
Two-Year Follow-Up of Trypanosoma brucei gambiense Serology after Successful Treatment of Human African Trypanosomiasis: Results of Four Different Sero-Diagnostic Tests

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Study Procedures
2.3. Data Analysis
3. Results
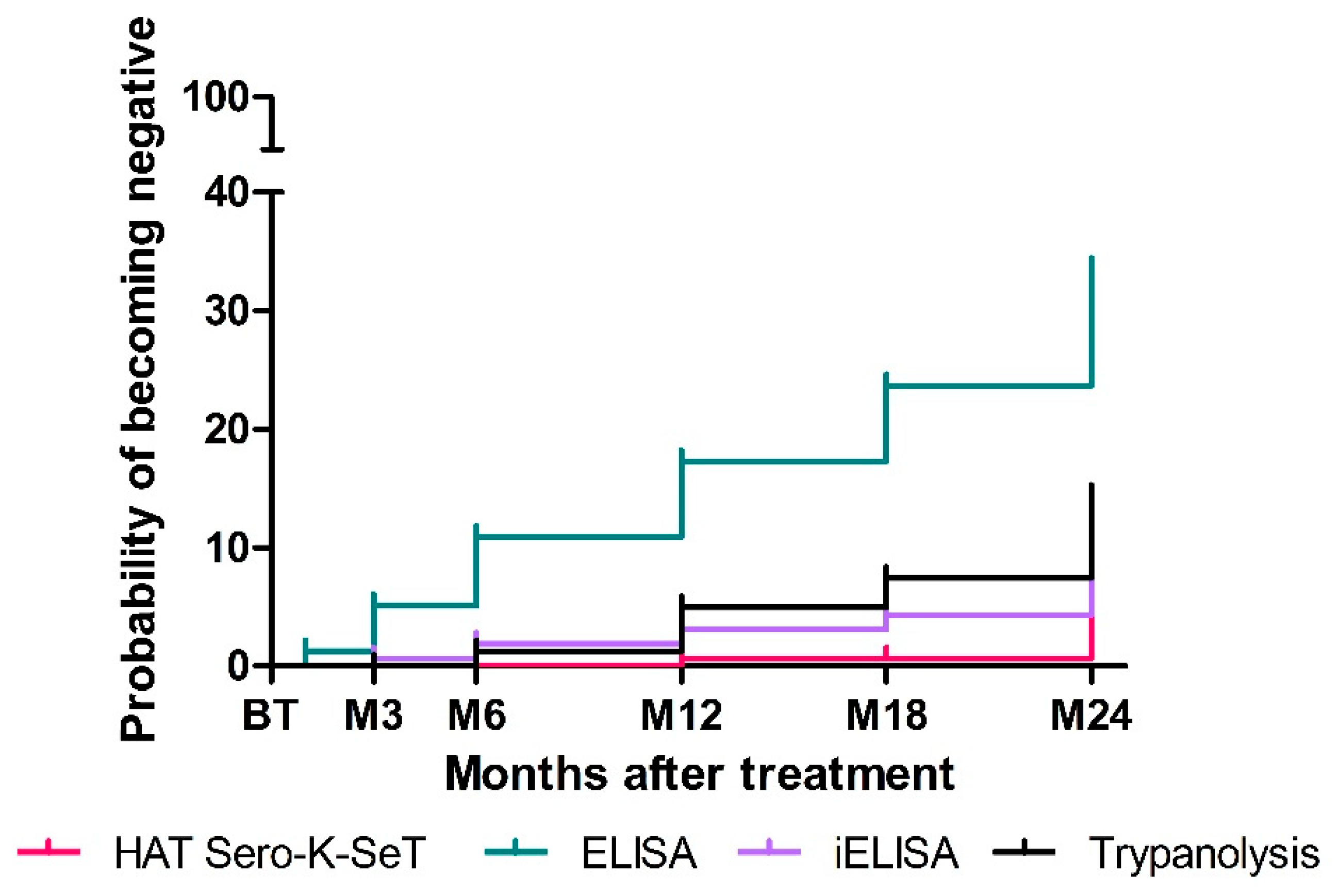
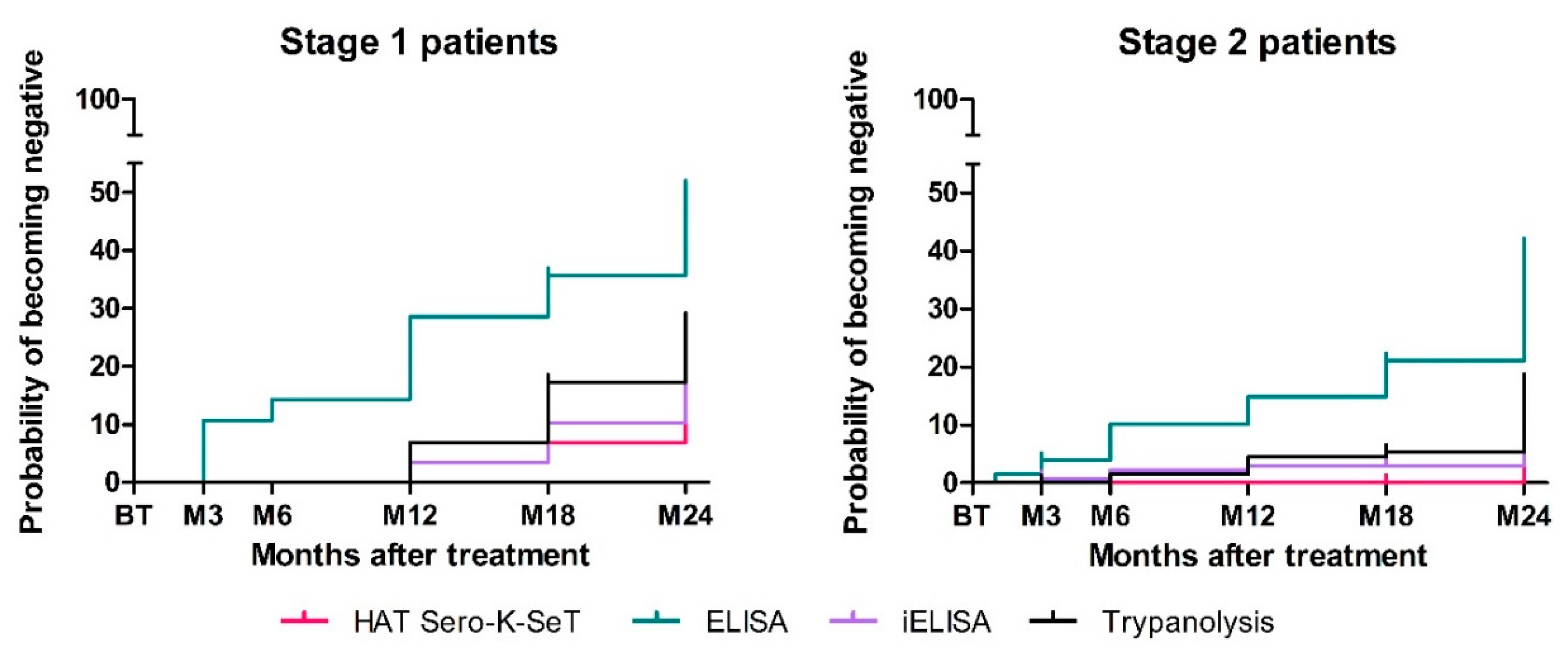
3.1. Serological Reversion Rates Post-Treatment as Measured with Four Serological Tests
3.2. Agreement between Tests
3.3. Intensity of the Test Signals over Time
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Büscher, P.; Cecchi, G.; Jamonneau, V.; Priotto, G. Human African trypanosomiasis. Lancet 2017, 390, 2397–2409. [Google Scholar] [CrossRef]
- Lejon, V.; Bentivoglio, M.; Franco, J.R. Human African Trypanosomiasis, 1st ed.; Elsevier B.V.: Amsterdam, The Netherlands, 2013; Volume 114. [Google Scholar]
- Jamonneau, V.; Ilboudo, H.; Kaboré, J.; Kaba, D.; Koffi, M.; Solano, P.; Garcia, A.; Courtin, D.; Laveissière, C.; Lingue, K.; et al. Untreated human infections by trypanosoma brucei gambiense are not 100% fatal. PLoS Negl. Trop. Dis. 2012, 6, e1691. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Health Observatory Data Repository—Number of New Reported Cases (T. b. Gambiense). Available online: https://apps.who.int/gho/data/node.main.A1636?lang=en (accessed on 27 September 2021).
