
Automated Diagnosis of Cervical Intraepithelial Neoplasia in Histology Images via Deep Learning

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Dataset Construction
2.3. Dataset Preprocessing
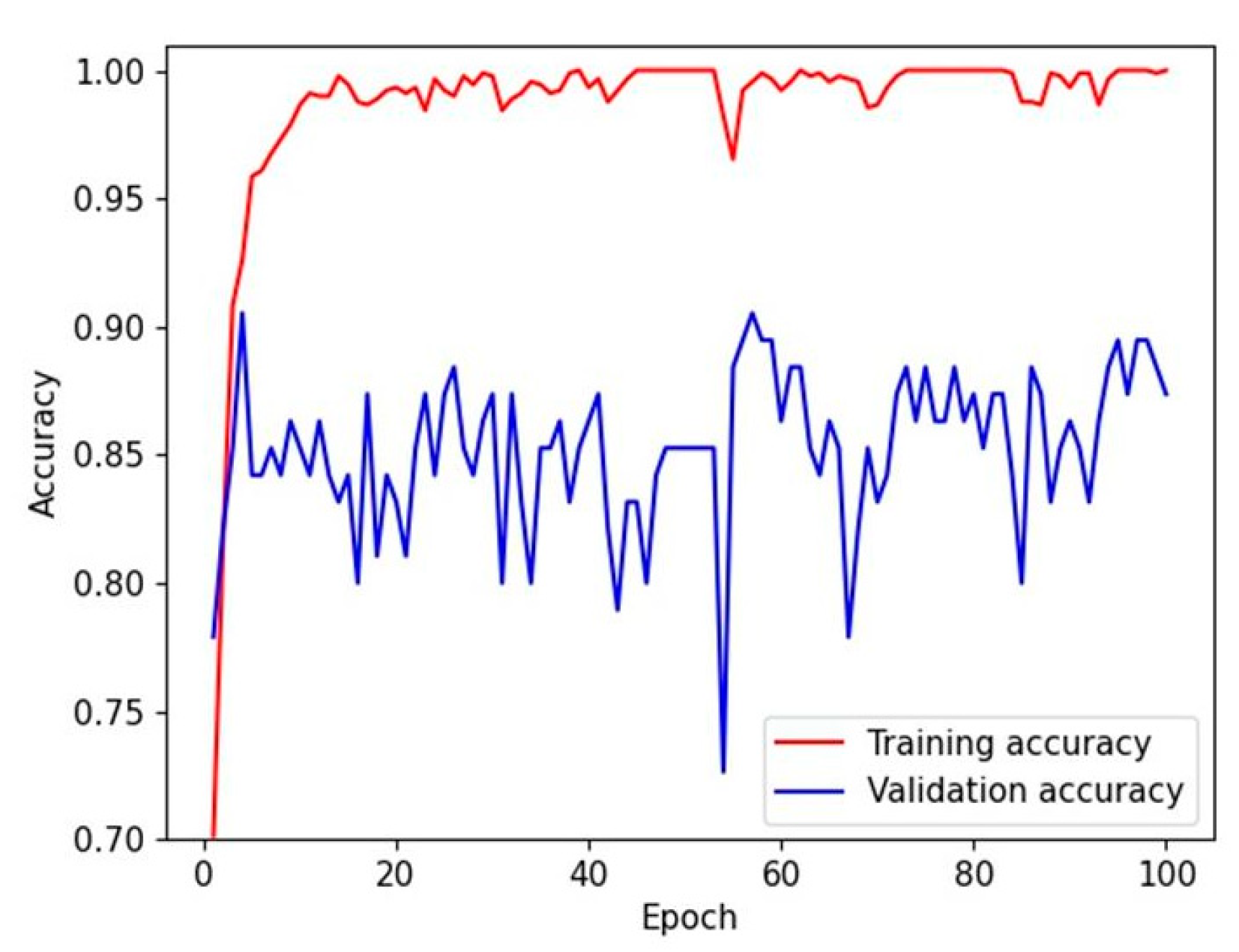
2.4. Deep Learning Model Training
2.5. Human Performance Evaluation
2.6. Main Outcome Measures and Statistical Methods
3. Results
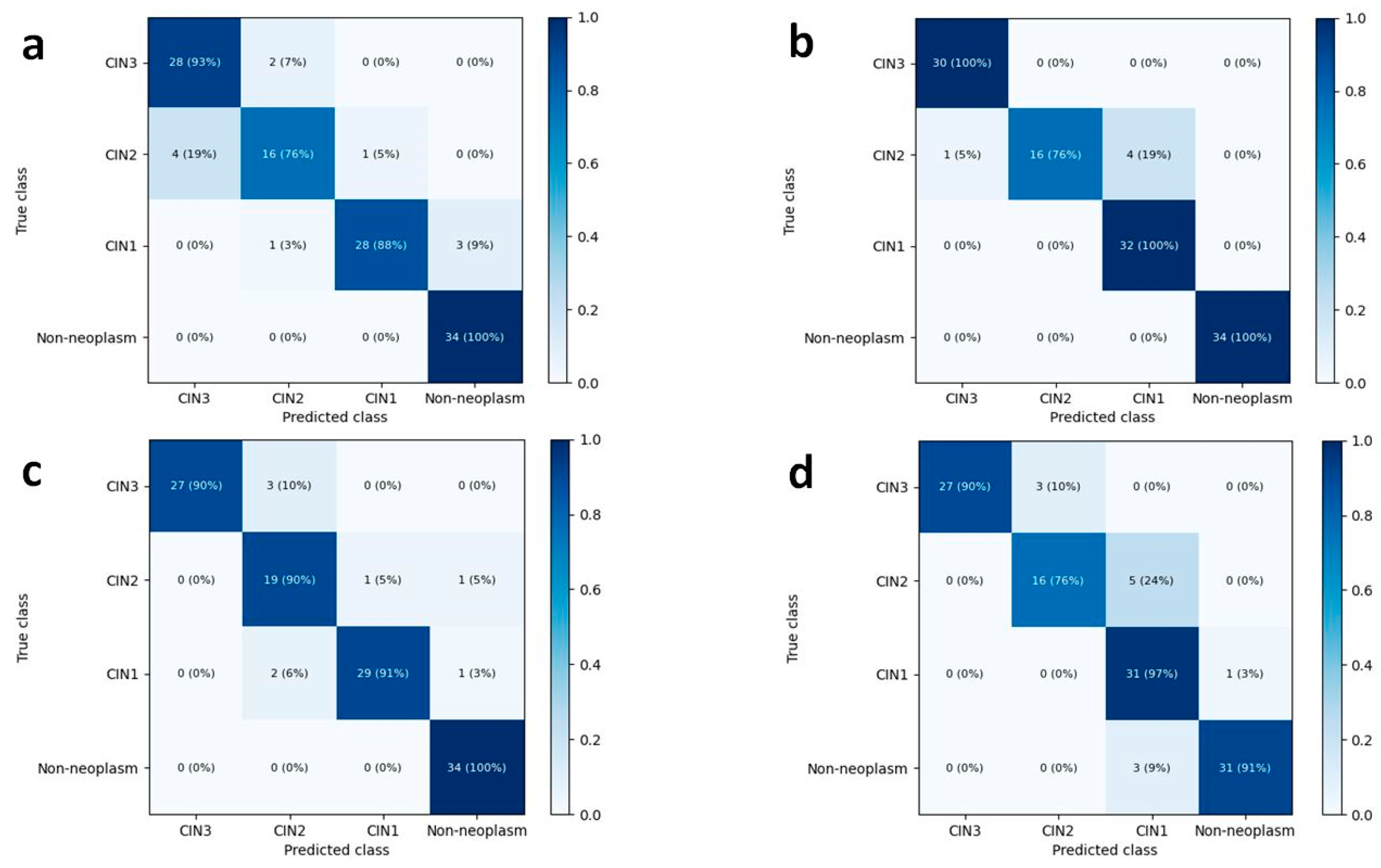
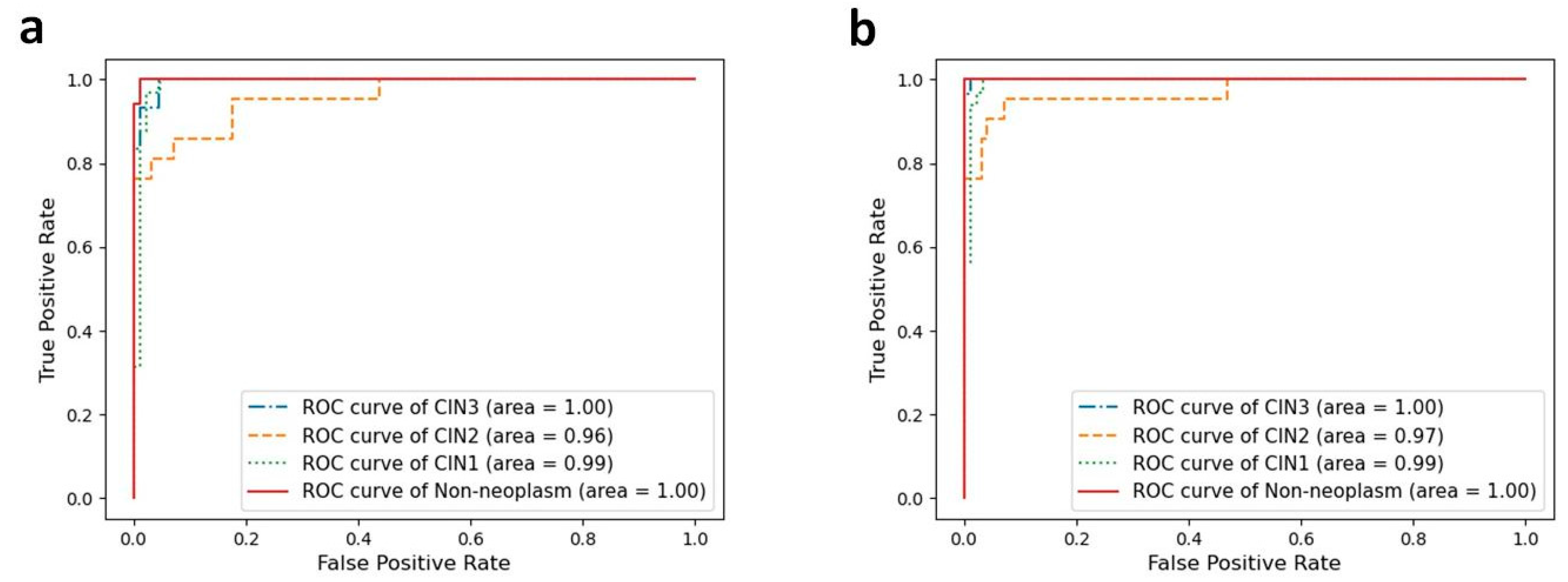
3.1. Four-Class Classification Performance of Deep Learning Models and Human Pathologists
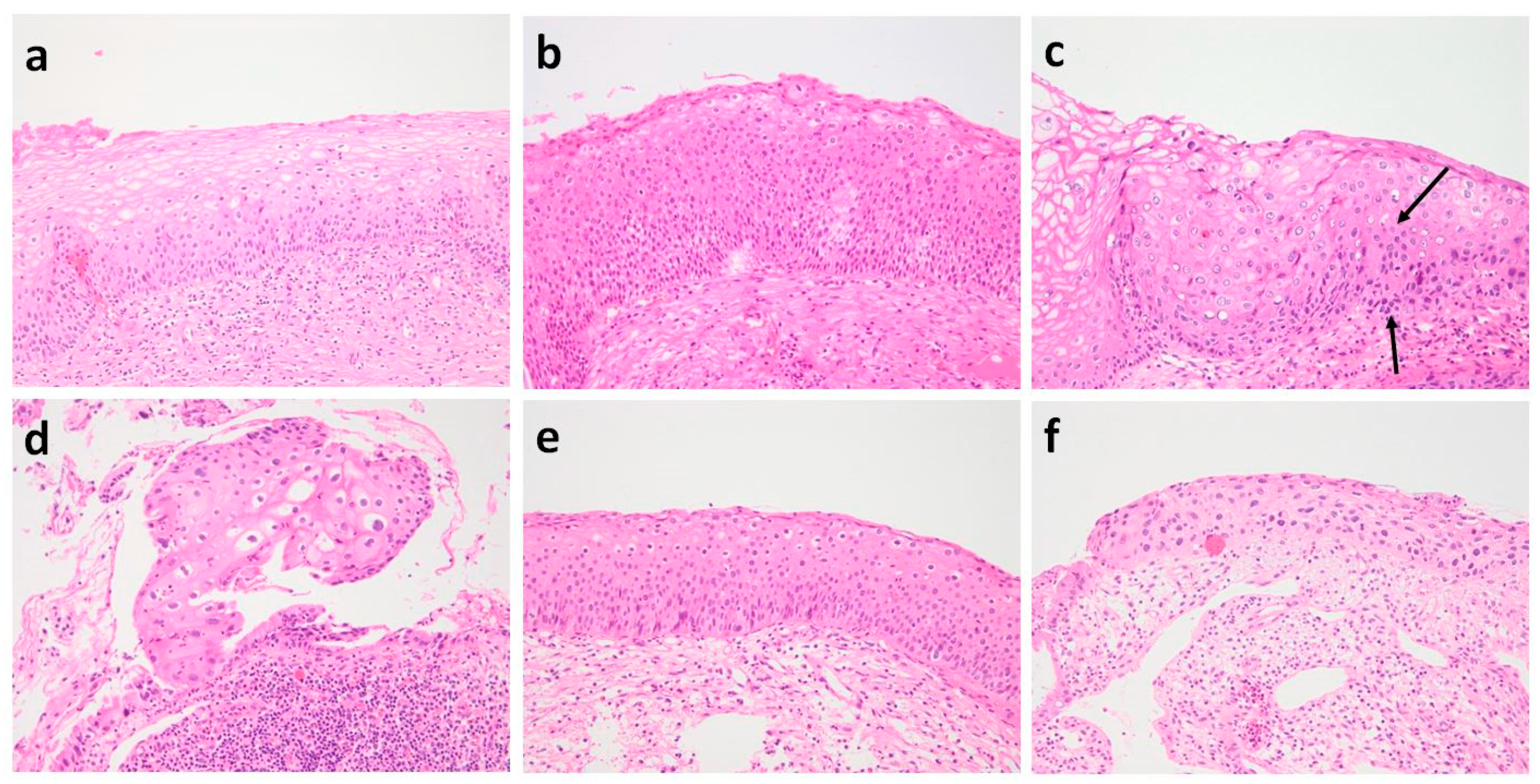
3.2. Histologic Review of Misclassified Cases in Four-Class Classification Using Best-Performing CNN Models
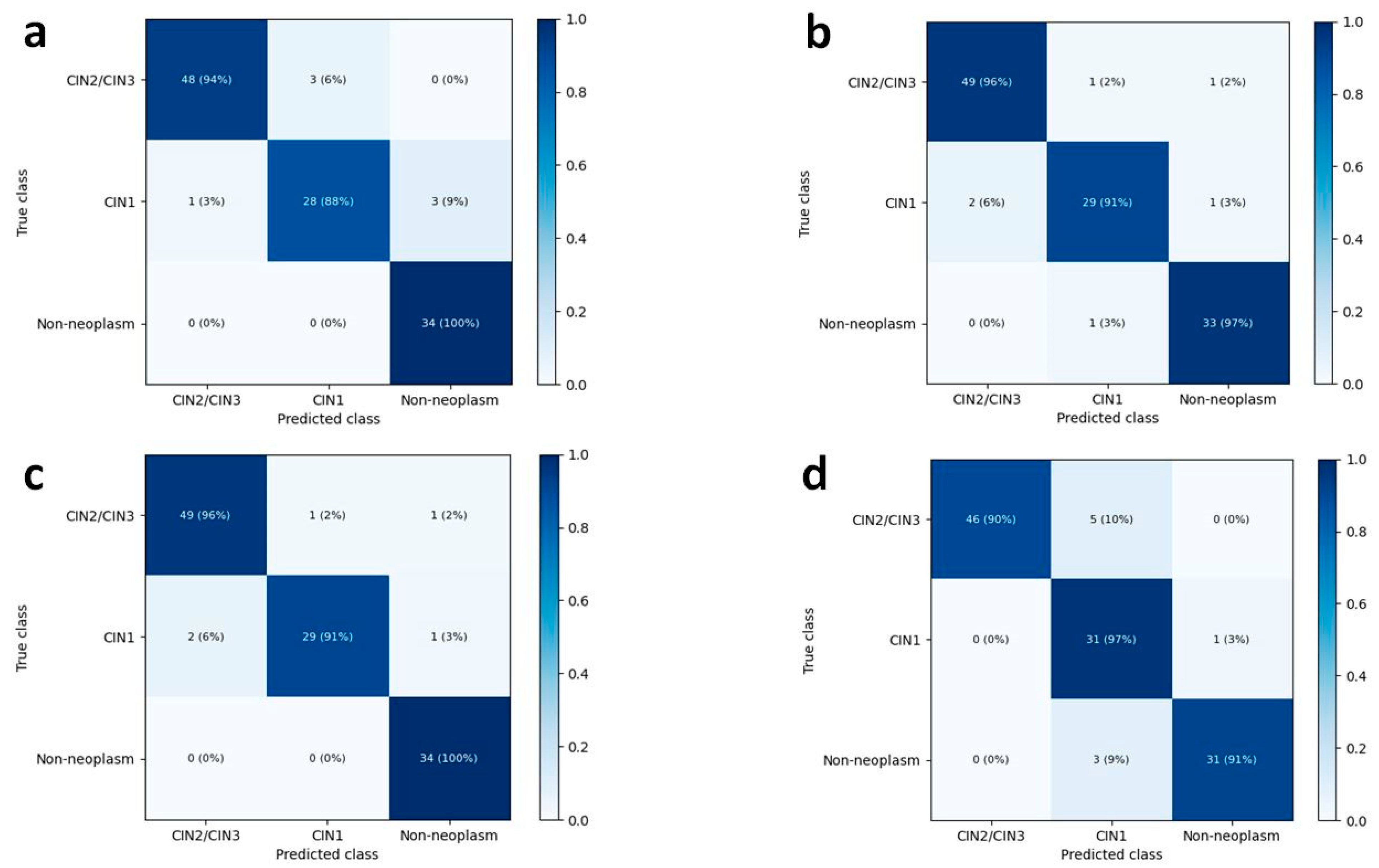
3.3. Three-Class Classification Performance of Deep Learning Models and Human Pathologists
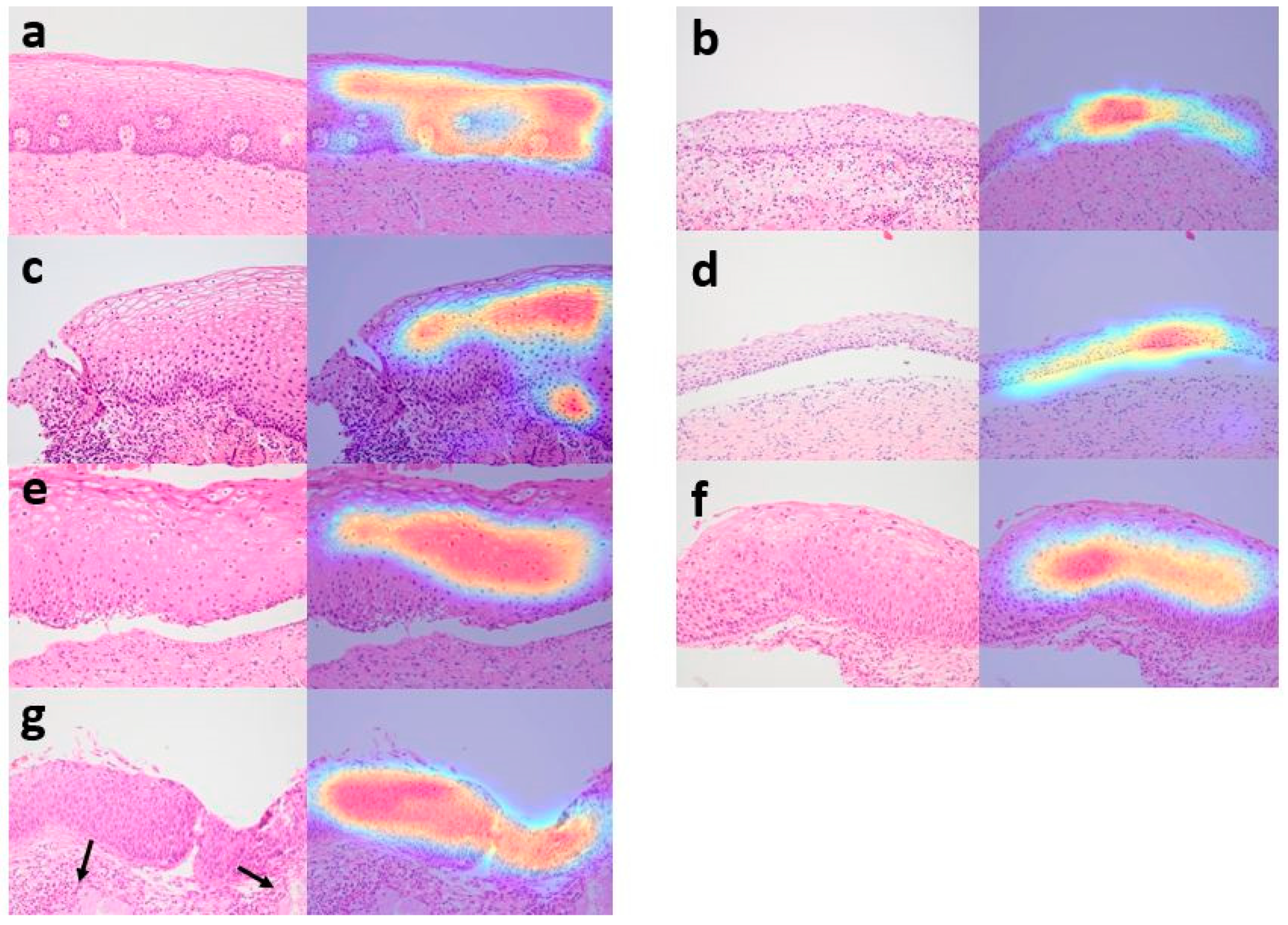
3.4. Analysis of Grad-CAM Images by CNN Model
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Four-Class Classification | Three-Class Classification | |||
|---|---|---|---|---|
| DenseNet-161 | EfficientNet-b7 | DenseNet-161 | EfficientNet-b7 | |
| Mean accuracy | 0.885 | 0.895 | 0.914 | 0.926 |
| 95% CI | 0.863–0.906 | 0.833–0.957 | 0.888–0.940 | 0.904–949 |
| Test 1 | 0.906 | 0.957 | 0.940 | 0.949 |
| Test 2 | 0.873 | 0.853 | 0.901 | 0.919 |
| Test 3 | 0.875 | 0.875 | 0.901 | 0.911 |

References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Darragh, T.M.; Colgan, T.J.; Cox, J.T.; Heller, D.S.; Henry, M.R.; Luff, R.D.; McCalmont, T.; Nayar, R.; Palefsky, J.M.; Stoler, M.H.; et al. The Lower Anogenital Squamous Terminology Standardization Project for HPV-Associated Lesions: Background and consensus recommendations from the College of American Pathologists and the American Society for Colposcopy and Cervical Pathology. Arch. Pathol. Lab. Med. 2012, 136, 1266–1297. [Google Scholar] [CrossRef] [PubMed]
