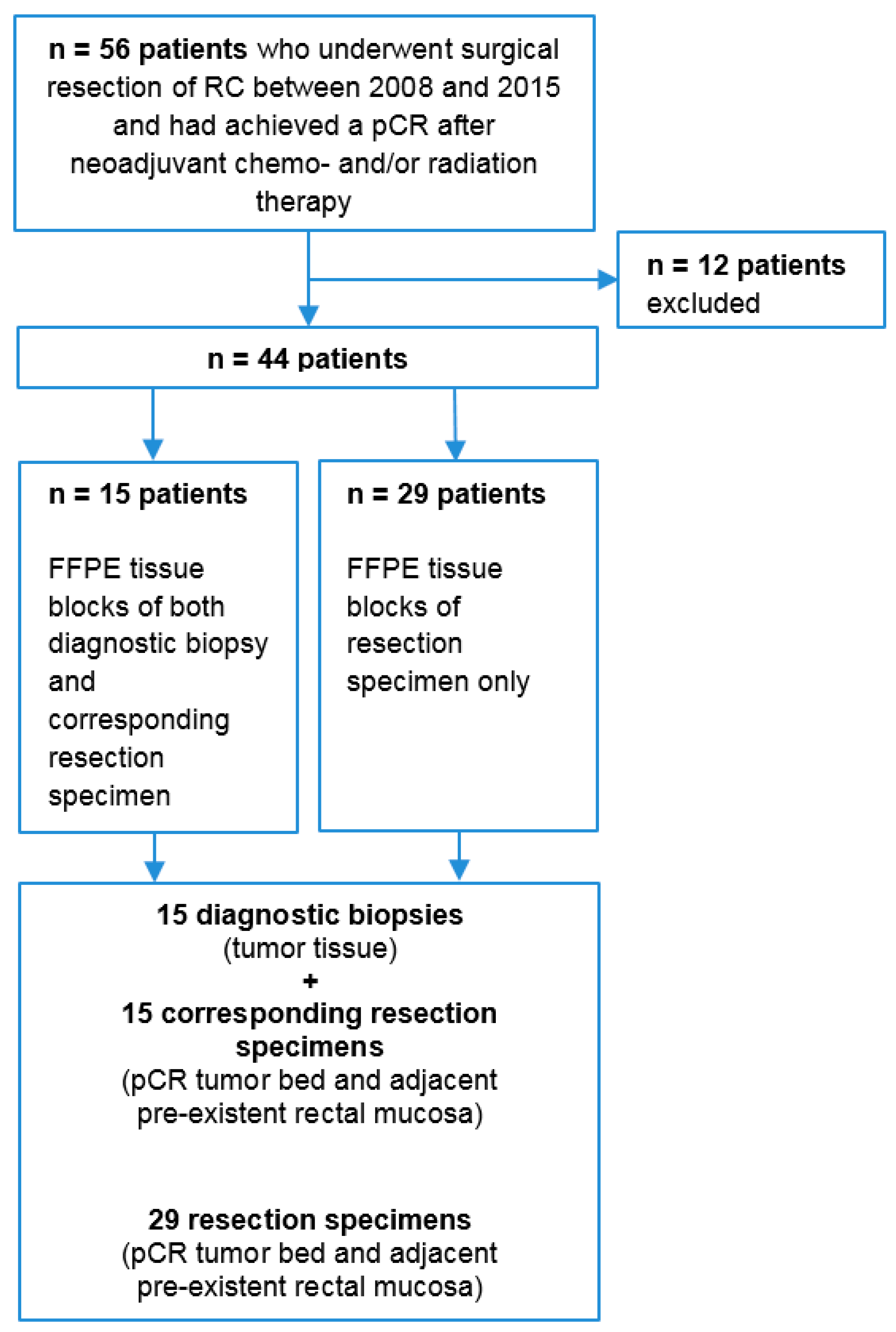
2.1. Human Rectal Cancer Tissue Samples
2.2. Immunohistochemistry (IHC)
2.3. Scoring Method
2.4. Statistical Analysis
3. Results
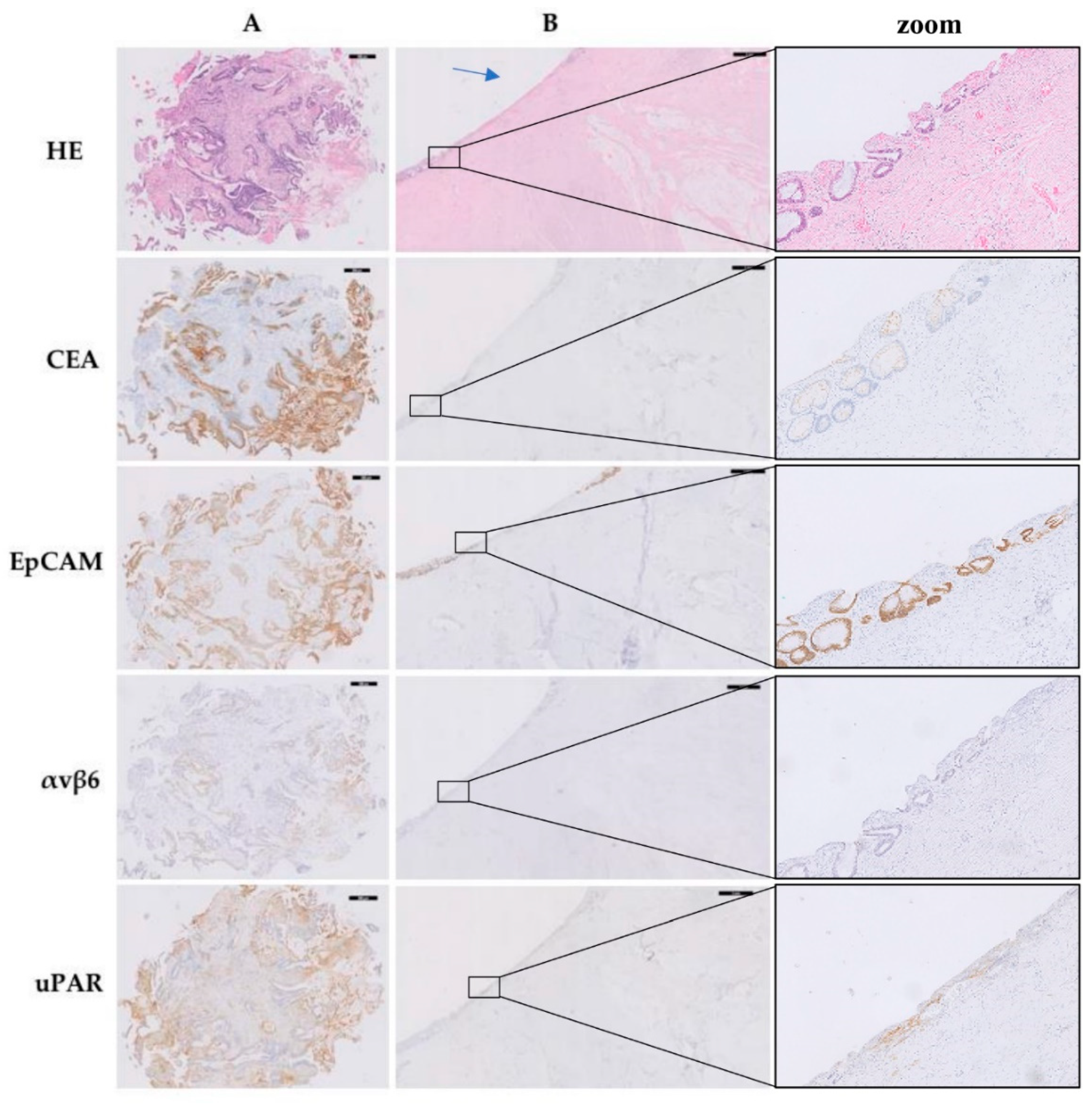
3.1. CEA, EpCAM, αvβ6, and uPAR Expression
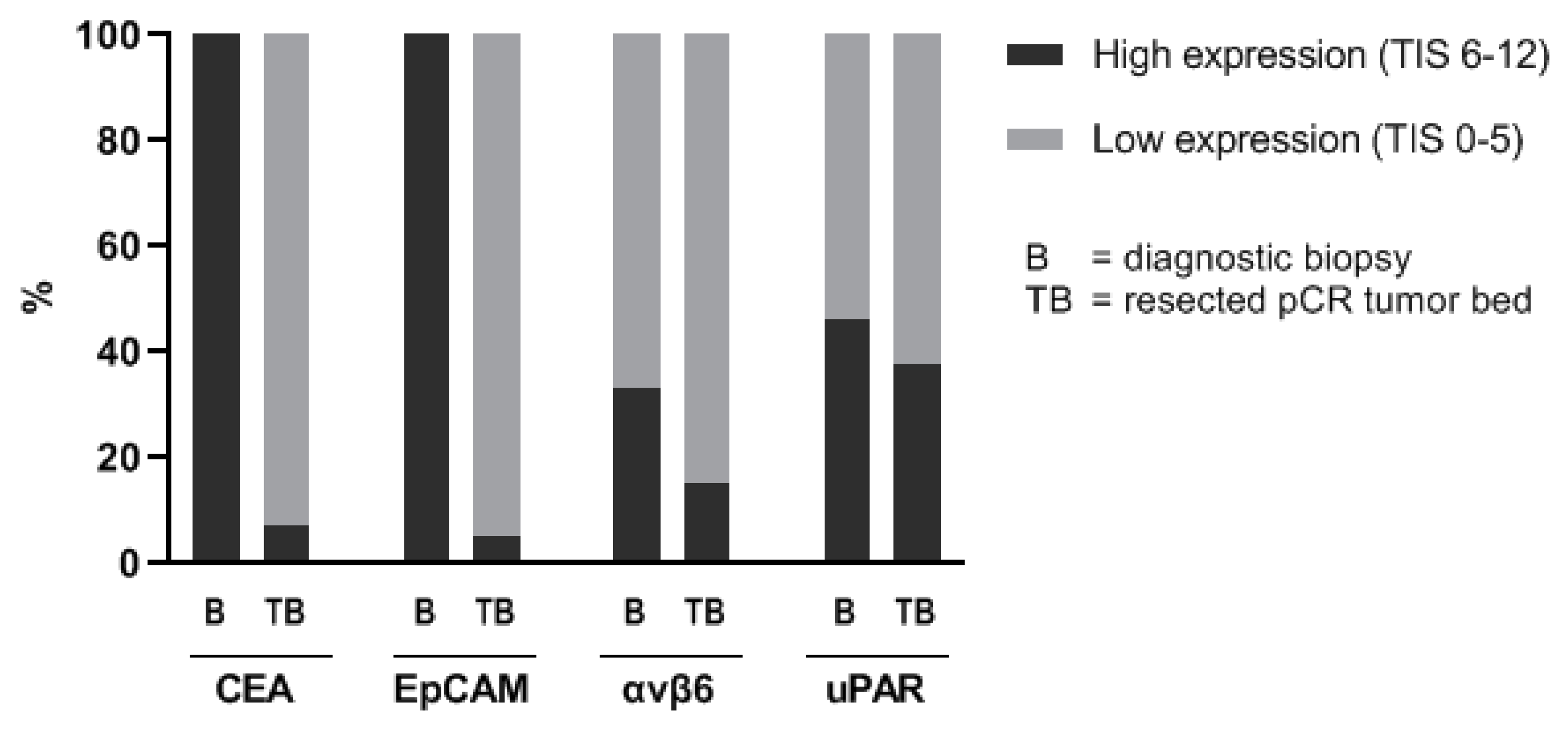
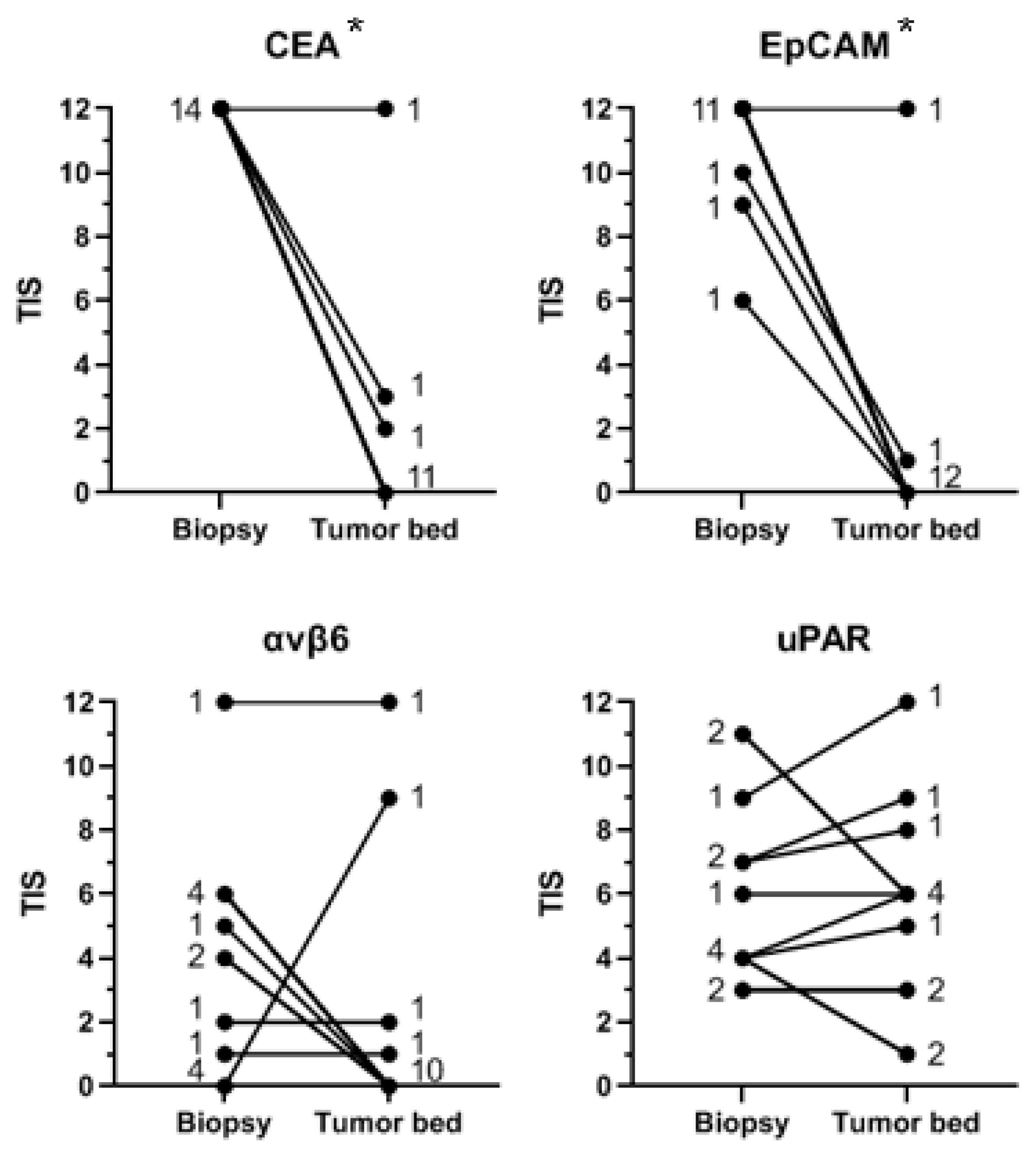
3.2. Comparison of Protein Expression in Tumor Tissue in Diagnostic Biopsy and Corresponding Tumor Bed after Neoadjuvant Therapy
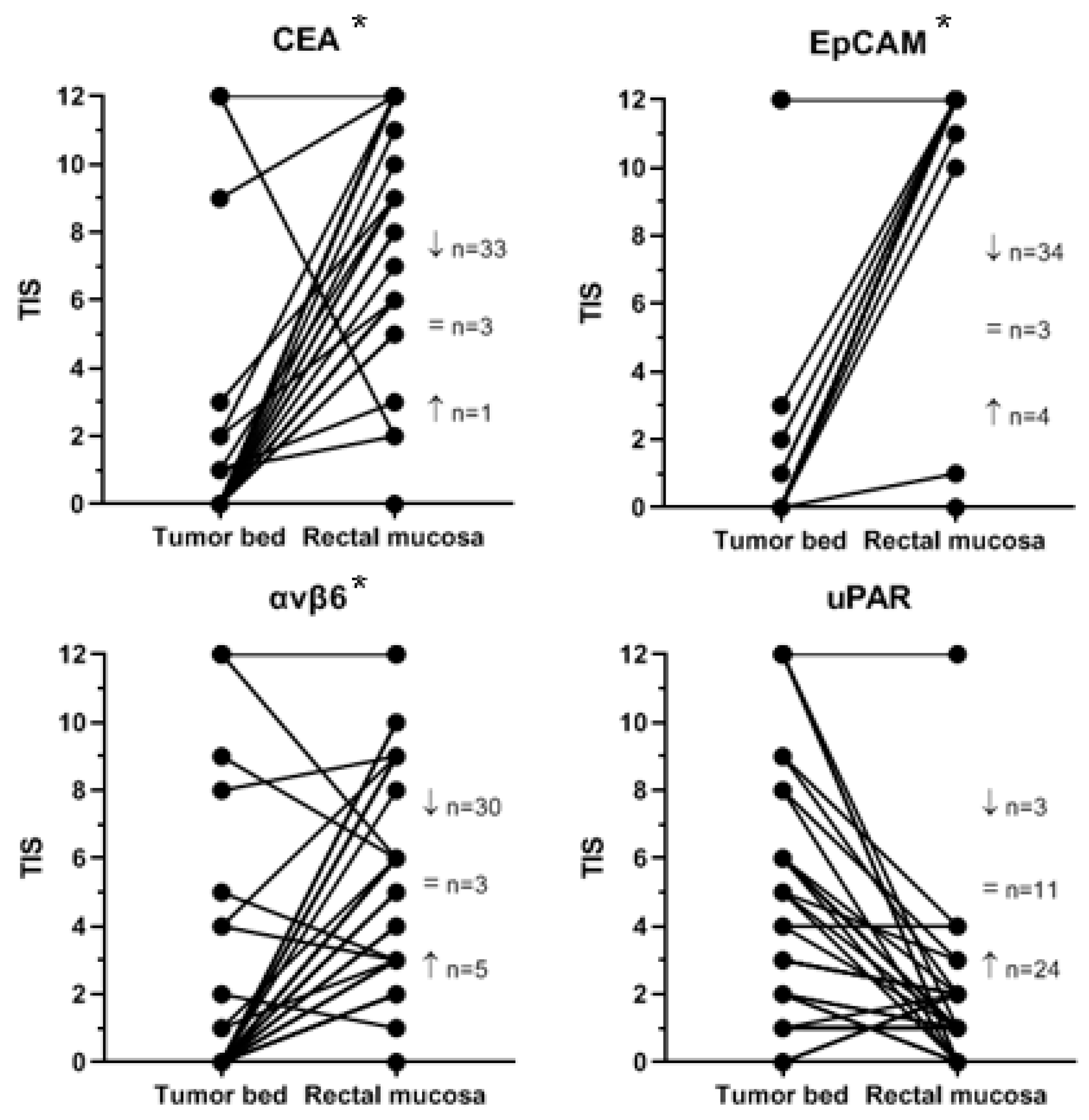
3.3. Comparison of Protein Expression in Tumor Bed and Adjacent Pre-Existent Rectal Mucosa
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antibody | Company | Clone | Stock Concentration | Dilution | Antigen Retrieval |
|---|---|---|---|---|---|
| Anti-CEACAM5 | SantaCruz Biotechnology | Cl-P83-1 | 0.2 µg/mL | 1/1000 | Dako PT Link Target Retrieval Solution, pH 6.0 |
| Anti-EpCAM | Acris Antibodies | MOC31 | 0.64 mg/mL | 1/10,000 | Dako PT Link Target Retrieval Solution, pH 6.0 |
| Anti-αvβ6 | Biogen Idec | 6.2A1 | 0.5 µg/mL | - | 0.4% Pepsin |
| Anti-uPAR | Monopar Therapeutics Inc | ATN617 | 0.48 mg/mL | 1/400 | Dako PT Link Target Retrieval Solution, pH 6.0 |
| Biopsy and Resection (n) | Tumor Bed and Normal Epithelium (n) | |
|---|---|---|
| CEA | 14 | 37 |
| EpCAM | 14 | 37 |
| αvβ6 | 14 | 38 |
| uPAR | 12 | 38 |
References
- MacFarlane, J.K.; Ryall, R.D.; Heald, R.J. Mesorectal excision for rectal cancer. Lancet 1993, 341, 457–460. [Google Scholar] [CrossRef]
- Sauer, R.; Becker, H.; Hohenberger, W.; Rodel, C.; Wittekind, C.; Fietkau, R.; Martus, P.; Tschmelitsch, J.; Hager, E.; Hess, C.F.; et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N. Engl. J. Med. 2004, 351, 1731–1740. [Google Scholar] [CrossRef] [Green Version]
- Maas, M.; Nelemans, P.J.; Valentini, V.; Das, P.; Rodel, C.; Kuo, L.J.; Calvo, F.A.; Garcia-Aguilar, J.; Glynne-Jones, R.; Haustermans, K.; et al. Long-term outcome in patients with a pathological complete response after chemoradiation for rectal cancer: A pooled analysis of individual patient data. Lancet Oncol. 2010, 11, 835–844. [Google Scholar] [CrossRef]
- Appelt, A.L.; Ploen, J.; Harling, H.; Jensen, F.S.; Jensen, L.H.; Jorgensen, J.C.; Lindebjerg, J.; Rafaelsen, S.R.; Jakobsen, A. High-dose chemoradiotherapy and watchful waiting for distal rectal cancer: A prospective observational study. Lancet Oncol. 2015, 16, 919–927. [Google Scholar] [CrossRef]
