
Colon Tissues Classification and Localization in Whole Slide Images Using Deep Learning

 ,
,  , ,
, ,  ,
,  ,
,
Abstract
:1. Introduction
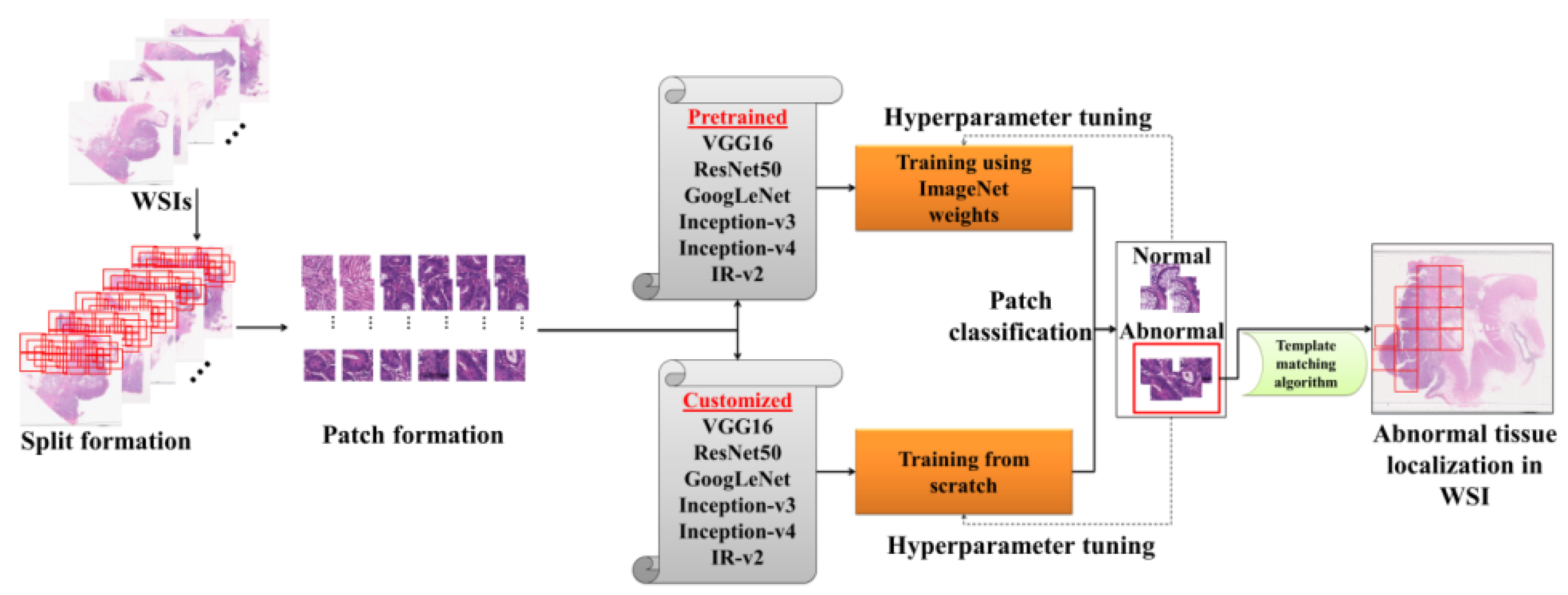
- A new dataset consisting of 297 WSI for the colon was collected and manually annotated by a well-experienced pathologist.
- Transfer learning was investigated considering the training of different CNN architectures using weights obtained from different domain datasets, and performances were recorded after hyperparameter tuning.