- World Health Organization. Ending the Neglected to Attain the Sustainable Development Goals: A Roadmap for Neglected Tropical Diseases 2021–2030; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Checchi, F.; Cox, A.P.; Chappuis, F.; Priotto, G.; Chandramohan, D.; Haydon, D.T. Prevalence and under-detection of gambiense human African trypanosomiasis during mass screening sessions in Uganda and Sudan. Parasites Vectors 2012, 5, 157. [Google Scholar] [CrossRef] [PubMed]
- Dickie, E.A.; Giordani, F.; Gould, M.K.; Mäser, P.; Burri, C.; Mottram, J.C.; Rao, S.P.S.; Barrett, M.P. New drugs for human African trypanosomiasis: A twenty first century success story. Trop. Med. Infect. Dis. 2020, 5, 29. [Google Scholar] [CrossRef] [Green Version]
- Drugs for Neglected Diseases Initiative. Acoziborole|DNDi. Available online: https://dndi.org/research-development/portfolio/acoziborole/ (accessed on 2 December 2021).
- Eperon, G.; Balasegaram, M.; Potet, J.; Mowbray, C.; Valverde, O.; Chappuis, F. Treatment options for second-stage gambiense human African trypanosomiasis. Expert Rev. Anti-Infect. Ther. 2014, 12, 1407–1417. [Google Scholar] [CrossRef] [Green Version]
- Lumbala, C.; Biéler, S.; Kayembe, S.; Makabuza, J.; Ongarello, S.; Ndung’u, J.M. Prospective evaluation of a rapid diagnostic test for Trypanosoma brucei gambiense infection developed using recombinant antigens. PLoS Negl. Trop. Dis. 2018, 12, e0006386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koné, M.; Kaba, D.; Kaboré, J.; Thomas, L.F.; Falzon, L.C.; Koffi, M.; Kouamé, C.M.; Ahouty, B.; Compaoré, C.F.A.; N’Gouan, E.K.; et al. Passive surveillance of human African trypanosomiasis in Côte d’Ivoire: Understanding prevalence, clinical symptoms and signs, and diagnostic test characteristics. PLoS Negl. Trop. Dis. 2021, 15, e0009656. [Google Scholar] [CrossRef]
- Hasker, E.; Lutumba, P.; Mumba, D.; Lejon, V.; Büscher, P.; Kande, V.; Muyembe, J.J.; Menten, J.; Robays, J.; Boelaert, M. Diagnostic accuracy and feasibility of serological tests on filter paper samples for outbreak detection of T.b. gambiense human African trypanosomiasis. Am. J. Trop. Med. Hyg. 2010, 83, 374–379. [Google Scholar] [CrossRef]
- Camara, O.; Camara, M.; Lejon, V.; Ilboudo, H.; Sakande, H.; Léno, M.; Büscher, P.; Bucheton, B.; Jamonneau, V. Immune trypanolysis test with blood spotted on filter paper for epidemiological surveillance of sleeping sickness. Trop. Med. Int. Health 2014, 19, 828–831. [Google Scholar] [CrossRef] [Green Version]
- Jamonneau, V.; Bucheton, B.; Kaboré, J.; Ilboudo, H.; Camara, O.; Courtin, F.; Solano, P.; Kaba, D.; Kambire, R.; Lingue, K.; et al. Revisiting the immune trypanolysis test to optimise epidemiological surveillance and control of sleeping sickness in West Africa. PLoS Negl. Trop. Dis. 2010, 4, e917. [Google Scholar] [CrossRef] [Green Version]
