
Effects of CALR-Mutant Type and Burden on the Phenotype of Myeloproliferative Neoplasms
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Patients
2.2. CALR Mutation Analysis
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. CALR Mutant Types and Their Effects on the Phenotype
3.3. Effects of CALR Mutant Type on Phenotype in ET and PMF
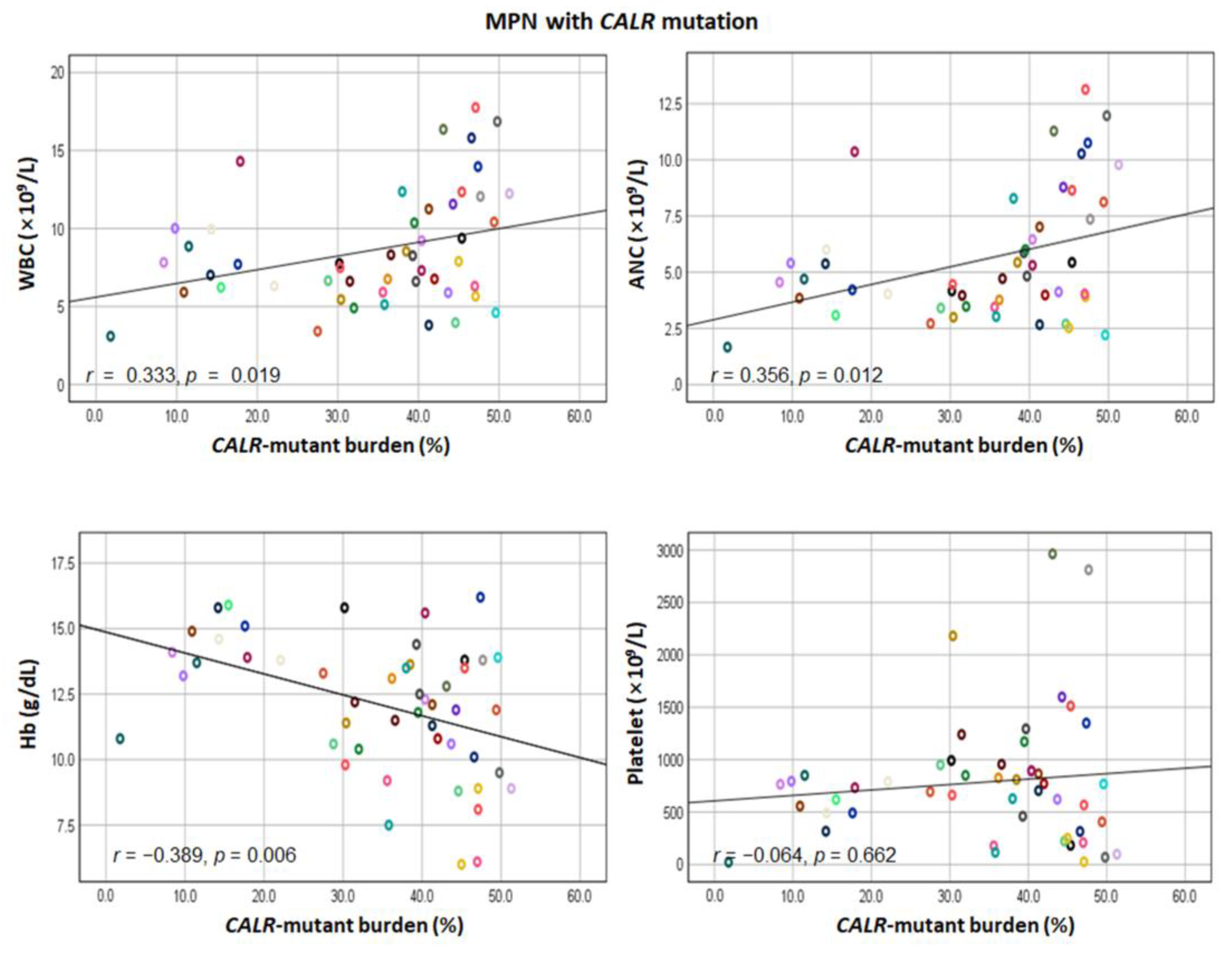
3.4. Correlation between CALR Mutant Burden and Hematological Phenotype in Type 1-like and Type 2-like CALR Mutations
3.5. Correlation of CALR Mutant Burden and Hematological Phenotype in ET and PMF
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Michalak, M.; Groenendyk, J.; Szabo, E.; Gold, L.I.; Opas, M. Calreticulin, a multi-process calcium-buffering chaperone of the endoplasmic reticulum. Biochem. J. 2009, 417, 651–666. [Google Scholar] [CrossRef] [PubMed]
- Klampfl, T.; Gisslinger, H.; Harutyunyan, A.S.; Nivarthi, H.; Rumi, E.; Milosevic, J.D.; Them, N.C.; Berg, T.; Gisslinger, B.; Pietra, D.; et al. Somatic mutations of calreticulin in myeloproliferative neoplasms. N. Engl. J. Med. 2013, 369, 2379–2390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nangalia, J.; Massie, C.E.; Baxter, E.J.; Nice, F.L.; Gundem, G.; Wedge, D.C.; Avezov, E.; Li, J.; Kollmann, K.; Kent, D.G.; et al. Somatic CALR mutations in myeloproliferative neoplasms with nonmutated JAK2. N. Engl. J. Med. 2013, 369, 2391–2405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rotunno, G.; Mannarelli, C.; Guglielmelli, P.; Pacilli, A.; Pancrazzi, A.; Pieri, L.; Fanelli, T.; Bosi, A.; Vannucchi, A.M. Impact of calreticulin mutations on clinical and hematological phenotype and outcome in essential thrombocythemia. Blood 2014, 123, 1552–1555. [Google Scholar] [CrossRef] [Green Version]
- Tefferi, A.; Lasho, T.L.; Finke, C.M.; Knudson, R.A.; Ketterling, R.; Hanson, C.H.; Maffioli, M.; Caramazza, D.; Passamonti, F.; Pardanani, A. CALR vs JAK2 vs MPL-mutated or triple-negative myelofibrosis: Clinical, cytogenetic and molecular comparisons. Leukemia 2014, 28, 1472–1477. [Google Scholar] [CrossRef]
- Pietra, D.; Rumi, E.; Ferretti, V.V.; Di Buduo, C.A.; Milanesi, C.; Cavalloni, C.; Sant’Antonio, E.; Abbonante, V.; Moccia, F.; Casetti, I.C.; et al. Differential clinical effects of different mutation subtypes in CALR-mutant myeloproliferative neoplasms. Leukemia 2016, 30, 431–438. [Google Scholar] [CrossRef] [Green Version]
