
The Wide Morphological Spectrum of Deep (Aggressive) Angiomyxoma of the Vulvo-Vaginal Region: A Clinicopathologic Study of 36 Cases, including Recurrent Tumors

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
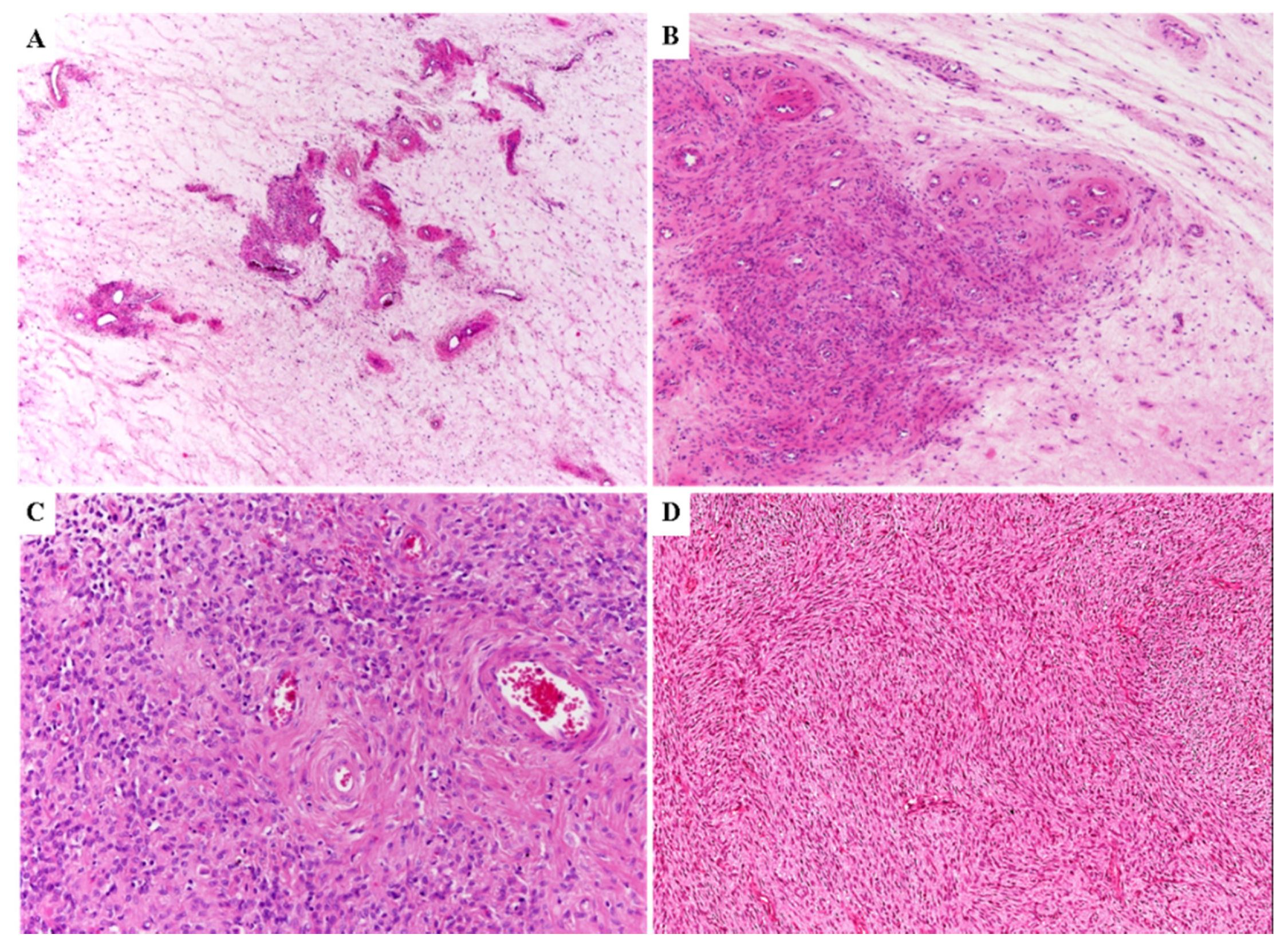
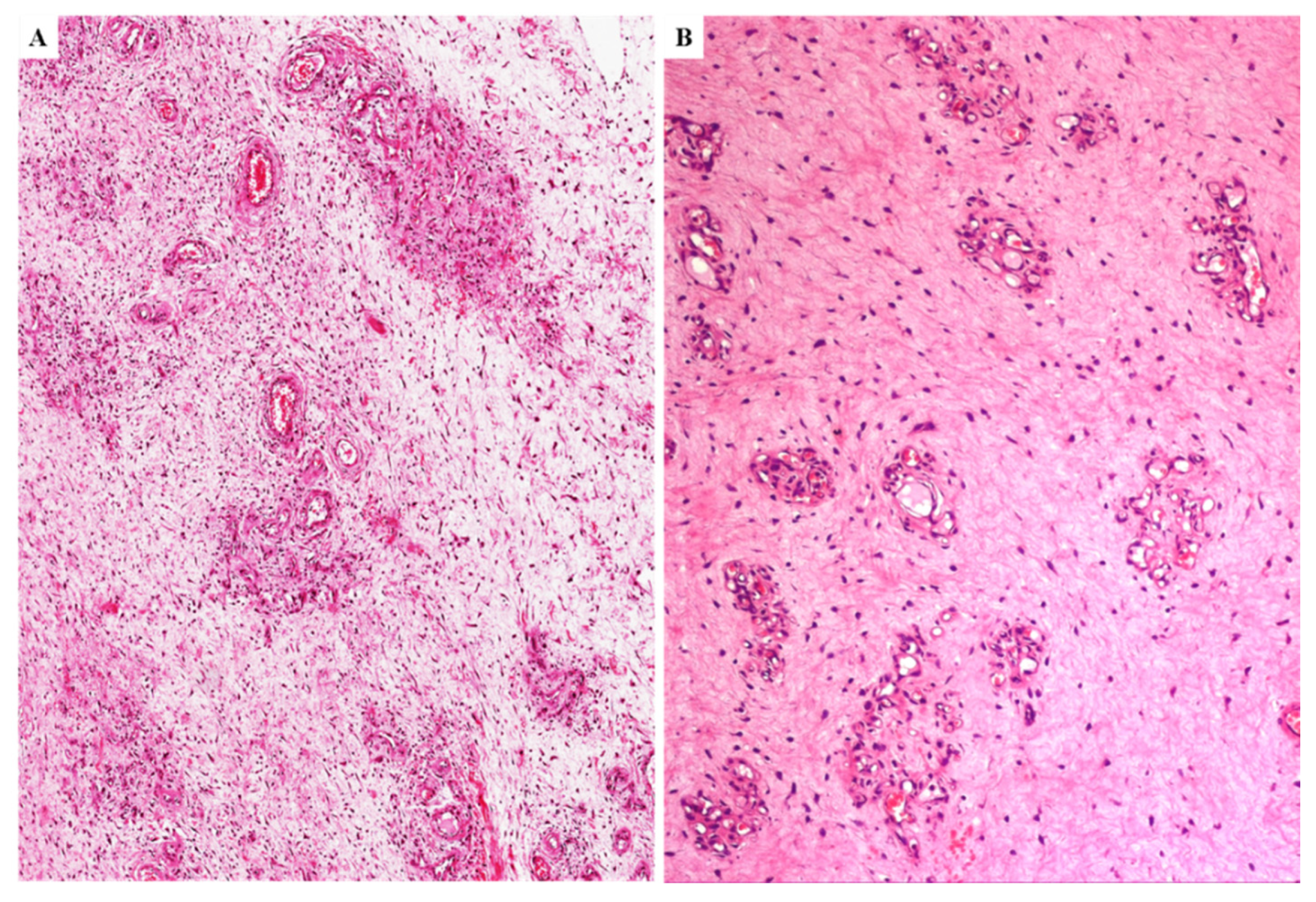
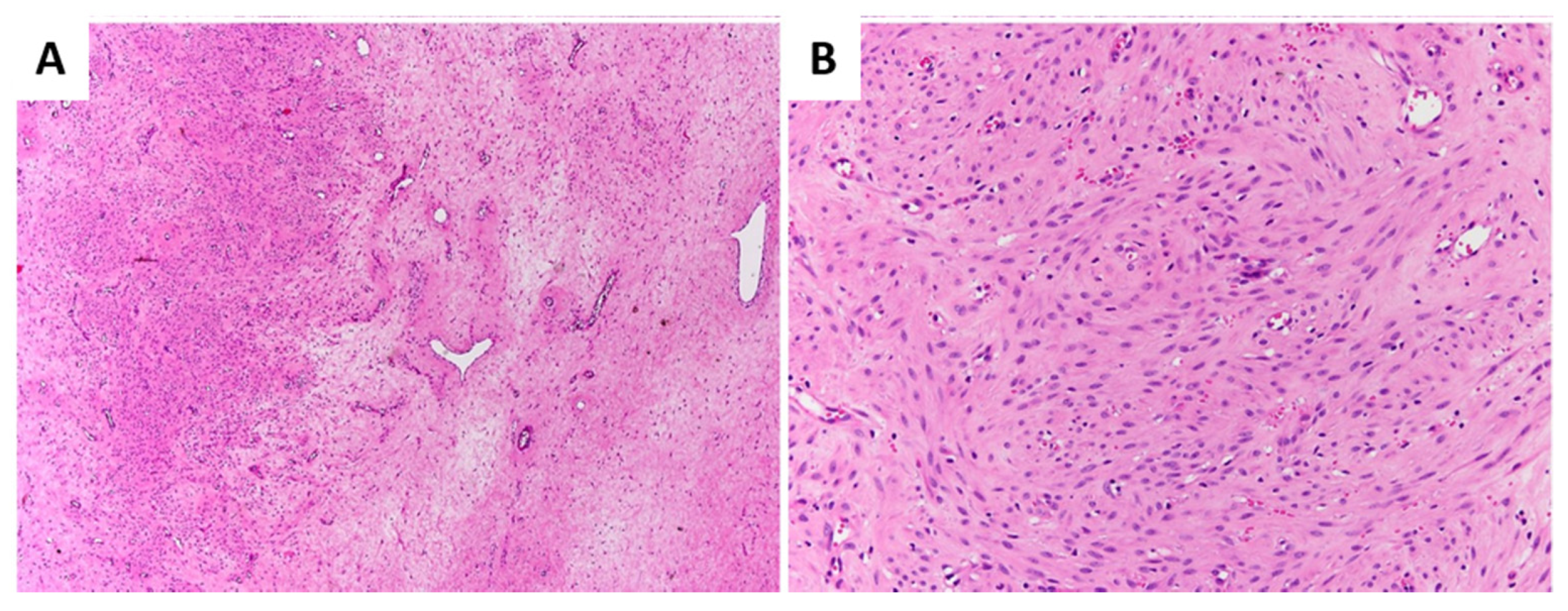
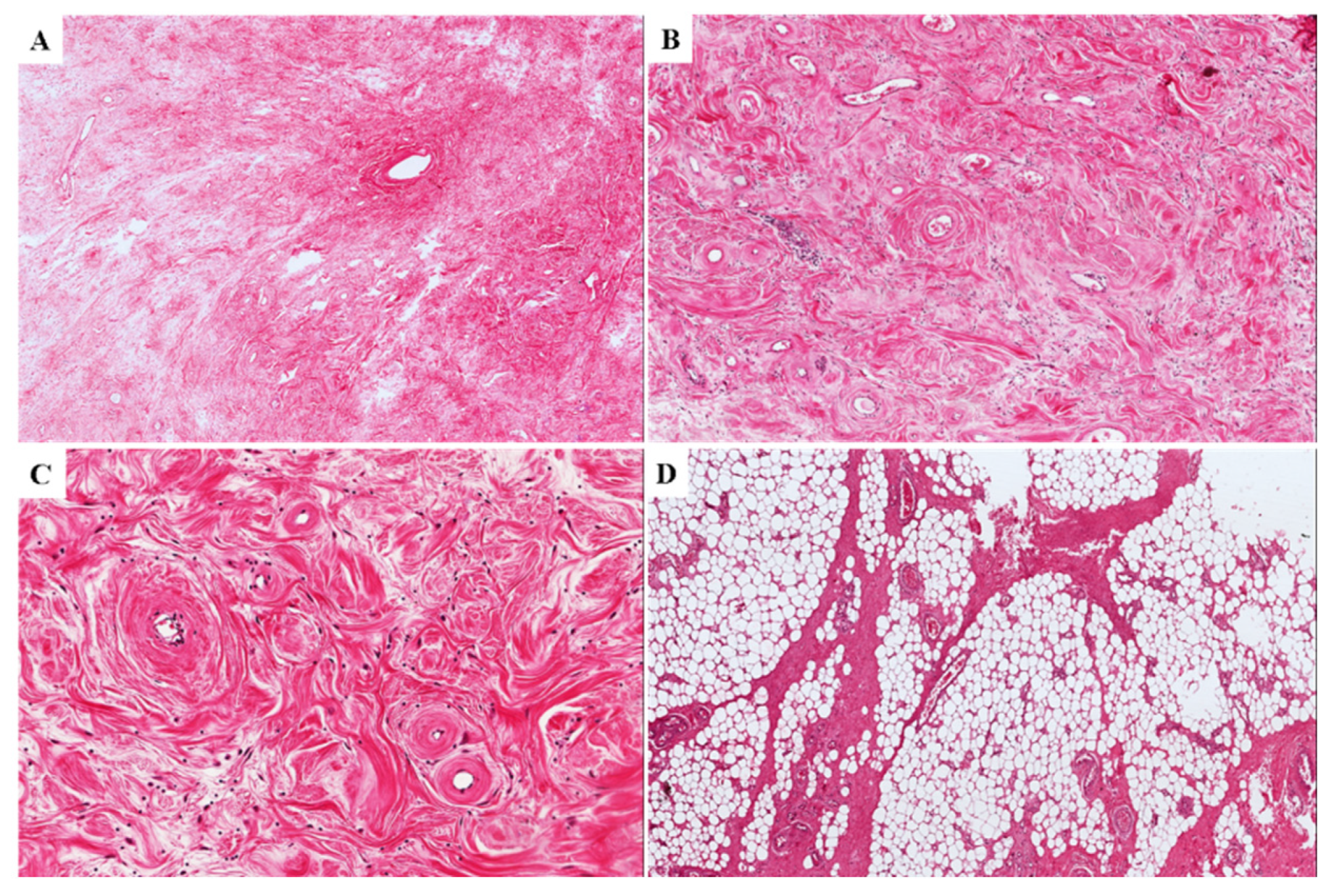
3.1. Primary Tumors
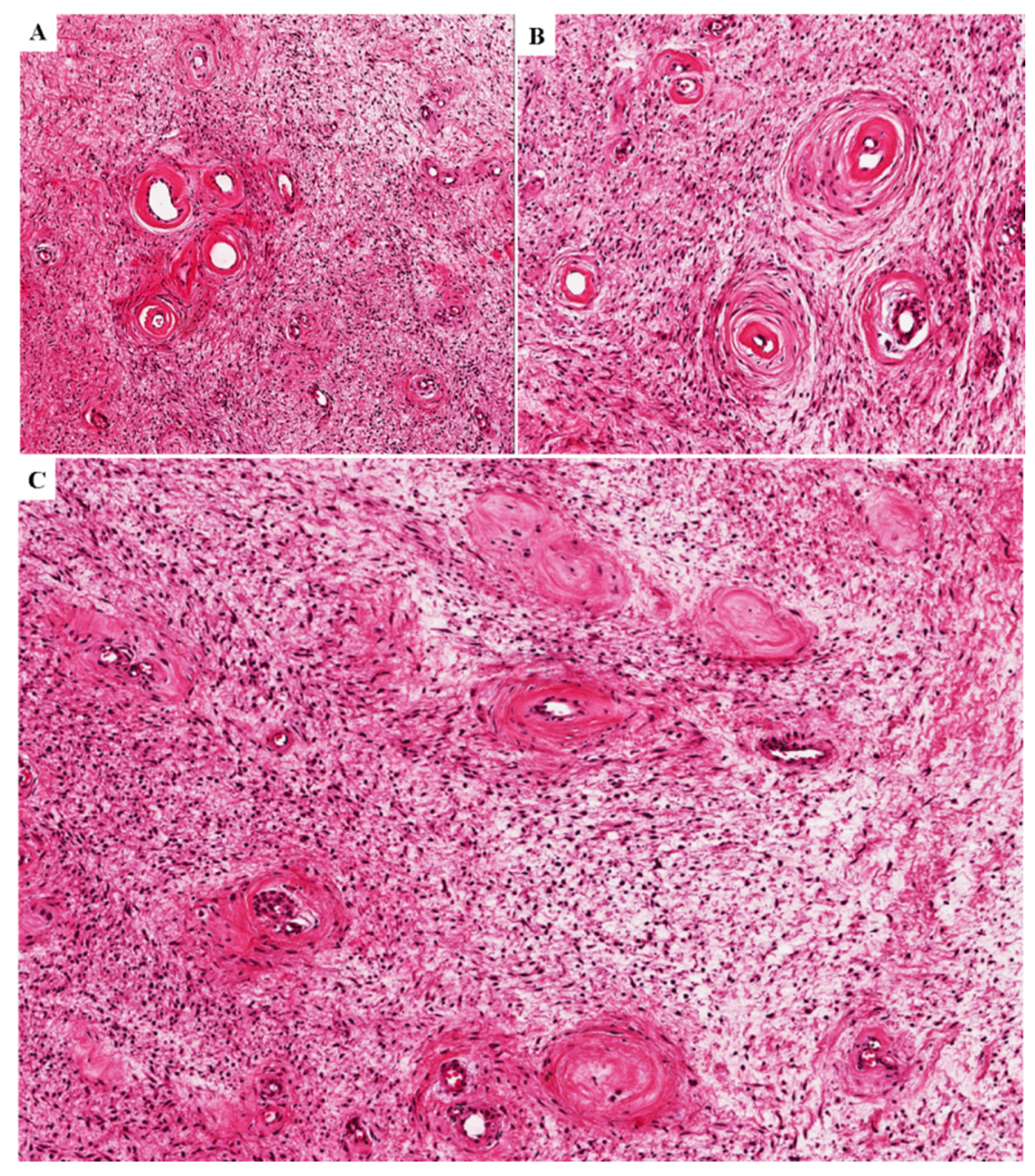
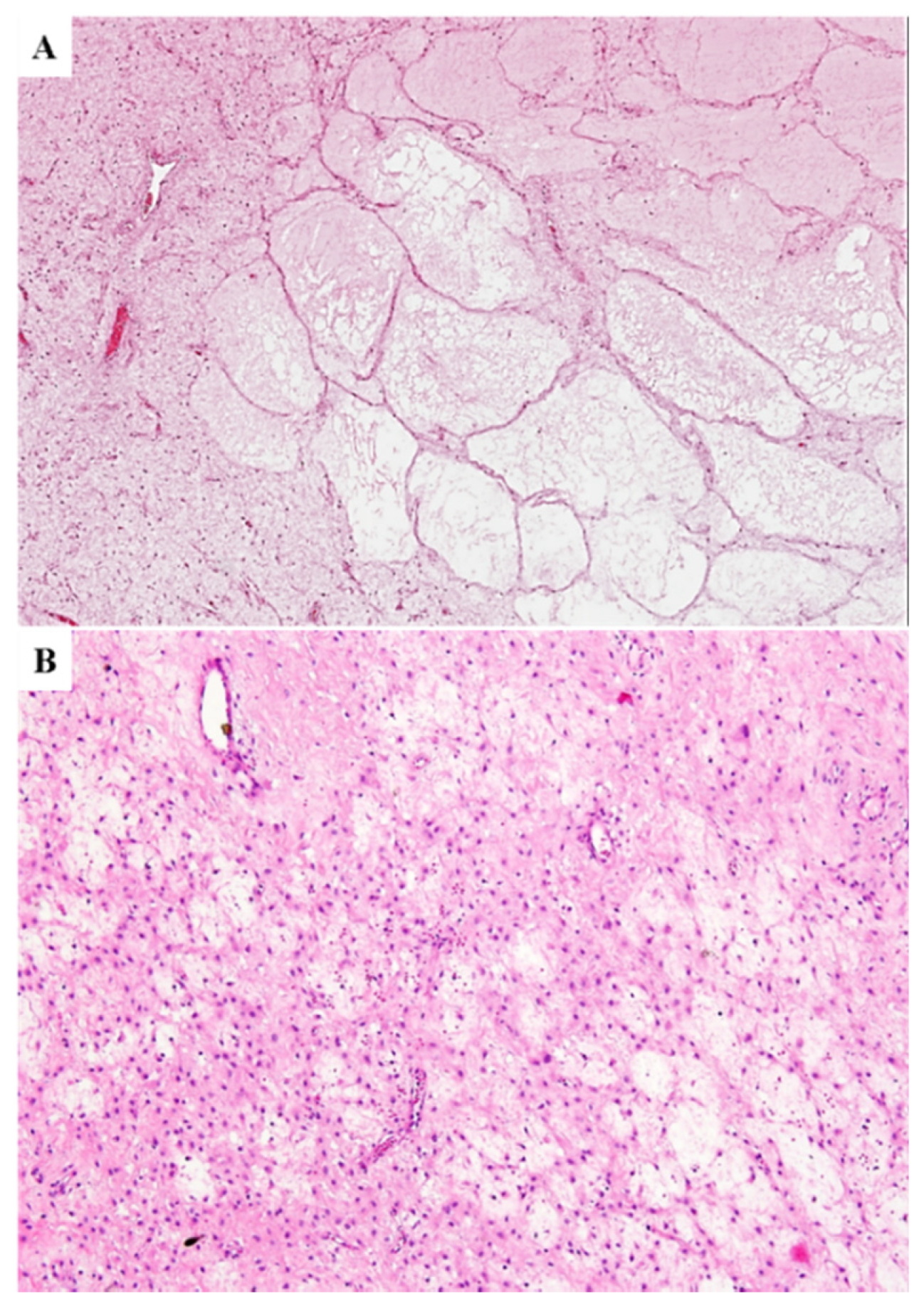
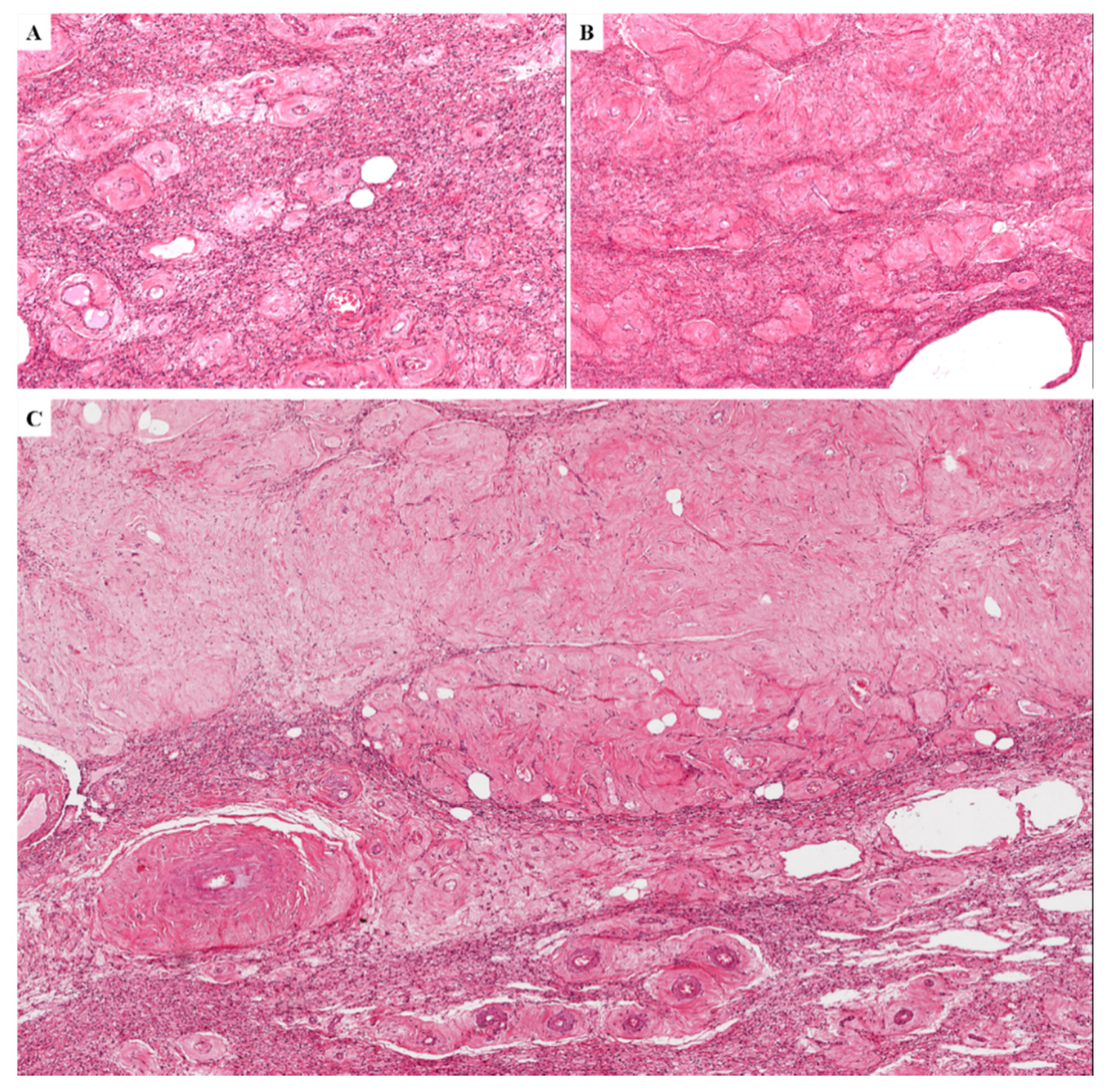
3.2. Locally Recurrent Tumors
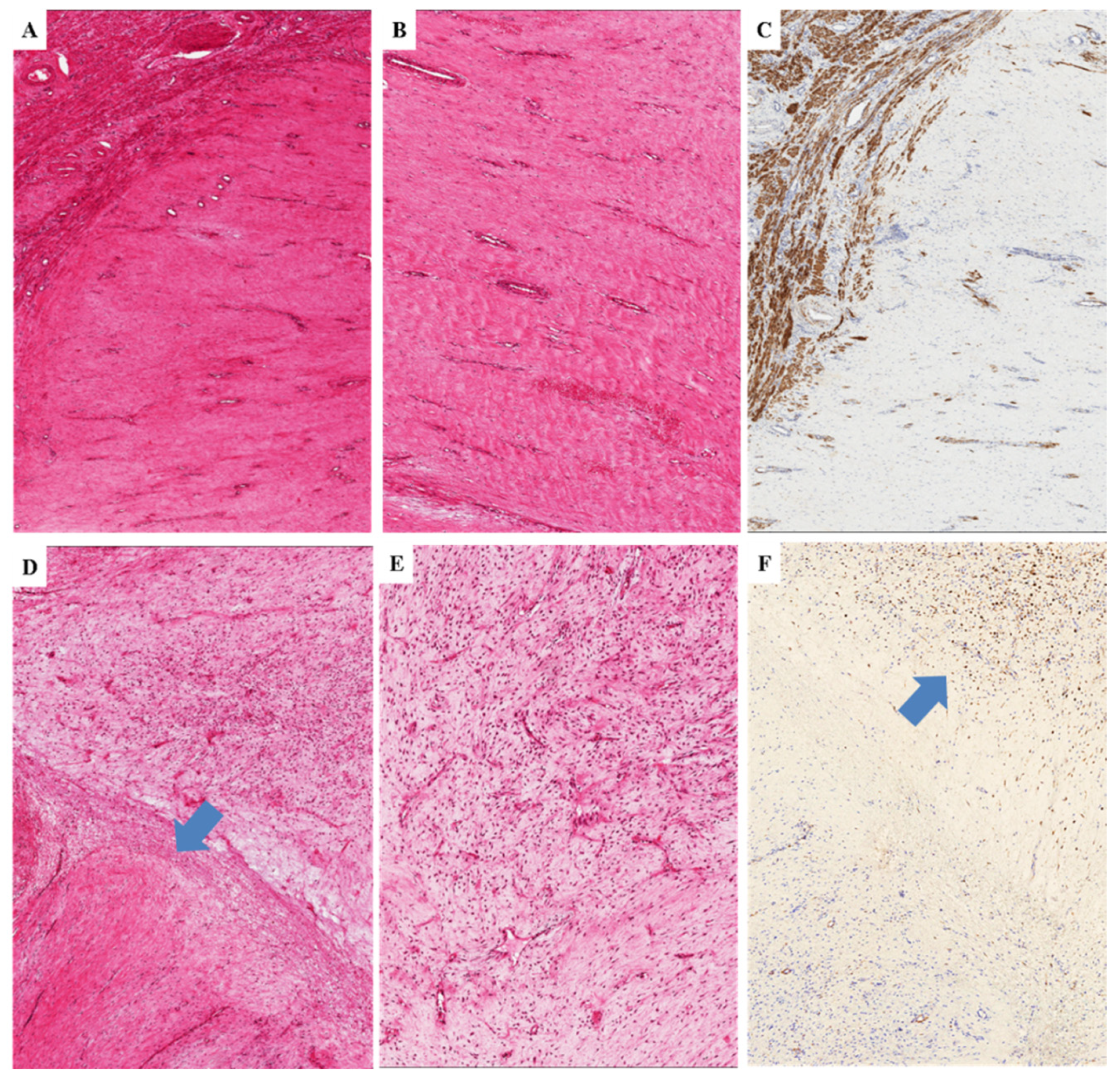
3.3. Immunohistochemical Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Steeper, T.A.; Rosai, J. Aggressive angiomyxoma of the female pelvis and perineum. Report of nine cases of a distinctive type of gynecologic soft-tissue neoplasm. Am. J. Surg. Pathol. 1983, 7, 463–475. [Google Scholar] [CrossRef] [PubMed]
