
Diagnosis of Visceral Leishmaniasis in an Elimination Setting: A Validation Study of the Diagnostic Algorithm in India

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
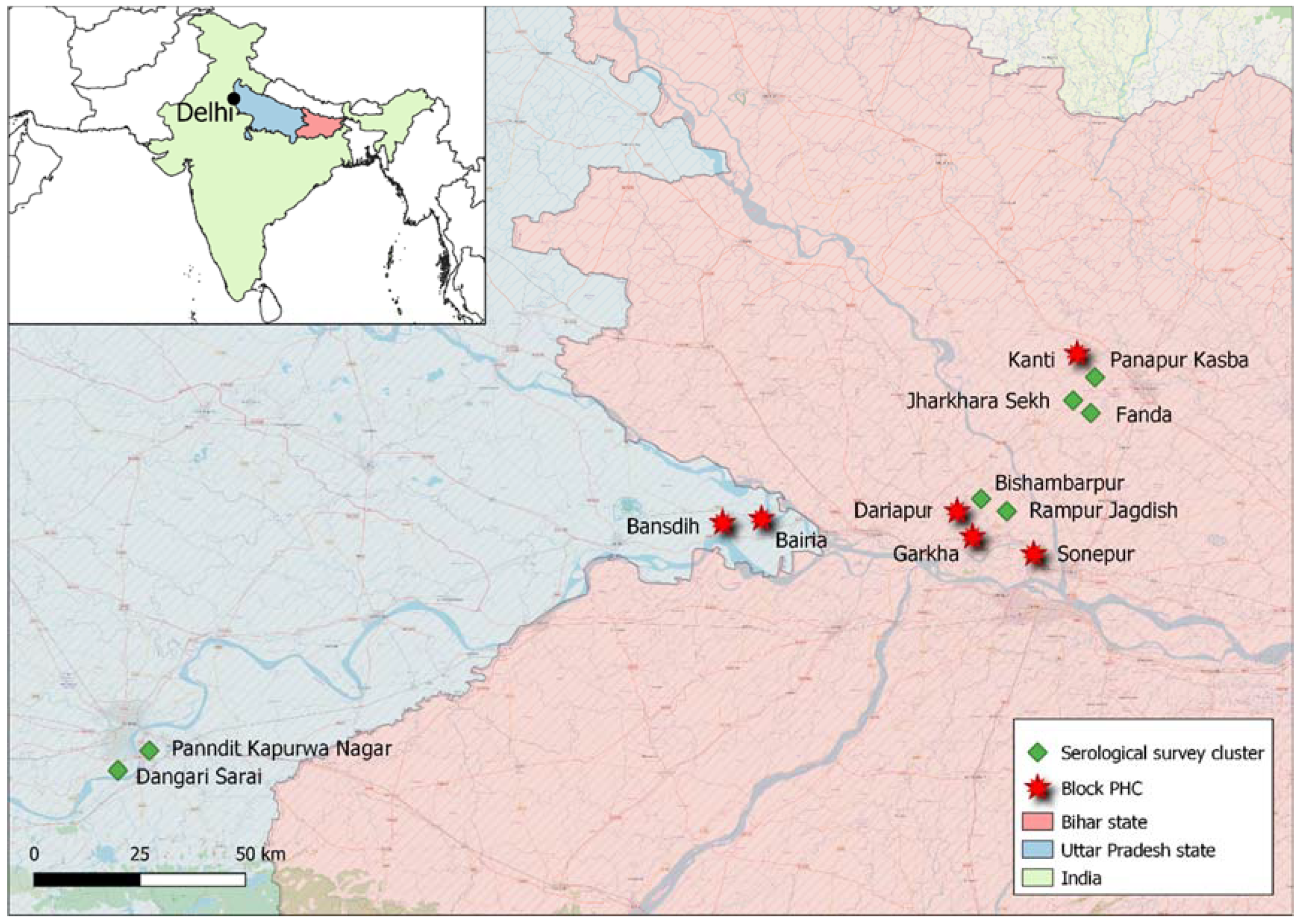
2.1. Field Work and Study Sites
2.2. Sample Testing and Laboratory Analysis
2.3. Data Analysis
3. Results
3.1. Findings among Newly Diagnosed VL Patients at the PHC Level
3.2. Findings among Non-VL Cases
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Global Health Observatory. Number of Cases of Visceral Leishmaniasis Reported; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Rijal, S.; Sundar, S.; Mondal, D.; Das, P.; Alvar, J.; Boelaert, M. Eliminating visceral leishmaniasis in South Asia: The road ahead. BMJ 2019, 364, k5224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gass, K. Time for a diagnostic sea-change: Rethinking neglected tropical disease diagnostics to achieve elimination. PLoS Negl. Trop. Dis. 2020, 14, e0008933. [Google Scholar] [CrossRef] [PubMed]
- Directorate National Vector Borne Disease Control Programme India. Accelerated Plan for Kala-azar Elimination 2017. Available online: https://nvbdcp.gov.in/WriteReadData/l892s/Accelerated-Plan-Kala-azar1-Feb2017.pdf (accessed on 20 January 2022).