- Tefferi, A.; Lasho, T.L.; Tischer, A.; Wassie, E.A.; Finke, C.M.; Belachew, A.A.; Ketterling, R.P.; Hanson, C.A.; Pardanani, A.D. The prognostic advantage of calreticulin mutations in myelofibrosis might be confined to type 1 or type 1-like CALR variants. Blood 2014, 124, 2465–2466. [Google Scholar] [CrossRef] [Green Version]
- Tefferi, A.; Lasho, T.L.; Finke, C.; Belachew, A.A.; Wassie, E.A.; Ketterling, R.P.; Hanson, C.A.; Pardanani, A. Type 1 vs type 2 calreticulin mutations in primary myelofibrosis: Differences in phenotype and prognostic impact. Leukemia 2014, 28, 1568–1570. [Google Scholar] [CrossRef]
- Cabagnols, X.; Defour, J.P.; Ugo, V.; Ianotto, J.C.; Mossuz, P.; Mondet, J.; Girodon, F.; Alexandre, J.H.; Mansier, O.; Viallard, J.F.; et al. Differential association of calreticulin type 1 and type 2 mutations with myelofibrosis and essential thrombocytemia: Relevance for disease evolution. Leukemia 2015, 29, 249–252. [Google Scholar] [CrossRef]
- Arber, D.A.; Orazi, A.; Hasserjian, R.; Thiele, J.; Borowitz, M.J.; Le Beau, M.M.; Bloomfield, C.D.; Cazzola, M.; Vardiman, J.W. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood 2016, 127, 2391–2405. [Google Scholar] [CrossRef]
- Andrikovics, H.; Krahling, T.; Balassa, K.; Halm, G.; Bors, A.; Koszarska, M.; Batai, A.; Dolgos, J.; Csomor, J.; Egyed, M.; et al. Distinct clinical characteristics of myeloproliferative neoplasms with calreticulin mutations. Haematologica 2014, 99, 1184–1190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rumi, E.; Pietra, D.; Ferretti, V.; Klampfl, T.; Harutyunyan, A.S.; Milosevic, J.D.; Them, N.C.; Berg, T.; Elena, C.; Casetti, I.C.; et al. JAK2 or CALR mutation status defines subtypes of essential thrombocythemia with substantially different clinical course and outcomes. Blood 2014, 123, 1544–1551. [Google Scholar] [CrossRef] [PubMed]
- Marty, C.; Pecquet, C.; Nivarthi, H.; El-Khoury, M.; Chachoua, I.; Tulliez, M.; Villeval, J.L.; Raslova, H.; Kralovics, R.; Constantinescu, S.N.; et al. Calreticulin mutants in mice induce an MPL-dependent thrombocytosis with frequent progression to myelofibrosis. Blood 2016, 127, 1317–1324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elf, S.; Abdelfattah, N.S.; Chen, E.; Perales-Patón, J.; Rosen, E.A.; Ko, A.; Peisker, F.; Florescu, N.; Giannini, S.; Wolach, O.; et al. Mutant Calreticulin Requires Both Its Mutant C-terminus and the Thrombopoietin Receptor for Oncogenic Transformation. Cancer Discov. 2016, 6, 368–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larsen, T.S.; Pallisgaard, N.; Møller, M.B.; Hasselbalch, H.C. The JAK2 V617F allele burden in essential thrombocythemia, polycythemia vera and primary myelofibrosis—Impact on disease phenotype. Eur. J. Haematol. 2007, 79, 508–515. [Google Scholar] [CrossRef]