- Begin, L.R.; Clement, P.B.; Kirk, M.E.; Jothy, S.; McCaughey, W.T.; Ferenczy, A. Aggressive angiomyxoma of pelvic soft parts. A clinicopathologic study of nine cases. Hum. Pathol. 1985, 16, 621–628. [Google Scholar] [CrossRef]
- Fetsch, J.F.; Laskin, W.B.; Lefkowitz, M.; Kindblom, L.G.; Meis-Kindblom, J.M. Aggressive angiomyxoma: A clinicopathologic study of 29 female patients. Cancer 1996, 78, 79–90. [Google Scholar] [CrossRef]
- Granter, S.R.; Nucci, M.R.; Fletcher, C.D. Aggressive angiomyxoma: Reappraisal of its relationship to angiomyofibroblastoma in a series of 16 cases. Histopathology 1997, 30, 3–10. [Google Scholar] [CrossRef]
- Amezcua, C.A.; Begley, S.J.; Mata, N.; Felix, J.C.; Ballard, C.A. Aggressive angiomyxoma of the female genital tract: A clinicopathologic and immunohistochemical study of 12 cases. Int. J. Gynecol. Cancer 2005, 15, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Tsang, W.Y.; Chan, J.K.; Lee, K.C.; Fisher, C.; Fletcher, C.D. Aggressive angiomyxoma. A report of four cases occurring in men. Am. J. Surg. Pathol. 1992, 16, 1059–1065. [Google Scholar] [CrossRef] [PubMed]