- Mills, A.M.; Carrilho, C.; Focchi, G.R.A.; Kong, C.S.; Park, K.J.; Regauer, S.; Saco, A. Squamous intraepithelial lesions of the uterine cervix. In WHO Classification of Tumors Editorial Board. Female Genital Tumors, 5th ed.; International Agency for Research on Cancer: Lyon, France, 2019; pp. 342–346. [Google Scholar]
- McCredie, M.R.; Sharples, K.J.; Paul, C.; Baranyai, J.; Medley, G.; Jones, R.W.; Skegg, D.C. Natural history of cervical neoplasia and risk of invasive cancer in women with cervical intraepithelial neoplasia 3: A retrospective cohort study. Lancet Oncol. 2008, 9, 425–434. [Google Scholar] [CrossRef]
- Massad, L.S.; Einstein, M.H.; Huh, W.K.; Katki, H.A.; Kinney, W.K.; Schiffman, M.; Solomon, D.; Wentzensen, N.; Lawson, H.W. 2012 updated consensus guidelines for the management of abnormal cervical cancer screening tests and cancer precursors. J. Low. Genit. Tract Dis. 2013, 17, S1–S27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perkins, R.B.; Guido, R.S.; Castle, P.E.; Chelmow, D.; Einstein, M.H.; Garcia, F.; Huh, W.K.; Kim, J.J.; Moscicki, A.B.; Nayar, R.; et al. 2019 ASCCP Risk-Based Management Consensus Guidelines for Abnormal Cervical Cancer Screening Tests and Cancer Precursors. J. Low. Genit. Tract Dis. 2020, 24, 102–131. [Google Scholar] [CrossRef] [Green Version]
- Stoler, M.H.; Schiffman, M. Interobserver reproducibility of cervical cytologic and histologic interpretations: Realistic estimates from the ASCUS-LSIL Triage Study. JAMA 2001, 285, 1500–1505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castle, P.E.; Stoler, M.H.; Solomon, D.; Schiffman, M. The relationship of community biopsy-diagnosed cervical intraepithelial neoplasia grade 2 to the quality control pathology-reviewed diagnoses: An ALTS report. Am. J. Clin. Pathol. 2007, 127, 805–815. [Google Scholar] [CrossRef] [PubMed]
