
Association of Non-Alcoholic Fatty Liver Disease and Hepatic Fibrosis with Epicardial Adipose Tissue Volume and Atrial Deformation Mechanics in a Large Asian Population Free from Clinical Heart Failure

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
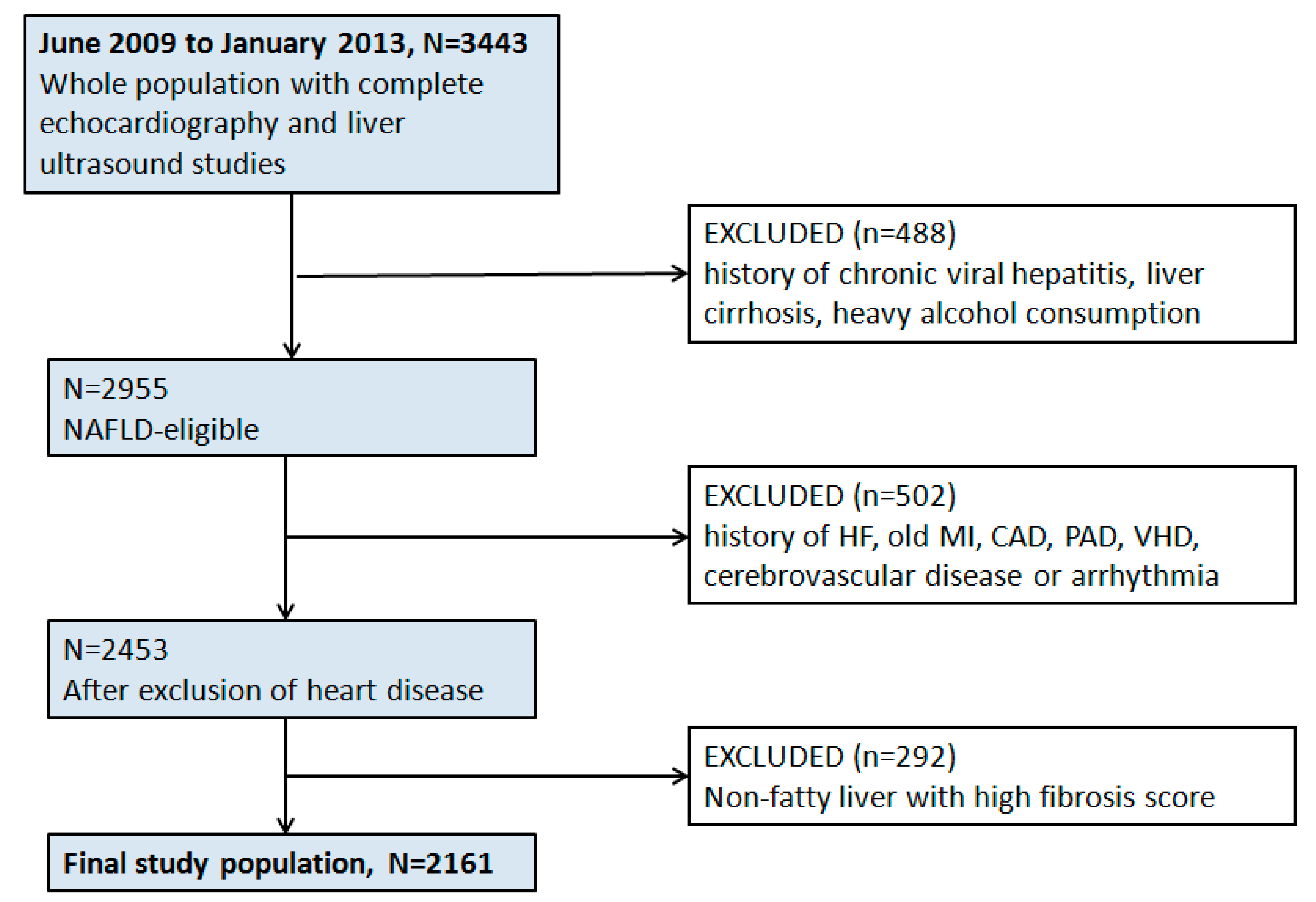
2.1. Study Population
2.2. Laboratory Data and Body Fat Assessment
2.3. Assessment of Fatty Liver and Fibrosis Score
2.4. Assessment of Epicardial Fat
2.5. Conventional Echocardiography and Diastolic Function Indices
2.6. Two-Dimensional Speckle-Tracking Analysis Protocol
2.7. Statistical Analysis
3. Results
3.1. Baseline Demographics, Adiposity Measures, and Metabolic Profiles
3.2. Cardiac Structures, Diastolic Function and Strain Indices
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Eslam, M.; Newsome, P.N.; Sarin, S.K.; Anstee, Q.M.; Targher, G.; Romero-Gomez, M.; Zelber-Sagi, S.; Wong, V.W.-S.; Dufour, J.-F.; Schattenberg, J.M.; et al. A new definition for metabolic dysfunction-associated fatty liver disease: An international expert consensus statement. J. Hepatol. 2020, 73, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Rinella, M.E.; Sanyal, A.J.; Harrison, S.A.; Brunt, E.M.; Goodman, Z.; Cohen, D.E.; Loomba, R. From NAFLD to MAFLD: Implications of a Premature Change in Terminology. Hepatology 2020, 73, 1194–1198. [Google Scholar] [CrossRef]
- Anstee, Q.M.; Targher, G.; Day, C.P. Progression of NAFLD to diabetes mellitus, cardiovascular disease or cirrhosis. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 330–344. [Google Scholar] [CrossRef] [PubMed]
- McPherson, S.; Hardy, T.; Henderson, E.; Burt, A.D.; Day, C.P.; Anstee, Q.M. Evidence of NAFLD progression from steatosis to fibrosing-steatohepatitis using paired biopsies: Implications for prognosis and clinical management. J. Hepatol. 2015, 62, 1148–1155. [Google Scholar] [CrossRef] [PubMed]
- Adams, L.A.; Anstee, Q.M.; Tilg, H.; Targher, G. Non-alcoholic fatty liver disease and its relationship with cardiovascular disease and other extrahepatic diseases. Gut 2017, 66, 1138–1153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Francque, S.M.; van der Graaff, D.; Kwanten, W. Non-alcoholic fatty liver disease and cardiovascular risk: Pathophysiological mechanisms and implications. J. Hepatol. 2016, 65, 425–443. [Google Scholar] [CrossRef] [Green Version]