- Idrees, M.T.; Hoch, B.L.; Wang, B.Y.; Unger, P.D. Aggressive angiomyxoma of male genital region. Report of 4 cases with immunohistochemical evaluation including hormone receptor status. Ann. Diagn. Pathol. 2006, 10, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Chan, Y.M.; Hon, E.; Ngai, S.W.; Ng, T.Y.; Wong, L.C. Aggressive angiomyxoma in females: Is radical resection the only option? Acta Obstet. Gynecol. Scand. 2000, 79, 216–220, Erratum in Acta Obstet. Gynecol. Scand. 2000, 79, 432. [Google Scholar] [CrossRef] [PubMed]
- Kallen, M.E.; Hornick, J.L. The 2020 WHO Classification: What’s New in Soft Tissue Tumor Pathology? Am. J. Surg. Pathol. 2021, 45, e1–e23. [Google Scholar] [CrossRef] [PubMed]
- Magro, G.; Caltabiano, R.; Kacerovská, D.; Vecchio, G.M.; Kazakov, D.; Michal, M. Vulvovaginal myofibroblastoma: Expanding the morphological and immunohistochemical spectrum. A clinicopathologic study of 10 cases. Hum. Pathol. 2012, 43, 243–253. [Google Scholar] [CrossRef] [PubMed]