- Carreon, J.D.; Sherman, M.E.; Guillen, D.; Solomon, D.; Herrero, R.; Jeronimo, J.; Wacholder, S.; Rodriguez, A.C.; Morales, J.; Hutchinson, M.; et al. CIN2 is a much less reproducible and less valid diagnosis than CIN3: Results from a histological review of population-based cervical samples. Int. J. Gynecol. Pathol. 2007, 26, 441–446. [Google Scholar] [CrossRef]
- Adesina, A.; Chumba, D.; Nelson, A.M.; Orem, J.; Roberts, D.J.; Wabinga, H.; Wilson, M.; Rebbeck, T.R. Improvement of pathology in sub-Saharan Africa. Lancet Oncol. 2013, 14, e152–e157. [Google Scholar] [CrossRef]
- Bulten, W.; Pinckaers, H.; van Boven, H.; Vink, R.; de Bel, T.; van Ginneken, B.; van der Laak, J.; Hulsbergen-van de Kaa, C.; Litjens, G. Automated deep-learning system for Gleason grading of prostate cancer using biopsies: A diagnostic study. Lancet Oncol. 2020, 21, 233–241. [Google Scholar] [CrossRef] [Green Version]
- Courtiol, P.; Maussion, C.; Moarii, M.; Pronier, E.; Pilcer, S.; Sefta, M.; Manceron, P.; Toldo, S.; Zaslavskiy, M.; Le Stang, N.; et al. Deep learning-based classification of mesothelioma improves prediction of patient outcome. Nat. Med. 2019, 25, 1519–1525. [Google Scholar] [CrossRef] [PubMed]
- Halicek, M.; Shahedi, M.; Little, J.V.; Chen, A.Y.; Myers, L.L.; Sumer, B.D.; Fei, B. Head and Neck Cancer Detection in Digitized Whole-Slide Histology Using Convolutional Neural Networks. Sci. Rep. 2019, 9, 14043. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ker, J.; Bai, Y.; Lee, H.Y.; Rao, J.; Wang, L. Automated brain histology classification using machine learning. J. Clin. Neurosci. 2019, 66, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Yoon, H.; Lee, J.; Oh, J.E.; Kim, H.R.; Lee, S.; Chang, H.J.; Sohn, D.K. Tumor Identification in Colorectal Histology Images Using a Convolutional Neural Network. J. Digit. Imaging 2019, 32, 131–140. [Google Scholar] [CrossRef]