- Different customized CNNs models were built and trained from scratch using target dataset, and performances were recorded and investigated after hyperparameter tuning.
- Among the customized models, the top-performing model was studied further to check if the model can be further tuned to obtain the best customized model.
- The best-customized model IR-v2 Type 5 achieved an F-score of 0.99 and AUC 0.99.
- The patches classified as abnormal were localized in the WSI, which could be beneficial for pathologists to examine less area compared to the whole slide.
- On the basis of our study, we empirically proved that the customized IR-v2 Type 5 model provides better results for the CRC dataset if trained from scratch.
- The IR-v2 Type 5 model developed through this study may be deployed in different hospitals for automatic classification and localization of abnormal tissues in WSI, which can assist pathologists in making accurate decisions in a faster mode and can ultimately help to expedite the treatment and therapy procedure for CRC patients.
2. Materials and Methods
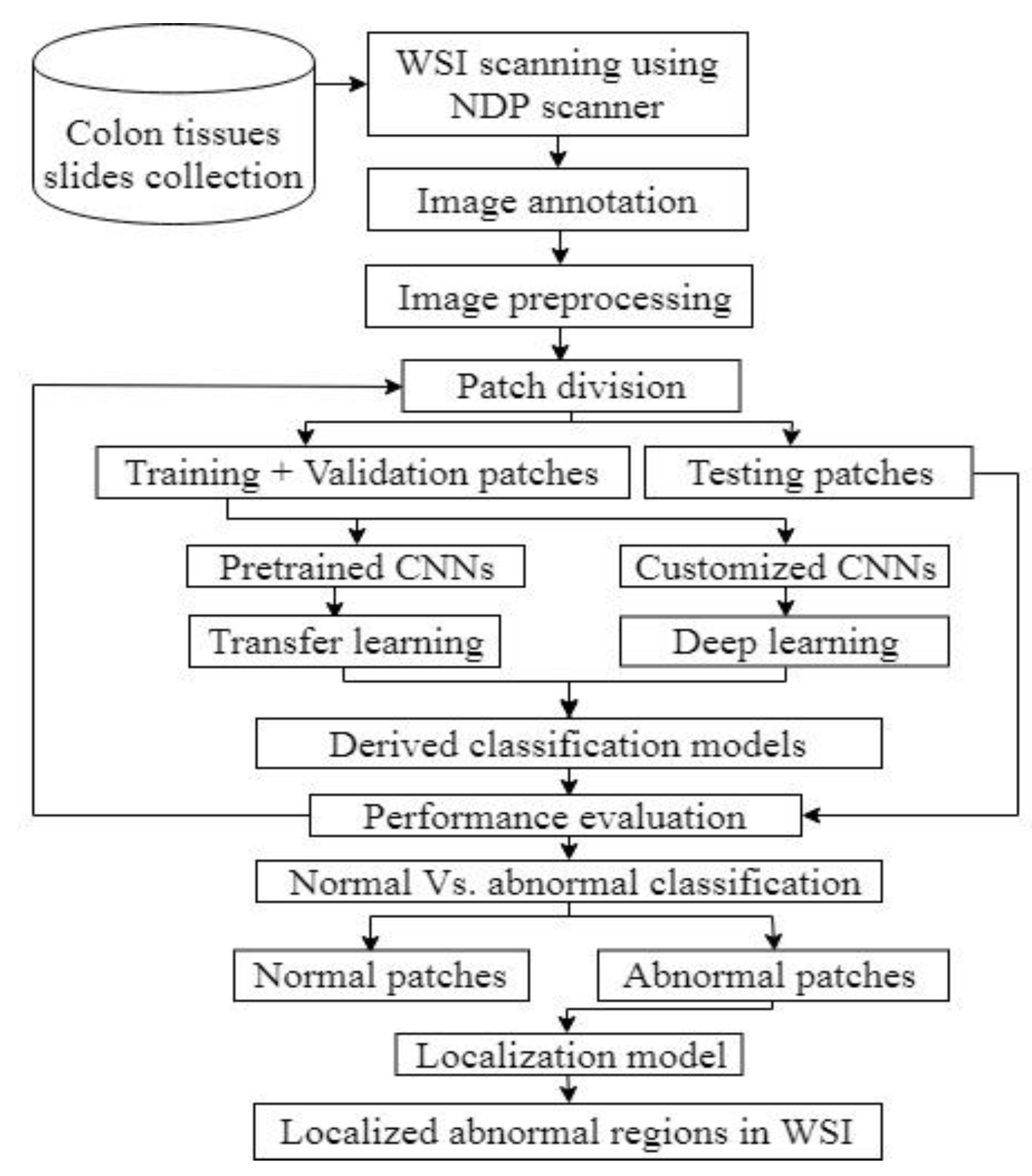
2.1. Study Outline
2.2. Data Acquisition
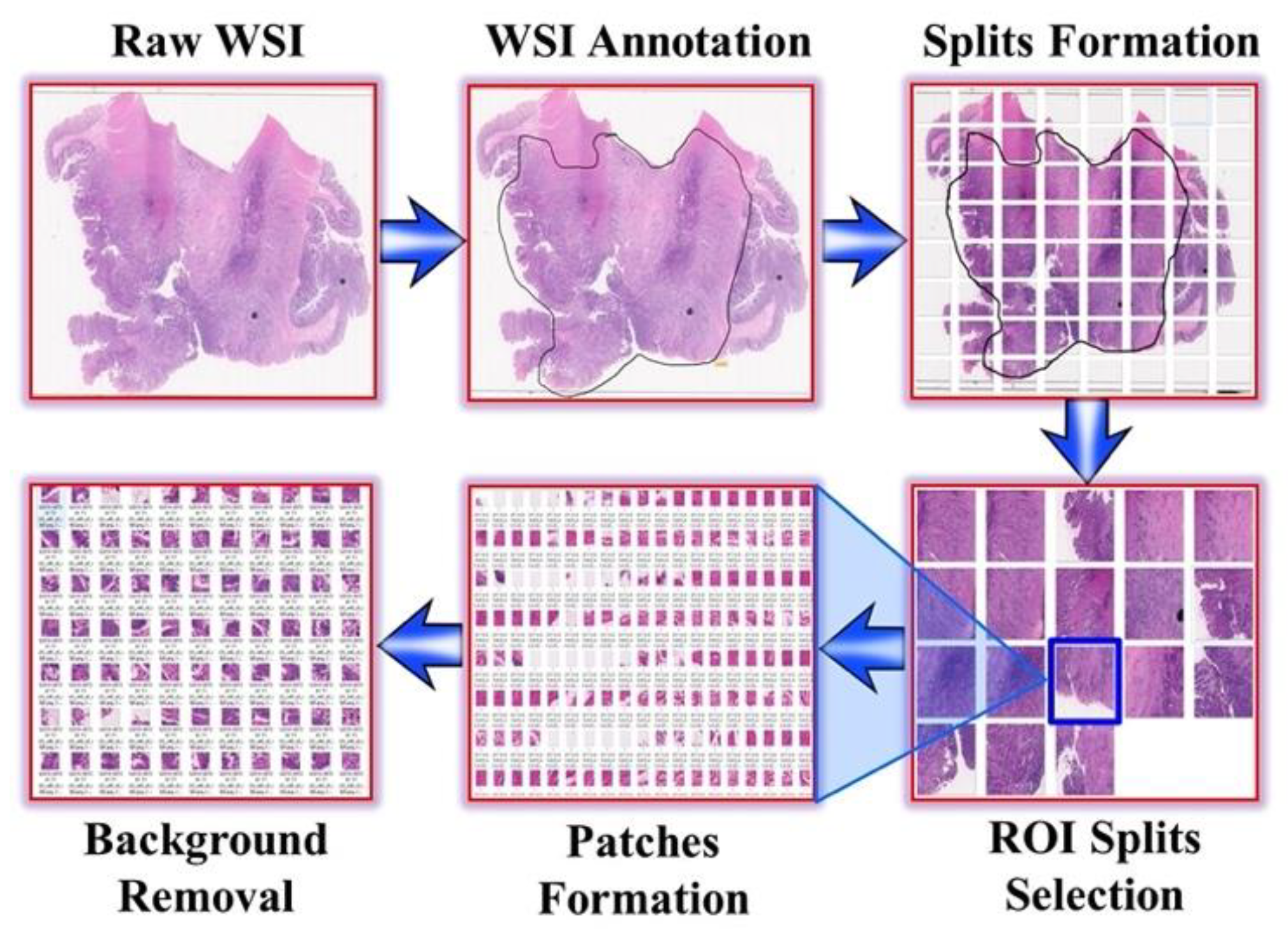
2.3. Image Annotation
2.4. Image Preprocessing
2.5. Artificial Intelligence-Based Analysis
3. Experiments
3.1. Data Divisibility
3.2. Transfer Learning Using Pretrained CNN Architectures
3.3. Deep Learning Using Customized CNN Architectures
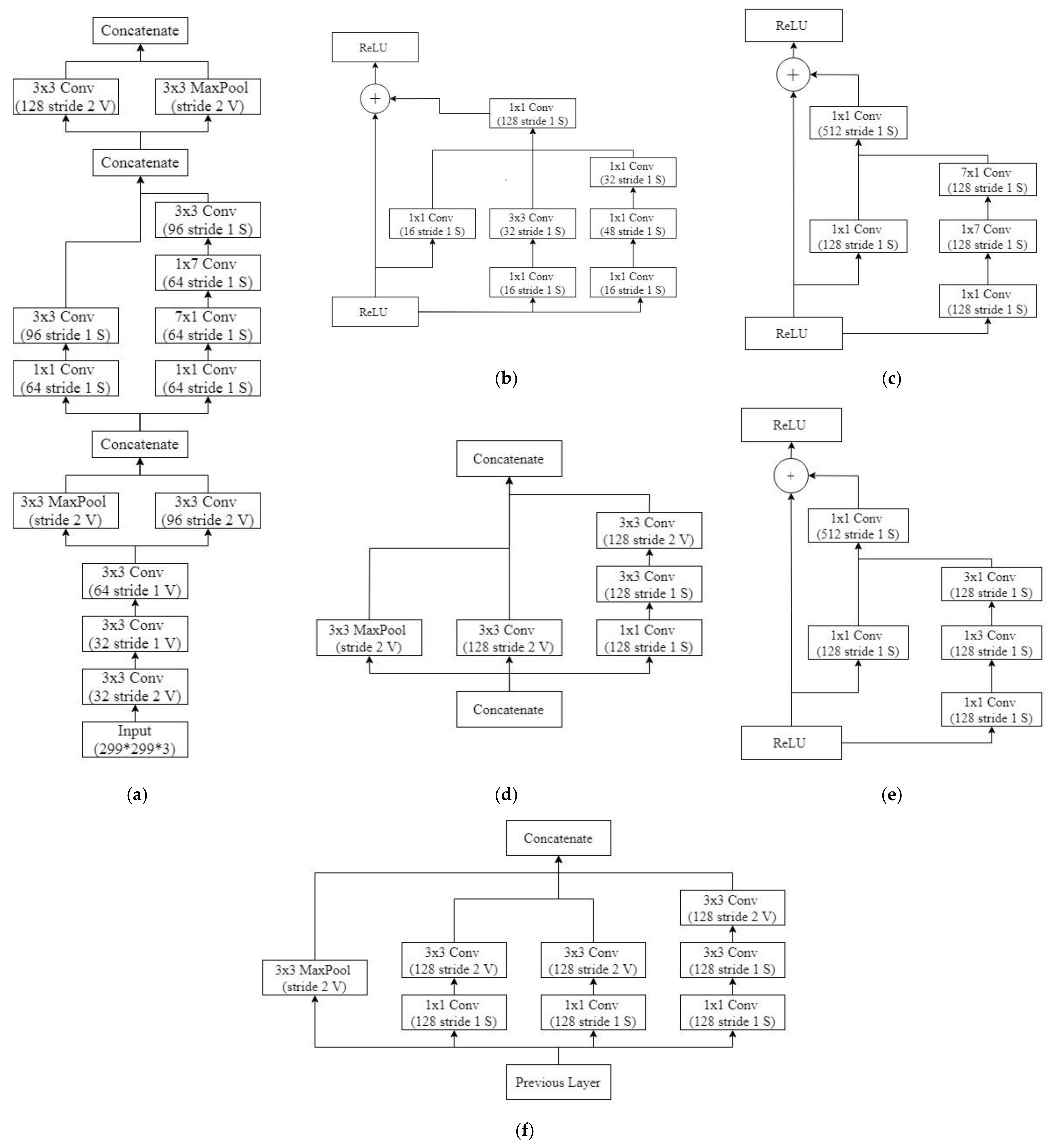
3.4. Deep Learning Using Variants of Customized Inception-ResNet-v2
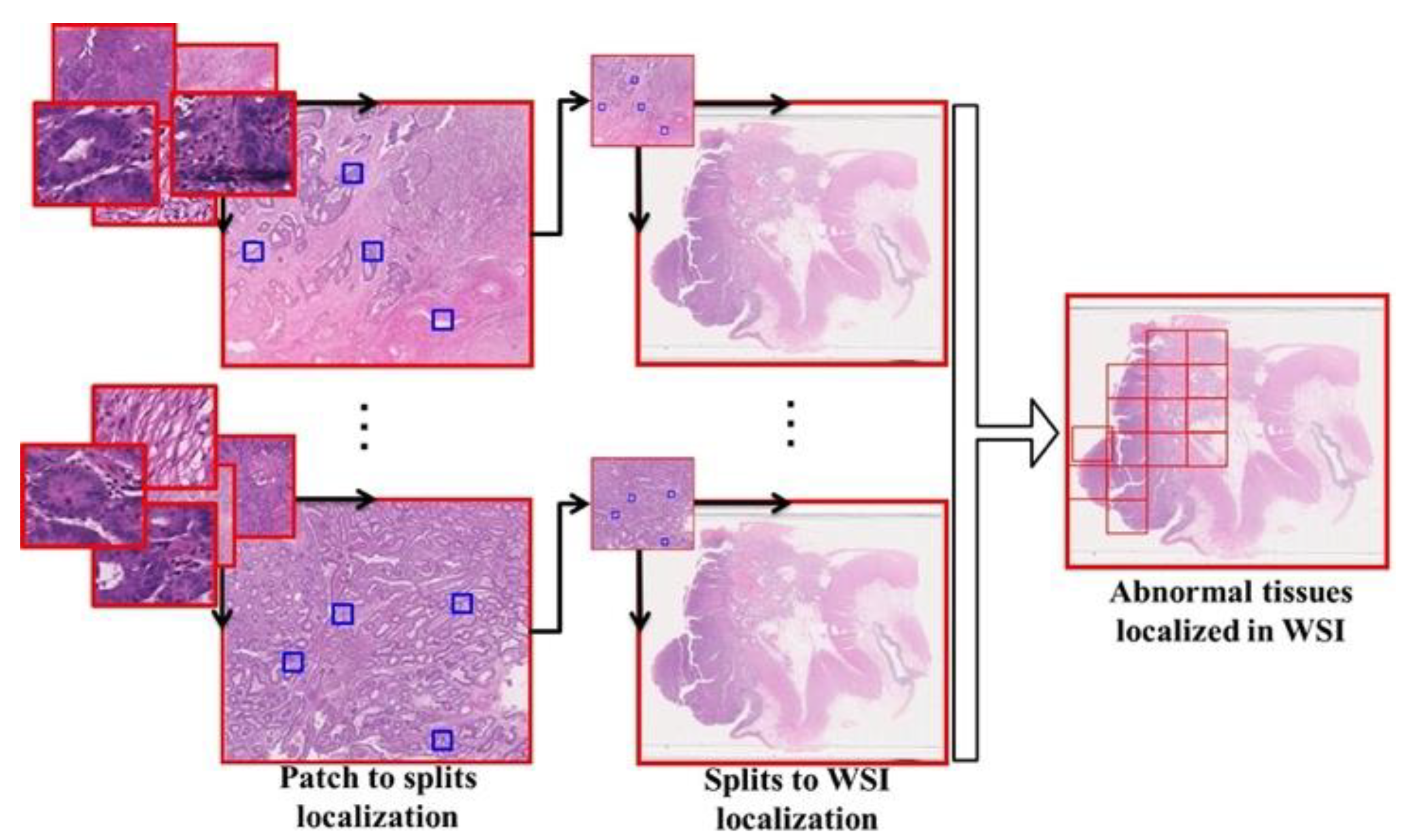
3.5. Localization