- Dossa, F.; Chesney, T.R.; Acuna, S.A.; Baxter, N.N. A watch-and-wait approach for locally advanced rectal cancer after a clinical complete response following neoadjuvant chemoradiation: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2017, 2, 501–513. [Google Scholar] [CrossRef]
- Maas, M.; Beets-Tan, R.G.; Lambregts, D.M.; Lammering, G.; Nelemans, P.J.; Engelen, S.M.; van Dam, R.M.; Jansen, R.L.; Sosef, M.; Leijtens, J.W.; et al. Wait-and-see policy for clinical complete responders after chemoradiation for rectal cancer. J. Clin. Oncol. 2011, 29, 4633–4640. [Google Scholar] [CrossRef]
- Renehan, A.G.; Malcomson, L.; Emsley, R.; Gollins, S.; Maw, A.; Myint, A.S.; Rooney, P.S.; Susnerwala, S.; Blower, A.; Saunders, M.P.; et al. Watch-and-wait approach versus surgical resection after chemoradiotherapy for patients with rectal cancer (the OnCoRe project): A propensity-score matched cohort analysis. Lancet Oncol. 2016, 17, 174–183. [Google Scholar] [CrossRef]
- Smith, J.D.; Ruby, J.A.; Goodman, K.A.; Saltz, L.B.; Guillem, J.G.; Weiser, M.R.; Temple, L.K.; Nash, G.M.; Paty, P.B. Nonoperative management of rectal cancer with complete clinical response after neoadjuvant therapy. Ann. Surg. 2012, 256, 965–972. [Google Scholar] [CrossRef] [Green Version]
- Van der Valk, M.J.M.; Hilling, D.E.; Bastiaannet, E.; Meershoek-Klein Kranenbarg, E.; Beets, G.L.; Figueiredo, N.L.; Habr-Gama, A.; Perez, R.O.; Renehan, A.G.; van de Velde, C.J.H.; et al. Long-term outcomes of clinical complete responders after neoadjuvant treatment for rectal cancer in the International Watch & Wait Database (IWWD): An international multicentre registry study. Lancet 2018, 391, 2537–2545. [Google Scholar] [CrossRef] [Green Version]
- Maas, M.; Lambregts, D.M.; Nelemans, P.J.; Heijnen, L.A.; Martens, M.H.; Leijtens, J.W.; Sosef, M.; Hulsewe, K.W.; Hoff, C.; Breukink, S.O.; et al. Assessment of Clinical Complete Response After Chemoradiation for Rectal Cancer with Digital Rectal Examination, Endoscopy, and MRI: Selection for Organ-Saving Treatment. Ann. Surg. Oncol. 2015, 22, 3873–3880. [Google Scholar] [CrossRef] [Green Version]
- Van der Sande, M.E.; Beets, G.L.; Hupkens, B.J.; Breukink, S.O.; Melenhorst, J.; Bakers, F.C.; Lambregts, D.M.; Grabsch, H.I.; Beets-Tan, R.G.; Maas, M. Response assessment after (chemo)radiotherapy for rectal cancer: Why are we missing complete responses with MRI and endoscopy? Eur. J. Surg. Oncol. 2019, 45, 1011–1017. [Google Scholar] [CrossRef] [PubMed]
