
Patient-Reported Outcomes and Preferences for Colon Capsule Endoscopy and Colonoscopy: A Systematic Review with Meta-Analysis

 , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Inclusion and Exclusion Criteria
- full text articles;
- articles reporting PRO after undergoing both COC and CCE or randomized controlled trials (RCT);
- articles in English/Danish/Italian/French/Spanish language.
- non-RCT articles in which patients underwent either COC or CCE alone;
- the following article types: reviews, conference papers, case reports.
2.3. Screening of References
2.4. Data Extraction
2.5. Study Assessment and Risk of Bias
2.6. Statistical Analysis
3. Results
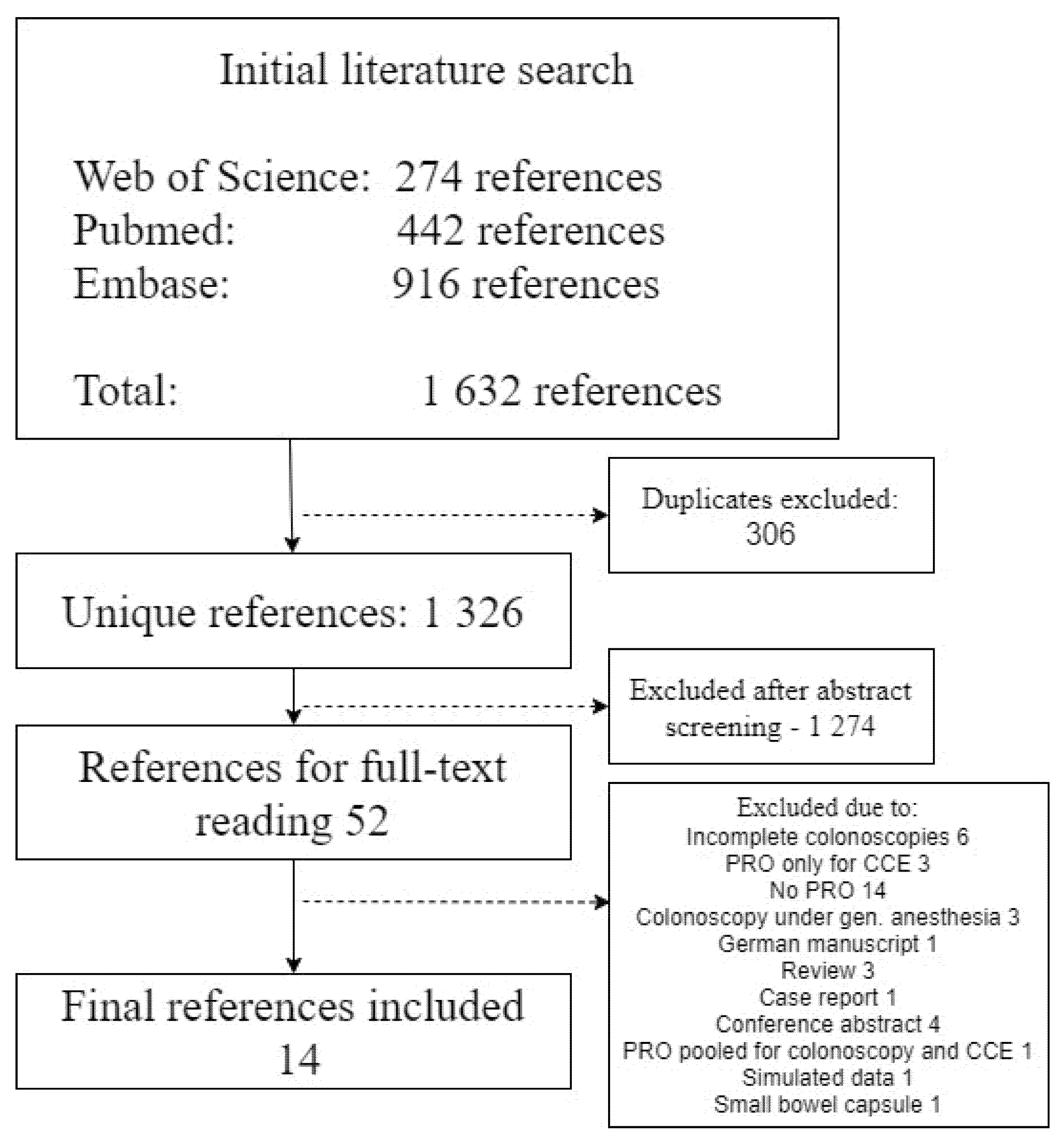
3.1. Search
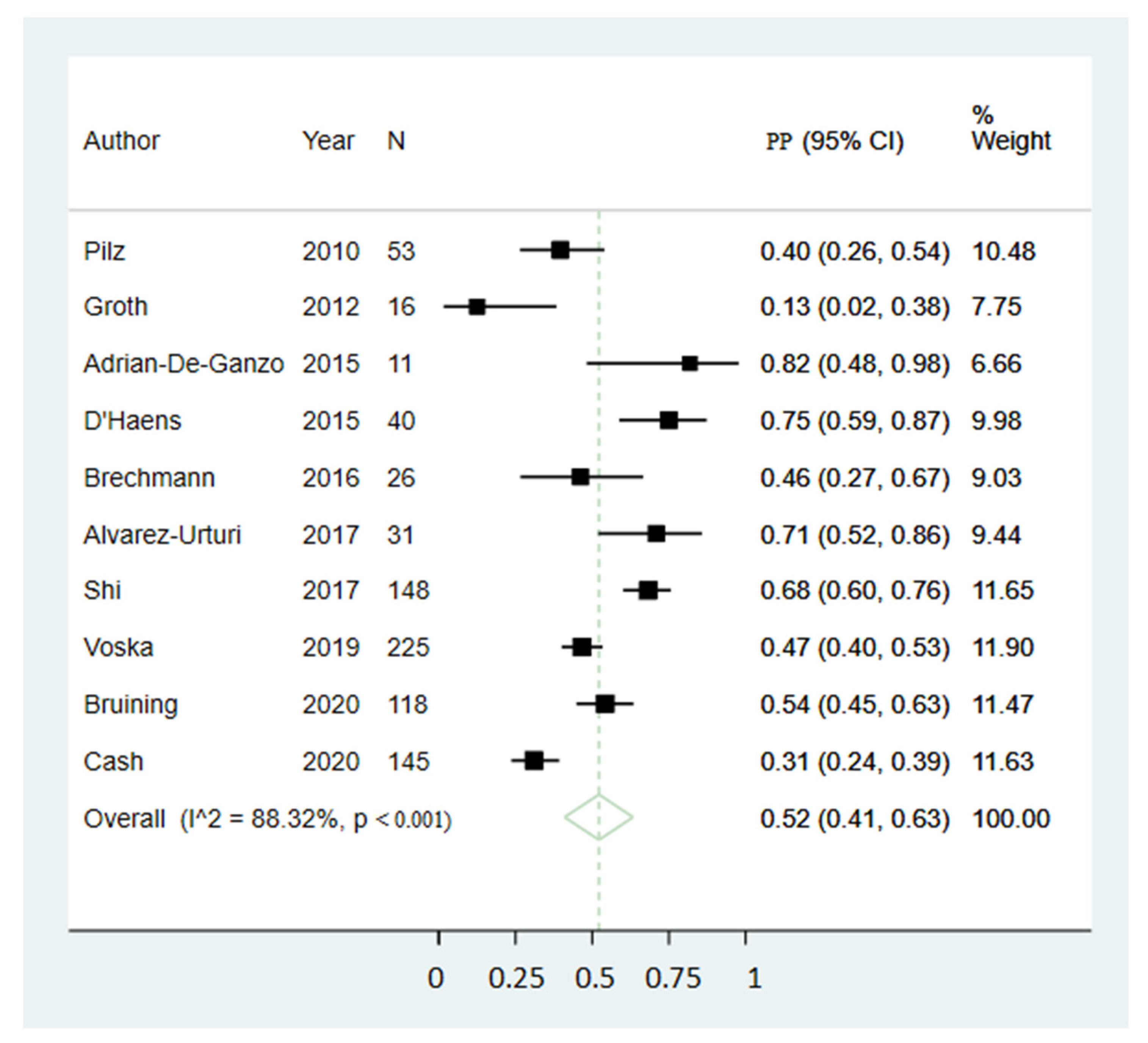
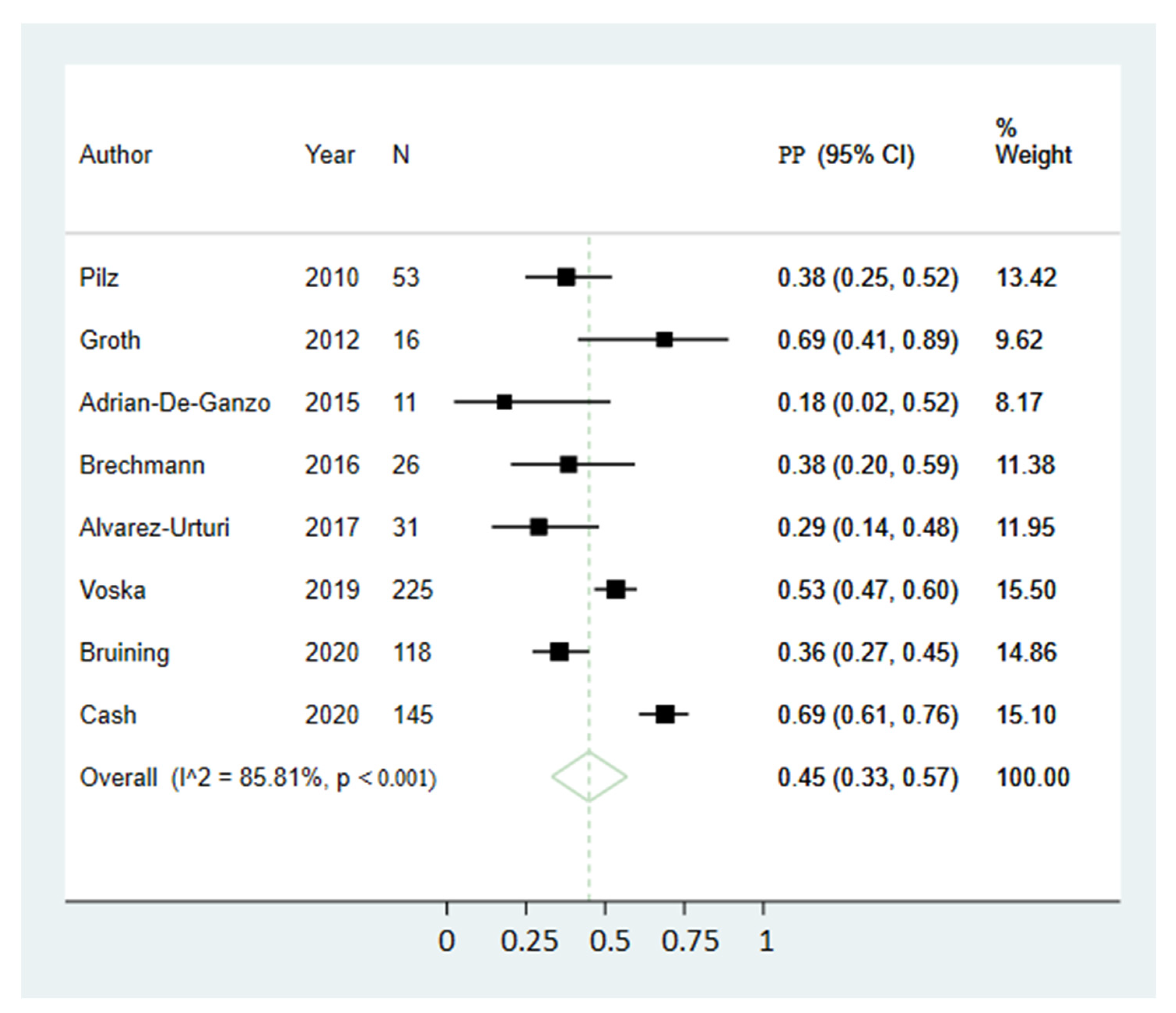
3.2. Patient Preference
3.3. Adverse Events
3.4. Tolerability
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix A.1. PICO

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Investigation | Comparator | Outcome |
|---|---|---|
| Capsule camera* Wireless camera* Wireless camera endoscop* WCE CCE Colon capsule endoscop* PillCam* Pill Cam* Camera pill* Capsule endoscop* Endoscop*, Capsule Wireless Capsule Endoscop* Capsule Endoscop*, Wireless Endoscop*, Wireless Capsule Video Capsule Endoscop* Capsule Endoscop*, Video Capsule Endoscopy, Video Endoscop*, Video Capsule Pan-enteric capsule endoscop* | Colonoscopy(MESH) Colonoscop* Colonoscopic Surgical Procedure* Procedure*, Colonoscopic Surgical Surgical Procedure*, Colonoscopic Surger*, Colonoscopic Surgical Procedure*, Colonoscopic Colonoscopic Surger* Colonoscopes(MESH) Colonoscope* | Patient-related outcome Patient acceptance of health care(MESH) Health Care Utilization Utilization, Health Care Patient Acceptance of Healthcare Healthcare Patient Acceptance* Nonacceptor* of Health Care Care Nonacceptor*, Health Health Care Nonacceptor* Health Care Seeking Behavior Acceptor* of Health Care Care Acceptor*, Health Health