3.6. Implementation Environment
4. Results
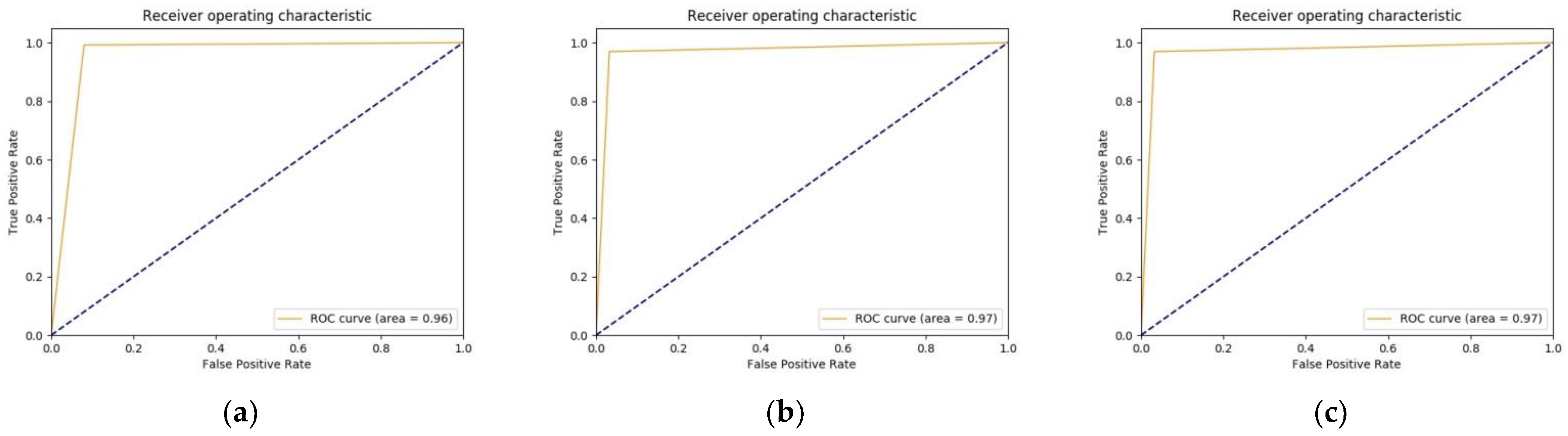
4.1. Transfer Learning Using Pretrained CNN Architectures
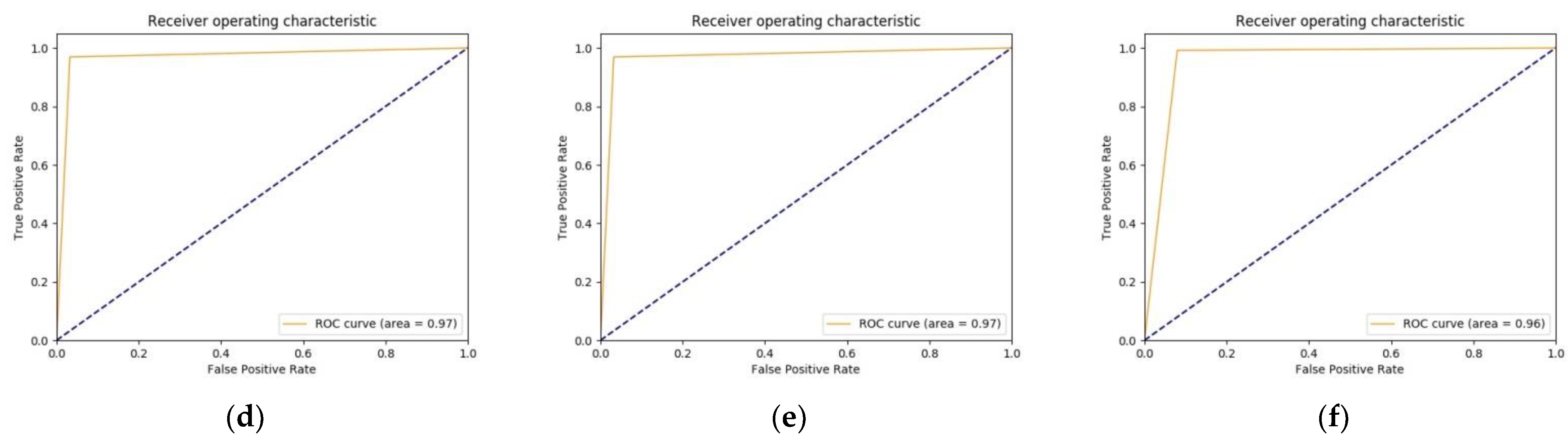
4.2. Deep Learning Using Customized CNN Architectures
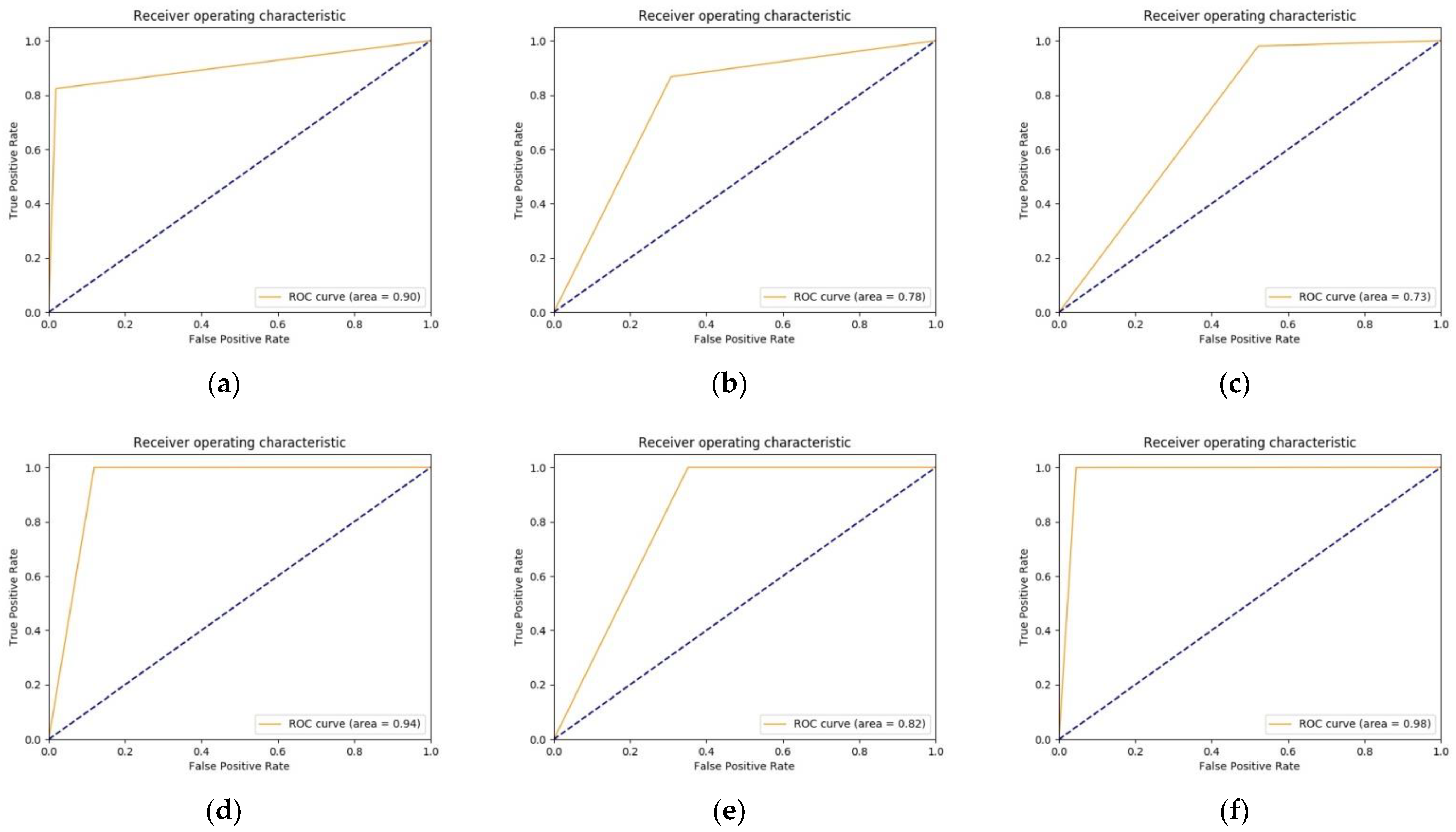
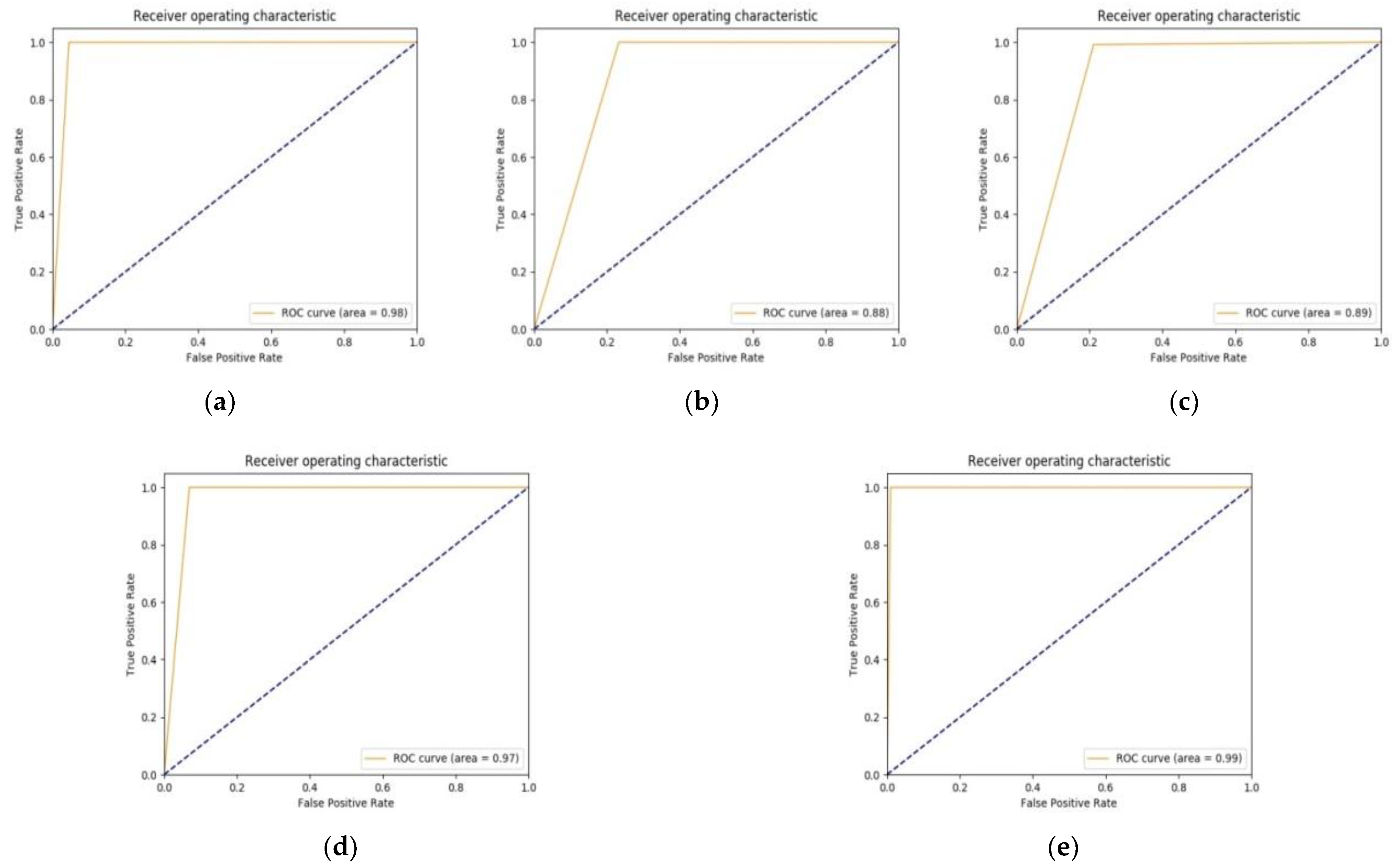
4.3. Deep LEARNING Using Variants of Customized Inception-ResNet-v2
4.4. Classification and Localization Results
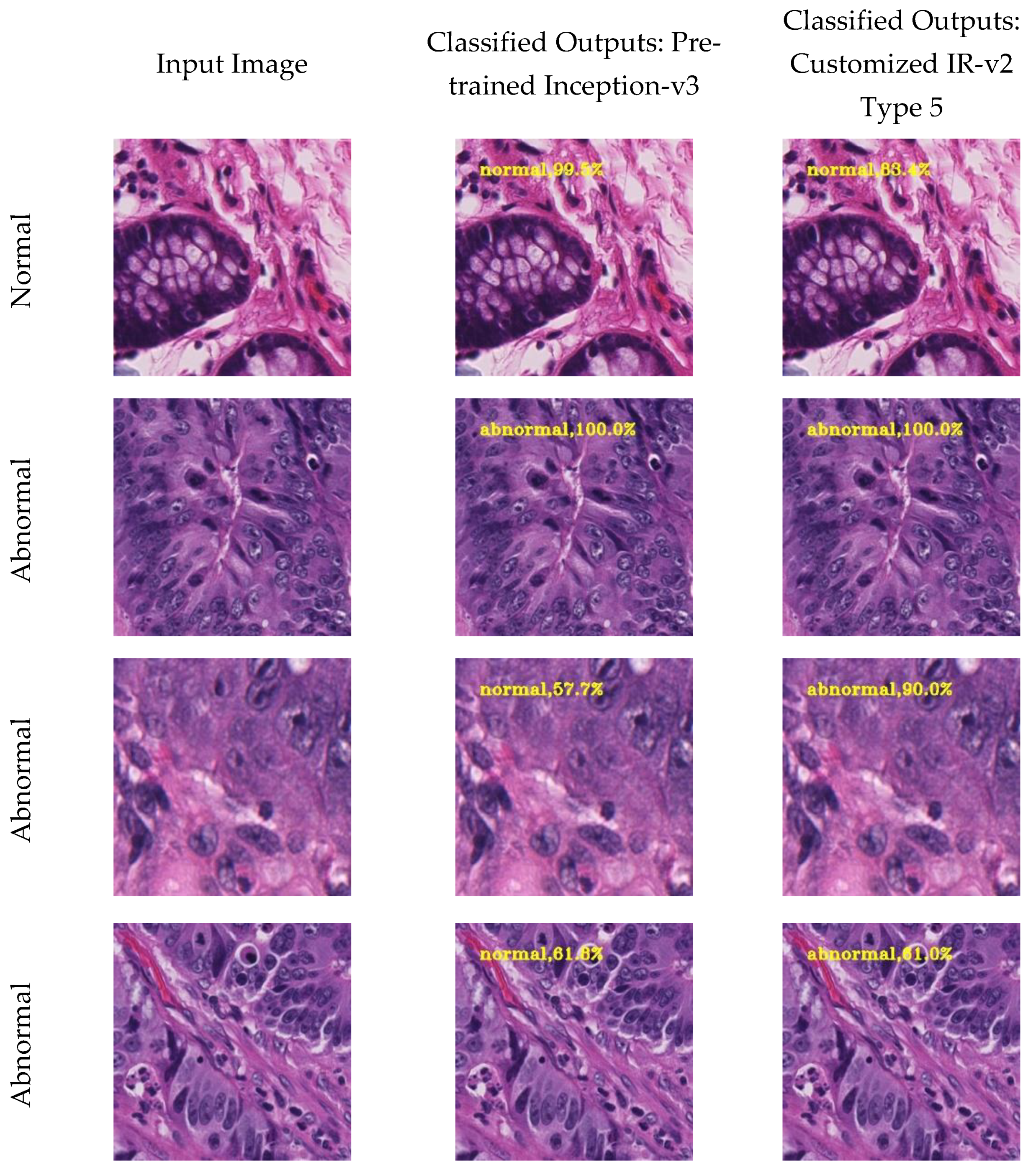
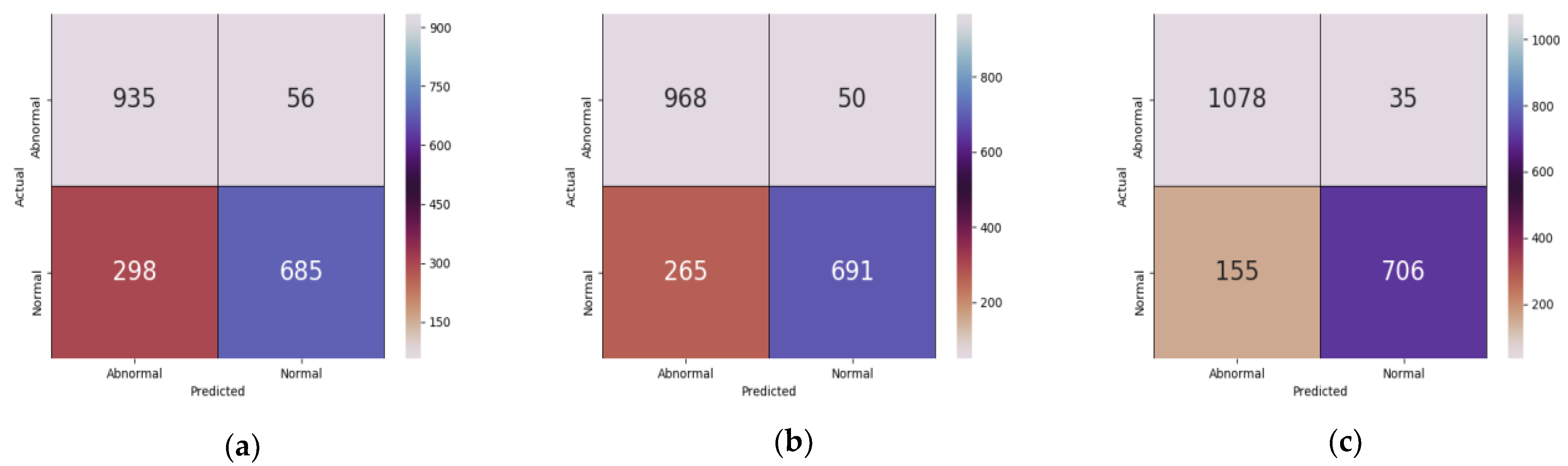
