
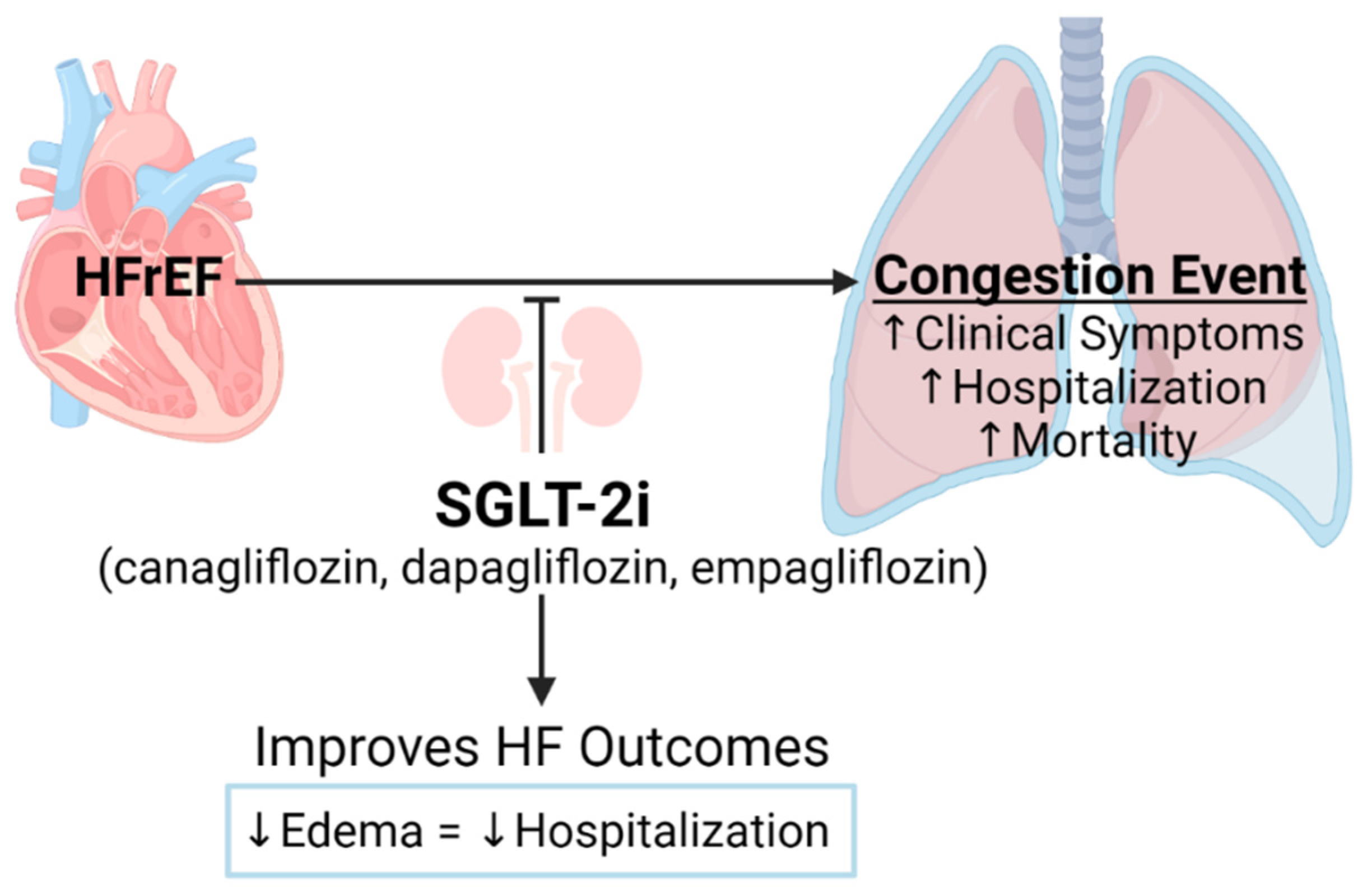
Sodium-Glucose Cotransporter-2 Inhibitors Improve Heart Failure with Reduced Ejection Fraction Outcomes by Reducing Edema and Congestion

 , ,
, ,
Abstract
:1. Introduction
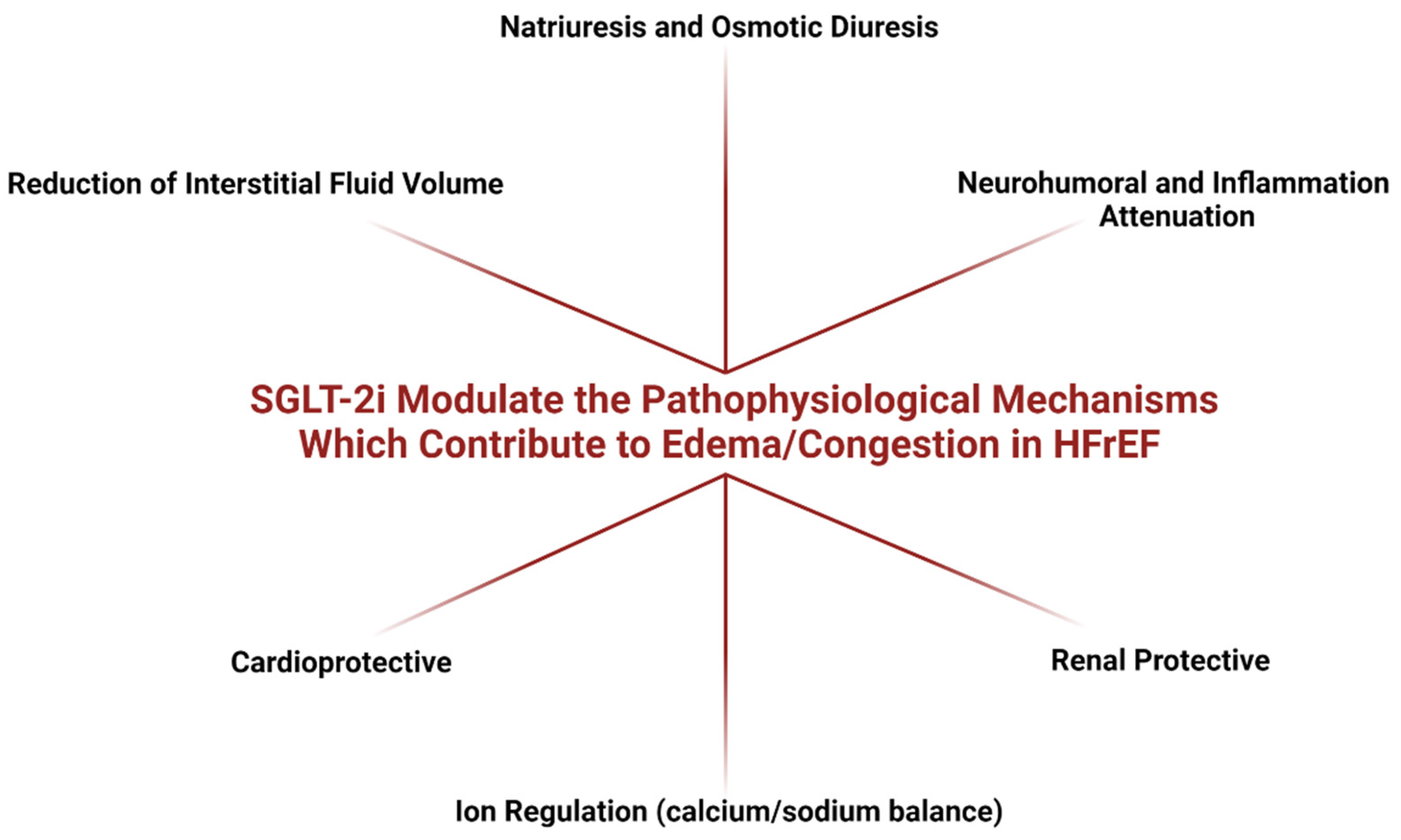
2. Impact of SGLT-2i on Diuretic, Natriuretic and Renal Hemodynamic Outcomes in HFrEF: Focus on Edema/Congestion
2.1. Impact of SGLT-2i on Natriuresis and Osmotic Diuresis
2.2. SGLT-2i Reduced Pathological HF-Related Intestinal Fluid Volume Rather Than Blood Plasma Volume
2.3. Impact of SGLT-2i on Renal Function
2.4. Effects of SGLT-2i on Neurohumoral Activation
3. Overview of SGLT-2i Treatment Outcomes Contributing to Edema/Congestion Modulation in HFrEF-Related Clinical Trials
3.1. Impact of SGLT-2i on Death and Hospitalization Rates
3.2. Impact of SGLT-2i on Cardiac Remodeling and Metabolism
3.3. Impact of SGLT-2i on Plasma Biomarkers
3.4. Impact of SGLT-2i on Renal Function
3.5. Impact of SGLT-2i on Functional Status and Quality of Life
3.6. Direct Impact of SGLT-2i on Fluid Retention
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| AF | Atrial Fibrillation |
| ANP/NT-proANP | Atrial natriuretic peptide/N-terminal-proANP |
| ASCVD | Atherosclerotic cardiovascular disease |
| BNP/NT-proBNP | Brain/B-type natriuretic peptide/N-terminal-proBNP |
| CKD | Chronic kidney disease |
| CSS | Clinical summary score |
| CV | Cardiovascular |
| EF | Ejection fraction |
| eGFR | Estimated glomerular filtration rate |
| ESRD | End-stage renal disease |
| HF | Heart failure |
| HFrEF | Heart failure with reduced ejection fraction |
| HFpEF | Heart failure with preserved ejection fraction |
| HHF | Hospitalization due to heart failure |
| HR | Hazard ratio |
| KCCQ | Kansas City Cardiomyopathy Questionnaire |
| LVEF | Left ventricular ejection fraction |
| MACE | Major adverse cardiac events |
| NO | Nitric oxide |
| NPs | Natriuretic peptides |
| NYHA | New York Heart Association |
| OMT | Optimal medical therapy |
| RAAS | Renin-angiotensin-aldosterone system |
| SGLT-2i | Sodium-glucose cotransporter-2 inhibitors |
| SNS | Sympathetic nervous system |
