
Serum Peptide Immunoglobulin G Autoantibody Response in Patients with Different Central Nervous System Inflammatory Demyelinating Disorders

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Samples
2.2. Peptide Microarray Design
2.3. Microarray Staining and Reading
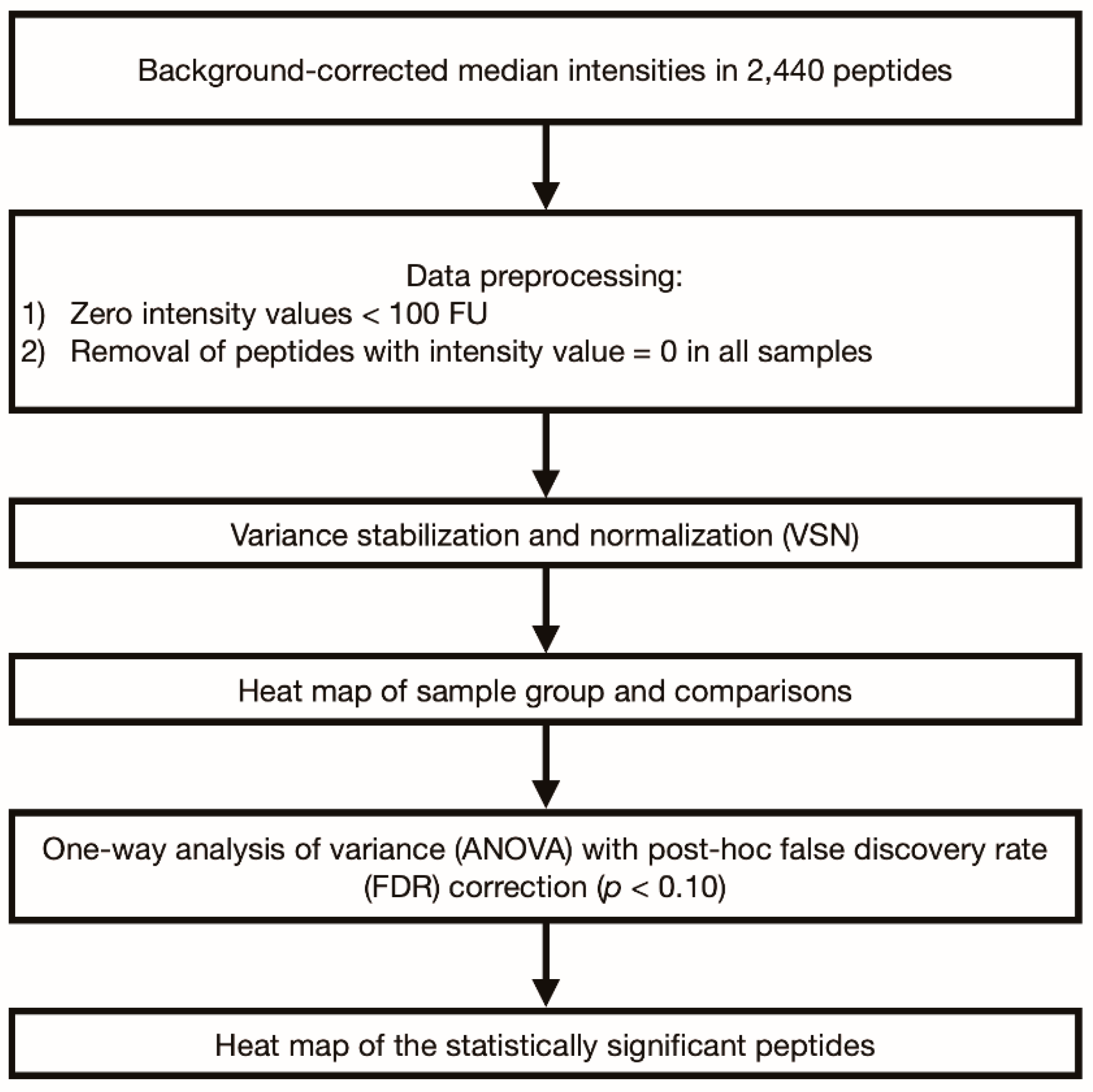
2.4. Statistical Analysis
3. Results
3.1. Participant Demographics and Clinical Data
3.2. Analysis of IgG Autoantibody Responses of Each Disease Group Compared to the HC Group
3.3. Analysis of IgG Autoantibody Responses among the Disease Groups
3.3.1. Comparison between MS and Seropositive NMOSD
3.3.2. Comparison between MS and Seronegative NMOSD
3.3.3. Comparison between Seropositive NMOSD and Seronegative NMOSD
3.3.4. Comparison between Each Disease Group and MOGAD
3.4. Heatmap of IgG Autoantibody Responses among the Disease and Control Groups
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Juryńczyk, M.; Craner, M.; Palace, J. Overlapping CNS inflammatory diseases: Differentiating features of NMO and MS. J. Neurol. Neurosurg. Psychiatry 2015, 86, 20–25. [Google Scholar] [CrossRef]
- Jarius, S.; Ruprecht, K.; Wildemann, B.; Kuempfel, T.; Ringelstein, M.; Geis, C.; Kleiter, I.; Kleinschnitz, C.; Berthele, A.; Brettschneider, J. Contrasting disease patterns in seropositive and seronegative neuromyelitis optica: A multicentre study of 175 patients. J. Neuroinflamm. 2012, 9, 14. [Google Scholar] [CrossRef]
- Lennon, V.A.; Wingerchuk, D.M.; Kryzer, T.J.; Pittock, S.J.; Lucchinetti, C.F.; Fujihara, K.; Nakashima, I.; Weinshenker, B.G. A serum autoantibody marker of neuromyelitis optica: Distinction from multiple sclerosis. Lancet 2004, 364, 2106–2112. [Google Scholar] [CrossRef]
- Kim, W.; Kim, S.H.; Kim, H.J. New insights into neuromyelitis optica. J. Clin. Neurol. 2011, 7, 115–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koike, H.; Katsuno, M. Macrophages and Autoantibodies in Demyelinating Diseases. Cells 2021, 10, 844. [Google Scholar] [CrossRef]
- Wynford-Thomas, R.; Jacob, A.; Tomassini, V. Neurological update: MOG antibody disease. J. Neurol. 2019, 266, 1280–1286. [Google Scholar] [CrossRef] [Green Version]
- Yoo, I.H.; Kim, W.; Shim, Y.; Choi, S.A.; Kim, S.Y.; Kim, H.; Lim, B.C.; Hwang, H.; Choi, J.; Kim, K.J.; et al. Clinical Spectrum of Myelin Oligodendrocyte Glycoprotein-Immunoglobulin G-Associated Disease in Korean Children. J. Clin. Neurol. 2020, 16, 461–469. [Google Scholar] [CrossRef] [PubMed]
- Cusick, M.F.; Libbey, J.E.; Fujinami, R.S. Multiple sclerosis: Autoimmunity and viruses. Curr. Opin. Rheumatol. 2013, 25, 496–501. [Google Scholar] [CrossRef] [Green Version]
- Marrodan, M.; Alessandro, L.; Farez, M.F.; Correale, J. The role of infections in multiple sclerosis. Mult. Scler. 2019, 25, 891–901. [Google Scholar] [CrossRef] [PubMed]
