
The Evaluation of Left Ventricle Ischemic Extent in Patients with Significantly Suspicious Cardiovascular Disease by 99mTc-Sestamibi Dynamic SPECT/CT and Myocardial Perfusion Imaging: A Head-to-Head Comparison

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
- ➢
- Excluded caffeine intake before study—three patients.
- ➢
- Excluded not done PCI—10 patients
- ➢
- Excluded PCI done at other hospital—one patient
- ➢
- There were 167 patients for data analysis.
2.2. Dynamic SPECT/CT Imaging
2.3. Image Evaluation
2.4. Cardiac Catheterization
2.5. Statistical Analysis
3. Results
3.1. Overall Population
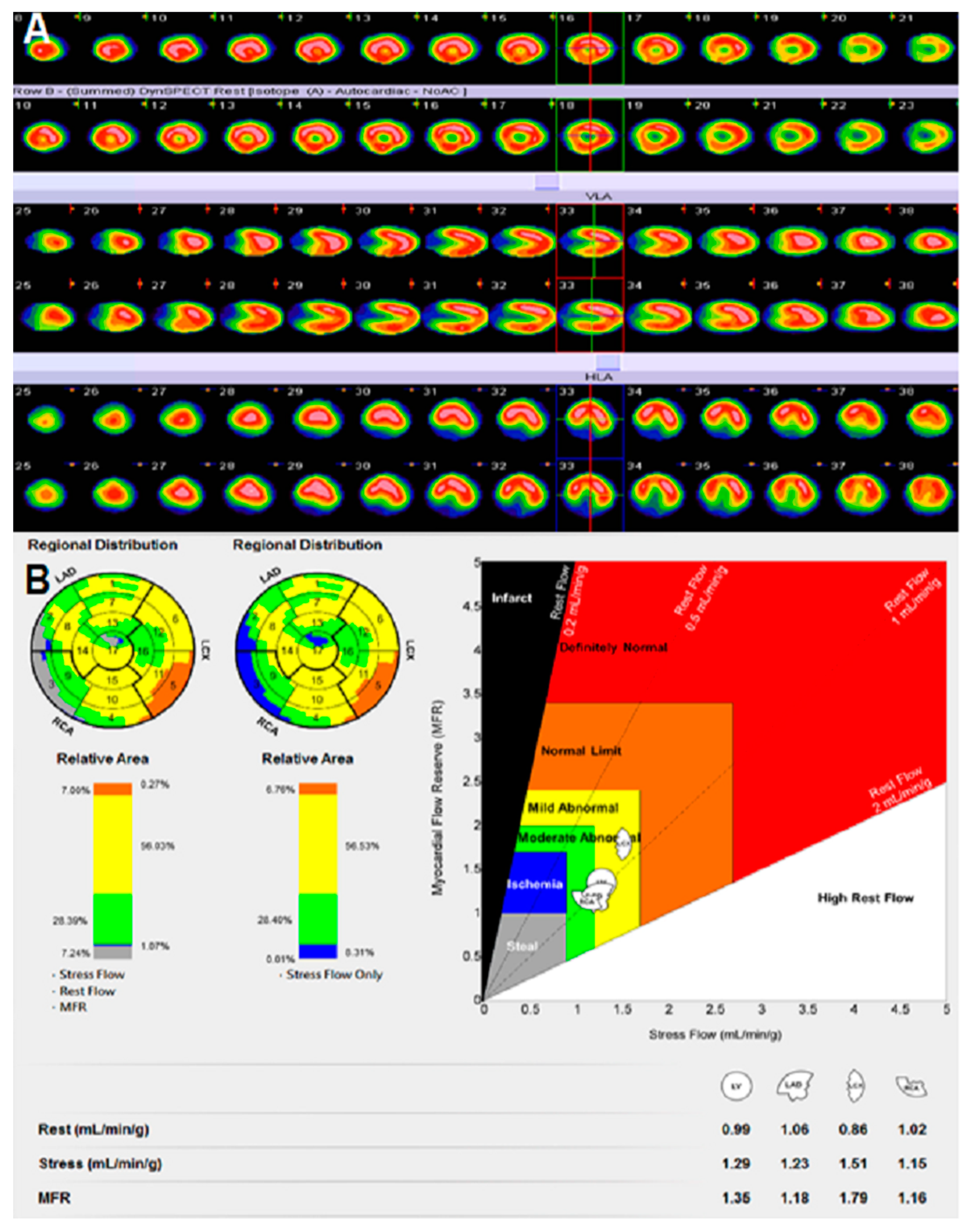
3.2. The Analysis of Semi-Quantitative MPI and Quantitative Dynamic SPECT/CT
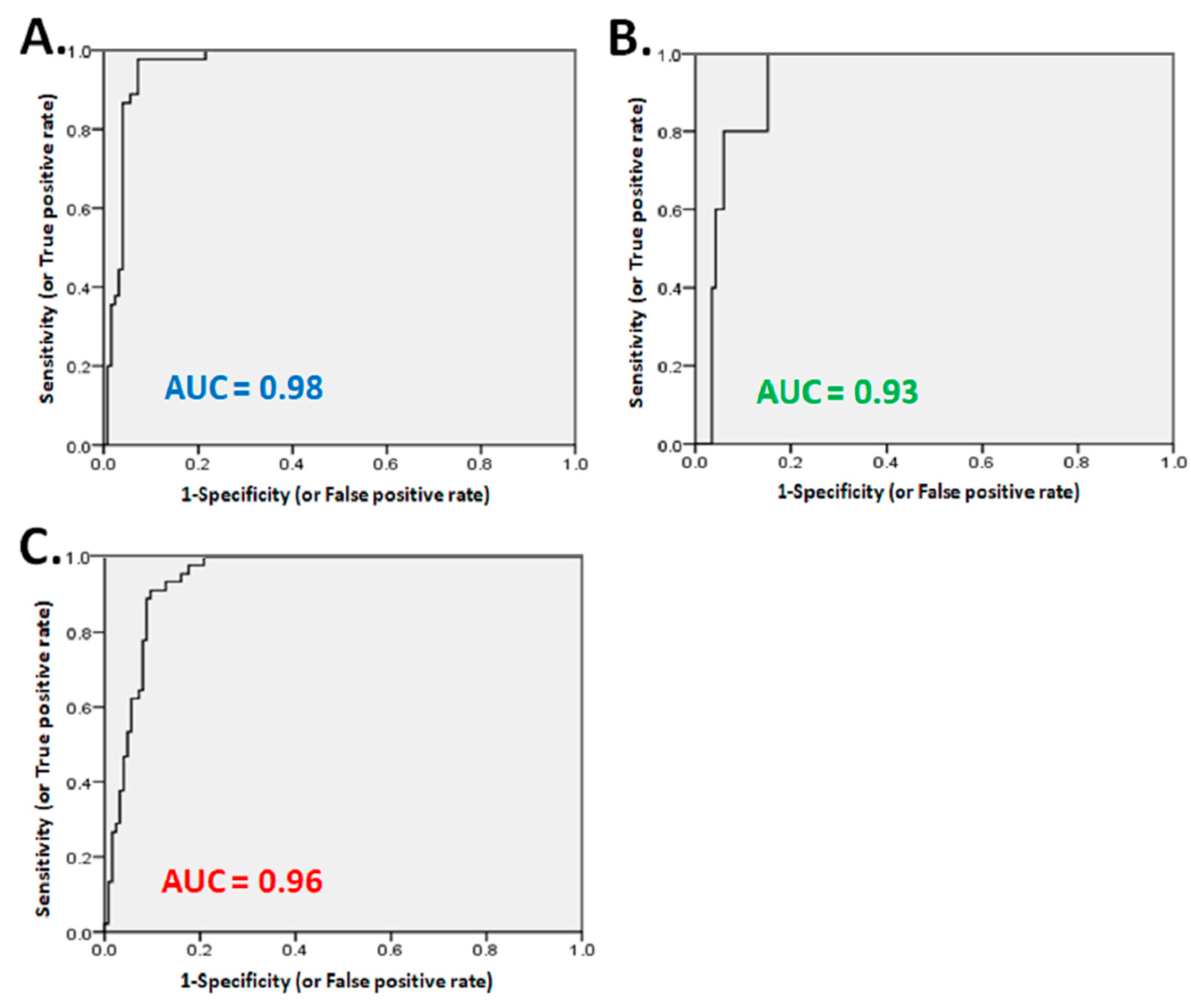
3.3. The Relationship of Semi-Quantitative MPI with Cardiac Catheterization
3.4. The Relationship of Dynamic SPECT/CT with Cardiac Catheterization
3.5. The Evaluation of Ischemic Extent, Moderate Abnormal Perfusion, or Combined Ischemic with Moderate Abnormal Perfusion of LV Myocardium in Dynamic SPECT/CT According to PCI Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shao, C.; Wang, J.; Tian, J.; Tang, Y.D. Coronary artery disease: From mechanism to clinical practice. Adv. Exp. Med. Biol. 2020, 1177, 1–36. [Google Scholar]
- Finn, A.V.; Nakano, M.; Narula, J.; Kolodgie, F.D.; Virmani, R. Concept of vulnerable/unstable plaque. Arter. Thromb. Vasc. Biol. 2010, 30, 1282–1292. [Google Scholar] [CrossRef] [Green Version]
- Baqi, A.; Ahmed, I.; Nagher, B. Multi vessel coronary artery disease presenting as a false negative myocardial perfusion imaging and true positive exercise tolerance test: A case of balanced ischemia. Cureus 2020, 12, e11321. [Google Scholar]
- Harisankar, C.; Mittal, B.R.; Kamaleshwaran, K.; Bhattacharya, A.; Singh, B.; Mahajan, R. Role of myocardial perfusion scintigraphy post invasive coronary angiography in patients with Myocardial Infarction. Indian J. Nucl. Med. 2010, 25, 53–56. [Google Scholar] [PubMed]
- Dilsizian, V.; Panza, J.A.; Bonow, R.O. Myocardial perfusion imaging in hypertrophic cardiomyopathy. JACC Cardiovasc. Imaging 2010, 3, 1078–1080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van de Hoef, T.P.; Echavarría-Pinto, M.; Escaned, J.; Piek, J.J. Coronary flow capacity: Concept, promises, and challenges. Int. J. Cardiovasc. Imaging 2017, 33, 1033–1039. [Google Scholar] [CrossRef] [Green Version]