| T2DM/T1DM | Type 2/Type 1 diabetes mellitus |
References
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Bohm, M.; Burri, H.; Butler, J.; Celutkiene, J.; Chioncel, O.; et al. 2021 Esc Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Bozkurt, B.; Coats, A.J.; Tsutsui, H.; Abdelhamid, M.; Adamopoulos, S.; Albert, N.; Anker, S.D.; Atherton, J.; Bohm, M.; Butler, J.; et al. Universal Definition and Classification of Heart Failure: A Report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and Writing Committee of the Universal Definition of Heart Failure. J. Card. Fail. 2021, 27, 387–413. [Google Scholar] [CrossRef]
- Bozkurt, B.; Coats, A.J.S.; Tsutsui, H.; Abdelhamid, C.M.; Adamopoulos, S.; Albert, N.; Anker, S.D.; Atherton, J.; Bohm, M.; Butler, J.; et al. Universal Definition and Classification of Heart Failure: A Report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and Writing Committee of the Universal Definition of Heart Failure: Endorsed by the Canadian Heart Failure Society, Heart Failure Association of India, Cardiac Society of Australia and New Zealand, and Chinese Heart Failure Association. Eur. J. Heart Fail. 2021, 23, 352–380. [Google Scholar] [CrossRef]
- Weber, K.T. Aldosterone in Congestive Heart Failure. N. Engl. J. Med. 2001, 345, 1689–1697. [Google Scholar] [CrossRef] [PubMed]
- Ware, L.B.; Matthay, M.A. Clinical Practice. Acute Pulmonary Edema. N. Engl. J. Med. 2005, 353, 2788–2796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Writing Committee Members; Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Drazner, M.H.; Fonarow, G.C.; Geraci, S.A.; Horwich, T.; et al. 2013 Accf/Aha Guideline for the Management of Heart Failure: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation 2013, 128, e240–e327. [Google Scholar] [CrossRef]
- Clark, A.L.; Cleland, J.G. Causes and Treatment of Oedema in Patients with Heart Failure. Nat. Rev. Cardiol. 2013, 10, 156–170. [Google Scholar] [CrossRef]
- Parrinello, G.; Greene, S.J.; Torres, D.; Alderman, M.; Bonventre, J.V.; Di Pasquale, P.; Gargani, L.; Nohria, A.; Fonarow, G.C.; Vaduganathan, M.; et al. Water and Sodium in Heart Failure: A Spotlight on Congestion. Heart Fail. Rev. 2015, 20, 13–24. [Google Scholar] [CrossRef] [Green Version]