- Hernot, S.; van Manen, L.; Debie, P.; Mieog, J.S.D.; Vahrmeijer, A.L. Latest developments in molecular tracers for fluorescence image-guided cancer surgery. Lancet Oncol. 2019, 20, e354–e367. [Google Scholar] [CrossRef]
- Boonstra, M.C.; de Geus, S.W.; Prevoo, H.A.; Hawinkels, L.J.; van de Velde, C.J.; Kuppen, P.J.; Vahrmeijer, A.L.; Sier, C.F. Selecting Targets for Tumor Imaging: An Overview of Cancer-Associated Membrane Proteins. Biomark Cancer 2016, 8, 119–133. [Google Scholar] [CrossRef] [Green Version]
- Boogerd, L.S.F.; Boonstra, M.C.; Prevoo, H.; Handgraaf, H.J.M.; Kuppen, P.J.K.; van de Velde, C.J.H.; Fish, A.; Cordfunke, R.A.; Valentijn, A.; Terwisscha van Scheltinga, A.G.; et al. Fluorescence-guided tumor detection with a novel anti-EpCAM targeted antibody fragment: Preclinical validation. Surg. Oncol. 2019, 28, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Boogerd, L.S.F.; Hoogstins, C.E.S.; Schaap, D.P.; Kusters, M.; Handgraaf, H.J.M.; van der Valk, M.J.M.; Hilling, D.E.; Holman, F.A.; Peeters, K.; Mieog, J.S.D.; et al. Safety and effectiveness of SGM-101, a fluorescent antibody targeting carcinoembryonic antigen, for intraoperative detection of colorectal cancer: A dose-escalation pilot study. Lancet Gastroenterol. Hepatol. 2018, 3, 181–191. [Google Scholar] [CrossRef]
- Juhl, K.; Christensen, A.; Persson, M.; Ploug, M.; Kjaer, A. Peptide-Based Optical uPAR Imaging for Surgery: In Vivo Testing of ICG-Glu-Glu-AE105. PLoS ONE 2016, 11, e0147428. [Google Scholar] [CrossRef]
- Tummers, W.S.; Kimura, R.H.; Abou-Elkacem, L.; Beinat, C.; Vahrmeijer, A.L.; Swijnenburg, R.J.; Willmann, J.K.; Gambhir, S.S. Development and Preclinical Validation of a Cysteine Knottin Peptide Targeting Integrin alphavbeta6 for Near-infrared Fluorescent-guided Surgery in Pancreatic Cancer. Clin. Cancer Res. 2018, 24, 1667–1676. [Google Scholar] [CrossRef] [Green Version]
- Boonstra, M.C.; Tolner, B.; Schaafsma, B.E.; Boogerd, L.S.; Prevoo, H.A.; Bhavsar, G.; Kuppen, P.J.; Sier, C.F.; Bonsing, B.A.; Frangioni, J.V.; et al. Preclinical evaluation of a novel CEA-targeting near-infrared fluorescent tracer delineating colorectal and pancreatic tumors. Int. J. Cancer 2015, 137, 1910–1920. [Google Scholar] [CrossRef] [Green Version]