- Metz, I.; Beißbarth, T.; Ellenberger, D.; Pache, F.; Stork, L.; Ringelstein, M.; Aktas, O.; Jarius, S.; Wildemann, B.; Dihazi, H.; et al. Serum peptide reactivities may distinguish neuromyelitis optica subgroups and multiple sclerosis. Neurol. Neuroimmunol. Neuroinflamm. 2016, 3, e204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sospedra, M.; Martin, R. Immunology of multiple sclerosis. Annu. Rev. Immunol. 2005, 23, 683–747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cornaby, C.; Gibbons, L.; Mayhew, V.; Sloan, C.S.; Welling, A.; Poole, B.D. B cell epitope spreading: Mechanisms and contribution to autoimmune diseases. Immunol. Lett. 2015, 163, 56–68. [Google Scholar] [CrossRef]
- Rudge, P. Does a retrovirally encoded superantigen cause multiple sclerosis? J. Neurol. Neurosurg. Psychiatry 1991, 54, 853–855. [Google Scholar] [CrossRef] [Green Version]
- Mohammadi-Milasi, F.; Mahnam, K.; Shakhsi-Niaei, M. In silico study of the association of the HLA-A*31:01 allele (human leucocyte antigen allele 31:01) with neuroantigenic epitopes of PLP (proteolipid protein), MBP (myelin basic protein) and MOG proteins (myelin oligodendrocyte glycoprotein) for studying the multiple sclerosis disease pathogenesis. J. Biomol. Struct. Dyn. 2020, 39, 2526–2542. [Google Scholar] [CrossRef]
- Saravani, M.; Rokni, M.; Mehrbani, M.; Amirkhosravi, A.; Faramarz, S.; Fatemi, I.; Tarzi, M.E.; Nematollahi, M.H. The evaluation of VEGF and HIF-1α gene polymorphisms and multiple sclerosis susceptibility. J. Gene Med. 2019, 21, e3132. [Google Scholar] [CrossRef]
- Lee, H.L.; Seok, J.M.; Kim, J.-H.; Kim, H.J.; Kim, S.-H.; Ha-Young, S.; Kim, B.-J.; Baek, S.-H.; Sun-Young, K.S. Multi-center Network of Multiple Sclerosis and Neuromyelitis Optical Spectrum Disorder in Korea: Results of the First Year Research. J. Mult. Scler. 2019, 10, 1–6. [Google Scholar]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef]
- Hecker, M.; Fitzner, B.; Wendt, M.; Lorenz, P.; Flechtner, K.; Steinbeck, F.; Schröder, I.; Thiesen, H.-J.; Zettl, U.K. High-density peptide microarray analysis of IgG autoantibody reactivities in serum and cerebrospinal fluid of multiple sclerosis patients. Mol. Cell. Proteom. 2016, 15, 1360–1380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Haren, K.; Tomooka, B.H.; Kidd, B.A.; Banwell, B.; Bar-Or, A.; Chitnis, T.; Tenembaum, S.N.; Pohl, D.; Rostasy, K.; Dale, R.C. Serum autoantibodies to myelin peptides distinguish acute disseminated encephalomyelitis from relapsing–remitting multiple sclerosis. Mult. Scler. J. 2013, 19, 1726–1733. [Google Scholar] [CrossRef] [PubMed]