- Murthy, V.L.; Naya, M.; Foster, C.R.; Hainer, J.; Gaber, M.; Di Carli, G.; Blankstein, R.; Dorbala, S.; Sitek, A.; Pencina, M.J.; et al. Improved cardiac risk assessment with noninvasive measures of coronary flow reserve. Circulation 2011, 124, 2215–2224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gould, K.L.; Johnson, N.P.; Roby, A.E.; Nguyen, T.; Kirkeeide, R.; Haynie, M.; Lai, D.; Zhu, H.; Patel, M.B.; Smalling, R.; et al. Regional artery specific thresholds of quantitative myocardial perfusion by PET associated with reduced MI and death after revascularization in stable CAD. J. Nucl. Med. 2018, 60, 410–417. [Google Scholar] [CrossRef]
- Gould, K.L.; Johnson, N.P. Coronary physiology: Beyond CFR in microvascular angina. J. Am. Coll Cardiol. 2018, 72, 2642–2662. [Google Scholar] [CrossRef] [PubMed]
- Hsu, B.; Chen, F.C.; Wu, T.C.; Huang, W.S.; Hou, P.N.; Chen, C.C.; Hung, G.U. Quantitation of myocardial blood flow and myocardial flow reserve with Tc-99m sestamibi dynamic SPECT/CT to enhance detection of coronary artery disease. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 2294–2306. [Google Scholar] [CrossRef]
- Hudson, H.M.; Larkin, R.S. Accelerated image reconstruction using ordered subsets of projection. IEEE Trans. Med. Imaging 1994, 13, 601–609. [Google Scholar] [CrossRef] [Green Version]
- Graf, S.; Khorsand, A.; Gwechenberger, M.; Novotny, C.; Kletter, K.; Sochor, H.; Pirich, C.; Maurer, G.; Porenta, G.; Zehetgruber, M. Typical chest pain and normal coronary angiogram: Cardiac risk factor analysis versus PET for detection of microvascular disease. J. Nucl. Med. 2007, 48, 175–181. [Google Scholar] [PubMed]
- Muzik, O.; Shen, C.; DiCurli, M. IDL software package for absolute quantification of myocardial blood Row based on (N-13) ammonia PET data. In Proceedings of the 25th Annual Meeting of Computers in Cardiology, Cleveland, OH, USA, 13–16 September 1998; IEEE Computer Society Press: Piscataway, NJ, USA, 1996; Volume 25, pp. 33–36. [Google Scholar]
- Hutchins, G.D.; Schwaiger, M.; Rosenspire, K.C.; Krivokapich, J.; Schelbert, H.; Kuhl, D.E. Noninvasive quantification of regional blood flow in the human heart using N-13 ammonia anil dynamic positron emission tomographic imaging. J. Am. Coll Cardiol. 1990, 15, 1032–1042. [Google Scholar] [CrossRef] [Green Version]