Care Acceptor* Health Care Acceptabili* Acceptability of Healthcare Healthcare Acceptabilit* Patient satisfaction(MESH) Patient preference(MESH) Patient Preference*. patient Patient comfort(MESH) Comfort, patient Comfort care Care, comfort Patient Confidence Tolerance Compliance Preference Patient-reported treatment outcome Patient-reported patientreported Self-reported Selfreported Interview* Questionnaire* Adverse event* Minor complication* Major complication* Complication* Adverse effect* Adverse reaction* PROM* |
Appendix A.2. Search Strings
Appendix B
| Author, Year | Checklist | Evaluation |
|---|---|---|
| Alvarez-Urturi, 2017 | STROBE | Medium |
| Brechmann, 2016 | STROBE | Medium |
| Bruining, 2020 | STROBE | High |
| D’Haens, 2015 | STROBE | High |
| Eliakim, 2010 | STROBE | High |
| Fiorillo, 2020 | STROBE | High |
| Groth, 2012 | STROBE | Medium |
| Meister, 2013 | STROBE | Medium |
| Pilz, 2010 | STROBE | High |
| Shi, 2017 | STROBE | High |
| Thygesen, 2019 | STROBE | High |
| Voska, 2019 | STROBE | High |
| Adrian-De-Ganzo, 2015 | RoB | High (low risk of bias) |
| Cash, 2020 | RoB | High (low risk of bias) |
References
- Moore, J.S.; Aulet, T.H. Colorectal Cancer Screening. Surg. Clin. N. Am. 2017, 97, 487–502. [Google Scholar] [CrossRef] [PubMed]
- Burtin, P.; Bour, B.; Charlois, T.; Ruget, O.; Calès, P.; Dauver, A.; Boyer, J. Colonic investigations in the elderly: Colonoscopy or barium enema? Aging Clin. Exp. Res. 1995, 7, 190–194. [Google Scholar] [CrossRef] [PubMed]
- Winawer, S.J.; Fletcher, R.H.; Miller, L.; Godlee, F.; Stolar, M.H.; Mulrow, C.D.; Woolf, S.H.; Glick, S.N.; Ganiats, T.G.; Bond, J.H.; et al. Colorectal cancer screening: Clinical guidelines and rationale. Gastroenterology 1997, 112, 594–642. [Google Scholar] [CrossRef] [PubMed]
- Anderson, M.L.; Heigh, R.I.; McCoy, G.A.; Parent, K.; Muhm, J.R.; McKee, G.S.; Eversman, W.G.; Collins, J.M. Accuracy of assessment of the extent of examination by experienced colonoscopists. Gastrointest. Endosc. 1992, 38, 560–563. [Google Scholar] [CrossRef]