- Boelaert, M.; Verdonck, K.; Menten, J.; Sunyoto, T.; van Griensven, J.; Chappuis, F.; Rijal, S. Rapid tests for the diagnosis of visceral leishmaniasis in patients with suspected disease. Cochrane Database Syst. Rev. 2014, Cd009135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sundar, S.; Singh, R.K.; Bimal, S.K.; Gidwani, K.; Mishra, A.; Maurya, R.; Singh, S.K.; Manandhar, K.D.; Boelaert, M.; Rai, M. Comparative evaluation of parasitology and serological tests in the diagnosis of visceral leishmaniasis in India: A phase III diagnostic accuracy study. Trop. Med. Int. Health 2007, 12, 284–289. [Google Scholar] [CrossRef]
- Office of the Registrar General & Census Commissioner, Ministry of Health & Family Welfare, Government of India. Report of the Technical Group on Population Projections for India and States 2011–2036; ORGI: New Delhi, India, 2020; p. 46. [Google Scholar]
- National Center for Vector Borne Diseases Control, Directorate General of Health Services, Ministry of Health & Family Welfare, Government of India. Kala-azar Situation in India; Kala-azar Cases and Deaths in the Country Since 2014. Available online: https://nvbdcp.gov.in/index4.php?lang=1&level=0&linkid=467&lid=3750 (accessed on 17 January 2022).
- Matlashewski, G.; Das, V.N.; Pandey, K.; Singh, D.; Das, S.; Ghosh, A.K.; Pandey, R.N.; Das, P. Diagnosis of visceral leishmaniasis in Bihar India: Comparison of the rK39 rapid diagnostic test on whole blood versus serum. PLoS Negl. Trop. Dis. 2013, 7, e2233. [Google Scholar] [CrossRef] [Green Version]
- Sudarshan, M.; Singh, T.; Singh, A.K.; Chourasia, A.; Singh, B.; Wilson, M.E.; Chakravarty, J.; Sundar, S. Quantitative PCR in epidemiology for early detection of visceral leishmaniasis cases in India. PLoS Negl. Trop. Dis. 2014, 8, e3366. [Google Scholar] [CrossRef] [Green Version]
- de Ruiter, C.M.; van der Veer, C.; Leeflang, M.M.; Deborggraeve, S.; Lucas, C.; Adams, E.R. Molecular tools for diagnosis of visceral leishmaniasis: Systematic review and meta-analysis of diagnostic test accuracy. J. Clin. Microbiol. 2014, 52, 3147–3155. [Google Scholar] [CrossRef] [Green Version]
- Singh, O.P.; Tiwary, P.; Kushwaha, A.K.; Singh, S.K.; Singh, D.K.; Lawyer, P.; Rowton, E.; Chaubey, R.; Singh, A.K.; Rai, T.K.; et al. Xenodiagnosis to evaluate the infectiousness of humans to sandflies in an area endemic for visceral leishmaniasis in Bihar, India: A transmission-dynamics study. Lancet Microbe 2021, 2, e23–e31. [Google Scholar] [CrossRef]
- Sudarshan, M.; Singh, T.; Chakravarty, J.; Sundar, S. A Correlative Study of Splenic Parasite Score and Peripheral Blood Parasite Load Estimation by Quantitative PCR in Visceral Leishmaniasis. J. Clin. Microbiol. 2015, 53, 3905–3907. [Google Scholar] [CrossRef] [Green Version]
- Hossain, F.; Ghosh, P.; Khan, M.A.A.; Duthie, M.S.; Vallur, A.C.; Picone, A.; Howard, R.F.; Reed, S.G.; Mondal, D. Real-time PCR in detection and quantitation of Leishmania donovani for the diagnosis of Visceral Leishmaniasis patients and the monitoring of their response to treatment. PLoS ONE 2017, 12, e0185606. [Google Scholar] [CrossRef]
- Chappuis, F.; Sundar, S.; Hailu, A.; Ghalib, H.; Rijal, S.; Peeling, R.W.; Alvar, J.; Boelaert, M. Visceral leishmaniasis: What are the needs for diagnosis, treatment and control? Nat. Rev. Microbiol. 2007, 5, 873–882. [Google Scholar] [CrossRef] [PubMed]
- Adhya, S.; Chatterjee, M.; Hassan, M.Q.; Mukherjee, S.; Sen, S. Detection of Leishmania in the blood of early kala-azar patients with the aid of the polymerase chain reaction. Trans. R. Soc. Trop. Med. Hyg. 1995, 89, 622–624. [Google Scholar] [CrossRef]