- Hutchins, G.D.; Caraher, J.M.; Raylman, R.R. A region of interest strategy for minimizing resolution distortions in quantitative myocordial PET studies. J. Nucl. Med. 1992, 13, 1243–1250. [Google Scholar]
- Graf, S.; Khorsand, A.; Gwechenberger, M.; Schütz, M.; Kletter, K.; Sochor, H.; Dudczak, R.; Maurer, G.; Pirich, C.; Porenta, G.; et al. Myociirdial perfusion in patients with typical chest pain and normal angiogmm. Eur. J. Clin. Investig. 2006, 36, 326–332. [Google Scholar] [CrossRef]
- Kubo, S.; Tadamura, E.; Toyoda, H.; Mamede, M.; Yamamuro, M.; Magata, Y.; Mukai, T.; Kitano, H.; Tamaki, N.; Konishi, J. Effect of caffeine intake on myocardial hyperemic flow induced by adenosine triphosphate and dipyridamole. J. Nucl. Med. 2004, 45, 730–738. [Google Scholar]
- Böttcher, M.; Czernin, J.; Sun, K.T.; Phelps, M.E.; Schelbert, H.R. Effect of caffeine on myocardial blood flow at rest and during pharmacological vasodilation. J. Nucl. Med. 1995, 11, 2016–2021. [Google Scholar]
- Berman, D.S.; Kang, X.; Slomka, P.J.; Gerlach, J.; de Yang, L.; Hayes, S.W.; Friedman, J.D.; Thomson, L.E.; Germano, G. Underestimation of extent of ischemia by gated SPECT myocardial perfusion imaging in patients with left main coronary artery disease. J. Nucl. Cardiol. 2007, 14, 521–528. [Google Scholar] [CrossRef]
- Schepis, T.; Benz, K.; Haldemann, A.; Kaufmann, P.A.; Schmidhauser, C.; Frielingsdorf, J. Prognostic value of stress-gated 99m-technetium SPECT myocardial perfusion imaging: Risk stratification of patients with multivessel coronary artery disease and prior coronary revascularization. J. Nucl. Cardiol. 2013, 20, 755–762. [Google Scholar] [CrossRef]
- Kang, S.H.; Choi, H.I.; Kim, T.H.; Lee, E.Y.; Ahn, J.M.; Han, S.; Lee, P.H.; Roh, J.H.; Yun, S.H.; Park, W.; et al. Impact of follow-up ischemia on myocardial perfusion single-photon emission computed tomography in patients with coronary artery disease. Yonsei Med. J. 2017, 58, 934–943. [Google Scholar] [CrossRef]
- Burrell, S.; MacDonald, A. Artifacts and pitfalls in myocardial perfusion imaging. J. Nucl. Med. Technol. 2006, 34, 193–211. [Google Scholar] [PubMed]