- Sperling, L.S.; Mechanick, J.I.; Neeland, I.J.; Herrick, C.J.; Després, J.P.; Ndumele, C.E.; Vijayaraghavan, K.; Handelsman, Y.; Puckrein, G.A.; Araneta, M.R.; et al. The CardioMetabolic Health Alliance: Working toward a new care model for the metabolic syndrome. J. Am. Coll. Cardiol. 2015, 66, 1050–1067. [Google Scholar] [CrossRef] [Green Version]
- Cusi, K. Role of obesity and lipotoxitcity in the development of nonalcoholic steatohepatitis: Pathophysiology and clinical implications. Gastroenterology 2012, 142, 711.e6–725.e6. [Google Scholar] [CrossRef]
- Lai, Y.-H.; Yun, C.-H.; Yang, F.-S.; Liu, C.-C.; Wu, Y.-J.; Kuo, J.-Y.; Yeh, H.-I.; Lin, T.-Y.; Bezerra, H.G.; Shih, S.-C.; et al. Epicardial Adipose Tissue Relating to Anthropometrics, Metabolic Derangements and Fatty Liver Disease Independently Contributes to Serum High-Sensitivity C-Reactive Protein Beyond Body Fat Composition: A Study Validated with Computed Tomography. J. Am. Soc. Echocardiogr. 2012, 25, 234–241. [Google Scholar] [CrossRef]
- Lai, Y.-H.; Hou, C.J.-Y.; Yun, C.-H.; Sung, K.-T.; Su, C.-H.; Wu, T.-H.; Yang, F.-S.; Hung, T.-C.; Hung, C.-L.; Bezerra, H.G.; et al. The association among MDCT-derived three-dimensional visceral adiposities on cardiac diastology and dyssynchrony in asymptomatic population. BMC Cardiovasc. Disord. 2015, 15, 142. [Google Scholar] [CrossRef] [Green Version]
- Kankaanpää, M.; Lehto, H.R.; Pärkkä, J.P.; Komu, M.; Viljanen, A.; Ferrannini, E.; Knuuti, J.; Nuutila, P.; Parkkola, R.; Iozzo, P. Myocardial triglyceride content and epicardial adipose mass in human obesity: Relationship to left ventricular function and serum free fatty acid levels. J. Clin. Endocrinol. Metab. 2006, 91, 4689–4695. [Google Scholar] [CrossRef] [PubMed]
- Fitzgibbons, T.P.; Czech, M.P. Epicardial and Perivascular Adipose Tissues and Their Influence on Cardiovascular Disease: Basic Mechanisms and Clinical Associations. J. Am. Hear. Assoc. 2014, 3, e000582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obokata, M.; Reddy, Y.; Pislaru, S.; Melenovsky, V.; Borlaug, B.A. Evidence Supporting the Existence of a Distinct Obese Phenotype of Heart Failure with Preserved Ejection Fraction. Circulation 2017, 136, 6–19. [Google Scholar] [CrossRef] [PubMed]
- VanWagner, L.B.; Wilcox, J.E.; Colangelo, L.A.; Lloyd-Jones, D.; Carr, J.J.; Lima, J.A.; Lewis, C.E.; Rinella, M.E.; Shah, S.J. Association of nonalcoholic fatty liver disease with subclinical myocardial remodeling and dysfunction: A population-based study. Hepatology 2015, 62, 773–783. [Google Scholar] [CrossRef] [PubMed]