- Hoogstins, C.E.S.; Boogerd, L.S.F.; Sibinga Mulder, B.G.; Mieog, J.S.D.; Swijnenburg, R.J.; van de Velde, C.J.H.; Farina Sarasqueta, A.; Bonsing, B.A.; Framery, B.; Pelegrin, A.; et al. Image-Guided Surgery in Patients with Pancreatic Cancer: First Results of a Clinical Trial Using SGM-101, a Novel Carcinoembryonic Antigen-Targeting, Near-Infrared Fluorescent Agent. Ann. Surg. Oncol. 2018, 25, 3350–3357. [Google Scholar] [CrossRef] [PubMed]
- Patriarca, C.; Macchi, R.M.; Marschner, A.K.; Mellstedt, H. Epithelial cell adhesion molecule expression (CD326) in cancer: A short review. Cancer Treat. Rev. 2012, 38, 68–75. [Google Scholar] [CrossRef]
- Winter, M.J.; Nagtegaal, I.D.; van Krieken, J.H.; Litvinov, S.V. The epithelial cell adhesion molecule (Ep-CAM) as a morphoregulatory molecule is a tool in surgical pathology. Am. J. Pathol. 2003, 163, 2139–2148. [Google Scholar] [CrossRef] [Green Version]
- Spizzo, G.; Fong, D.; Wurm, M.; Ensinger, C.; Obrist, P.; Hofer, C.; Mazzoleni, G.; Gastl, G.; Went, P. EpCAM expression in primary tumour tissues and metastases: An immunohistochemical analysis. J. Clin. Pathol. 2011, 64, 415–420. [Google Scholar] [CrossRef] [Green Version]
- Went, P.T.; Lugli, A.; Meier, S.; Bundi, M.; Mirlacher, M.; Sauter, G.; Dirnhofer, S. Frequent EpCam protein expression in human carcinomas. Hum. Pathol. 2004, 35, 122–128. [Google Scholar] [CrossRef]
- Zhu, B.; Wu, G.; Robinson, H.; Wilganowski, N.; Hall, M.A.; Ghosh, S.C.; Pinkston, K.L.; Azhdarinia, A.; Harvey, B.R.; Sevick-Muraca, E.M. Tumor margin detection using quantitative NIRF molecular imaging targeting EpCAM validated by far red gene reporter iRFP. Mol. Imaging Biol. 2013, 15, 560–568. [Google Scholar] [CrossRef] [PubMed]
- Van Driel, P.B.; Boonstra, M.C.; Prevoo, H.A.; van de Giessen, M.; Snoeks, T.J.; Tummers, Q.R.; Keereweer, S.; Cordfunke, R.A.; Fish, A.; van Eendenburg, J.D.; et al. EpCAM as multi-tumour target for near-infrared fluorescence guided surgery. BMC Cancer 2016, 16, 884. [Google Scholar] [CrossRef] [Green Version]
- Desgrosellier, J.S.; Cheresh, D.A. Integrins in cancer: Biological implications and therapeutic opportunities. Nat. Rev. Cancer 2010, 10, 9–22. [Google Scholar] [CrossRef] [Green Version]
- Bates, R.C.; Bellovin, D.I.; Brown, C.; Maynard, E.; Wu, B.; Kawakatsu, H.; Sheppard, D.; Oettgen, P.; Mercurio, A.M. Transcriptional activation of integrin beta6 during the epithelial-mesenchymal transition defines a novel prognostic indicator of aggressive colon carcinoma. J. Clin. Investig. 2005, 115, 339–347. [Google Scholar] [CrossRef] [PubMed]