- Melamed, E.; Levy, M.; Waters, P.J.; Sato, D.K.; Bennett, J.L.; John, G.R.; Hooper, D.C.; Saiz, A.; Bar-Or, A.; Kim, H.J. Update on biomarkers in neuromyelitis optica. Neurol. Neuroimmunol. Neuroinflamm. 2015, 2, e134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quintana, F.; Farez, M.; Izquierdo, G.; Lucas, M.; Cohen, I.; Weiner, H. Antigen microarrays identify CNS-produced autoantibodies in RRMS. Neurology 2012, 78, 532–539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlemm, L.; Giess, R.M.; Rasche, L.; Pfuhl, C.; Wakonig, K.; Behrens, J.R.; Scheibenbogen, C.; Bellmann-Strobl, J.; Paul, F.; Reimer, U. Fine specificity of the antibody response to Epstein-Barr nuclear antigen-2 and other Epstein-Barr virus proteins in patients with clinically isolated syndrome: A peptide microarray-based case-control study. J. Neuroimmunol. 2016, 297, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Bai, S.; Liu, S.; Guo, X.; Qin, Z.; Wang, B.; Li, X.; Qin, Y. Proteome analysis of haptoglobin in cerebrospinal fluid of neuromyelitis optica. Mol. Biol. Rep. 2010, 37, 1619–1625. [Google Scholar] [CrossRef]
- Huber, W.; von Heydebreck, A.; Sültmann, H.; Poustka, A.; Vingron, M. Variance stabilization applied to microarray data calibration and to the quantification of differential expression. Bioinformatics 2002, 18, S96–S104. [Google Scholar] [CrossRef]
- Putterman, C.; Wu, A.; Reiner-Benaim, A.; Batty, D.S., Jr.; Sanz, I.; Oates, J.; Jakobi, K.; Petri, M.; Safer, P.; Gerwien, R. SLE-key® rule-out serologic test for excluding the diagnosis of systemic lupus erythematosus: Developing the ImmunArray iCHIP®. J. Immunol. Methods 2016, 429, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Ristori, G.; Mechelli, R.; Anderson, J.; Mengoni, F.; Sauzullo, I.; Annibali, V.; Cannoni, S.; Aloisi, F.; James, J.A.; Salvetti, M. Antiviral immune response in patients with multiple sclerosis, healthy siblings and twins. Mult. Scler. J. 2010, 16, 1527. [Google Scholar] [CrossRef]
- Dreyfus, D.H.; Farina, A.; Farina, G.A. Molecular mimicry, genetic homology, and gene sharing proteomic “molecular fingerprints” using an EBV (Epstein-Barr virus)-derived microarray as a potential diagnostic method in autoimmune disease. Immunol. Res. 2018, 66, 686–695. [Google Scholar] [CrossRef] [Green Version]
- Vanheusden, M.; Stinissen, P.; Hart, B.A.; Hellings, N. Cytomegalovirus: A culprit or protector in multiple sclerosis? Trends Mol. Med. 2015, 21, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Sundqvist, E.; Bergström, T.; Daialhosein, H.; Nyström, M.; Sundström, P.; Hillert, J.; Alfredsson, L.; Kockum, I.; Olsson, T. Cytomegalovirus seropositivity is negatively associated with multiple sclerosis. Mult. Scler. J. 2014, 20, 165–173. [Google Scholar] [CrossRef]