- VanWagner, L.B.; Wilcox, J.E.; Ning, H.; Lewis, C.E.; Carr, J.J.; Rinella, M.E.; Shah, S.J.; Lima, J.A.C.; Lloyd-Jones, D.M. Lon-gitudinal association of non-alcoholic fatty liver disease with changes in myocardial structure and function: The CARDIA Study. J. Am. Heart Assoc. 2020, 9, e014279. [Google Scholar] [CrossRef] [PubMed]
- Petta, S.; Argano, C.; Colomba, D.; Cammà, C.; Di Marco, V.; Cabibi, D.; Tuttolomondo, A.; Marchesini, G.; Pinto, A.; Licata, G.; et al. Epicardial fat, cardiac geometry and cardiac function in patients with non-alcoholic fatty liver disease: Association with the severity of liver disease. J. Hepatol. 2014, 62, 928–933. [Google Scholar] [CrossRef] [PubMed]
- Pacifico, L.; Di Martino, M.; De Merulis, A.; Bezzi, M.; Osborn, J.F.; Catalano, C.; Chiesa, C. Left ventricular dysfunction in obese children and adolescents with nonalcoholic fatty liver disease. Hepatology 2013, 59, 461–470. [Google Scholar] [CrossRef] [Green Version]
- Angulo, P.; Hui, J.M.; Marchesini, G.; Bugianesi, E.; George, J.; Farrell, G.C.; Enders, F.; Saksena, S.; Burt, A.D.; Bida, J.P.; et al. The NAFLD fibrosis score: A noninvasive system that identifies liver fibrosis in patients with NAFLD. Hepatology 2007, 45, 846–854. [Google Scholar] [CrossRef]
- Zeb, I.; Li, D.; Budoff, M.J.; Katz, R.; Lloyd-Jones, D.; Agatston, A.; Blumenthal, R.S.; Blaha, M.J.; Blankstein, R.; Carr, J.; et al. Nonalcoholic fatty liver disease and incident cardiac events: The Multi-Ethnic Study of Atherosclerosis. J. Am. Coll. Cardiol. 2016, 67, 1965–1966. [Google Scholar] [CrossRef]
- Kim, D.; Kim, W.R.; Kim, H.J.; Therneau, T.M. Association between noninvasive fibrosis markers and mortality among adults with nonalcoholic fatty liver disease in the United States. Hepatology 2012, 57, 1357–1365. [Google Scholar] [CrossRef] [Green Version]
- Hung, C.-L.; Gonçalves, A.; Lai, Y.-J.; Lai, Y.-H.; Sung, K.-T.; Lo, C.-I.; Liu, C.-C.; Kuo, J.-Y.; Hou, C.J.-Y.; Chao, T.-F.; et al. Light to Moderate Habitual Alcohol Consumption Is Associated with Subclinical Ventricular and Left Atrial Mechanical Dysfunction in an Asymptomatic Population: Dose-Response and Propensity Analysis. J. Am. Soc. Echocardiogr. 2016, 29, 1043.e4–1051.e4. [Google Scholar] [CrossRef] [PubMed]
- Osawa, H.; Mori, Y. Sonographic diagnosis of fatty liver using a histogram technique that compares liver and renal cortical echo amplitudes. J. Clin. Ultrasound 1996, 24, 25–29. [Google Scholar] [CrossRef]