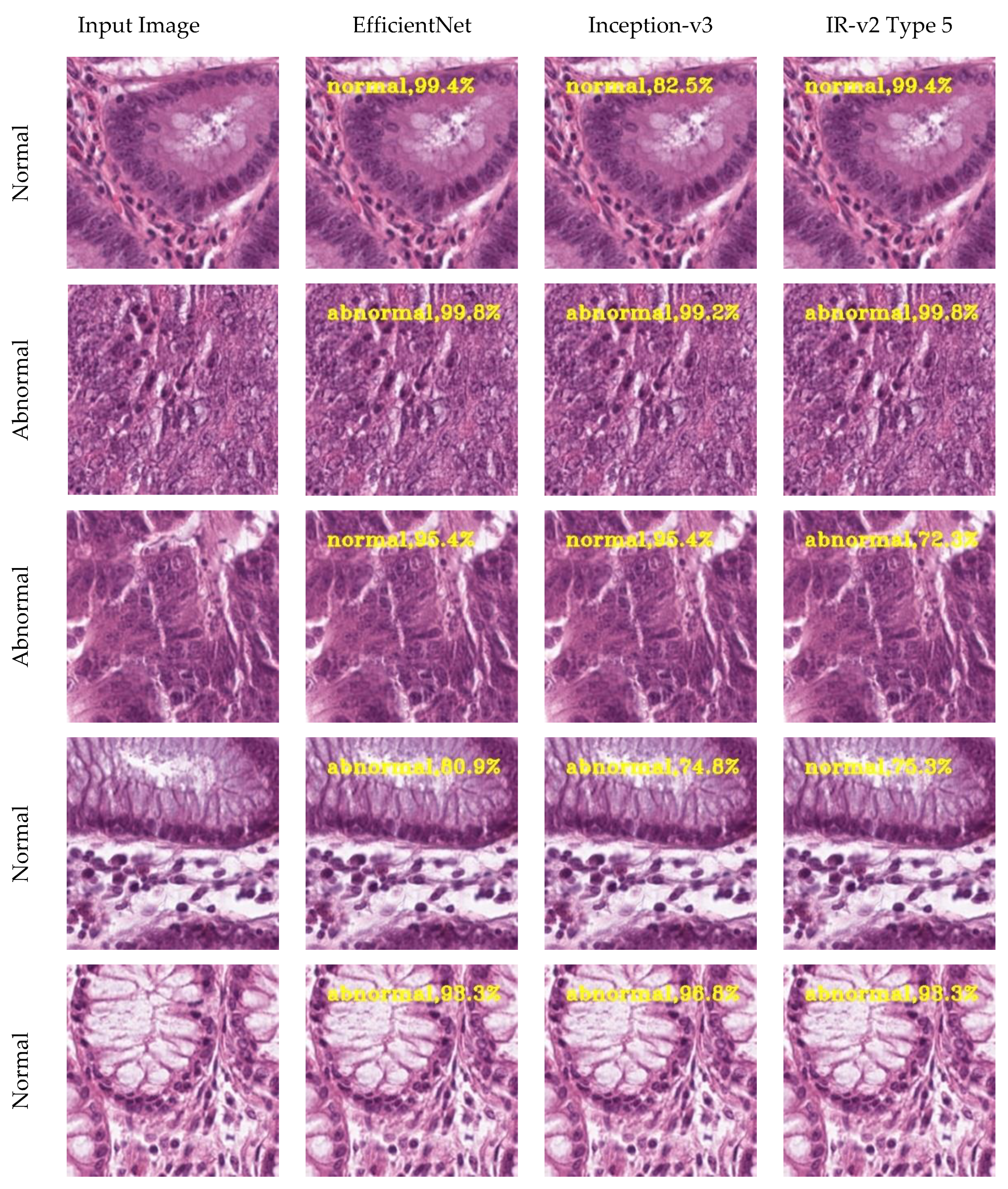
4.4.1. Classification Results
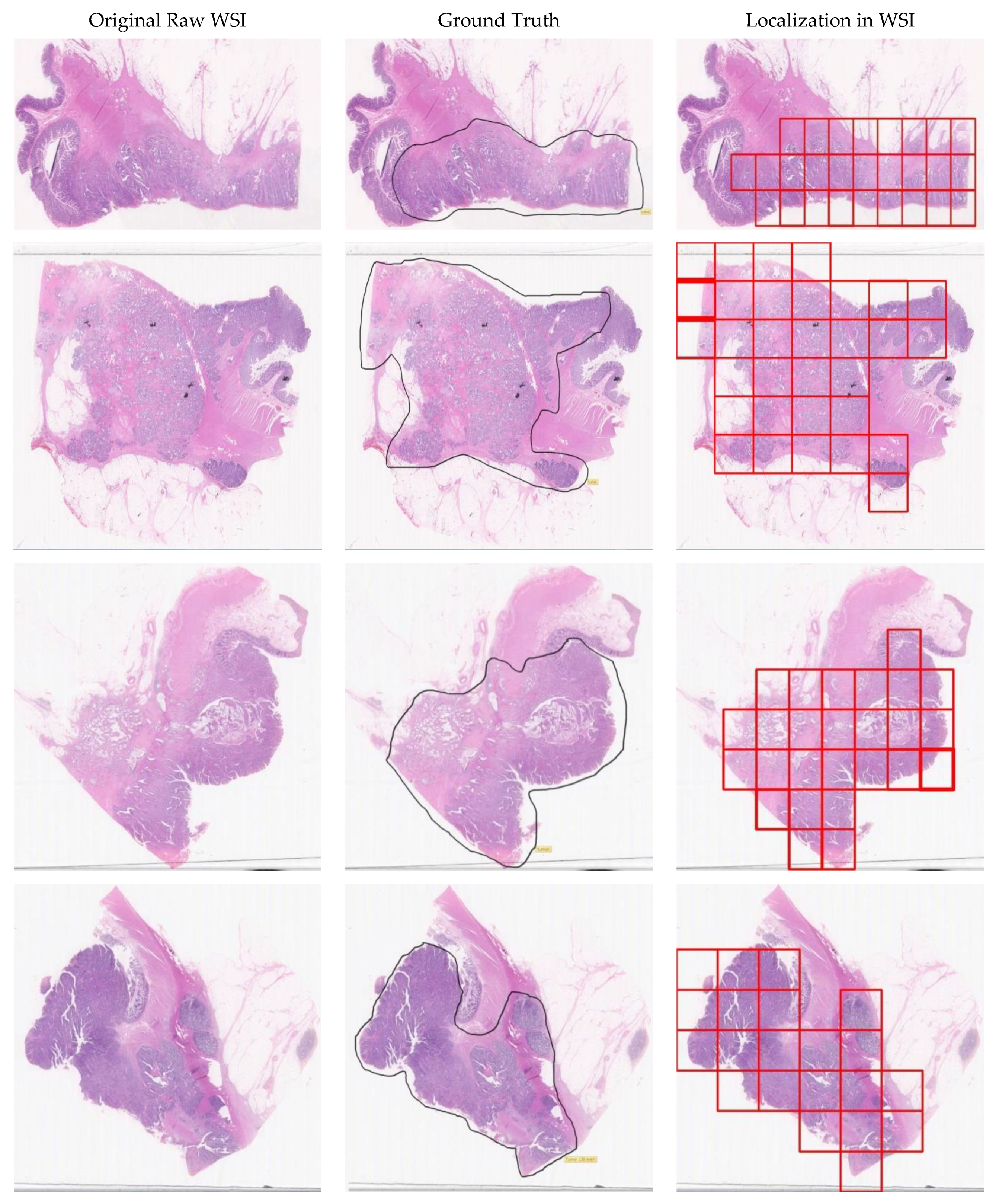
4.4.2. Localization Results
5. Discussion
5.1. Comparison with Previous Works in the Same Domain
5.2. Comparison of Different CNN Architectures Taking Public Dataset
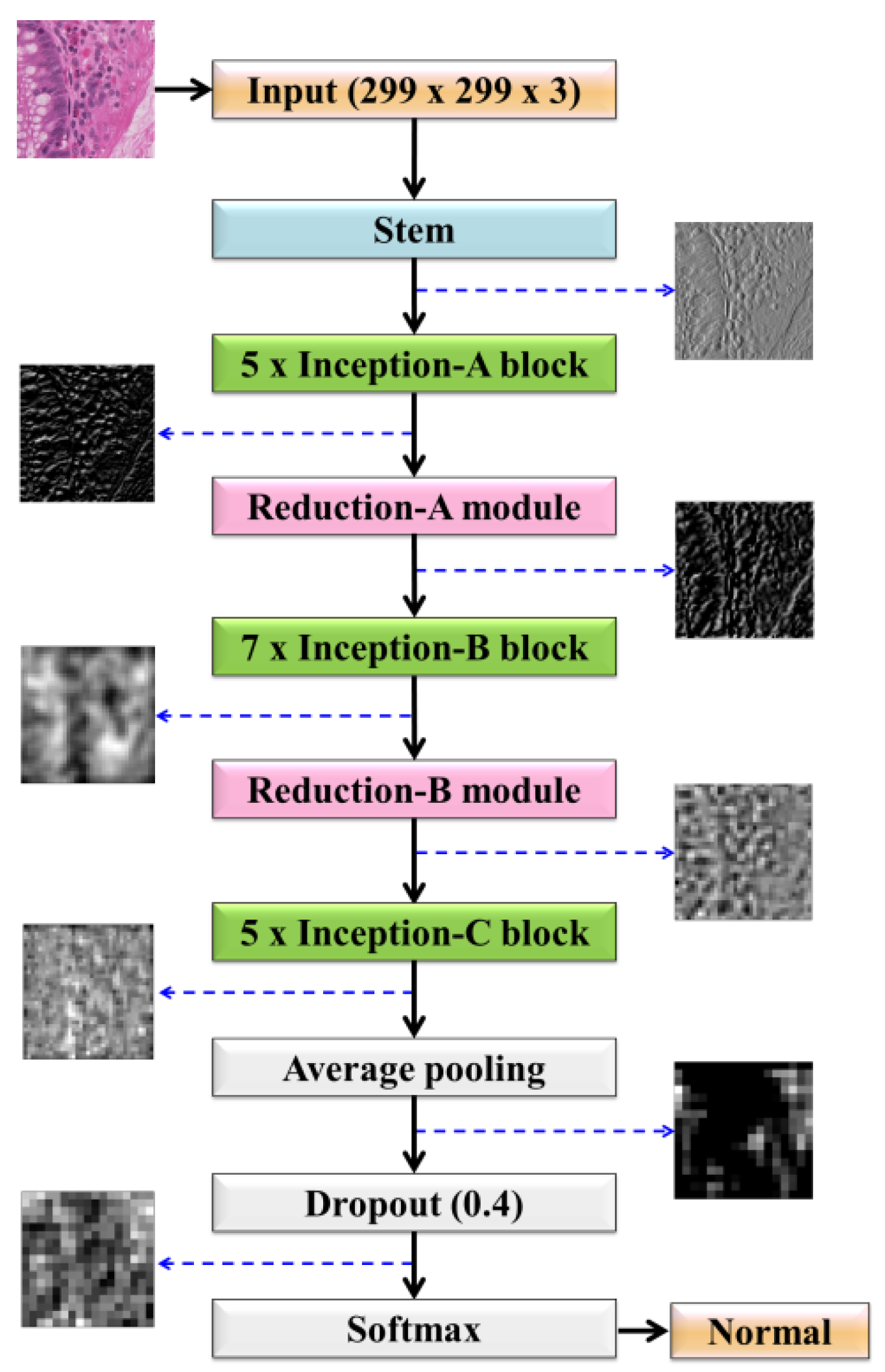
5.3. Processing Time and Visualization of Intermediate Outputs
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar]
- Taiwan News 2020. Available online: www.taiwannews.com.tw/en/news/3948748 (accessed on 12 August 2020).