- Boonstra, M.C.; Verbeek, F.P.; Mazar, A.P.; Prevoo, H.A.; Kuppen, P.J.; van de Velde, C.J.; Vahrmeijer, A.L.; Sier, C.F. Expression of uPAR in tumor-associated stromal cells is associated with colorectal cancer patient prognosis: A TMA study. BMC Cancer 2014, 14, 269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sier, C.F.; Quax, P.H.; Vloedgraven, H.J.; Verheijen, J.H.; Griffioen, G.; Ganesh, S.; Lamers, C.B.; Verspaget, H.W. Increased urokinase receptor levels in human gastrointestinal neoplasia and related liver metastases. Invasion Metastasis 1993, 13, 277–288. [Google Scholar]
- Mahmood, N.; Mihalcioiu, C.; Rabbani, S.A. Multifaceted Role of the Urokinase-Type Plasminogen Activator (uPA) and Its Receptor (uPAR): Diagnostic, Prognostic, and Therapeutic Applications. Front. Oncol. 2018, 8, 24. [Google Scholar] [CrossRef] [Green Version]
- Boonstra, M.C.; van Driel, P.B.; van Willigen, D.M.; Stammes, M.A.; Prevoo, H.A.; Tummers, Q.R.; Mazar, A.P.; Beekman, F.J.; Kuppen, P.J.; van de Velde, C.J.; et al. uPAR-targeted multimodal tracer for pre- and intraoperative imaging in cancer surgery. Oncotarget 2015, 6, 14260–14273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christensen, A.; Juhl, K.; Persson, M.; Charabi, B.W.; Mortensen, J.; Kiss, K.; Lelkaitis, G.; Rubek, N.; von Buchwald, C.; Kjaer, A. uPAR-targeted optical near-infrared (NIR) fluorescence imaging and PET for image-guided surgery in head and neck cancer: Proof-of-concept in orthotopic xenograft model. Oncotarget 2017, 8, 15407–15419. [Google Scholar] [CrossRef] [Green Version]
- Skovgaard, D.; Persson, M.; Brandt-Larsen, M.; Christensen, C.; Madsen, J.; Klausen, T.L.; Holm, S.; Andersen, F.L.; Loft, A.; Berthelsen, A.K.; et al. Safety, Dosimetry, and Tumor Detection Ability of (68)Ga-NOTA-AE105: First-in-Human Study of a Novel Radioligand for uPAR PET Imaging. J. Nucl. Med. 2017, 58, 379–386. [Google Scholar] [CrossRef] [Green Version]
- Park, J.W.; Chang, H.J.; Kim, B.C.; Yeo, H.Y.; Kim, D.Y. Clinical validity of tissue carcinoembryonic antigen expression as ancillary to serum carcinoembryonic antigen concentration in patients curatively resected for colorectal cancer. Colorectal Dis. 2013, 15, e503–e511. [Google Scholar] [CrossRef]
- Boogerd, L.S.; van der Valk, M.J.; Boonstra, M.C.; Prevoo, H.A.; Hilling, D.E.; van de Velde, C.J.; Sier, C.F.; Farina Sarasqueta, A.; Vahrmeijer, A.L. Biomarker expression in rectal cancer tissue before and after neoadjuvant therapy. Onco Targets Ther. 2018, 11, 1655–1664. [Google Scholar] [CrossRef] [Green Version]