- Miller, W.L. Fluid Volume Overload and Congestion in Heart Failure: Time to Reconsider Pathophysiology and How Volume Is Assessed. Circ. Heart Fail. 2016, 9, e002922. [Google Scholar] [CrossRef] [Green Version]
- Lam, C.S.P.; Yancy, C. Universal Definition and Classification of Heart Failure: Is It Universal? Does It Define Heart Failure? J. Card. Fail. 2021, 27, 509–511. [Google Scholar] [CrossRef]
- Hunt, S.A.; Baker, D.W.; Chin, M.H.; Cinquegrani, M.P.; Feldman, A.M.; Francis, G.S.; Ganiats, T.G.; Goldstein, S.; Gregoratos, G.; Jessup, M.L.; et al. Guidelines for the Evaluation and Management of Chronic Heart Failure in the Adult: Executive Summary a Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Revise the 1995 Guidelines for the Evaluation and Management of Heart Failure): Developed in Collaboration with the International Society for Heart and Lung Transplantation; Endorsed by the Heart Failure Society of America. Circulation 2001, 104, 2996–3007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dzau, V.J.; Colucci, W.S.; Hollenberg, N.K.; Williams, G.H. Relation of the Renin-Angiotensin-Aldosterone System to Clinical State in Congestive Heart Failure. Circulation 1981, 63, 645–651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sullivan, R.D.; Mehta, R.M.; Tripathi, R.; Reed, G.L.; Gladysheva, I.P. Renin Activity in Heart Failure with Reduced Systolic Function-New Insights. Int. J. Mol. Sci. 2019, 20, 3182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lam, C.S.P.; Chandramouli, C.; Ahooja, V.; Verma, S. Sglt-2 Inhibitors in Heart Failure: Current Management, Unmet Needs, and Therapeutic Prospects. J. Am. Heart Assoc. 2019, 8, e013389. [Google Scholar] [CrossRef]
- Correale, M.; Petroni, R.; Coiro, S.; Antohi, E.L.; Monitillo, F.; Leone, M.; Triggiani, M.; Ishihara, S.; Dungen, H.D.; Sarwar, C.M.S.; et al. Paradigm Shift in Heart Failure Treatment: Are Cardiologists Ready to Use Gliflozins? Heart Fail. Rev. 2021, 1–17. [Google Scholar] [CrossRef]