- Wieslander, H.; Harrison, P.J.; Skogberg, G.; Jackson, S.; Friden, M.; Karlsson, J.; Spjuth, O.; Wahlby, C. Deep learning with conformal prediction for hierarchical analysis of large-scale whole-slide tissue images. IEEE J. Biomed. Heal. Inform. 2021, 25, 371–380. [Google Scholar] [CrossRef]
- Cruz, J.A.; Wishart, D.S. Applications of machine learning in cancer prediction and prognosis. Cancer Inform. 2006, 2, 59–77. [Google Scholar] [CrossRef]
- Komura, D.; Ishikawa, S. Machine learning methods for histopathological image analysis. Comput. Struct. Biotechnol. J. 2018, 16, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.; Tang, J.; Wang, Z.; Zhang, K.; Zhang, L.; Sun, Q. Deep learning for image-based cancer detection and diagnosis—A survey. Pattern Recognit. 2018, 83, 134–149. [Google Scholar] [CrossRef]
- Srinidhi, C.L.; Ciga, O.; Martel, A.L. Deep neural network models for computational histopathology: A survey. Med. Image Anal. 2020, 67, 101813. [Google Scholar] [CrossRef] [PubMed]
- Malik, J.; Kiranyaz, S.; Kunhoth, S.; Ince, T.; Al-Maadeed, S.; Hamila, R.; Gabbouj, M. Colorectal cancer diagnosis from histology images: A comparative study. arXiv 2019, arXiv:1903.11210. [Google Scholar]
- Korbar, B.; Olofson, A.M.; Miraflor, A.P.; Nicka, C.M.; Suriawinata, M.A.; Torresani, L.; Suriawinata, A.A.; Hassanpour, S. Deep learning for classification of colorectal polyps on whole-slide images. J. Pathol. Inform. 2017, 8, 30. [Google Scholar] [PubMed]
- Deng, J.; Dong, W.; Socher, R.; Li, L.J.; Li, K.; Fei-Fei, L. Imagenet: A large-scale hierarchical image database. In Proceedings of the 2009 IEEE Conference on Computer Vision and Pattern Recognition, Miami, FL, USA, 20–25 June 2009; pp. 248–255. [Google Scholar]
- Raghu, M.; Zhang, C.; Kleinberg, J.; Bengio, S. Transfusion: Understanding transfer learning for medical imaging. arXiv 2019, arXiv:1902.07208. [Google Scholar]
- Munien, C.; Viriri, S. Classification of hematoxylin and eosin-stained breast cancer histology microscopy images using transfer learning with EfficientNets. Comput. Intell. Neurosci. 2021, 2021, 1–17. [Google Scholar] [CrossRef]
- Alzubaidi, L.; Fadhel, M.A.; Al-Shamma, O.; Zhang, J.; Santamaría, J.; Duan, Y.; Oleiwi, S.R. Towards a better understanding of transfer learning for medical imaging: A case study. Appl. Sci. 2020, 10, 4523. [Google Scholar] [CrossRef]
- Alzubaidi, L.; Al-Shamma, O.; Fadhel, M.A.; Farhan, L.; Zhang, J.; Duan, Y. Optimizing the performance of breast cancer classification by employing the same domain transfer learning from hybrid deep convolutional neural network model. Electronics 2020, 9, 445. [Google Scholar] [CrossRef] [Green Version]
- Alzubaidi, L.; Al-Amidie, M.; Al-Asadi, A.; Humaidi, A.J.; Al-Shamma, O.; Fadhel, M.A.; Zhang, J.; Santamaría, J.; Duan, Y. Novel transfer learning approach for medical imaging with limited labeled data. Cancers 2021, 13, 1590. [Google Scholar] [CrossRef]
- Géron, A. Hands-on Machine Learning with Scikit-Learn, Keras, and TensorFlow: Concepts, Tools, and Techniques to Build Intelligent Systems; O’Reilly Media: Newton, MA, USA, 2019. [Google Scholar]
- Sudha, V.; Ganeshbabu, T.R. A convolutional neural network classifier VGG-19 architecture for lesion detection and grading in diabetic retinopathy based on deep learning. Comput. Mater. Contin. 2021, 66, 827–842. [Google Scholar] [CrossRef]
- Yu, X.; Kang, C.; Guttery, D.S.; Kadry, S.; Chen, Y.; Zhang, Y.D. ResNet-SCDA-50 for breast abnormality classification. IEEE/ACM Trans. Comput. Biol. Bioinform. 2021, 18, 94–102. [Google Scholar] [CrossRef] [PubMed]
- Dong, N.; Zhao, L.; Wu, C.H.; Chang, J.F. Inception v3 based cervical cell classification combined with artificially extracted features. Appl. Soft Comput. 2020, 93. [Google Scholar] [CrossRef]
- Szegedy, C.; Vanhoucke, V.; Ioffe, S.; Shlens, J.; Wojna, Z. Rethinking the inception architecture for computer vision. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Seattle, WA, USA, 14–19 June 2020; pp. 2818–2826. [Google Scholar]
- Szegedy, C.; Ioffe, S.; Vanhoucke, V.; Alemi, A. Inception-ResNet and the impact of residual connections on learning. arXiv 2016, arXiv:1602.07261. [Google Scholar]
- Deroulers, C.; Ameisen, D.; Badoual, M.; Gerin, C.; Granier, A.; Lartaud, M. Analyzing huge pathology images with open source software. Diagn. Pathol. 2013, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedman, J.; Hastie, T.; Tibshirani, R. The Elements of Statistical Learning; Springer Series in Statistics: New York, NY, USA, 2001; Volume 1. [Google Scholar]
- Olson, D.L.; Delen, D. Advanced Data Mining Techniques; Springer Science & Business Media: Berlin, Germany, 2008. [Google Scholar]
- Boughorbel, S.; Jarray, F.; El-Anbari, M. Optimal classifier for imbalanced data using matthews correlation coefficient metric. PLoS ONE 2017, 12, e0177678. [Google Scholar] [CrossRef]
- Fawcett, T. An introduction to ROC analysis. Pattern Recognit. Lett. 2006, 27, 861–874. [Google Scholar] [CrossRef]
- Zhang, E.; Zhang, Y. Average precision. In Encyclopedia of Database Systems; Liu, L., ÖZsu, M.T., Eds.; Springer US: Boston, MA, USA, 2009; pp. 192–193. [Google Scholar] [CrossRef]
- OpenCV Documentation. Available online: https://docs.opencv.org/master/index.html (accessed on 11 March 2018).
- Abadi, M.; Barham, P.; Chen, J.; Chen, Z.; Davis, A.; Dean, J.; Devin, M.; Ghemawat, S.; Irving, G.; Isard, M.; et al. TensorFlow: Large-Scale Machine Learning on Heterogeneous Systems. 2015. Available online: https://www.tensorflow.org/ (accessed on 15 May 2016).
- Onthoni, D.D.; Sheng, T.-W.; Sahoo, P.K.; Wang, L.-J.; Gupta, P. Deep learning assisted localization of polycystic kidney on contrast-enhanced CT images. Diagnostics 2020, 10, 1113. [Google Scholar] [CrossRef] [PubMed]
- Gupta, P.; Chiang, S.-F.; Sahoo, P.K.; Mohapatra, S.K.; You, J.-F.; Onthoni, D.D.; Hung, H.-Y.; Chiang, J.-M.; Huang, Y.; Tsai, W.-S. Prediction of colon cancer stages and survival period with machine learning approach. Cancers 2019, 11, 2007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rathore, S.; Hussain, M.; Khan, A. Automated colon cancer detection using hybrid of novel geometric features and some traditional features. Comput Biol Med 2015, 65, 279–296. [Google Scholar] [CrossRef] [PubMed]
- Deng, S.J.; Zhang, X.; Yan, W.; Chang, E.I.C.; Fan, Y.B.; Lai, M.D.; Xu, Y. Deep learning in digital pathology image analysis: A survey. Front. Med. 2020, 14, 470–487. [Google Scholar] [CrossRef] [PubMed]
- Lakshmi, V.V.; Jasmine, J.S.L. A hybrid artificial intelligence model for skin cancer diagnosis. Comput. Syst. Sci. Eng. 2021, 37, 233–245. [Google Scholar]
- Farris, A.B.; Vizcarra, J.; Amgad, M.; Cooper, L.A.D.; Gutman, D.; Hogan, J. Artificial intelligence and algorithmic computational pathology: An introduction with renal allograft examples. Histopathology 2021, 78, 791–804. [Google Scholar] [CrossRef]