- Schnittert, J.; Bansal, R.; Storm, G.; Prakash, J. Integrins in wound healing, fibrosis and tumor stroma: High potential targets for therapeutics and drug delivery. Adv. Drug Deliv. Rev. 2018, 129, 37–53. [Google Scholar] [CrossRef]
- De Jongh, S.J.; Voskuil, F.J.; Schmidt, I.; Karrenbeld, A.; Kats-Ugurlu, G.; Meersma, G.J.; Westerhof, J.; Witjes, M.J.H.; van Dam, G.M.; Robinson, D.J.; et al. C-Met targeted fluorescence molecular endoscopy in Barrett’s esophagus patients and identification of outcome parameters for phase-I studies. Theranostics 2020, 10, 5357–5367. [Google Scholar] [CrossRef]
- De Jongh, S.J.; Vrouwe, J.P.M.; Voskuil, F.J.; Schmidt, I.; Westerhof, J.; Koornstra, J.J.; de Kam, M.L.; Karrenbeld, A.; Hardwick, J.C.H.; Robinson, D.J.; et al. The Optimal Imaging Window for Dysplastic Colorectal Polyp Detection Using c-Met-Targeted Fluorescence Molecular Endoscopy. J. Nucl. Med. 2020, 61, 1435–1441. [Google Scholar] [CrossRef] [PubMed]
- Keller, R.; Winde, G.; Terpe, H.J.; Foerster, E.C.; Domschke, W. Fluorescence endoscopy using a fluorescein-labeled monoclonal antibody against carcinoembryonic antigen in patients with colorectal carcinoma and adenoma. Endoscopy 2002, 34, 801–807. [Google Scholar] [CrossRef] [PubMed]
- Mayinger, B.; Neumann, F.; Kastner, C.; Haider, T.; Schwab, D. Hexaminolevulinate-induced fluorescence colonoscopy versus white light endoscopy for diagnosis of neoplastic lesions in the colon. Endoscopy 2010, 42, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Burggraaf, J.; Kamerling, I.M.; Gordon, P.B.; Schrier, L.; de Kam, M.L.; Kales, A.J.; Bendiksen, R.; Indrevoll, B.; Bjerke, R.M.; Moestue, S.A.; et al. Detection of colorectal polyps in humans using an intravenously administered fluorescent peptide targeted against c-Met. Nat. Med. 2015, 21, 955–961. [Google Scholar] [CrossRef] [PubMed]
- Hartmans, E.; Tjalma, J.J.J.; Linssen, M.D.; Allende, P.B.G.; Koller, M.; Jorritsma-Smit, A.; Nery, M.; Elias, S.G.; Karrenbeld, A.; de Vries, E.G.E.; et al. Potential Red-Flag Identification of Colorectal Adenomas with Wide-Field Fluorescence Molecular Endoscopy. Theranostics 2018, 8, 1458–1467. [Google Scholar] [CrossRef] [PubMed]