- Magro, G.; Righi, A.; Caltabiano, R.; Casorzo, L.; Michal, M. Vulvovaginal angiomyofibroblastomas: Morphologic, immunohistochemical, and fluorescence in situ hybridization analysis for deletion of 13q14 region. Hum. Pathol. 2014, 45, 1647–1655. [Google Scholar] [CrossRef] [PubMed]
- Magro, G.; Righi, A.; Casorzo, L.; Antonietta, T.; Salvatorelli, L.; Kacerovská, D.; Kazakov, D.; Michal, M. Mammary and vaginal myofibroblastomas are genetically related lesions: Fluorescence in situ hybridization analysis shows deletion of 13q14 region. Hum. Pathol. 2012, 43, 1887–1893. [Google Scholar] [CrossRef]
- Van Roggen, J.F.; McMenamin, M.E.; Fletcher, C.D. Cellular myxoma of soft tissue: A clinicopathological study of 38 cases confirming indolent clinical behaviour. Histopathology 2001, 39, 287–297. [Google Scholar] [CrossRef]
- Tajima, S.; Kohashi, K.; Fan, B.; Doi, W.; Kimura, R.; Tamura, Y.; Abe, H.; Oda, Y. Aggressive Angiomyxoma of the Pelvis with a Cellular Nodule Composed of Tumor Cells showing Epithelioid Features. Rare Tumors 2014, 6, 5397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Roggen, J.F.; van Unnik, J.A.; Briaire-de Bruijn, I.H.; Hogendoorn, P.C. Aggressive angiomyxoma: A clinicopathological and immunohistochemical study of 11 cases with long-term follow-up. Virchows Arch. 2005, 446, 157–163. [Google Scholar] [CrossRef]
- Magro, G.; Salvatorelli, L.; Angelico, G.; Vecchio, G.M.; Caltabiano, R. Lipomatous angiomyofibroblastoma of the vulva: Diagnostic and histogenetic considerations. Pathologica 2014, 106, 322–326. [Google Scholar]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number cases (%) | 11/36 (30.5%) |
| Alternating myxoid/fibrous areas | 8/11 (72.7%) |
| Hypercellular areas | 7/11 (63.6%) |
| Neurofibroma-like areas | 4/11 (36.3%) |
| Perivascular hyalinization | 4/11 (36.3%) |