- Langer-Gould, A.; Wu, J.; Lucas, R.; Smith, J.; Gonzales, E.; Amezcua, L.; Haraszti, S.; Chen, L.H.; Quach, H.; James, J.A. Epstein-Barr virus, cytomegalovirus, and multiple sclerosis susceptibility: A multiethnic study. Neurology 2017, 89, 1330–1337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanadgol, N.; Ramroodi, N.; Ahmadi, G.A.; Komijani, M.; Moghtaderi, A.; Bouzari, M.; Rezaei, M.; Kardi, M.T.; Dabiri, S.; Moradi, M. Prevalence of cytomegalovirus infection and its role in total immunoglobulin pattern in Iranian patients with different subtypes of multiple sclerosis. Microbiol. Q. J. Microbiol. Sci. 2011, 34, 263. [Google Scholar]
- Sawai, S.; Satoh, M.; Mori, M.; Misawa, S.; Sogawa, K.; Kazami, T.; Ishibashi, M.; Beppu, M.; Shibuya, K.; Ishige, T.; et al. Moesin is a possible target molecule for cytomegalovirus-related Guillain-Barré syndrome. Neurology 2014, 83, 113–117. [Google Scholar] [CrossRef]
- Koike, H.; Fukami, Y.; Nishi, R.; Kawagashira, Y.; Iijima, M.; Katsuno, M.; Sobue, G. Ultrastructural mechanisms of macrophage-induced demyelination in Guillain-Barré syndrome. J. Neurol. Neurosurg. Psychiatry 2020, 91, 650–659. [Google Scholar] [CrossRef]
- Luo, J.; Shi, X.; Lin, Y.; Cheng, N.; Shi, Y.; Wang, Y.; Wu, B.Q. Cytomegalovirus Infection in an Adult Patient with Neuromyelitis Optica and Acute Hemorrhagic Rectal Ulcer: Case Report and Literature Review. Front. Immunol. 2020, 11, 1634. [Google Scholar] [CrossRef]
- Tran, C.; Du Pasquier, R.A.; Cavassini, M.; Guex-Crosier, Y.; Meuli, R.; Ciuffreda, D.; Waeber, G. Neuromyelitis optica following CMV primo-infection. J. Intern. Med. 2007, 261, 500–503. [Google Scholar] [CrossRef]
- Cannon, M.J.; Schmid, D.S.; Hyde, T.B. Review of cytomegalovirus seroprevalence and demographic characteristics associated with infection. Rev. Med. Virol. 2010, 20, 202–213. [Google Scholar] [CrossRef]
- Quintana, F.J.; Patel, B.; Yeste, A.; Nyirenda, M.; Kenison, J.; Rahbari, R.; Fetco, D.; Hussain, M.; O’Mahony, J.; Magalhaes, S. Epitope spreading as an early pathogenic event in pediatric multiple sclerosis. Neurology 2014, 83, 2219–2226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quintana, F.J.; Farez, M.F.; Viglietta, V.; Iglesias, A.H.; Merbl, Y.; Izquierdo, G.; Lucas, M.; Basso, A.S.; Khoury, S.J.; Lucchinetti, C.F. Antigen microarrays identify unique serum autoantibody signatures in clinical and pathologic subtypes of multiple sclerosis. Proc. Natl. Acad. Sci. USA 2008, 105, 18889–18894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, S.H.; Lee, Y.A.; Moon, W.Y.; Ko, T.S.; Park, Y.S.; Moon, H.N.; Hong, C.Y.; Kim, D.W. Prevalence of Epstein-Barr virus (EBV) antibody in Korean children. J. Korean Pediatr. Soc. 1994, 37, 804–811. [Google Scholar]
- Christensen, T. Association of human endogenous retroviruses with multiple sclerosis and possible interactions with herpes viruses. Rev. Med. Virol. 2005, 15, 179–211. [Google Scholar] [CrossRef]