- Papadopoulos, N.; Vasileiadi, S.; Papavdi, M.; Sveroni, E.; Antonakaki, P.; Dellaporta, E.; Koutli, E.; Michalea, S.; Manolakopoulos, S.; Koskinas, J.; et al. Liver fibrosis staging with combination of APRI and FIB-4 scoring systems in chronic hepatitis C as an alternative to transient elastography. Ann. Gastroenterol. 2019, 32, 498–503. [Google Scholar] [CrossRef]
- Yun, C.-H.; Lin, T.-Y.; Wu, Y.-J.; Liu, C.-C.; Kuo, J.-Y.; Yeh, H.-I.; Yang, F.-S.; Chen, S.-C.; Hou, C.J.-Y.; Bezerra, H.G.; et al. Pericardial and thoracic peri-aortic adipose tissues contribute to systemic inflammation and calcified coronary atherosclerosis independent of body fat composition, anthropometric measures and traditional cardiovascular risks. Eur. J. Radiol. 2012, 81, 749–756. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39. [Google Scholar] [CrossRef] [Green Version]
- Chang, W.; Wang, Y.; Sun, L.; Yu, N.; Li, Y.; Li, G. Evaluation of left atrial function in type 2 diabetes mellitus patients with nonalcoholic fatty liver disease by two-dimensional speckle tracking echocardiography. Echocardiography 2019, 36, 1290–1297. [Google Scholar] [CrossRef]
- Kocabay, G.; Karabay, C.Y.; Colak, Y.; Oduncu, V.; Kalayci, A.; Akgun, T.; Guler, A.; Kirma, C. Left atrial deformation pa-rameters in patients with non-alcoholic fatty liver disease: A 2D speckle tracking imaging study. Clin. Sci. 2014, 126, 297–304. [Google Scholar] [CrossRef]
- Wijarnpreecha, K.; Lou, S.; Panjawatanan, P.; Cheungpasitporn, W.; Pungpapong, S.; Lukens, F.J.; Ungprasert, P. Association between diastolic cardiac dysfunction and nonalcoholic fatty liver disease: A systematic review and meta-analysis. Dig. Liver Dis. 2018, 50, 1166–1175. [Google Scholar] [CrossRef]
- Goland, S.; Shimoni, S.; Zornitzki, T.; Knobler, H.; Azoulai, O.; Lutaty, G.; Melzer, E.; Orr, A.; Caspi, A.; Malnick, S. Cardiac abnormalities as a new manifestation of nonalcoholic fatty liver disease: Echocardiographic and tissue Doppler imaging as-sessment. J. Clin. Gastroenterol. 2006, 40, 949–955. [Google Scholar] [CrossRef]
- Fotbolcu, H.; Yakar, T.; Duman, D.; Karaahmet, T.; Tigen, K.; Cevik, C.; Kurtoglu, U.; Dindar, I. Impairment of the left ven-tricular systolic and diastolic function in patients with non-alcoholic fatty liver disease. Cardiol. J. 2010, 17, 457–463. [Google Scholar]