- Vannucchi, A.M.; Antonioli, E.; Guglielmelli, P.; Rambaldi, A.; Barosi, G.; Marchioli, R.; Marfisi, R.M.; Finazzi, G.; Guerini, V.; Fabris, F.; et al. Clinical profile of homozygous JAK2 617V>F mutation in patients with polycythemia vera or essential thrombocythemia. Blood 2007, 110, 840–846. [Google Scholar] [CrossRef]
- Hussein, K.; Bock, O.; Theophile, K.; von Neuhoff, N.; Buhr, T.; Schlué, J.; Büsche, G.; Kreipe, H. JAK2(V617F) allele burden discriminates essential thrombocythemia from a subset of prefibrotic-stage primary myelofibrosis. Exp. Hematol. 2009, 37, 1186–1193.e7. [Google Scholar] [CrossRef]
- Vannucchi, A.M.; Pieri, L.; Guglielmelli, P. JAK2 Allele Burden in the Myeloproliferative Neoplasms: Effects on Phenotype, Prognosis and Change with Treatment. Ther. Adv. Hematol. 2011, 2, 21–32. [Google Scholar] [CrossRef] [Green Version]
- Sallman, D.A.; Padron, E. Integrating mutation variant allele frequency into clinical practice in myeloid malignancies. Hematol. Oncol. Stem. Cell Ther. 2016, 9, 89–95. [Google Scholar] [CrossRef] [Green Version]
- Li, N.; Yao, Q.M.; Gale, R.P.; Li, J.L.; Li, L.D.; Zhao, X.S.; Jiang, H.; Jiang, Q.; Jiang, B.; Shi, H.X.; et al. Frequency and allele burden of CALR mutations in Chinese with essential thrombocythemia and primary myelofibrosis without JAK2(V617F) or MPL mutations. Leuk. Res. 2015, 39, 510–514. [Google Scholar] [CrossRef]
- Gángó, A.; Mózes, R.; Boha, Z.; Kajtár, B.; Timár, B.; Király, P.A.; Kiss, R.; Fésüs, V.; Nagy, N.; Demeter, J.; et al. Quantitative assessment of JAK2 V617F and CALR mutations in Philadelphia negative myeloproliferative neoplasms. Leuk. Res. 2018, 65, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Bertozzi, I.; Biagetti, G.; Vezzaro, T.; Barzon, I.; Carraro, M.; Fabris, F.; Randi, M.L. Clinical effect of CALR allele burden in patients with essential thrombocythemia. Ann. Hematol. 2022, 101, 1345–1346. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Total (n = 49) | ET (n = 32) | PMF (n = 17) | p-Value | |
|---|---|---|---|---|
| Age, years (IQR) | 56 (47–64) | 54 (47–63) | 61 (46–67) | 0.366 |
| Male, n (%) | 19 (39%) | 11 (34%) | 8 (47%) | 0.386 |
| WBC, ×109/L (IQR) | 7.76 (6.08–10.84) | 7.51 (6.25–9.78) | 9.38 (5.40–13.17) | 0.324 |