- Tjalma, J.J.J.; Koller, M.; Linssen, M.D.; Hartmans, E.; de Jongh, S.; Jorritsma-Smit, A.; Karrenbeld, A.; de Vries, E.G.; Kleibeuker, J.H.; Pennings, J.P.; et al. Quantitative fluorescence endoscopy: An innovative endoscopy approach to evaluate neoadjuvant treatment response in locally advanced rectal cancer. Gut 2020, 69, 406–410. [Google Scholar] [CrossRef] [Green Version]
- Buka, D.; Dvorak, J.; Sitorova, V.; Sirak, I.; Voboril, R.; Melichar, B.; Richter, I. The changes of tumour vascular endothelial growth factor expression after neoadjuvant chemoradiation in patients with rectal adenocarcinoma. Contemp. Oncol. 2017, 21, 48–53. [Google Scholar] [CrossRef] [Green Version]
- Habr-Gama, A.; Gama-Rodrigues, J.; Sao Juliao, G.P.; Proscurshim, I.; Sabbagh, C.; Lynn, P.B.; Perez, R.O. Local recurrence after complete clinical response and watch and wait in rectal cancer after neoadjuvant chemoradiation: Impact of salvage therapy on local disease control. Int. J. Radiat. Oncol. Biol. Phys. 2014, 88, 822–828. [Google Scholar] [CrossRef] [PubMed]
- Keereweer, S.; Van Driel, P.B.; Snoeks, T.J.; Kerrebijn, J.D.; Baatenburg de Jong, R.J.; Vahrmeijer, A.L.; Sterenborg, H.J.; Lowik, C.W. Optical image-guided cancer surgery: Challenges and limitations. Clin. Cancer Res. 2013, 19, 3745–3754. [Google Scholar] [CrossRef] [Green Version]





| Biopsy and Resection (n = 15) | Only Resection (n = 29) | All (n = 44) | |
|---|---|---|---|
| Age at surgery, median years (range) | 71 (48–88) | 61 (28–78) | 66 (28–88) |
| Gender | |||
| Male | 10 | 13 | 23 |
| Female | 5 | 16 | 21 |
| Tumor type | |||
| Adenocarcinoma | 14 | 24 | 38 |
| Tubulovillous adenoma with dysplasia | 1 | 1 | 2 |
| Unknown | 0 | 4 | 4 |
| Tumor size, median cm (range) | 5 (3–12) | 5 (2–15) | 5 (2–15) |
| Type of neoadjuvant therapy | |||
| 25 × 2 Gy + capecitabine | 12 | 24 | 36 |
| 5 × 5 Gy | 2 | 2 | 4 |
| 5 × 5 Gy + capecitabine, oxaliplatin, bevacizumab | 0 | 2 | 2 |
| 5 × 5 Gy + capecitabine, oxaliplatin | 1 | 1 | 2 |
| Type of surgery | |||
| Low anterior resection | 7 | 15 | 22 |
| Abdominoperineal resection | 6 | 12 | 18 |
| Transanal endoscopic microsurgery | 1 | 2 | 3 |
| Hartmann’s procedure | 1 | 0 | 1 |
| Clinical stage | |||
| Tumor stage, n | |||
| cTx | 5 | 7 | 12 |
| cT2 | 2 | 1 | 3 |
| cT3 | 7 | 9 | 16 |
| cT4 | 1 | 12 | 13 |
| Nodal stage, n | |||
| cNx | 5 | 7 | 12 |
| cN0 | 2 | 5 | 7 |
| cN1 | 5 | 3 | 8 |
| cN2 | 3 | 14 | 17 |
| Metastatic stage, n | |||
| cMx | 6 | 7 | 13 |
| cM0 | 9 | 20 | 29 |
| cM1 | 0 | 2 | 2 |
| Pathologic stage | |||
| Tumor stage, n | |||
| pT0 | 15 | 29 | 44 |
| Nodal stage, n | |||