- Dama, E.; Camara, O.; Kaba, D.; Koffi, M.; Camara, M.; Compaoré, C.; Ilboudo, H.; Courtin, F.; Kaboré, J.; N’Gouan, E.K.; et al. Immune trypanolysis test as a promising bioassay to monitor the elimination of gambiense human African trypanosomiasis. Parasite 2019, 26, 68. [Google Scholar] [CrossRef] [Green Version]
- Khonde, N.; Pépin, J.; Niyonsenga, T.; Milord, F.; De Wals, P. Epidemiological evidence for immunity following Trypanosoma brucei gambiense sleeping sickness. Trans. R. Soc. Trop. Med. Hyg. 1995, 89, 607–611. [Google Scholar] [CrossRef]
- Pyana, P.P.; Sere, M.; Kaboré, J.; De MeeÛs, T.; MacLeod, A.; Bucheton, B.; Van Reet, N.; Büscher, P.; Belem, A.M.G.; Jamonneau, V. Population genetics of Trypanosoma brucei gambiense in sleeping sickness patients with treatment failures in the focus of Mbuji-Mayi, Democratic Republic of the Congo. Infect. Genet. Evol. 2015, 30, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Richardson, J.B.; Evans, B.; Pyana, P.P.; Van Reet, N.; Sistrom, M.; Büscher, P.; Aksoy, S.; Caccone, A. Whole genome sequencing shows sleeping sickness relapse is due to parasite regrowth and not reinfection. Evol. Appl. 2016, 9, 381–393. [Google Scholar] [CrossRef] [PubMed]
- Mudji, J.; Blum, A.; Grize, L.; Wampfler, R.; Ruf, M.T.; Cnops, L.; Nickel, B.; Burri, C.; Blum, J. Gambiense human African trypanosomiasis sequelae after treatment: A follow-up study 12 years after treatment. Trop. Med. Infect. Dis. 2020, 5, 10. [Google Scholar] [CrossRef] [Green Version]
- Camara, M.; Soumah, A.M.; Ilboudo, H.; Travaillé, C.; Clucas, C.; Cooper, A.; Kuispond Swar, N.R.; Camara, O.; Sadissou, I.; Calvo Alvarez, E.; et al. Extravascular Dermal Trypanosomes in Suspected and Confirmed Cases of gambiense Human African Trypanosomiasis. Clin. Infect. Dis. 2021, 73, 12–20. [Google Scholar] [CrossRef]
- Lejon, V.; Ngoyi, D.M.; Boelaert, M.; Büscher, P. A CATT negative result after treatment for human african trypanosomiasis is no indication for cure. PLoS Negl. Trop. Dis. 2010, 4, e590. [Google Scholar] [CrossRef] [Green Version]
- Miezan, T.W.; Dje, N.N.; Doua, F.; Boa, F. Trypanosomose humaine africaine en Côte d’Ivoire: Caractéristiques biologiques après traitement. A propos de 812 cas traités dans le foyer de Daloa (Côte d’Ivoire). Bull. Soc. Pathol. Exot. 2003, 95, 362–365. [Google Scholar]
- Pepin, J.; Guern, C.; Mercier, D.; Moore, P. Utilisation du Testryp CATT pour le depistage de la trypanosomiase a Nioki, Zaire. Ann. Soc. Belg. Med. Trop. 1986, 66, 213–224. [Google Scholar] [PubMed]