- Johnson, N.P.; Gould, K.L. Integrating noninvasive absolute flow, coronary flow reserve, and ischemic thresholds into a comprehensive map of physiological severity. JACC Cardiovasc. Imaging 2012, 5, 430–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fiechter, M.; Ghadri, J.R.; Gebhard, C.; Fuchs, T.A.; Pazhenkottil, A.P.; Nkoulou, R.N.; Herzog, B.A.; Wyss, C.A.; Gaemperli, O.; Kaufmann, P.A. Diagnostic value of 13N-ammonia myocardial perfusion PET: Added value of myocardial flow reserve. J. Nucl. Med. 2012, 53, 1230–1234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ziadi, M.C.; Dekemp, R.A.; Williams, K.; Guo, A.; Renaud, J.M.; Chow, B.J.; Klein, R.; Ruddy, T.D.; Aung, M.; Garrard, L.; et al. Does quantification of myocardial flow reserve using rubidium-82 positron emission tomography facilitate detection of multivessel coronary artery disease? J. Nucl. Cardiol. 2012, 19, 670–680. [Google Scholar] [CrossRef] [PubMed]
- Gould, K.L.; Kitkungvan, D.; Johnson, N.P.; Nguyen, T.; Kirkeeide, R.; Bui, L.; Patel, M.B.; Roby, A.E.; Madjid, M.; Zhu, H.; et al. Mortality prediction by quantitative PET perfusion expressed as coronary flow capacity with and without revascularization. JACC Cardiovasc. Imaging 2021, 14, 1020–1034. [Google Scholar] [CrossRef] [PubMed]
- Agostini, D.; Roule, V.; Nganoa, C.; Roth, N.; Baavour, R.; Parienti, J.J.; Beygui, F.; Manrique, A. First validation of myocardial flow reserve assessed by dynamic 99mTc-sestamibi CZT-SPECT camera: Head to head comparison with 15O-water PET and fractional flow reserve in patients with suspected coronary artery disease. The WATERDAY study. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 1079–1090. [Google Scholar] [CrossRef] [Green Version]
- Hachamovitch, R.; Hayes, S.W.; Friedman, J.D.; Cohen, I.; Berman, D.S. Comparison of the short-term survival benefit associated with revascularization compared with medical therapy in patients with no prior coronary artery disease undergoing stress myocardial perfusion single photon emission computed tomography. Circulation 2003, 107, 2900–2907. [Google Scholar] [CrossRef] [Green Version]
- Green, R.; Cantoni, V.; Acampa, W.; Assante, R.; Zampella, E.; Nappi, C.; Gaudieri, V.; Mannarino, T.; Cuocolo, R.; Petretta, M.; et al. Prognostic value of coronary flow reserve in patients with suspected or known coronary artery disease referred to PET myocardial perfusion imaging: A meta-analysis. J. Nucl. Cardiol. 2019, 26, 826–838. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Age (Year) (Mean ± SD) | 68.5 ± 7.2 |