- Hawkes, C.H.; Giovannoni, G.; Keir, G.; Cunnington, M.; Thompson, E.J. Seroprevalence of herpes simplex virus type 2 in multiple sclerosis. Acta Neurol. Scand. 2006, 114, 363–367. [Google Scholar] [CrossRef]
- Voumvourakis, K.I.; Kitsos, D.K.; Tsiodras, S.; Petrikkos, G.; Stamboulis, E. Human herpesvirus 6 infection as a trigger of multiple sclerosis. Mayo Clin. Proc. 2010, 85, 1023–1030. [Google Scholar] [CrossRef] [Green Version]
- Czarnowska, A.; Kapica-Topczewska, K.; Zajkowska, O.; Świerzbińska, R.; Chorąży, M.; Tarasiuk, J.; Zajkowska, J.; Kochanowicz, J.; Kułakowska, A. Herpesviridae Seropositivity in Patients with Multiple Sclerosis: First Polish Study. Eur. Neurol. 2018, 80, 229–235. [Google Scholar] [CrossRef]
- Etemadifar, M.; Izadi, A.; Sabeti, F.; Noorshargh, P. Anti-HSV-2 antibody in patients with MS and NMO. Mult. Scler. Relat. Disord. 2019, 28, 286–289. [Google Scholar] [CrossRef] [PubMed]
- Wajgt, A.; Górny, M. CSF antibodies to myelin basic protein and to myelin-associated glycoprotein in multiple sclerosis. Evidence of the intrathecal production of antibodies. Acta Neurol. Scand. 1983, 68, 337–343. [Google Scholar] [CrossRef]
- Bar-Or, A.; Vollmer, T.; Antel, J.; Arnold, D.L.; Bodner, C.A.; Campagnolo, D.; Gianettoni, J.; Jalili, F.; Kachuck, N.; Lapierre, Y. Induction of antigen-specific tolerance in multiple sclerosis after immunization with DNA encoding myelin basic protein in a randomized, placebo-controlled phase 1/2 trial. Arch. Neurol. 2007, 64, 1407–1415. [Google Scholar] [CrossRef] [Green Version]
- Garren, H.; Robinson, W.H.; Krasulová, E.; Havrdová, E.; Nadj, C.; Selmaj, K.; Losy, J.; Nadj, I.; Radue, E.W.; Kidd, B.A. Phase 2 trial of a DNA vaccine encoding myelin basic protein for multiple sclerosis. Ann. Neurol. 2008, 63, 611–620. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| MS(n = 5) | Seropositive NMOSD (n = 6) | Seronegative NMOSD (n = 5) | MOGAD (n = 6) | HC (n = 5) | |
|---|---|---|---|---|---|
| Male: Female (n:n) | 2:3 | 1:5 | 1:4 | 2:4 | 3:2 |
| Age, years (mean, range) | 38.4 (26–47) | 39.3 (24–50) | 37.8 (27–52) | 38.0 (29–53) | 33.8 (26–45) |
| EDSS (median[quartile]) | 2.3 (2,3) | 3 (2.25, 3.875) | 3.5 (2.75, 3.5) | 2.75 (1.625, 6.125) | - |
| Optic nerve lesion (n) | 1 | 0 | 0 | 1 | - |
| Spinal cord lesion (n) | 1 | 2 | 0 | 0 | - |
| Brain lesion (n) | 2 | 0 | 0 | 0 | - |
| Spinal cord with optic nerve lesion (n) | 0 | 2 | 4 | 2 | - |
| Spinal cord with brain lesion (n) | 1 | 0 | 0 | 1 | - |
| Optic nerve with brain lesion (n) | 0 | 1 | 0 | 0 | - |
| Comparison (A vs. B) | Antigen Type | Peptide | Mean Difference (A–B, FU) | p Values |
|---|---|---|---|---|
| MS vs. HC | CMV envelope glycoprotein B | GVNETIYNTTLKYGD | 7.94 | 0.064 * |