- Lucas, M.; Jansen, I.; Savci-Heijink, C.D.; Meijer, S.L.; de Boer, O.J.; van Leeuwen, T.G.; de Bruin, D.M.; Marquering, H.A. Deep learning for automatic Gleason pattern classification for grade group determination of prostate biopsies. Virchows Arch. 2019, 475, 77–83. [Google Scholar] [CrossRef] [Green Version]
- Valente, P.T.; Schantz, H.D. Cytology automation: An overview. Lab. Med. 2001, 32, 686–690. [Google Scholar] [CrossRef]
- Landau, M.S.; Pantanowitz, L. Artificial intelligence in cytopathology: A review of the literature and overview of commercial landscape. J. Am. Soc. Cytopathol. 2019, 8, 230–241. [Google Scholar] [CrossRef]
- Guo, P.; Almubarak, H.; Banerjee, K.; Stanley, R.J.; Long, R.; Antani, S.; Thoma, G.; Zuna, R.; Frazier, S.R.; Moss, R.H.; et al. Enhancements in localized classification for uterine cervical cancer digital histology image assessment. J. Pathol. Inform. 2016, 7, 51. [Google Scholar] [CrossRef]
- Sornapudi, S.; Stanley, R.J.; Stoecker, W.V.; Almubarak, H.; Long, R.; Antani, S.; Thoma, G.; Zuna, R.; Frazier, S.R. Deep Learning Nuclei Detection in Digitized Histology Images by Superpixels. J. Pathol. Inform. 2018, 9, 5. [Google Scholar] [CrossRef]
- Keenan, S.J.; Diamond, J.; Glenn McCluggage, W.; Bharucha, H.; Thompson, D.; Bartels, P.H.; Hamilton, P.W. An automated machine vision system for the histological grading of cervical intraepithelial neoplasia (CIN). J. Pathol. 2000, 192, 351–362. [Google Scholar] [CrossRef]
- Guo, P.; Banerjee, K.; Stanley, R.J.; Long, R.; Antani, S.; Thoma, G.; Zuna, R.; Frazier, S.R.; Moss, R.H.; Stoecker, W.V. Nuclei-based features for uterine cervical cancer histology image analysis with fusion-based classification. IEEE J. Biomed. Health Inform. 2015, 20, 1595–1607. [Google Scholar] [CrossRef] [PubMed]