- Moulik, S.; Sengupta, S.; Chatterjee, M. Molecular Tracking of the Leishmania Parasite. Front. Cell. Infect. Microbiol. 2021, 11, 623437. [Google Scholar] [CrossRef] [PubMed]
- Salotra, P.; Sreenivas, G.; Pogue, G.P.; Lee, N.; Nakhasi, H.L.; Ramesh, V.; Negi, N.S. Development of a species-specific PCR assay for detection of Leishmania donovani in clinical samples from patients with kala-azar and post-kala-azar dermal leishmaniasis. J. Clin. Microbiol. 2001, 39, 849–854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- da Costa Lima, M.S.J.; Zorzenon, D.C.R.; Dorval, M.E.C.; Pontes, E.R.J.C.; Oshiro, E.T.; Cunha, R.; Andreotti, R.; Matos, M.D.F.C. Sensitivity of PCR and real-time PCR for the diagnosis of human visceral leishmaniasis using peripheral blood. Asian Pac. J. Trop. Dis. 2013, 3, 10–15. [Google Scholar] [CrossRef]
- Silva, L.A.; Romero, H.D.; Fagundes, A.; Nehme, N.; Fernandes, O.; Rodrigues, V.; Costa, R.T.; Prata, A. Use of the polymerase chain reaction for the diagnosis of asymptomatic leishmania infection in a visceral leishmaniasis-endemic area. Rev. Inst. Med. Trop. Sao Paulo 2013, 55, 101–104. [Google Scholar] [CrossRef] [Green Version]
- Abbasi, I.; Aramin, S.; Hailu, A.; Shiferaw, W.; Kassahun, A.; Belay, S.; Jaffe, C.; Warburg, A. Evaluation of PCR procedures for detecting and quantifying Leishmania donovani DNA in large numbers of dried human blood samples from a visceral leishmaniasis focus in Northern Ethiopia. BMC Infect. Dis. 2013, 13, 153. [Google Scholar] [CrossRef] [Green Version]
- Deborggraeve, S.; Boelaert, M.; Rijal, S.; De Doncker, S.; Dujardin, J.C.; Herdewijn, P.; Buscher, P. Diagnostic accuracy of a new Leishmania PCR for clinical visceral leishmaniasis in Nepal and its role in diagnosis of disease. Trop. Med. Int. Health 2008, 13, 1378–1383. [Google Scholar] [CrossRef] [Green Version]
- Srivastava, P.; Gidwani, K.; Picado, A.; Van der Auwera, G.; Tiwary, P.; Ostyn, B.; Dujardin, J.C.; Boelaert, M.; Sundar, S. Molecular and serological markers of Leishmania donovani infection in healthy individuals from endemic areas of Bihar, India. Trop. Med. Int. Health 2013, 18, 548–554. [Google Scholar] [CrossRef]
- Das, V.N.; Siddiqui, N.A.; Verma, R.B.; Topno, R.K.; Singh, D.; Das, S.; Ranjan, A.; Pandey, K.; Kumar, N.; Das, P. Asymptomatic infection of visceral leishmaniasis in hyperendemic areas of Vaishali district, Bihar, India: A challenge to kala-azar elimination programmes. Trans. R. Soc. Trop. Med. Hyg. 2011, 105, 661–666. [Google Scholar] [CrossRef]
- Bhattarai, N.R.; Van der Auwera, G.; Khanal, B.; De Doncker, S.; Rijal, S.; Das, M.L.; Uranw, S.; Ostyn, B.; Praet, N.; Speybroeck, N.; et al. PCR and direct agglutination as Leishmania infection markers among healthy Nepalese subjects living in areas endemic for Kala-Azar. Trop. Med. Int. Health 2009, 14, 404–411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sudarshan, M.; Sundar, S. Parasite load estimation by qPCR differentiates between asymptomatic and symptomatic infection in Indian visceral leishmaniasis. Diagn. Microbiol. Infect. Dis. 2014, 80, 40–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burza, S.; Croft, S.L.; Boelaert, M. Leishmaniasis. Lancet 2018, 392, 951–970. [Google Scholar] [CrossRef]
- van Griensven, J.; Diro, E. Visceral Leishmaniasis: Recent Advances in Diagnostics and Treatment Regimens. Infect. Dis. Clin. N. Am. 2019, 33, 79–99. [Google Scholar] [CrossRef] [PubMed]