| ANC, ×109/L (IQR) | 4.70 (3.63–7.19) | 4.63 (3.79–5.98) | 5.44 (2.87–10.04) | 0.515 |
| AMC, ×109/L (IQR) | 0.56 (0.40–0.73) | 0.50 (0.35–0.66) | 0.67 (0.40–0.98) | 0.085 |
| Hb, g/dL (IQR) | 12.3 (10.5–13.9) | 13.2 (11.6–14.3) | 10.1 (8.9–13.5) | 0.007 |
| Platelets, ×109/L (IQR) | 734 (363–923) | 793 (581–937) | 252 (108–1028) | 0.019 |
| LDH, IU/L (IQR) | 434 (370–607) | 399 (301–462) | 581 (434–1014) | 0.011 |
| Splenomegaly, n (%) | 15 (31%) | 5 (16%) | 10 (59%) | 0.002 |
| CALR mutant burden, % | 35 (28–45) | 34 (18–40) | 45 (40–47) | 0.001 |
| Follow-up duration, months | 47 (27–57) | 41 (26–55) | 49 (27–69) | 0.535 |
| Thrombotic events, n (%) | 6 (12%) | 3 (9%) | 3 (18%) | 0.405 |
| Leukemic transformation, n (%) | 1 (2%) | 0 (0%) | 1 (6%) | 0.347 |
| Deceased, n (%) | 4 (8%) | 1 (3%) | 3 (18%) | 0.114 |
| CALR Mutant Type a (COSMIC ID) | Nucleotide Change | Amino Acid Change | No. of Patients (%) | ||
|---|---|---|---|---|---|
| ET | PMF | Total | |||
| Type 1-like mutation | |||||
| Type 1 (COSM1738055) | c.1099_1150del | p.Leu367Thrfs*46 | 11 (55%) | 9 (45%) | 20 (41%) |
| Type 3 (COSM1738150) | c.1100_1145del | p.Leu367Glnfs*48 | 1 (100%) | - | 1 (2%) |
| Type 7 (COSM1738343) | c.1103_1154del | p.Lys368Argfs*45 | - | 1 (100%) | 1 (2%) |
| n.d. (COSM3355766) | c.1103_1148del | p.Lys368Argfs*47 | - | 1 (100%) | 1 (2%) |
| Type 2-like mutation | |||||
| Type 2 (COSM1738056) | c.1154_1155insTTGTC | p.Lys385Asnfs*47 | 18 (82%) | 4 (18%) | 22 (45%) |
| Type 33 (COSM1738355) | c.1154_1155insATGTC | p.Glu386Cysfs*46 | - | 1 (100%) | 1 (2%) |
| Type 35 (COSM1738356) | c.1154delinsTTTGTC | p.Lys385Ilefs*47 | 1 (100%) | - | 1 (2%) |
| CALR-Mutated MPN | |||
|---|---|---|---|
| Type 1-like Mutation (n = 23) | Type 2-like Mutation (n = 24) | p-Value | |
| Age, years (IQR) | 61 (47–65) | 51 (47–61) | 0.250 |
| Male, n (%) | 11 (48%) | 6 (25%) | 0.104 |
| WBC, ×109/L (IQR) | 7.90 (6.31–11.25) | 7.40 (5.92–11.3) | 0.537 |
| ANC, ×109/L (IQR) | 4.70 (3.77–8.13) | 4.64 (3.57–7.14) | 0.941 |
| AMC, ×109/L (IQR) | 0.59 (0.40–0.79) | 0.53 (0.33–0.68) | 0.317 |
| Hb, g/dL (IQR) | 12.1 (8.9–13.8) | 12.4 (11.0–13.9) | 0.383 |
| Platelets, ×109/L (IQR) | 491 (210–790) | 892 (705–1336) | <0.001 |
| LDH, IU/L (IQR) | 580 (426–1112) | 413 (268–483) | 0.020 |
| Subtypes of MPN | |||
| ET, n (%) | 12 (52%) | 19 (79%) | 0.051 |
| PMF, n (%) | 11 (48%) | 5 (21%) | |
| Splenomegaly, n (%) | 10 (44%) | 4 (17%) | 0.045 |