| pN0 | 14 | 29 | 43 |
| pN1 | 1 | 0 | 1 |
| Metastatic stage, n | |||
| pM0 | 15 | 27 | 42 |
| pM1 | 0 | 2 | 2 |
| Time between neoadjuvant therapy and surgery, median weeks (range) | 11 (6–57) |
| Total Immunostaining Score (TIS) on Biopsy, pCR Tumor Bed, and Pre-Existent Rectal Mucosa n (%) | |||||
|---|---|---|---|---|---|
| Expression TIS | No 0 | Weak 1–5 | Moderate 6–8 | Intense 9–12 | Total Tissues |
| CEA | |||||
| Biopsy | 0 (0%) | 0 (0%) | 0 (0%) | 15 (100%) | 15 |
| Tumor bed | 30 (75%) | 7 (18%) | 0 (0%) | 3 (7%) | 40 |
| Pre-existent rectal mucosa | 2 (5%) | 6 (15%) | 10 (25%) | 22 (55%) | 40 |
| EpCAM | |||||
| Biopsy | 0 (0%) | 0 (0%) | 1 (7%) | 14 (93%) | 15 |
| Tumor bed | 33 (85%) | 4 (10%) | 0 (0%) | 2 (5%) | 39 |
| Pre-existent rectal mucosa | 1 (2.5%) | 1 (2.5%) | 0 (0%) | 39 (95%) | 41 |
| αvβ6 | |||||
| Biopsy | 4 (27%) | 6 (40%) | 4 (27%) | 1 (6%) | 15 |
| Tumor bed | 28 (70%) | 6 (15%) | 2 (5%) | 4 (10%) | 40 |
| Pre-existent rectal mucosa | 1 (3%) | 19 (45%) | 11 (26%) | 11 (26%) | 42 |
| uPAR | |||||
| Biopsy | 0 (0%) | 7 (54%) | 3 (23%) | 3 (23%) | 13 |
| Tumor bed | 5 (12.5%) | 20 (50%) | 8 (20%) | 7 (17.5%) | 40 |
| Pre-existent rectal mucosa | 10 (24%) | 30 (73%) | 0 (0%) | 1 (3%) | 41 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Linders, D.; Deken, M.; van der Valk, M.; Tummers, W.; Bhairosingh, S.; Schaap, D.; van Lijnschoten, G.; Zonoobi, E.; Kuppen, P.; van de Velde, C.; et al. CEA, EpCAM, αvβ6 and uPAR Expression in Rectal Cancer Patients with a Pathological Complete Response after Neoadjuvant Therapy. Diagnostics 2021, 11, 516. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11030516
Linders D, Deken M, van der Valk M, Tummers W, Bhairosingh S, Schaap D, van Lijnschoten G, Zonoobi E, Kuppen P, van de Velde C, et al. CEA, EpCAM, αvβ6 and uPAR Expression in Rectal Cancer Patients with a Pathological Complete Response after Neoadjuvant Therapy. Diagnostics. 2021; 11(3):516. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11030516
Chicago/Turabian StyleLinders, Daan, Marion Deken, Maxime van der Valk, Willemieke Tummers, Shadhvi Bhairosingh, Dennis Schaap, Gesina van Lijnschoten, Elham Zonoobi, Peter Kuppen, Cornelis van de Velde, and et al. 2021. "CEA, EpCAM, αvβ6 and uPAR Expression in Rectal Cancer Patients with a Pathological Complete Response after Neoadjuvant Therapy" Diagnostics 11, no. 3: 516. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11030516