- Singh, G.K.; Vitola, B.E.; Holland, M.R.; Sekarski, T.; Patterson, B.W.; Magkos, F.; Klein, S. Alterations in Ventricular Structure and Function in Obese Adolescents with Nonalcoholic Fatty Liver Disease. J. Pediatr. 2013, 162, 1160.e1–1168.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bugianesi, E. Nonalcoholic fatty liver disease (NAFLD) and cardiac lipotoxicity: Another piece of the puzzle. Hepatology 2008, 47, 2–4. [Google Scholar] [CrossRef] [PubMed]
- Itier, R.; Guillaume, M.; Ricci, J.; Roubille, F.; Delarche, N.; Picard, F.; Galinier, M.; Roncalli, J. Non-alcoholic fatty liver disease and heart failure with preserved ejection fraction: From pathophysiology to practical issues. ESC Hear. Fail. 2021, 8, 789–798. [Google Scholar] [CrossRef] [PubMed]
- Packer, M. Atrial Fibrillation and Heart Failure with Preserved Ejection Fraction in Patients With Nonalcoholic Fatty Liver Disease. Am. J. Med. 2020, 133, 170–177. [Google Scholar] [CrossRef] [PubMed]
- Yoshihisa, A.; Sato, Y.; Yokokawa, T.; Sato, T.; Suzuki, S.; Oikawa, M.; Kobayashi, A.; Yamaki, T.; Kunii, H.; Nakazato, K.; et al. Liver fibrosis score predicts mortality in heart failure patients with preserved ejection fraction. ESC Hear. Fail. 2018, 5, 262–270. [Google Scholar] [CrossRef] [PubMed]
- Lai, Y.-H.; Liu, L.; Sung, K.-T.; Tsai, J.-P.; Huang, W.-H.; Yun, C.-H.; Lin, J.-L.; Chen, Y.-J.; Su, C.-H.; Hung, T.-C.; et al. Diverse Adiposity and Atrio-Ventricular Dysfunction across Obesity Phenotypes: Implication of Epicardial Fat Analysis. Diagnostics 2021, 11, 408. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.; Ganesan, A.; Selvanayagam, J.B. Epicardial fat and atrial fibrillation: Current evidence, potential mechanisms, clinical implications, and future directions. Eur. Hear. J. 2017, 38, ehw045–1302. [Google Scholar] [CrossRef] [Green Version]
- Donal, E.; Galli, E.; Schnell, F. Left atrial strain: A must or a plus for routine clinical practice? Circ. Cardiovasc. Imaging. 2017, 10, e007023. [Google Scholar] [CrossRef] [Green Version]
- Mehrzad, R.; Rajab, M.; Spodick, D.H. The Three Integrated Phases of Left Atrial Macrophysiology and Their Interactions. Int. J. Mol. Sci. 2014, 15, 15146–15160. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Non-Fatty Liver | NAFLD, Low Fibrosis Score (<−1.455) | NAFLD, High Fibrosis Score (≥−1.455) | Ptrend | |
|---|---|---|---|---|
| N = 1019 | N = 840 | N = 302 | ||
| Age, years | 46.32(9.96) | 47.69(9.1) * | 56.37(8.34) *† | <0.001 |
| Female sex, % | 502 (49.3%) | 211 (25.1%) * | 76 (25.2%) * | <0.001 |
| NAFLD Fibrosis score | −2.76(0.79) | −2.67(0.79) * | −0.82(0.54) *† | <0.001 |
| FIB-4 score | 0.86(0.34) | 0.93(0.29) * | 1.35(0.48) *† | <0.001 |