- Moglia, A.; Menciassi, A.; Schurr, M.O.; Dario, P. Wireless capsule endoscopy: From diagnostic devices to multipurpose robotic systems. Biomed. Microdevices 2006, 9, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Eliakim, R.; Fireman, Z.; Gralnek, I.M.; Yassin, K.; Waterman, M.; Kopelman, Y.; Lachter, J.; Koslowsky, B.; Adler, S.N. Evaluation of the PillCam Colon capsule in the detection of colonic pathology: Results of the first multicenter, prospective, comparative study. Endoscopy 2006, 38, 963–970. [Google Scholar] [CrossRef]
- Eliakim, R.; Yassin, K.; Niv, Y.; Metzger, Y.; Lachter, J.; Gal, E.; Sapoznikov, B.; Konikoff, F.; Leichtmann, G.; Fireman, Z.; et al. Prospective multicenter performance evaluation of the second-generation colon capsule compared with colonoscopy. Endoscopy 2009, 41, 1026–1031. [Google Scholar] [CrossRef]
- Spada, C.; Hassan, C.; Munoz-Navas, M.; Neuhaus, H.; Deviere, J.; Fockens, P.; Coron, E.; Gay, G.; Toth, E.; Riccioni, M.E.; et al. Second-generation colon capsule endoscopy compared with colonoscopy. Gastrointest. Endosc. 2011, 74, 581–589.e1. [Google Scholar] [CrossRef] [PubMed]
- Koulaouzidis, G.; Robertson, A.; Wenzek, H.; Koulaouzidis, A. Colon capsule endoscopy: The evidence is piling up. Gut 2021. [Google Scholar] [CrossRef]
- Koulaouzidis, A.; Marlicz, W.; Wenzek, H.; Koulaouzidis, G.; Eliakim, R.; Toth, E. Returning to digestive endoscopy normality will be slow and must include novelty and telemedicine. Dig. Liver Dis. 2020, 52, 1099–1101. [Google Scholar] [CrossRef]
- Thygesen, M.K.; Baatrup, G.; Petersen, C.; Qvist, N.; Krøijer, R.; Kobaek-Larsen, M. Screening individuals’ experiences of colonoscopy and colon capsule endoscopy; a mixed methods study. Acta Oncol. 2019, 58, S71–S76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and Elaboration. Ann. Intern. Med. 2007, 147, W-163–W-194. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cumpston, M.; Li, T.; Page, M.; Chandler, J.; Welch, V.A.; Higgins, J.; Thomas, J. Updated guidance for trusted systematic reviews: A new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst. Rev. 2019, 10, ED000142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Nyaga, V.N.; Arbyn, M.; Aerts, M. Metaprop: A Stata command to perform meta-analysis of binomial data. Arch. Public Health 2014, 72, 39. [Google Scholar] [CrossRef] [Green Version]
- Adrián-De-Ganzo, Z.; Alarcón-Fernández, O.; Ramos, L.; Gimeno-Garcia, A.Z.; Alonso-Abreu, I.; Carrillo, M.; Quintero, E. Uptake of Colon Capsule Endoscopy vs. Colonoscopy for Screening Relatives of Patients With Colorectal Cancer. Clin. Gastroenterol. Hepatol. 2015, 13, 2293–2301.e1. [Google Scholar] [CrossRef] [Green Version]
- Alvarez-Urturi, C.; Fernández-Esparrach, M.G.; Ibáñez, I.A.; de Miguel, C.R.; Dedeu, J.M.; Bessa, X.; Córdova, H.; Pellise, M.; Balaguer, F.; Ginès, A.; et al. Accuracy of Colon Capsule Endoscopy in Detecting Colorectal Polyps in Individuals with Familial Colorectal Cancer: Could We Avoid Colonoscopies? Gastroenterol. Res. Pract. 2017, 2017, 1507914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brechmann, T.; Schmiegel, W.; Klute, L.; Rösch, T.; Pox, C. Feasibility of a colon capsule overnight procedure followed by colonoscopy. Z. Für Gastroenterol. 2016, 54, 146–151. [Google Scholar] [CrossRef]
- Bruining, D.H.; Oliva, S.; Fleisher, M.R.; Fischer, M.; Fletcher, J.G. Panenteric capsule endoscopy versus ileocolonoscopy plus magnetic resonance enterography in Crohn’s disease: A multicentre, prospective study. BMJ Open Gastroenterol. 2020, 7, e000365. [Google Scholar] [CrossRef]
- Cash, B.D.; Fleisher, M.R.; Fern, S.; Rajan, E.; Haithcock, R.; Kastenberg, D.M.; Pound, D.; Papageorgiou, N.P.; Fernández-Urién, I.; Schmelkin, I.J.; et al. Multicentre, prospective, randomised study comparing the diagnostic yield of colon capsule endoscopy versus CT colonography in a screening population (the TOPAZ study). Gut 2020. [Google Scholar] [CrossRef] [PubMed]