- Huang, P.; Zhang, S.; Li, M.; Wang, J.; Ma, C.; Wang, B.; Lv, X. Classification of cervical biopsy images based on LASSO and EL-SVM. IEEE Access 2020, 8, 24219–24228. [Google Scholar] [CrossRef]
- Meng, Z.; Zhao, Z.; Li, B.; Su, F.; Guo, L. A Cervical Histopathology Dataset for Computer Aided Diagnosis of Precancerous Lesions. IEEE Trans. Med. Imaging 2021, 40, 1531–1541. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Crookes, D.; Eldin, O.S.; Wang, S.; Hamilton, P.; Diamond, J. Assisted diagnosis of cervical intraepithelial neoplasia (CIN). IEEE J. Sel. Top. Signal Processing 2009, 3, 112–121. [Google Scholar] [CrossRef] [Green Version]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely Connected Convolutional Networks. In Proceedings of the 2017 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017; pp. 2261–2269. [Google Scholar]
- Tan, M.; Le, Q. Efficientnet: Rethinking model scaling for convolutional neural networks. In Proceedings of the International Conference on Machine Learning, Long Beach, CA, USA, 10–15 June 2019; pp. 6105–6114. [Google Scholar]
- Selvaraju, R.R.; Cogswell, M.; Das, A.; Vedantam, R.; Parikh, D.; Batra, D. Grad-CAM: Visual Explanations from Deep Networks via Gradient-Based Localization. Int. J. Comput. Vis. 2020, 128, 336–359. [Google Scholar] [CrossRef] [Green Version]
- Park, J.; Jang, B.G.; Kim, Y.W.; Park, H.; Kim, B.-H.; Kim, M.J.; Ko, H.; Gwak, J.M.; Lee, E.J.; Chung, Y.R. A prospective validation and observer performance study of a deep learning algorithm for pathologic diagnosis of gastric tumors in endoscopic biopsies. Clin. Cancer Res. 2021, 27, 719–728. [Google Scholar] [CrossRef]