| Microcystic/reticular stromal changes | 3/11 (27.7%) |
| Perivascular cuffing | 2/11 (18.1%) |
| Microvascular growth pattern | 2/11 (18.1%) |
| Nodular leiomyomatous differentiation | 1/11 (9%) |
| Prominent fibrosclerotic stroma | 1/11 (9%) |
| Cases | Recurrent Tumor | Primary Tumor |
|---|---|---|
| Case n. 1 | Classic-type morphology | Classic-type morphology |
| Case n. 2 | Classic-type morphology | Classic-type morphology |
| Case n. 3 | Hypocellular with prominent/exclusive fibrosclerotic stroma; Perivascular hyalinization | Classic-type morphology |
| Case n. 4 | Hypocellular with prominent/exclusive fibrosclerotic stroma; Perivascular hyalinization | Classic-type morphology |
| Case n. 5 | Hypocellular with prominent/exclusive fibrosclerotic stroma; Perivascular hyalinization with lumen obliteration and formation of confluent nodular structures | Classic-type morphology with microcystic/reticular stromal changes |
| Case n. 6 | Hypercellularity (40% of tumor); Perivascular hyalinization with lumen obliteration | Classic-type morphology |
| References | Desmin | α-SMA | Vimentin | S-100 | CD34 | h-caldesmon |
|---|---|---|---|---|---|---|
| Steeper TA et al. [1] | NA | NA | NA | NA | NA | NA |
| Begin LR et al. [2] | NA | 4/5 (80%) | NA | 0/5 (0%) | NA | NA |
| Fetsch JF et al. [3] | 22/22 (100%) | 19/20 (95%) | 17/17 (100%) | 0/20 (0%) | 8/16 (50%) | NA |
| Granter SR et al. [4] | 13/14 (93%) | 10/11 (91%) | NA | 0/16 (0%) | NA | NA |
| Amezcua CA et al. [5] | 8/11 (73%) | 3/11 (27%) | 11/11 (100%) | 0/11 (0%) | NA | NA |
| Present series (Magro G et al.) | 36/36 (100%) | 10/36 (28%) | 36/36 (100%) | 0/36 (0%) | 6/36 (17%) | 10/36 (28%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Magro, G.; Angelico, G.; Michal, M.; Broggi, G.; Zannoni, G.F.; Covello, R.; Marletta, S.; Salvatorelli, L.; Parenti, R. The Wide Morphological Spectrum of Deep (Aggressive) Angiomyxoma of the Vulvo-Vaginal Region: A Clinicopathologic Study of 36 Cases, including Recurrent Tumors. Diagnostics 2021, 11, 1360. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11081360
Magro G, Angelico G, Michal M, Broggi G, Zannoni GF, Covello R, Marletta S, Salvatorelli L, Parenti R. The Wide Morphological Spectrum of Deep (Aggressive) Angiomyxoma of the Vulvo-Vaginal Region: A Clinicopathologic Study of 36 Cases, including Recurrent Tumors. Diagnostics. 2021; 11(8):1360. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11081360
Chicago/Turabian StyleMagro, Gaetano, Giuseppe Angelico, Michal Michal, Giuseppe Broggi, Gian Franco Zannoni, Renato Covello, Stefano Marletta, Lucia Salvatorelli, and Rosalba Parenti. 2021. "The Wide Morphological Spectrum of Deep (Aggressive) Angiomyxoma of the Vulvo-Vaginal Region: A Clinicopathologic Study of 36 Cases, including Recurrent Tumors" Diagnostics 11, no. 8: 1360. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11081360