- D’Haens, G.; Löwenberg, M.; Samaan, M.A.; Franchimont, D.; Ponsioen, C.; Brink, G.R.V.D.; Fockens, P.; Bossuyt, P.; Amininejad, L.; Rajamannar, G.; et al. Safety and Feasibility of Using the Second-Generation Pillcam Colon Capsule to Assess Active Colonic Crohn’s Disease. Clin. Gastroenterol. Hepatol. 2015, 13, 1480–1486.e3. [Google Scholar] [CrossRef] [PubMed]
- Eliakim, R.; Yassin, K.; Niv, Y.; Metzger, Y.; Lachter, J.; Ga, E.; Sapoznikov, B.; Konikoff, F.; Leichtmann, G.; Fireman, Z.; et al. Ergebnisse eines prospektiven Multizentervergleichs der 2. Kolonkapselgeneration mit der Koloskopie. Endosk. Heute 2010, 23, 144–149. [Google Scholar] [CrossRef]
- Fiorillo, C.; Quero, G.; Longo, F.; Mascagni, P.; Delvaux, M.; Mutter, D. Capsule Endoscopy Versus Colonoscopy in Patients with Previous Colorectal Surgery: A Prospective Comparative Study. Gastroenterol. Res. 2020, 13, 217–224. [Google Scholar]
- Groth, S.; Krause, H.; Behrendt, R.; Hill, H.; Börner, M.; Bastürk, M.; Plathner, N.; Schütte, F.; Gauger, U.; Riemann, J.F.; et al. Capsule colonoscopy increases uptake of colorectal cancer screening. BMC Gastroenterol. 2012, 12, 80. [Google Scholar] [CrossRef] [Green Version]
- Meister, T.; Heinzow, H.S.; Domagk, D.; Dortgolz, A.; Lenze, F.; Ross, M.; Domschke, W.; Lügering, A. Colon capsule endoscopy versus standard colonoscopy in assessing disease activity of ulcerative colitis: A prospective trial. Tech. Coloproctol. 2013, 17, 641–646. [Google Scholar] [CrossRef]
- Pilz, J.B.; Portmann, S.; Peter, S.; Beglinger, C.; Degen, L. Colon Capsule Endoscopy compared to Conventional Colonoscopy under routine screening conditions. BMC Gastroenterol. 2010, 10, 66. [Google Scholar] [CrossRef] [Green Version]
- Shi, H.Y.; Chan, F.K.; Higashimori, A.; Kyaw, M.; Ching, J.Y.; Chan, H.C.; Chan, J.C.; Chan, A.; Lam, K.L.; Tang, R.S.; et al. A prospective study on second-generation colon capsule endoscopy to detect mucosal lesions and disease activity in ulcerative colitis (with video). Gastrointest. Endosc. 2017, 86, 1139–1146.e6. [Google Scholar] [CrossRef] [PubMed]