- Lytvyn, Y.; Bjornstad, P.; Udell, J.A.; Lovshin, J.A.; Cherney, D.Z.I. Sodium Glucose Cotransporter-2 Inhibition in Heart Failure: Potential Mechanisms, Clinical Applications, and Summary of Clinical Trials. Circulation 2017, 136, 1643–1658. [Google Scholar] [CrossRef]
- Wojcik, C.; Warden, B.A. Mechanisms and Evidence for Heart Failure Benefits from Sglt2 Inhibitors. Curr. Cardiol. Rep. 2019, 21, 130. [Google Scholar] [CrossRef]
- Zinman, B.; Wanner, C.; Lachin, J.M.; Fitchett, D.; Bluhmki, E.; Hantel, S.; Mattheus, M.; Devins, T.; Johansen, O.E.; Woerle, H.J.; et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N. Engl. J. Med. 2015, 373, 2117–2128. [Google Scholar] [CrossRef] [Green Version]
- Neal, B.; Perkovic, V.; Matthews, D.R. Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes. N. Engl. J. Med. 2017, 377, 2099. [Google Scholar] [CrossRef]
- Perkovic, V.; Jardine, M.J.; Neal, B.; Bompoint, S.; Heerspink, H.J.L.; Charytan, D.M.; Edwards, R.; Agarwal, R.; Bakris, G.; Bull, S.; et al. Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy. N. Engl. J. Med. 2019, 380, 2295–2306. [Google Scholar] [CrossRef] [Green Version]
- Solomon, S.D.; McMurray, J.J.V.; Anand, I.S.; Ge, J.; Lam, C.S.P.; Maggioni, A.P.; Martinez, F.; Packer, M.; Pfeffer, M.A.; Pieske, B.; et al. Committees. Angiotensin-Neprilysin Inhibition in Heart Failure with Preserved Ejection Fraction. N. Engl. J. Med. 2019, 381, 1609–1620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMurray, J.J.V.; DeMets, D.L.; Inzucchi, S.E.; Kober, L.; Kosiborod, M.N.; Langkilde, A.M.; Martinez, F.A.; Bengtsson, O.; Ponikowski, P.; Sabatine, M.S.; et al. A Trial to Evaluate the Effect of the Sodium-Glucose Co-Transporter 2 Inhibitor Dapagliflozin on Morbidity and Mortality in Patients with Heart Failure and Reduced Left Ventricular Ejection Fraction (Dapa-Hf). Eur. J. Heart Fail. 2019, 21, 665–675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMurray, J.J.V.; DeMets, D.L.; Inzucchi, S.E.; Kober, L.; Kosiborod, M.N.; Langkilde, A.M.; Martinez, F.A.; Bengtsson, O.; Ponikowski, P.; Sabatine, M.S.; et al. The Dapagliflozin and Prevention of Adverse-Outcomes in Heart Failure (Dapa-Hf) Trial: Baseline Characteristics. Eur. J. Heart Fail. 2019, 21, 1402–1411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMurray, J.J.V.; Solomon, S.D.; Inzucchi, S.E.; Kober, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; Anand, I.S.; Belohlavek, J.; et al. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. N. Engl. J. Med. 2019, 381, 1995–2008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nassif, M.E.; Windsor, S.L.; Tang, F.; Khariton, Y.; Husain, M.; Inzucchi, S.E.; McGuire, D.K.; Pitt, B.; Scirica, B.M.; Austin, B.; et al. Dapagliflozin Effects on Biomarkers, Symptoms, and Functional Status in Patients with Heart Failure with Reduced Ejection Fraction: The Define-Hf Trial. Circulation 2019, 140, 1463–1476. [Google Scholar] [CrossRef] [PubMed]
- Jensen, J.; Omar, M.; Kistorp, C.; Poulsen, M.K.; Tuxen, C.; Gustafsson, I.; Kober, L.; Gustafsson, F.; Fosbol, E.; Bruun, N.E.; et al. Empagliflozin in Heart Failure Patients with Reduced Ejection Fraction: A Randomized Clinical Trial (Empire Hf). Trials 2019, 20, 374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Pocock, S.J.; Carson, P.; Januzzi, J.; Verma, S.; Tsutsui, H.; Brueckmann, M.; et al. Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure. N. Engl. J. Med. 2020, 383, 1413–1424. [Google Scholar] [CrossRef]
- Zannad, F.; Ferreira, J.P.; Pocock, S.J.; Anker, S.D.; Butler, J.; Filippatos, G.; Brueckmann, M.; Ofstad, A.P.; Pfarr, E.; Jamal, W.; et al. Sglt2 Inhibitors in Patients with Heart Failure with Reduced Ejection Fraction: A Meta-Analysis of the Emperor-Reduced and Dapa-Hf Trials. Lancet 2020, 396, 819–829. [Google Scholar] [CrossRef]
- Damman, K.; Beusekamp, J.C.; Boorsma, E.M.; Swart, H.P.; Smilde, T.D.J.; Elvan, A.; van Eck, J.W.M.; Heerspink, H.J.L.; Voors, A.A. Randomized, Double-Blind, Placebo-Controlled, Multicentre Pilot Study on the Effects of Empagliflozin on Clinical Outcomes in Patients with Acute Decompensated Heart Failure (Empa-Response-Ahf). Eur. J. Heart Fail. 2020, 22, 713–722. [Google Scholar] [CrossRef] [Green Version]