| Thrombotic events, n (%) | 5 (22%) | 1 (4%) | 0.097 |
| CALR-mutant burden, % | 41 (22–47) | 39 (30–44) | 0.503 |
| ET | PMF | Type 1-like Mutation: ET vs. PMF | Type 2-like Mutation: ET vs. PMF | |||||
|---|---|---|---|---|---|---|---|---|
| Type 1-like Mutation (n = 12) | Type 2-like Mutation (n = 19) | p-Value | Type 1-like Mutation (n = 11) | Type 2-like Mutation (n = 5) | p-Value a | p-Value | p-Value a | |
| Age, years (IQR) | 58 (46–63) | 51 (47–61) | 0.715 | 63 (48–67) | 51 (42–72) | 0.395 | 0.323 | 0.859 |
| Male, n (%) | 6 (50%) | 4 (21%) | 0.127 | 5 (45%) | 2 (40%) | 1.000 | 0.827 | 0.568 |
| WBC, ×109/L (IQR) | 8.15 (6.83–10.31) | 6.66 (5.89–8.32) | 0.074 | 7.90 (5.13–12.4) | 12.35 (9.78–15.17) | 0.193 | 0.667 | 0.008 |
| ANC, ×109/L (IQR) | 5.04 (4.07–6.77) | 4.13 (3.45–5.87) | 0.201 | 4.04 (2.70–9.79) | 8.65 (5.91–11.03) | 0.126 | 0.538 | 0.014 |
| AMC, ×109/L (IQR) | 0.56 (0.44–0.71) | 0.45 (0.32–0.60) | 0.105 | 0.67 (0.40–0.98) | 0.68 (0.61–1.14) | 0.467 | 0.854 | 0.009 |
| Hb, g/dL (IQR) | 13.8 (12.4–15.6) | 12.2 (10.8–13.9) | 0.059 | 8.9 (7.50–11.30) | 13.5 (11.3–15.0) | 0.027 | 0.002 | 0.455 |
| Platelets, ×109/L (IQR) | 705 (492–845) | 851 (695–1173) | 0.092 | 210 (99–316) | 1513 (1007–2888) | 0.003 | 0.001 | 0.043 |
| LDH, IU/L (IQR) | 402 (382–422) | 399 (279–477) | 1.000 | 775 (542–1167) | 428 (245–500) | 0.039 | 0.046 | 0.800 |
| Splenomegaly, n (%) | 3 (25%) | 2 (11%) | 0.350 | 7 (64%) | 2 (40%) | 0.596 | 0.100 | 0.179 |
| Thrombotic events, n (%) | 3 (25%) | 0 (0%) | 0.049 | 2 (18%) | 1 (20%) | 1.000 | 1.000 | 0.208 |
| CALR-mutant burden, % | 26 (15–41) | 37 (29–40) | 0.292 | 45 (41–47) | 45 (37–48) | 0.910 | 0.008 | 0.051 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.-Y.; Han, Y.; Jang, J.H.; Jung, C.W.; Kim, S.-H.; Kim, H.-J. Effects of CALR-Mutant Type and Burden on the Phenotype of Myeloproliferative Neoplasms. Diagnostics 2022, 12, 2570. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12112570
Kim H-Y, Han Y, Jang JH, Jung CW, Kim S-H, Kim H-J. Effects of CALR-Mutant Type and Burden on the Phenotype of Myeloproliferative Neoplasms. Diagnostics. 2022; 12(11):2570. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12112570
Chicago/Turabian StyleKim, Hyun-Young, Yujin Han, Jun Ho Jang, Chul Won Jung, Sun-Hee Kim, and Hee-Jin Kim. 2022. "Effects of CALR-Mutant Type and Burden on the Phenotype of Myeloproliferative Neoplasms" Diagnostics 12, no. 11: 2570. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12112570