- Paquet, C.; Ancelle, T.; Gastellu-Etchegorry, M.; Castilla, J.; Harndt, I. Persistence of antibodies to Trypanosoma brucei gambiense after treatment of human trypanosomiasis in Uganda. Lancet 1992, 340, 250. [Google Scholar] [CrossRef]
- Frezil, J.L.; Coulm, J.; Alary, J.C. L’Immunofluorescence Indirecte Dans La Surveillance Therapeutique Des Trypanosomes (Note Preliminaire). Bull. Soc. Pathol. Exot. Fil. 1978, 71, 440–445. [Google Scholar]
- Ngoyi, D.M.; Lejon, V.; Pyana, P.; Boelaert, M.; Llunga, M.; Menten, J.; Mulunda, J.P.; Van Nieuwenhove, S.; Tamfum, J.J.M.; Büscher, P. How to shorten patient follow-up after treatment for Trypanosoma brucei gambiense sleeping sickness. J. Infect. Dis. 2010, 201, 453–463. [Google Scholar] [CrossRef] [PubMed]
- Franco, J.R.; Simarro, P.P.; Diarra, A.; Ruiz-Postigo, J.A.; Samo, M.; Jannin, J.G. Monitoring the use of nifurtimox-eflornithine combination therapy (NECT) in the treatment of second stage gambiense human African trypanosomiasis. Res. Rep. Trop. Med. 2012, 3, 93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lejon, V.; Kwete, J.; Büscher, P. Short communication: Towards saliva-based screening for sleeping sickness? Trop. Med. Int. Health 2003, 8, 585–588. [Google Scholar] [CrossRef] [Green Version]
- Lejon, V.; Jamonneau, V.; Solano, P.; Atchade, P.; Mumba, D.; Nkoy, N.; Bébronne, N.; Kibonja, T.; Balharbi, F.; Wierckx, A.; et al. Detection of trypanosome-specific antibodies in saliva, towards non-invasive serological diagnosis of sleeping sickness. Trop. Med. Int. Health 2006, 11, 620–627. [Google Scholar] [CrossRef]
- Geerts, M.; Van Reet, N.; Leyten, S.; Berghmans, R.; Rock, K.S.; Coetzer, T.H.T.; Eyssen, L.E.-A.; Büscher, P. Trypanosoma brucei gambiense-iELISA: A Promising New Test for the Post-Elimination Monitoring of Human African Trypanosomiasis. Clin. Infect. Dis. 2020, 73, e2477–e2483. [Google Scholar] [CrossRef]
- Van Meirvenne, N.; Magnus, E.; Büscher, P. Evaluation of variant specific trypanolysis tests for serodiagnosis of human infections with Trypanosoma brucei gambiense. Acta Trop. 1995, 60, 189–199. [Google Scholar] [CrossRef]
- Grandesso, F.; Nabasumba, C.; Nyehangane, D.; Page, A.L.; Bastard, M.; De Smet, M.; Boum, Y.; Etard, J.F. Performance and time to become negative after treatment of three malaria rapid diagnostic tests in low and high malaria transmission settings. Malar. J. 2016, 15, 496. [Google Scholar] [CrossRef] [Green Version]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159. [Google Scholar] [CrossRef] [Green Version]
- Feinstien, A.R.; Cicchetti, D.V. High Agreement but Low Kappa. J. Clin. Epidemiol. 1990, 43, 551–585. [Google Scholar]