- Boelaert, M.; Rijal, S.; Regmi, S.; Singh, R.; Karki, B.; Jacquet, D.; Chappuis, F.O.; Campino, L.; Desjeux, P.; Le Ray, D.; et al. A comparative study of the effectiveness of diagnostic tests for visceral leishmaniasis. Am. J. Trop. Med. Hyg. 2004, 70, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Medley, G.F.; Hollingsworth, T.D.; Olliaro, P.L.; Adams, E.R. Health-seeking behaviour, diagnostics and transmission dynamics in the control of visceral leishmaniasis in the Indian subcontinent. Nature 2015, 528, S102–S108. [Google Scholar] [CrossRef] [Green Version]
- Jeronimo, S.M.B.; De Queiroz Sousa, A.; Pearson, R.D. Leishmaniasis. In Tropical Infectious Diseases: Principles, Pathogens and Practice, 3rd ed.; Guerrant, R.L., Walker, D.H., Weller, P.F., Eds.; Saunders Elsevier: Philadephia, PA, USA, 2011; p. 696. [Google Scholar]
- Alvar, J.; Aparicio, P.; Aseffa, A.; Den Boer, M.; Canavate, C.; Dedet, J.P.; Gradoni, L.; Ter Horst, R.; Lopez-Velez, R.; Moreno, J. The relationship between leishmaniasis and AIDS: The second 10 years. Clin. Microbiol. Rev. 2008, 21, 334–359. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Participant Characteristics (n = 74) | Results | ||||
|---|---|---|---|---|---|
| State | Block | Median Age (y) (IQR) | Males (n (%)) | PCR Available (n) | PCR Positive (n (%)) |
| Bihar | Dariapur | 32 (16–50) | 29 (57%) | 51 | 49 (96%) |
| Bihar | Garkha | NA | NA | 0 | NA |
| Bihar | Sonepur | 24 (16–40) | 9 (75%) | 12 | 10 (83%) |
| Bihar | Kanti | 30 (30–30) | 1 (100%) | 1 | 1 (100%) |
| UP | Bairia | 23 (15–32) | 5 (50%) | 10 | 10 (100%) |
| UP | Bansdih | NA | NA | 0 | NA |
| Overall | 29 (16–41) | 44 (61%) | 74 | 70 (95%) | |
| Participant Characteristics (n = 15,422) | Results | |||||
|---|---|---|---|---|---|---|
| State | Cluster | Median Age (y) (IQR) | Males (n (%)) | rK39 RDT Available (n) | rK39 RDT Positive (n (%)) | |
| CE | Bihar | Rampur Jagdish | 18 (10–38) | 1220 (44%) | 2772 | 6 (0.22%) |
| Bihar | Bishambarpur | 24 (12–24) | 1281 (46%) | 2756 | 17 (0.62%) | |
| PE | Bihar | Jhakara Sekh | 20 (10–39) | 1152 (48%) | 2417 | 2 (0.08%) |
| Bihar | Fanda | 22 (11–40) | 1384 (47%) | 2944 | 12 (0.41%) | |
| UP | Panndit K.N. | 22 (12–37) | 311 (46%) | 679 | 2 (0.29%) | |
| NE | Bihar | Panapur Kasba | 28 (14–48) | 385 (49%) | 787 | 0 (0.00%) |
| UP | Dangari Sarai | 25 (15–42) | 1485 (48%) | 3067 | 0 (0.00%) | |
| Overall | 23 (12–40) | 7219 (47%) | 15,422 | 39 (0.25%) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cloots, K.; Singh, O.P.; Singh, A.K.; Kushwaha, A.K.; Malaviya, P.; Kansal, S.; Hasker, E.; Sundar, S. Diagnosis of Visceral Leishmaniasis in an Elimination Setting: A Validation Study of the Diagnostic Algorithm in India. Diagnostics 2022, 12, 670. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12030670
Cloots K, Singh OP, Singh AK, Kushwaha AK, Malaviya P, Kansal S, Hasker E, Sundar S. Diagnosis of Visceral Leishmaniasis in an Elimination Setting: A Validation Study of the Diagnostic Algorithm in India. Diagnostics. 2022; 12(3):670. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12030670
Chicago/Turabian StyleCloots, Kristien, Om Prakash Singh, Abhishek Kumar Singh, Anurag Kumar Kushwaha, Paritosh Malaviya, Sangeeta Kansal, Epco Hasker, and Shyam Sundar. 2022. "Diagnosis of Visceral Leishmaniasis in an Elimination Setting: A Validation Study of the Diagnostic Algorithm in India" Diagnostics 12, no. 3: 670. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12030670