- Onder, D.; Sarioglu, S.; Karacali, B. Automated labelling of cancer textures in colorectal histopathology slides using quasi-supervised learning. Micron 2013, 47, 33–42. [Google Scholar] [CrossRef] [Green Version]
- Kather, J.N.; Weis, C.A.; Bianconi, F.; Melchers, S.M.; Schad, L.R.; Gaiser, T.; Marx, A.; Zollner, F.G. Multi-class texture analysis in colorectal cancer histology. Sci. Rep. 2016, 6. [Google Scholar] [CrossRef]
- Shapcott, M.; Hewitt, K.J.; Rajpoot, N. Deep learning with sampling in colon cancer histology. Front. Bioeng. Biotechnol. 2019, 7. [Google Scholar] [CrossRef] [Green Version]
- Xu, J.; Luo, X.F.; Wang, G.H.; Gilmore, H.; Madabhushi, A. A deep convolutional neural network for segmenting and classifying epithelial and stromal regions in histopathological images. Neurocomputing 2016, 191, 214–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoon, H.; Lee, J.; Oh, J.E.; Kim, H.R.; Lee, S.; Chang, H.J.; Sohn, D.K. Tumor identification in colorectal histology images using a convolutional neural network. J. Digit. Imaging 2019, 32, 131–140. [Google Scholar] [CrossRef]
- Xu, Y.; Jia, Z.P.; Wang, L.B.; Ai, Y.Q.; Zhang, F.; Lai, M.D.; Chang, E.I.C. Large scale tissue histopathology image classification, segmentation, and visualization via deep convolutional activation features. BMC Bioinform. 2017, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bychkov, D.; Linder, N.; Turkki, R.; Nordling, S.; Kovanen, P.E.; Verrill, C.; Walliander, M.; Lundin, M.; Haglund, C.; Lundin, J. Deep learning based tissue analysis predicts outcome in colorectal cancer. Sci. Rep. 2018, 8. [Google Scholar] [CrossRef]
- Iizuka, O.; Kanavati, F.; Kato, K.; Rambeau, M.; Arihiro, K.; Tsuneki, M. Deep learning models for histopathological classification of gastric and colonic epithelial tumours. Sci. Rep. 2020, 10. [Google Scholar] [CrossRef] [Green Version]
- Wang, K.-S.; Yu, G.; Xu, C.; Meng, X.-H.; Zhou, J.; Zheng, C.; Deng, Z.; Shang, L.; Liu, R.; Su, S. Accurate diagnosis of colorectal cancer based on histopathology images using artificial intelligence. BMC Med. 2021, 19, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Kather, J.N.; Halama, N.; Marx, A. 100,000 histological images of human colorectal cancer and healthy tissue. Zenodo10 2018, 5281. [Google Scholar] [CrossRef]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Metrics | VGG16 | ResNet50 | GoogLeNet | Inception-v3 | Inception-v4 | IR-v2 |
|---|---|---|---|---|---|---|
| Sensitivity | 0.99 ± 0.012 | 0.96 ± 0.008 | 0.95 ± 0.011 | 0.97 ± 0.011 | 0.97 ± 0.019 | 0.94 ± 0.032 |
| Specificity | 0.92 ± 0.013 | 0.96 ± 0.019 | 0.97 ± 0.011 | 0.96 ± 0.014 | 0.95 ± 0.003 | 0.96 ± 0.023 |
| Precision | 0.97 ± 0.013 | 0.96 ± 0.019 | 0.97 ± 0.011 | 0.96 ± 0.008 | 0.95 ± 0.003 | 0.97 ± 0.025 |
| Accuracy | 0.95 ± 0.00 | 0.96 ± 0.004 | 0.96 ± 0.00 | 0.96 ± 0.010 | 0.96 ± 0.008 | 0.95 ± 0.005 |
| F-score | 0.95 ± 0.00 | 0.96 ± 0.004 | 0.96 ± 0.00 | 0.97 ± 0.005 | 0.96 ± 0.008 | 0.95 ± 0.005 |
| MCC | 0.94 ± 0.014 | 0.93 ± 0.005 | 0.91 ± 0.015 | 0.93 ± 0.005 | 0.93 ± 0.018 | 0.89 ± 0.003 |
| AP | 0.91 ± 0.003 | 0.95 ± 0.013 | 0.96 ± 0.003 | 0.95 ± 0.009 | 0.95 ± 0.018 | 0.96 ± 0.01 |
| Metrics | VGG16 | ResNet50 | GoogLeNet | Inception-v3 | Inception-v4 | IR-v2 |
|---|---|---|---|---|---|---|
| Sensitivity | 0.82 ± 0.021 | 0.86 ± 0.018 | 0.88 ± 0.031 | 0.99 ± 0.014 | 0.99 ± 0.009 | 0.99 ± 0.014 |
| Specificity | 0.98 ± 0.031 | 0.69 ± 0.023 | 0.67 ± 0.031 | 0.88 ± 0.014 | 0.65 ± 0.013 | 0.95 ± 0.023 |
| Precision | 0.97 ± 0.031 | 0.83 ± 0.023 | 0.85 ± 0.031 | 0.89 ± 0.028 | 0.88 ± 0.053 | 0.95 ± 0.031 |
| Accuracy | 0.90 ± 0.001 | 0.78 ± 0.014 | 0.82 ± 0.018 | 0.94 ± 0.011 | 0.82 ± 0.048 | 0.97 ± 0.014 |
| F-score | 0.89 ± 0.002 | 0.79 ± 0.009 | 0.86 ± 0.192 | 0.94 ± 0.015 | 0.84 ± 0.048 | 0.97 ± 0.024 |
| MCC | 0.74 ± 0.019 | 0.61 ± 0.005 | 0.64 ± 0.025 | 0.93 ± 0.015 | 0.8 ± 0.018 | 0.97 ± 0.021 |
| AP | 0.89 ± 0.013 | 0.71 ± 0.017 | 0.74 ± 0.013 | 0.89 ± 0.019 | 0.74 ± 0.018 | 0.96 ± 0.014 |
| Parameter | Value |
|---|---|
| Batch size | 128 |
| # of epochs | 50 |
| Optimizer | Adam |
| Momentum | 0.9 |
| Learning rate | 0.0008 |
| Dropout | 0.4 |
| Metrics | IR-v2 Type 1 | IR-v2 Type 2 | IR-v2 Type 3 | IR-v2 Type 4 | IR-v2 Type 5 |
|---|---|---|---|---|---|
| Sensitivity | 0.99 ± 0.014 | 1.00 ± 0.054 | 0.99 ± 0.064 | 0.97 ± 0.012 | 0.99 ± 0.002 |
| Specificity | 0.95 ± 0.023 | 0.76 ± 0.038 | 0.78 ± 0.064 | 0.97 ± 0.011 | 0.99 ± 0.004 |
| Precision | 0.95 ± 0.031 | 0.88 ± 0.044 | 0.90 ± 0.054 | 0.97 ± 0.012 | 0.99 ± 0.003 |
| Accuracy | 0.97 ± 0.014 | 0.88 ± 0.054 | 0.89 ± 0.034 | 0.97 ± 0.010 | 0.99 ± 0.005 |
| F-score | 0.97 ± 0.024 | 0.89 ± 0.044 | 0.90 ± 0.064 | 0.97 ± 0.010 | 0.99 ± 0.005 |
| MCC | 0.97 ± 0.021 | 0.87 ± 0.044 | 0.87 ± 0.032 | 0.94 ± 0.014 | 0.99 ± 0.003 |
| AP | 0.96 ± 0.014 | 0.81 ± 0.054 | 0.82 ± 0.052 | 0.96 ± 0.014 | 0.99 ± 0.001 |
| Reference | Method | Results |
|---|---|---|
| [32] | ML-based feature extraction | Accuracy: 98.07% |
| [36] | Quasi supervised learning | Accuracy: 95% |
| [37] | Multi-class texture analysis | Accuracy: 84% |
| [39] | DCNN | Accuracy: 100% F1-score: 100% MCC: 100% |
| [40] | VGG-variant | Accuracy: 93.48% Sensitivity: 95.1% Specificity: 92.76% |
| [41] | AlexNet | Accuracy: 97.5% |
| [42] | VGG16 + LSTM | AUC: 0.69 |
| [43] | CNN + RNN | AUC: 0.99 |
| [44] | Inception-v3 | AUC: 0.988 |
| Proposed model | IR-v2 Type 5 | AUC: 0.99 |
| Metrics | EfficientNet [12] | Inception-v3 [44] | IR-v2 Type 5 |
|---|---|---|---|
| Sensitivity | 75% | 78% | 87% |
| Specificity | 92% | 93% | 95% |
| Precision | 94% | 95% | 96% |
| Accuracy | 82% | 84% | 90% |
| F-score | 84% | 86% | 91% |
| Type of Time | Durations |
|---|---|
| Training time | 5 days, 7 h, 12 min, 38 s |
| Single epoch execution time | 2 h, 17 min, 21 s |
| Single image testing time | 0.58 s |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gupta, P.; Huang, Y.; Sahoo, P.K.; You, J.-F.; Chiang, S.-F.; Onthoni, D.D.; Chern, Y.-J.; Chao, K.-Y.; Chiang, J.-M.; Yeh, C.-Y.; et al. Colon Tissues Classification and Localization in Whole Slide Images Using Deep Learning. Diagnostics 2021, 11, 1398. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11081398
Gupta P, Huang Y, Sahoo PK, You J-F, Chiang S-F, Onthoni DD, Chern Y-J, Chao K-Y, Chiang J-M, Yeh C-Y, et al. Colon Tissues Classification and Localization in Whole Slide Images Using Deep Learning. Diagnostics. 2021; 11(8):1398. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11081398
Chicago/Turabian StyleGupta, Pushpanjali, Yenlin Huang, Prasan Kumar Sahoo, Jeng-Fu You, Sum-Fu Chiang, Djeane Debora Onthoni, Yih-Jong Chern, Kuo-Yu Chao, Jy-Ming Chiang, Chien-Yuh Yeh, and et al. 2021. "Colon Tissues Classification and Localization in Whole Slide Images Using Deep Learning" Diagnostics 11, no. 8: 1398. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11081398