- da Luz, R.I.; Phanzu, D.M.; Kiabanzawoko, O.N.; Miaka, E.; Verlé, P.; De Weggheleire, A.; Büscher, P.; Hasker, E.; Boelaert, M. Feasibility of a dried blood spot strategy for serological screening and surveillance to monitor elimination of human african trypanosomiasis in the Democratic Republic of the Congo. PLoS Negl. Trop. Dis. 2021, 15, e0009407. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Stage 1 Patients (n = 30) | Stage 2 Patients (n = 133) | |
|---|---|---|
| Treatment naïve/retreatment cases | 30/0 | 53/80 |
| Treatment | ||
| Pentamidine | 30 | 0 |
| Melarsoprol | 0 | 49 |
| Eflornithine | 0 | 48 |
| Melarsoprol/nifurtimox | 0 | 35 |
| Melarsoprol/eflornithine | 0 | 1 |
| Number of patients with available follow-up samples n (%) | ||
| Before treatment | 30 (100%) | 133 (100%) |
| End of treatment | 30 (100%) | 129 (97%) |
| 3 months | 29 (97%) | 127 (95%) |
| 6 months | 29 (97%) | 127 (95%) |
| 12 months | 27 (90%) | 118 (89%) |
| 18 months | 27 (90%) | 105 (79%) |
| 24 months | 28 (93%) | 131 (98%) |
| Total number of samples | 200 | 870 |
| BT (n = 163) * | EoT (n = 159) | 3M (n = 156) | 6M (n = 156) | 12M (n = 145) | 18M (n = 132) | 24M (n = 159) | |
|---|---|---|---|---|---|---|---|
| HAT Sero-K-SeT | 0 - | 0 - | 0.6% (0–1.8) | 0.6% (0–1.8) | 0.7% (0–2.1) | 1.5% (0–3.6) | 3.8% (0.8–6.8) |
| ELISA | 7% | 6% | 9% | 16%, | 24% | 32% | 35% |
| (3.1–10.9) | (2.3–9.7) | (4.5–13.5) | (10.2–21.8) | (17–31) | (24–40) | (27.6–42) | |
| iELISA ** | 2.5% | 0 | 1.9% | 2.6% | 6.2% | 5.3% | 7.5% |
| (0.1–4.9) | - | (0–4) | (0.1–5.1) | (2.3–10.1) | (1.5–9.1) | (3.4–11.6) | |
| TL ** | 0 | 0 | 0.6% | 1.9% | 7.6% | 9.1% | 14.5% |
| - | - | (0–1.8) | (0–4) | (3.3–11.9) | (4.2–14) | (9–20) |
| All Patients (n = 163) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| BT | EoT | 3M | 6M | 12M | 18M | 24M | Sero-Reversion Probability | ||
| RDT | Hazard | 0 | 0 | 0 | 0 | 0.6 | 0 | 6.3 | 6.7 |
| 95% CI | - | - | - | - | 0–1.8 | - | 0.8–1.19 | 3–14.6 | |
| ELISA | Hazard | 3.13 | 1.3 | 4 | 6.3 | 7.5 | 8.1 | 25.6 | 42.9 |
| 95% CI | 0.4–5.9 | 0–3.1 | 0.8–7.1 | 2.2–10.4 | 2.8–12.1 | 3.1–13.2 | 12.8–38.5 | 34.4–52.5 | |
| iELISA | Hazard | 0 | 0 | 6 | 1.3 | 1.3 | 1.3 | 6.6 | 10.4 |
| 95% CI | - | - | 0–18 | 0–3 | 0–3 | 0–3.1 | 0.8–12.3 | 5.9–18.2 | |
| TL | Hazard | 0 | 0 | 0 | 0 | 2.6 | 0.7 | 9.5 | 12 |
| 95% CI | - | - | - | - | 0.1–5 | 0–2 | 2.5–16.8 | 6.8–20.7 | |
| Stage 1 patients (n = 30) | |||||||||
| RDT | Hazard | 0 | 0 | 0 | 0 | 3.5 | 0 | 7.4 | 10.3 |
| 95% CI | - | - | - | - | 0–10.4 | - | 0–21.9 | 2.5–37.9 | |
| ELISA | Hazard | 3.4 | 0 | 11.3 | 4.1 | 18.2 | 10.8 | 23.5 | 51.1 |
| 95% CI | 0–10.4 | - | 0–24.1 | 0–12.1 | 0.4–35.9 | 0–25.8 | 0–55.9 | 32.3–73.2 | |
| iELISA | Hazard | 0 | 0 | 0 | 0 | 3.5 | 7.6 | 8 | 17.4 |