| APRI score | 0.23(0.15) | 0.37(0.26) * | 0.42(0.28) *† | <0.001 |
| SBP, mmHg | 116.93(15.14) | 123.86(16.42) * | 129.21(16.03) *† | <0.001 |
| DBP, mmHg | 72.76(10.22) | 78.04(10.21) * | 80.45(10.06) *† | <0.001 |
| Adiposity measures | ||||
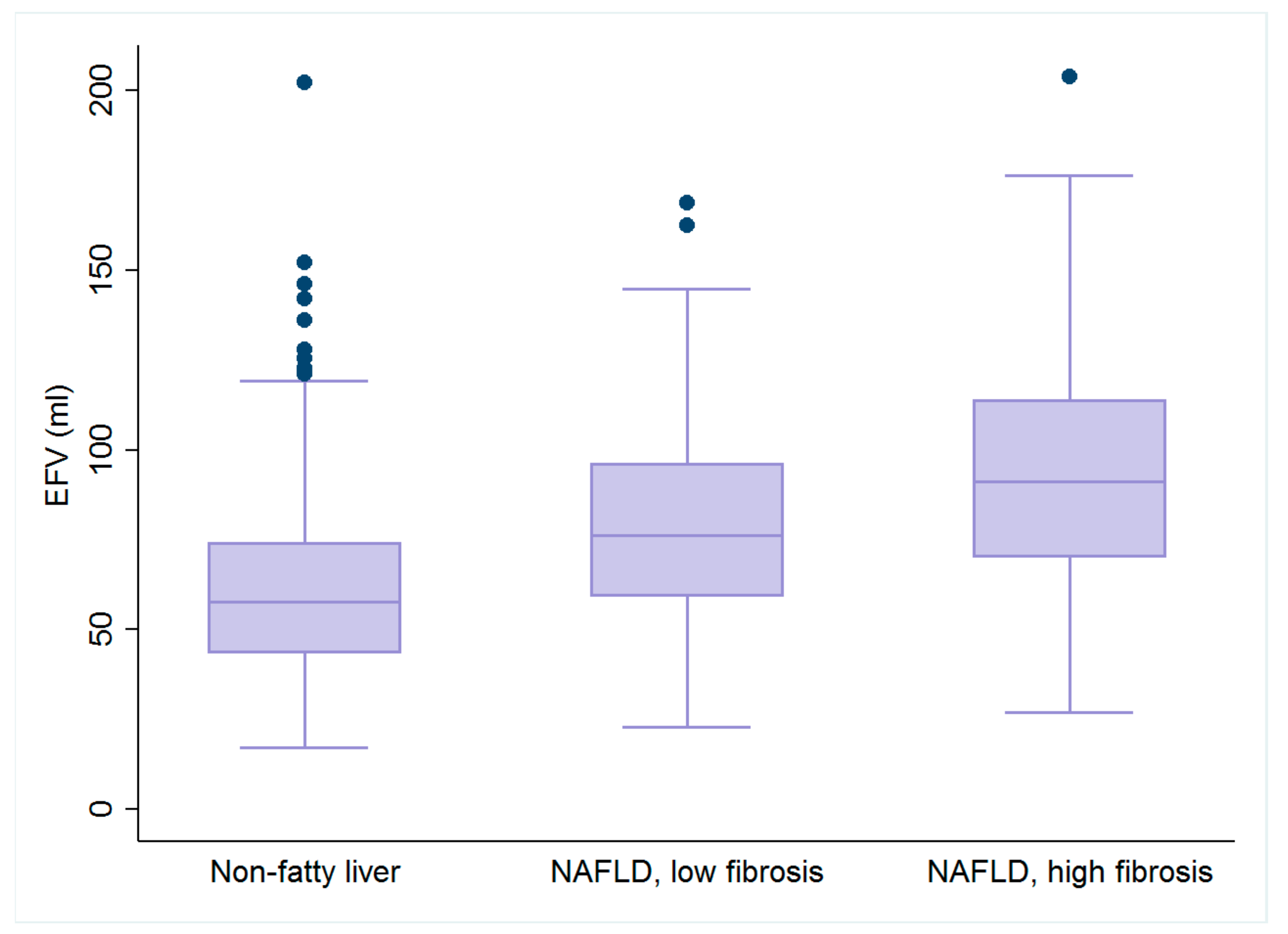
| EFV, ml | 65.02(25.5) | 79.73(26.25) * | 95.13(31.67) *† | <0.001 |
| BMI, kg/m2 | 22.26(2.58) | 25.69(3.17) * | 27.21(3.53) *† | <0.001 |
| WC, cm | 77.86(7.9) | 87.29(8.24) * | 91.06(9.46) *† | <0.001 |
| Body fat, % | 23.84(6.26) | 27.42(7.38) * | 28.9(7.61) *† | <0.001 |
| Biomarkers | ||||
| Fasting glucose, mg/dl | 93.53(10.59) | 100.15(18.17) * | 118.17(32.1) *† | <0.001 |
| HbA1c, % | 5.54(0.44) | 5.74(0.66) * | 6.32(1.18) *† | <0.001 |
| Fasting insulin, U/L | 6.62(3.61) | 10.01(6.16) * | 10.86(5.81) * | <0.001 |
| HOMA-IR | 1.53(0.94) | 2.5(1.78) * | 3.23(2.05) *† | <0.001 |
| Hs-CRP, mg/L | 1.61(4.36) | 2.42(4.16) * | 2.67(3.73) * | 0.001 |
| Platelet, 109/L | 257.15(46.67) | 243.96(48.03) * | 207.87(32.99) *† | <0.001 |
| PT-INR | 1.04(0.04) | 1.03(0.05) * | 1.04(0.05) | 0.03 |
| GOT, IU/L | 21.21(7.46) | 26.11(11.3) * | 28.1(14.57) *† | <0.001 |
| GPT, IU/L | 21.41(12.29) | 36.42(24.24) * | 34.44(21.94) * | <0.001 |
| GGT, IU/L | 20.55(18.49) | 34.28(40.76) * | 35.79(48.43) * | <0.001 |
| Bil(d), mg/dL | 0.21(0.07) | 0.2(0.07) | 0.22(0.08) | 0.06 |
| Bil(t), mg/dL | 0.78(0.34) | 0.81(0.36) | 0.83(0.37) | 0.06 |
| Albumin, g/dL | 4.52(0.25) | 4.59(0.24) * | 4.46(0.24) *† | <0.001 |
| TC, mg/dL | 200.91(36.12) | 211.29(36.5) * | 207.02(35.7) * | <0.001 |
| TG, mg/dL | 106.33(78.63) | 167.19(95.16) * | 170.79(111.15) * | <0.001 |
| LDL-C, mg/dL | 127.15(33.83) | 140.58(33.38) * | 136.89(31.84) * | <0.001 |
| HDL-C, mg/dL | 60.64(15.49) | 48.77(12.45) * | 47.96(11.41) * | <0.001 |
| eGFR, mL/min/m2 | 91.78(16.6) | 89.3(15.2) * | 85.39(16.84) *† | 0.001 |
| Comorbidities | ||||
| Hypertension, % | 82 (8%) | 149 (17.7%) * | 93 (30.8%) *† | <0.001 |
| Diabetes, % | 17 (1.7%) | 65 (7.7%) | 77 (25.5) *† | <0.001 |
| Hyperlipidemia, % | 43 (4.2%) | 64 (7.6%) | 36 (11.9%) * | <0.001 |
| Non-Fatty Liver | NAFLD, Low Fibrosis Score (<−1.455) | NAFLD, High Fibrosis Score (≥−1.455) | Ptrend | |
|---|---|---|---|---|
| N = 1019 | N = 840 | N = 302 | ||
| LVST, mm | 8.6(1.03) | 9.14(0.96) * | 9.54(1.02) *† | <0.001 |
| LVPT, mm | 8.6(0.94) | 9.13(0.88) * | 9.48(0.95) *† | <0.001 |
| RWT | 0.38(0.04) | 0.39(0.04) * | 0.4(0.04) *† | <0.001 |