|---|---|
| Gender | |
| Male | 99 |
| Female | 82 |
| Smoking (Y/N) | 32/149 (19%/81%) |
| Alcohol consumption (Y/N) | 10/171 (1%/99%) |
| Caffeine consumption (Y/N) | 72/109 (40%/60%) |
| Tea consumption (Y/N) | 56/125 (31%/69%) |
| HTN(Y/N) | 154/27 (85%/15%) |
| DM(Y/N) | 113/68 (62%/38%) |
| Hyperlipidemia (Y/N) | 91/90 (50%/50%) |
| MIBI MPI | Total (N) | |||
|---|---|---|---|---|
| No Ischemia | Had Ischemia | |||
| Cardiac Catheterization | Normal | 99 | 26 | 125 |
| Abnormal | 15 | 27 | 42 | |
| Total (N) | 114 | 53 | 167 | |
| Dynamic SPECT/CT (Ischemic Extent of LV) | Total (N) | |||
|---|---|---|---|---|
| <8% | ≥8% | |||
| Cardiac Catheterization | Normal | 120 | 5 | 125 |
| Abnormal | 5 | 37 | 42 | |
| Total (N) | 125 | 42 | 167 | |
| Normal Group (n = 125) | CAD Group (n = 42) | p Value | |
|---|---|---|---|
| LV-CFR | 2.6 ± 0.8 | 1.5 ± 0.4 | <0.01 |
| LV-stress flow (mL/min/g) | 2.2 ± 0.8 | 1.3 ± 0.3 | <0.01 |
| LV-rest flow (mL/min/g) | 1.04 ± 0.2 | 1.1 ± 0.2 | 0.058 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chan, H.-P.; Chang, C.-C.; Hu, C.; Wang, W.-H.; Peng, N.-J.; Tyan, Y.-C.; Yang, M.-H. The Evaluation of Left Ventricle Ischemic Extent in Patients with Significantly Suspicious Cardiovascular Disease by 99mTc-Sestamibi Dynamic SPECT/CT and Myocardial Perfusion Imaging: A Head-to-Head Comparison. Diagnostics 2021, 11, 1101. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11061101
Chan H-P, Chang C-C, Hu C, Wang W-H, Peng N-J, Tyan Y-C, Yang M-H. The Evaluation of Left Ventricle Ischemic Extent in Patients with Significantly Suspicious Cardiovascular Disease by 99mTc-Sestamibi Dynamic SPECT/CT and Myocardial Perfusion Imaging: A Head-to-Head Comparison. Diagnostics. 2021; 11(6):1101. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11061101
Chicago/Turabian StyleChan, Hung-Pin, Chin-Chuan Chang, Chin Hu, Wen-Hwa Wang, Nan-Jing Peng, Yu-Chang Tyan, and Ming-Hui Yang. 2021. "The Evaluation of Left Ventricle Ischemic Extent in Patients with Significantly Suspicious Cardiovascular Disease by 99mTc-Sestamibi Dynamic SPECT/CT and Myocardial Perfusion Imaging: A Head-to-Head Comparison" Diagnostics 11, no. 6: 1101. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11061101