| 95% CI | - | - | - | - | 0–10.4 | 0–18 | 0–23.7 | 6.4–42.1 | |
| TL | Hazard | 0 | 0 | 3.5 | 0 | 7.4 | 12.5 | 9.1 | 27.8 |
| 95% CI | - | - | 0–10.4 | - | 0–17.7 | 0–26.6 | 0–26.9 | 13.6–51.4 | |
| Stage 2 patients (n = 133) | |||||||||
| RDT | Hazard | 0 | 0 | 0 | 0 | 0 | 0 | 6.2 | 6 |
| 95% CI | - | - | - | - | - | - | 3.1–12.2 | 2.3–15.1 | |
| ELISA | Hazard | 3 | 1.6 | 8.22.4 | 6.7 | 5.4 | 7.7 | 26 | 41.1 |
| 95% CI | 0.1–6 | 0–3.7 | 0–5.1 | 2.1–11.4 | 1.1–9.6 | 2.4–13 | 12–40 | 31.8–51.9 | |
| iELISA | Hazard | 0 | 0 | 0.8 | 1.5 | 0.8 | 0 | 6.3 | 8.9 |
| 95% CI | - | - | 0–2.2 | 0–3.6 | 0–2.3 | - | 0.1–12.5 | 4.4–17.7 | |
| TL | Hazard | 0 | 0 | 0 | 1.5 | 3.9 | 0.8 | 13.1 | 17.6 |
| 95% CI | - | - | - | 0–3.6 | 0.5–7.3 | 0–2.4 | 4.1–22.2 | 10.9–27.8 | |
| BT | EoT | M3 | M6 | M12 | M18 | M24 | |
|---|---|---|---|---|---|---|---|
| RDT vs. ELISA | 92.6% | 94.3% | 91.7% (0.12) | 84.6% (0.06) | 76.6% (0.04) | 69.7% (0.06) | 67.9% (0.1) |
| RDT vs. iELISA | 97.5% | 100% | 98.7% (0.49) | 98.1% (0.39) | 94.5% (0.19) | 94.7% (0.2) | 93.7% (0.42) |
| RDT vs. TL | 100% | 100% | 100% (1) | 98.7% (0.5) | 93.2% (0.16) | 92.5% (0.27) | 84.3% (0.08) |
| ELISA vs. iELISA | 93.9% | 94.3% | 92.9% (0.33) | 86.5% (0.24) | 82.1% (0.34) | 73.4% (0.21) | 70.4% (0.19) |
| ELISA vs. TL | 92.6% | 94.3% | 91.7% (0.12) | 84.6% (0.11) | 76.5% (0.16) | 75.8% (0.3) | 72.3% (0.29) |
| iELISA vs. TL | 97.5% | 100% | 98.7% (0.49) | 96.8% (0.27) | 93.2% (0.46) | 93.2% (0.49) | 89.3% (0.46) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inocencio da Luz, R.; Tablado Alonso, S.; Büscher, P.; Verlé, P.; De Weggheleire, A.; Mumba Ngoyi, D.; Pyana, P.P.; Hasker, E. Two-Year Follow-Up of Trypanosoma brucei gambiense Serology after Successful Treatment of Human African Trypanosomiasis: Results of Four Different Sero-Diagnostic Tests. Diagnostics 2022, 12, 246. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12020246
Inocencio da Luz R, Tablado Alonso S, Büscher P, Verlé P, De Weggheleire A, Mumba Ngoyi D, Pyana PP, Hasker E. Two-Year Follow-Up of Trypanosoma brucei gambiense Serology after Successful Treatment of Human African Trypanosomiasis: Results of Four Different Sero-Diagnostic Tests. Diagnostics. 2022; 12(2):246. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12020246
Chicago/Turabian StyleInocencio da Luz, Raquel, Sara Tablado Alonso, Philippe Büscher, Paul Verlé, Anja De Weggheleire, Dieudonné Mumba Ngoyi, Pati Patient Pyana, and Epco Hasker. 2022. "Two-Year Follow-Up of Trypanosoma brucei gambiense Serology after Successful Treatment of Human African Trypanosomiasis: Results of Four Different Sero-Diagnostic Tests" Diagnostics 12, no. 2: 246. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12020246