- Voska, M.; Grega, T.; Ngo, O.; Buckova, B.; Majek, O.; Vojtechova, G.; Tacheci, I.; Benes, M.; Bures, J.; Spicak, J.; et al. The Comparison of the Efficiency of Colon Capsule Endoscopy and Optical Colonoscopy in Patients with Positive Immunochemical Fecal Occult Blood Test: Multicenter, Prospective Study. Gastrointest. Endosc. 2019, 89 (Suppl. 6), AB399. [Google Scholar] [CrossRef]
- Deding, U.; Bjoersum-Meyer, T.; Kaalby, L.; Kobaek-Larsen, M.; Thygesen, M.K.; Madsen, J.B.; Kroijer, R.; Baatrup, B. Colon capsule endoscopy in colorectal cancer screening: Interim analyses of randomized controlled trial care for colon 2015. Endosc. Int. Open 2021. [Google Scholar]
- Kerrison, R.S.; Sheik-Mohamud, D.; McBride, E.; Whitaker, K.L.; Rees, C.; Duffy, S.; von Wagner, C. Patient barriers and facilitators of colonoscopy use: A rapid systematic review and thematic synthesis of the qualitative literature. Prev. Med. 2021, 145, 106413. [Google Scholar] [CrossRef] [PubMed]
- Garg, R.; Singh, A.; Ahuja, K.R.; Mohan, B.P.; Ravi, S.J.K.; Shen, B.; Kirby, D.F.; Regueiro, M. Risks, time trends, and mortality of colonoscopy-induced perforation in hospitalized patients. J. Gastroenterol. Hepatol. 2020, 35, 1381–1386. [Google Scholar] [CrossRef] [PubMed]
- Panteris, V.; Haringsma, J.; Kuipers, E. Colonoscopy perforation rate, mechanisms and outcome: From diagnostic to therapeutic colonoscopy. Endoscopy 2009, 41, 941–951. [Google Scholar] [CrossRef] [PubMed] [Green Version]




| Author—Year | Country | Study Type | PR CCE Preference | PR COC Preference | PR AE | PR Tolerability |
|---|---|---|---|---|---|---|
| Adrian-De-Ganzo 2015 [18] | Spain | RCT | Yes | Yes | Yes | No |
| Alvarez-Urturi 2017 [19] | Spain | OBS | Yes | Yes | Yes | Yes |
| Brechmann 2016 [20] | Germany | OBS | Yes | Yes | Yes | No |
| Bruining 2020 [21] | USA, Austria, Israel | OBS | Yes | Yes | No | No |