| LVEDV, mL | 72.44(13.36) | 77.26(12.48) * | 80.75(11.04) *† | <0.001 |
| LVEF, % | 62.79(5.05) | 62.16(5.2) * | 62.34(5.08) | 0.03 |
| LVM, gm | 129.66(29.83) | 146.4(27.82) * | 159.65(30.33) *† | <0.001 |
| LVMi(BSA), gm/m2 | 72.32(13.73) | 74.89(12.56) * | 80.42(13.79) *† | <0.001 |
| LVMi, gm/m2.7 | 33.66(7.13) | 36.86(7.11) * | 41.08(7.94) *† | <0.001 |
| LAV, mL | 26.69(8.92) | 31.44(11.22) * | 35.63(12.48) *† | <0.001 |
| LAEF, % | 58.9(10.59) | 57.72(10.73) | 56.94(10.48) * | 0.006 |
| Diastolic function | ||||
| DT, ms | 196.21(37.2) | 201.19(35.32) * | 214.5(40.65) *† | 0.001 |
| IVRT, ms | 87.76(13.49) | 89.87(13.64) * | 94.03(18.93) *† | <0.001 |
| E/A | 1.4(0.49) | 1.19(0.37) * | 1.04(0.36) *† | <0.001 |
| LV e’, cm/sec | 10.27(2.39) | 9.11(2.04) * | 7.85(1.88) *† | <0.001 |
| LV s’, cm/sec | 8.49(1.52) | 8.32(2.07) | 7.98(1.45) *† | <0.001 |
| E/e’ | 6.71(2.21) | 7.11(2.43) * | 8.08(3.05) *† | <0.001 |
| Strain indices | ||||
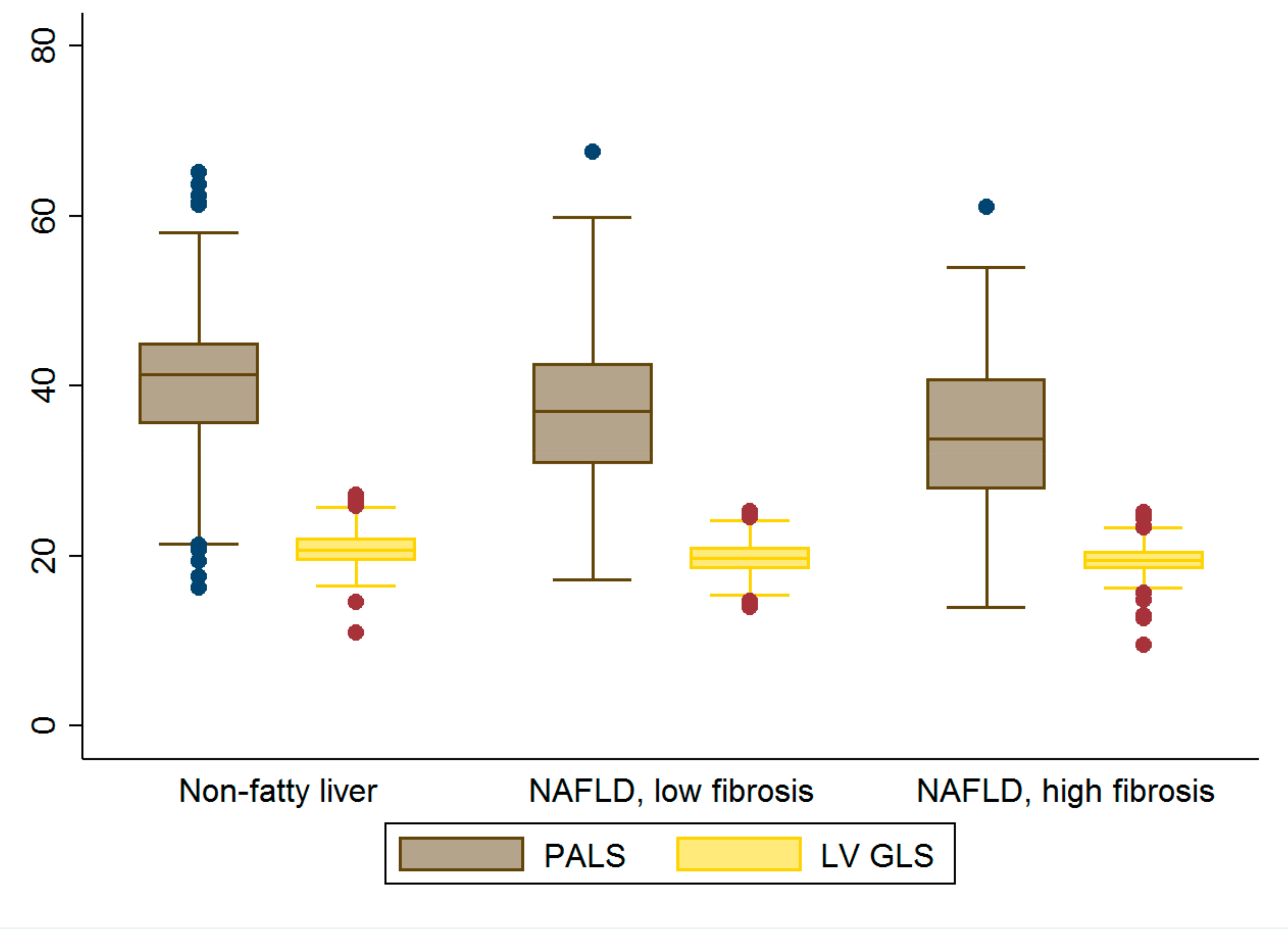
| LV GLS, % | 20.85(1.91) | 19.78(1.6) * | 19.53(1.71) * | <0.001 |
| PALS, % | 40.23(7.39) | 36.96(7.77) * | 34.05(8.01) *† | <0.001 |
| ALSRsyst | 1.78(0.38) | 1.66(0.36) * | 1.52(0.35) *† | <0.001 |
| ALSRearly | 2(0.54) | 1.66(0.49) * | 1.35(0.45) *† | <0.001 |
| ALSRlate | 2(0.49) | 2.07(0.5) * | 2.05(0.49) | 0.006 |
| LAstiff | 0.17(0.08) | 0.2(0.09) * | 0.26(0.15) *† | <0.001 |
| Pearson r | Univariate Model | Multivariate Model 1 | Multivariate Model 2 | ||||
|---|---|---|---|---|---|---|---|
| β [95% CI] | p | β [95% CI] | p | β [95% CI] | p | ||
| LAV | 0.22 | 0.76 [0.57, 0.95] | <0.001 | 0.18 [0.01, 0.36] | 0.04 | 0.7 [−0.67, 2.07] | 0.3 |
| LVM | 0.33 | 0.32 [0.25, 0.38] | <0.001 | 0.06 [−0.01, 0.14] | 0.08 | 0.11 [−0.32, 0.55] | 0.59 |
| LV e’ | −0.35 | −4.75 [−5.66, −3.83] | <0.001 | −1.33 [−2.36, −0.29] | 0.01 | −7.62 [−14.91, −0.32] | 0.04 |
| E/e’ | 0.19 | 2.23 [1.38, 3.07] | <0.001 | 0.71 [−0.07, 1.48] | 0.08 | 4.06 [0.17, 7.95] | 0.04 |
| LV GLS | −0.27 | −4.2 [−5.28, −3.12] | <0.001 | −1.14 [−2.15, −0.13] | 0.03 | 0.8 [−6.87, 8.48] | 0.83 |
| PALS | −0.34 | −1.26 [−1.52, −1.01] | <0.001 | −0.54 [−0.78, −0.3] | <0.001 | −2.48 [−4.41, −0.55] | 0.01 |
| ALSRsyst | −0.26 | −19.51 [−24.8, −14.22] | <0.001 | −8.57 [−13.31, −3.84] | <0.001 | −42.14 [−68, −16.28] | 0.002 |
| ALSRearly | −0.42 | −23.37 [−26.97, −19.78] | <0.001 | −8.05 [−12.38, −3.72] | <0.001 | −31.94 [−58.13, −5.75] | 0.02 |
| LAstiff | 0.33 | 102.47 [79.11, 125.83] | <0.001 | 41.51 [18.99, 64.04] | <0.001 | 41.14 [18.24, 64.05] | <0.001 |