- Han, Z.; Wei, B.; Zheng, Y.; Yin, Y.; Li, K.; Li, S. Breast cancer multi-classification from histopathological images with structured deep learning model. Sci. Rep. 2017, 7, 4172. [Google Scholar] [CrossRef]
- Coudray, N.; Ocampo, P.S.; Sakellaropoulos, T.; Narula, N.; Snuderl, M.; Fenyö, D.; Moreira, A.L.; Razavian, N.; Tsirigos, A. Classification and mutation prediction from non-small cell lung cancer histopathology images using deep learning. Nat. Med. 2018, 24, 1559–1567. [Google Scholar] [CrossRef]
- Tainio, K.; Athanasiou, A.; Tikkinen, K.A.O.; Aaltonen, R.; Cárdenas, J.; Hernándes, J.C.; Glazer-Livson, S.; Jakobsson, M.; Joronen, K.; Kiviharju, M.; et al. Clinical course of untreated cervical intraepithelial neoplasia grade 2 under active surveillance: Systematic review and meta-analysis. BMJ 2018, 360, k499. [Google Scholar] [CrossRef] [Green Version]
- Wetstein, S.C.; Stathonikos, N.; Pluim, J.P.W.; Heng, Y.J.; Ter Hoeve, N.D.; Vreuls, C.P.H.; van Diest, P.J.; Veta, M. Deep learning-based grading of ductal carcinoma in situ in breast histopathology images. Lab. Investig. 2021, 101, 525–533. [Google Scholar] [CrossRef]
- Olsson, S.; Akbarian, E.; Lind, A.; Razavian, A.S.; Gordon, M. Automating classification of osteoarthritis according to Kellgren-Lawrence in the knee using deep learning in an unfiltered adult population. BMC Musculoskelet. Disord. 2021, 22, 844. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Yoon, H.; Thakur, N.; Hwang, G.; Lee, E.J.; Kim, C.; Chong, Y. Deep learning-based histopathological segmentation for whole slide images of colorectal cancer in a compressed domain. Sci. Rep. 2021, 11, 22520. [Google Scholar] [CrossRef] [PubMed]
- Wei, L.; Gan, Q.; Ji, T. Cervical cancer histology image identification method based on texture and lesion area features. Comput. Assist. Surg. 2017, 22, 186–199. [Google Scholar] [CrossRef] [PubMed]