| Cash 2020 [22] | USA | RCT | Yes | Yes | Yes | No |
| D’Haens 2015 [23] | Netherlands, Belgium | OBS | Yes | No | Yes | Yes |
| Eliakim 2010 [24] | Israel | OBS | No | No | Yes | No |
| Fiorillo 2020 [25] | France | OBS | No | No | Yes | Yes |
| Groth 2012 [26] | Germany | OBS | Yes | Yes | Yes | No |
| Meister 2013 [27] | Germany | OBS | No | No | Yes | Yes |
| Pilz 2010 [28] | Switzerland | OBS | Yes | Yes | Yes | No |
| Shi 2017 [29] | Hong Kong | OBS | Yes | No | Yes | Yes |
| Thygesen 2019 [11] | Denmark | OBS | No | No | Yes | Yes |
| Voska 2019 [30] | Czech Republic | OBS | Yes | Yes | Yes | No |
| Colon Capsule Endoscopy | ||||
| Variable | Coefficient | Lower CI 95% | Upper CI 95% | p-value |
| Year published (continuous) | −0.003 | −0.081 | 0.074 | 0.936 |
| Year published (categorical, before vs. after 2016) | −0.058 | −0.517 | 0.401 | 0.804 |
| Sample size (continuous) | −0.002 | −0.004 | 0.001 | 0.319 |
| Study type (RCT vs. OBS) | 0.116 | −0.433 | 0.665 | 0.679 |
| Centers (multi vs. single) | −0.078 | −0.554 | 0.397 | 0.746 |
| Modality of data collection (oral vs. questionnaire) | −0.209 | −0.660 | 0.241 | 0.362 |
| Age mean (continuous) | −0.023 | −0.046 | <0.001 | 0.054 |
| Male percentage (continuous) | −0.013 | −0.042 | 0.015 | 0.366 |
| Completion rate (continuous) | −0.003 | −0.024 | 0.018 | 0.772 |
| Completion rate (categorical) | −0.018 | −0.481 | 0.444 | 0.938 |
| Capsule type (CCE2 vs. CCE1) | 0.190 | −0.363 | 0.742 | 0.501 |
| Capsule type (PillCam Crohn® vs. CCE1) | 0.142 | −0.709 | 0.994 | 0.743 |
| Patient group (symptomatic vs. screening) | −0.045 | −0.856 | 0.766 | 0.913 |
| Patient group (chronic illness vs. screening) | 0.301 | −0.163 | 0.764 | 0.204 |
| Evaluation of study (STROBE/Cochrane) | 0.040 | −0.520 | 0.601 | 0.887 |
| Colonoscopy | ||||
| Variable | Coefficient | Lower CI 95% | Upper CI 95% | p-value |
| Year published (continuous) | 0.010 | −0.063 | 0.083 | 0.797 |