| Pearson r | Univariate Model | Multivariate Model 1 | Multivariate Model 2 | ||||
|---|---|---|---|---|---|---|---|
| β [95% CI] | p | β [95% CI] | p | β [95% CI] | p | ||
| EFV | 0.31 | 0.012 [0.01, 0.014] | <0.001 | 0.01 [0.007, 0.011] | <0.001 | - | - |
| LAV | 0.22 | 0.02 [0.017, 0.025] | <0.001 | 0.013 [0.01, 0.017] | <0.001 | 0.002 [−0.005, 0.01] | 0.57 |
| LVM | 0.26 | 0.009 [0.007, 0.01] | <0.001 | 0.006 [0.004, 0.01] | <0.001 | 0.004 [0.001, 0.006] | 0.002 |
| LV e’ | −0.42 | −0.18 [−0.19, −0.16] | <0.001 | −0.14 [−0.15, −0.12] | <0.001 | −0.1 [−0.13, −0.06] | <0.001 |
| E/e’ | 0.24 | 0.11 [0.1, 0.13] | <0.001 | 0.08 [0.06, 0.1] | <0.001 | 0.06 [0.02, 0.09] | <0.001 |
| LV GLS | −0.14 | −0.08 [−0.1, −0.05] | <0.001 | −0.02 [−0.04, 0.003] | 0.095 | −0.01 [−0.05, 0.03] | 0.64 |
| PALS | −0.29 | −0.036 [−0.03, −0.04] | <0.001 | −0.025 [−0.03, −0.02] | <0.001 | −0.01 [−0.02, −0.001] | 0.02 |
| ALSRsyst | −0.25 | −0.65 [−0.76, −0.55] | <0.001 | −0.5 [−0.6, −0.4] | <0.001 | −0.26 [−0.44, −0.07] | 0.006 |
| ALSRearly | −0.44 | −0.79 [−0.86, −0.72] | <0.001 | −0.65 [−0.72, −0.55] | <0.001 | −0.4 [−0.55, −0.25] | <0.001 |
| LAstiff | 0.33 | 3.34 [2.92, 3.76] | <0.001 | 2.39 [1.97, 2.81] | <0.001 | 1.4 [0.63, 2.17] | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lai, Y.-H.; Su, C.-H.; Hung, T.-C.; Yun, C.-H.; Tsai, C.-T.; Yeh, H.-I.; Hung, C.-L. Association of Non-Alcoholic Fatty Liver Disease and Hepatic Fibrosis with Epicardial Adipose Tissue Volume and Atrial Deformation Mechanics in a Large Asian Population Free from Clinical Heart Failure. Diagnostics 2022, 12, 916. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12040916
Lai Y-H, Su C-H, Hung T-C, Yun C-H, Tsai C-T, Yeh H-I, Hung C-L. Association of Non-Alcoholic Fatty Liver Disease and Hepatic Fibrosis with Epicardial Adipose Tissue Volume and Atrial Deformation Mechanics in a Large Asian Population Free from Clinical Heart Failure. Diagnostics. 2022; 12(4):916. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12040916
Chicago/Turabian StyleLai, Yau-Huei, Cheng-Huang Su, Ta-Chuan Hung, Chun-Ho Yun, Cheng-Ting Tsai, Hung-I Yeh, and Chung-Lieh Hung. 2022. "Association of Non-Alcoholic Fatty Liver Disease and Hepatic Fibrosis with Epicardial Adipose Tissue Volume and Atrial Deformation Mechanics in a Large Asian Population Free from Clinical Heart Failure" Diagnostics 12, no. 4: 916. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12040916