| NETIYNTTLKYGDVV | 7.15 | 0.093 * | ||
| ETIYNTTLKYGDVVG | 6.9 | 0.098 * | ||
| Seronegative NMOSD vs. HC | CMV envelope glycoprotein B | GVNETIYNTTLKYGD | 7.35 | 0.064 * |
| NETIYNTTLKYGDVV | 6.76 | 0.093 * | ||
| ETIYNTTLKYGDVVG | 6.28 | 0.098 * | ||
| Seropositive NMOSD vs. HC | CMV envelope glycoprotein B | TIRSEAEDSYHFSSA | 1.81 | 0.088 * |
| VVGVNTTKYPYRVCS | 1.75 | 0.087 * | ||
| LVAFLERADSVISWD | 1.73 | 0.089 * | ||
| FLERADSVISWDIQD | 1.6 | 0.087 * | ||
| CMV pp65 | SDEELVTTERKTPRV | 4.52 | 0.089 * | |
| TRQQNQWKEPDVYYT | 2.45 | 0.092 * | ||
| RGRLKAESTVAPEED | 1.96 | 0.087 * | ||
| Seropositive NMOSD vs. MS | CMV envelope glycoprotein B | TIRSEAEDSYHFSSA | 1.81 | 0.088 * |
| VVGVNTTKYPYRVCS | 1.75 | 0.087 * | ||
| LVAFLERADSVISWD | 1.73 | 0.089 * | ||
| FLERADSVISWDIQD | 1.6 | 0.087 * | ||
| CMV pp65 | SDEELVTTERKTPRV | 4.52 | 0.089 * | |
| TRQQNQWKEPDVYYT | 2.45 | 0.092 * | ||
| RGRLKAESTVAPEED | 1.96 | 0.087 * | ||
| Seropositive NMOSD vs. seronegative NMOSD | CMV envelope glycoprotein B | TIRSEAEDSYHFSSA | 1.81 | 0.088 * |
| VVGVNTTKYPYRVCS | 1.75 | 0.087 * | ||
| LVAFLERADSVISWD | 1.73 | 0.089 * | ||
| FLERADSVISWDIQD | 1.6 | 0.087 * | ||
| CMV pp65 | TRQQNQWKEPDVYYT | 2.45 | 0.092 * | |
| RGRLKAESTVAPEED | 1.96 | 0.087 * | ||
| Seropositive NMOSD vs. MOGAD | CMV envelope glycoprotein B | TIRSEAEDSYHFSSA | 1.81 | 0.088 * |
| VVGVNTTKYPYRVCS | 1.75 | 0.087 * | ||
| LVAFLERADSVISWD | 1.73 | 0.089 * | ||
| FLERADSVISWDIQD | 1.6 | 0.087 * | ||
| CMV pp65 | SDEELVTTERKTPRV | 4.52 | 0.089 * | |
| TRQQNQWKEPDVYYT | 2.45 | 0.092 * | ||
| RGRLKAESTVAPEED | 1.96 | 0.087 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.L.; Park, J.-W.; Seok, J.M.; Jeon, M.Y.; Kim, H.; Lim, Y.-M.; Shin, H.Y.; Kang, S.-Y.; Kwon, O.-H.; Lee, S.-S.; et al. Serum Peptide Immunoglobulin G Autoantibody Response in Patients with Different Central Nervous System Inflammatory Demyelinating Disorders. Diagnostics 2021, 11, 1339. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11081339
Lee HL, Park J-W, Seok JM, Jeon MY, Kim H, Lim Y-M, Shin HY, Kang S-Y, Kwon O-H, Lee S-S, et al. Serum Peptide Immunoglobulin G Autoantibody Response in Patients with Different Central Nervous System Inflammatory Demyelinating Disorders. Diagnostics. 2021; 11(8):1339. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11081339
Chicago/Turabian StyleLee, Hye Lim, Jin-Woo Park, Jin Myoung Seok, Mi Young Jeon, Hojin Kim, Young-Min Lim, Ha Young Shin, Sa-Yoon Kang, Oh-Hyun Kwon, Sang-Soo Lee, and et al. 2021. "Serum Peptide Immunoglobulin G Autoantibody Response in Patients with Different Central Nervous System Inflammatory Demyelinating Disorders" Diagnostics 11, no. 8: 1339. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11081339