| Year published (categorical, before vs. after 2016) | 0.063 | −0.487 | 0.612 | 0.823 |
| Sample size (continuous) | 0.002 | −0.002 | 0.005 | 0.370 |
| Study type (RCT vs. OBS) | −0.345 | −0.879 | 0.189 | 0.206 |
| Centers (multi vs. single) | −0.017 | −0.609 | 0.575 | 0.955 |
| Modality of data collection (oral vs. questionnaire) | −0.024 | −0.613 | 0.565 | 0.937 |
| Age mean (continuous) | 0.022 | −0.009 | 0.053 | 0.155 |
| Male percentage (continuous) | 0.004 | −0.024 | 0.032 | 0.772 |
| Completion rate (continuous) | 0.057 | −0.035 | 0.150 | 0.223 |
| Completion rate (categorical) | 0.006 | −0.632 | 0.644 | 0.985 |
| Patient group (symptomatic vs. screening) | −0.267 | −1.103 | 0.568 | 0.531 |
| Patient group (chronic illness vs. screening) | −0.345 | −1.033 | 0.343 | 0.326 |
| Evaluation of studies (STROBE/Cochrane) | 0.036 | −0.533 | 0.606 | 0.900 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deding, U.; Cortegoso Valdivia, P.; Koulaouzidis, A.; Baatrup, G.; Toth, E.; Spada, C.; Fernández-Urién, I.; Pennazio, M.; Bjørsum-Meyer, T. Patient-Reported Outcomes and Preferences for Colon Capsule Endoscopy and Colonoscopy: A Systematic Review with Meta-Analysis. Diagnostics 2021, 11, 1730. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11091730
Deding U, Cortegoso Valdivia P, Koulaouzidis A, Baatrup G, Toth E, Spada C, Fernández-Urién I, Pennazio M, Bjørsum-Meyer T. Patient-Reported Outcomes and Preferences for Colon Capsule Endoscopy and Colonoscopy: A Systematic Review with Meta-Analysis. Diagnostics. 2021; 11(9):1730. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11091730
Chicago/Turabian StyleDeding, Ulrik, Pablo Cortegoso Valdivia, Anastasios Koulaouzidis, Gunnar Baatrup, Ervin Toth, Cristiano Spada, Ignacio Fernández-Urién, Marco Pennazio, and Thomas Bjørsum-Meyer. 2021. "Patient-Reported Outcomes and Preferences for Colon Capsule Endoscopy and Colonoscopy: A Systematic Review with Meta-Analysis" Diagnostics 11, no. 9: 1730. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11091730