- Huang, P.; Tan, X.; Chen, C.; Lv, X.; Li, Y. AF-SENet: Classification of cancer in cervical tissue pathological images based on fusing deep convolution features. Sensors 2021, 21, 122. [Google Scholar] [CrossRef]





| Whole Dataset | Training Set | Test Set | ||||
|---|---|---|---|---|---|---|
| Image N | Patient N | Image N | Patient N | Image N | Patient N | |
| Overall | 1106 | 588 | 989 | 542 | 117 | 68 |
| CIN 3 | 266 | 183 | 236 | 165 | 30 | 19 |
| CIN 2 | 231 | 108 | 210 | 97 | 21 | 11 |
| CIN 1 | 266 | 143 | 234 | 129 | 32 | 14 |
| Non-neoplasm | 343 | 250 | 309 | 225 | 34 | 25 |
| Model/Class | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | F1 Score | AUC (95% CI) |
|---|---|---|---|---|---|---|
| DenseNet-161 | ||||||
| CIN3 | 95.3 (93.7–96.8) | 94.4 (93.1–95.6) | 85.0 (82.3–87.7) | 98.3 (97.8–98.9) | 89.8 (88.8–90.8) | 0.989 (0.982–0.996) |
| CIN2 | 75.2 (67.7–82.8) | 94.1 (91.8–96.4) | 76.1 (62.3–89.9) | 93.8 (92.5–95.0) | 75.5 (64.9–86.1) | 0.947 (0.932–0.963) |
| CIN1 | 82.1 (77.8–86.5) | 98.3 (97.4–99.2) | 94.2 (92.2–96.2) | 94.5 (92.6–96.4) | 87.7 (84.5–91.0) | 0.979 (0.968–0.990) |
| Non-neoplasm | 95.6 (90.9–100.0) | 98.0 (96.3–99.7) | 95.0 (91.0–99.0) | 98.3 (96.6–100.0) | 95.2 (92.0–98.4) | 0.996 (0.991–1.000) |
| EfficientNet-B7 | ||||||
| CIN3 | 97.5 (95.4–99.5) | 96.3 (94.1–98.6) | 90.0 (84.2–95.8) | 99.1 (98.4–99.8) | 93.6 (89.6–97.5) | 0.990 (0.981–0.999) |
| CIN2 | 73.0 (62.2–83.9) | 96.7 (93.7–99.7) | 86.8 (75.2–98.4) | 93.6 (92.3–94.8) | 79.1 (69.1–89.1) | 0.956 (0.946–0.967) |
| CIN1 | 85.2 (73.3–97.1) | 96.3 (95.1–97.6) | 88.5 (88.2–88.8) | 95.5 (91.3–99.8) | 86.5 (80.4–92.6) | 0.971 (0.950–0.993) |
| Non-neoplasm | 95.6 (90.9–100.0) | 96.3 (92.2–100.0) | 92.3 (84.8–99.8) | 98.3 (96.6–100.0) | 93.8 (88.8–98.8) | 0.996 (0.992–0.999) |
| Model/Class | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | F1 Score | AUC (95% CI) |
|---|---|---|---|---|---|---|
| DenseNet-161 | ||||||
| CIN2-3 | 92.0 (86.9–97.1) | 92.4 (85.3–99.6) | 92.5 (87.0–98.0) | 93.4 (90.2–96.7) | 92.1 (88.9–95.3) | 0.981 (0.973–0.989) |
| CIN1 | 80.9 (70.9–90.8) | 96.0 (94.2–97.7) | 87.0 (84.0–89.9) | 94.5 (93.3–95.6) | 83.5 (77.6–89.4) | 0.974 (0.968–0.980) |
| Non-neoplasm | 97.8 (94.2–100.0) | 97.5 (95.6–99.5) | 94.4 (90.0–98.9) | 99.1 (97.6–100.0) | 95.9 (95.5–96.4) | 0.996 (0.992–0.999) |
| EfficientNet-B7 | ||||||
| CIN2-3 | 94.8 (92.8–96.7) | 93.4 (90.1–96.8) | 92.9 (90.3–95.6) | 95.1 (92.3–97.9) | 93.8 (91.7–96.0) | 0.982 (0.971–0.993) |
| CIN1 | 86.1 (82.4–89.7) | 96.4 (95.2–97.5) | 87.6 (81.2–94.0) | 95.6 (94.3–96.9) | 86.8 (82.1–91.4) | 0.979 (0.972–0.985) |
| Non-neoplasm | 94.7 (92.8–96.6) | 98.4 (97.0–99.7) | 96.0 (92.8–99.2) | 97.8 (97.1–98.6) | 95.3 (94.0–96.6) | 0.993 (0.985–1.000) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, B.-J.; Kim, J.-W.; Park, J.; Kwon, G.-Y.; Hong, M.; Jang, S.-H.; Bang, H.; Kim, G.; Park, S.-T. Automated Diagnosis of Cervical Intraepithelial Neoplasia in Histology Images via Deep Learning. Diagnostics 2022, 12, 548. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12020548
Cho B-J, Kim J-W, Park J, Kwon G-Y, Hong M, Jang S-H, Bang H, Kim G, Park S-T. Automated Diagnosis of Cervical Intraepithelial Neoplasia in Histology Images via Deep Learning. Diagnostics. 2022; 12(2):548. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12020548
Chicago/Turabian StyleCho, Bum-Joo, Jeong-Won Kim, Jungkap Park, Gui-Young Kwon, Mineui Hong, Si-Hyong Jang, Heejin Bang, Gilhyang Kim, and Sung-Taek Park. 2022. "Automated Diagnosis of Cervical Intraepithelial Neoplasia in Histology Images via Deep Learning" Diagnostics 12, no. 2: 548. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12020548