- Kosiborod, M.N.; Jhund, P.S.; Docherty, K.F.; Diez, M.; Petrie, M.C.; Verma, S.; Nicolau, J.C.; Merkely, B.; Kitakaze, M.; DeMets, D.L.; et al. Effects of Dapagliflozin on Symptoms, Function, and Quality of Life in Patients with Heart Failure and Reduced Ejection Fraction: Results from the Dapa-Hf Trial. Circulation 2020, 141, 90–99. [Google Scholar] [CrossRef]
- Solomon, S.D.; Jhund, P.S.; Claggett, B.L.; Dewan, P.; Kober, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; Inzucchi, S.E.; et al. Effect of Dapagliflozin in Patients with Hfref Treated with Sacubitril/Valsartan: The Dapa-Hf Trial. JACC Heart Fail. 2020, 8, 811–818. [Google Scholar] [CrossRef] [PubMed]
- Docherty, K.F.; Jhund, P.S.; Inzucchi, S.E.; Kober, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; DeMets, D.L.; Sabatine, M.S.; Bengtsson, O.; et al. Effects of Dapagliflozin in Dapa-Hf According to Background Heart Failure Therapy. Eur. Heart J. 2020, 41, 2379–2392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez, F.A.; Serenelli, M.; Nicolau, J.C.; Petrie, M.C.; Chiang, C.E.; Tereshchenko, S.; Solomon, S.D.; Inzucchi, S.E.; Kober, L.; Kosiborod, M.N.; et al. Efficacy and Safety of Dapagliflozin in Heart Failure with Reduced Ejection Fraction According to Age: Insights from Dapa-Hf. Circulation 2020, 141, 100–111. [Google Scholar] [CrossRef] [PubMed]
- Serenelli, M.; Bohm, M.; Inzucchi, S.E.; Kober, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; Solomon, S.D.; DeMets, D.L.; et al. Effect of Dapagliflozin According to Baseline Systolic Blood Pressure in the Dapagliflozin and Prevention of Adverse Outcomes in Heart Failure Trial (Dapa-Hf). Eur. Heart J. 2020, 41, 3402–3418. [Google Scholar] [CrossRef] [PubMed]
- Jackson, A.M.; Dewan, P.; Anand, I.S.; Belohlavek, J.; Bengtsson, O.; de Boer, R.A.; Bohm, M.; Boulton, D.W.; Chopra, V.K.; DeMets, D.L.; et al. Dapagliflozin and Diuretic Use in Patients with Heart Failure and Reduced Ejection Fraction in Dapa-Hf. Circulation 2020, 142, 1040–1054. [Google Scholar] [CrossRef]
- Packer, M. Are the Benefits of Sglt2 Inhibitors in Heart Failure and a Reduced Ejection Fraction Influenced by Background Therapy? Expectations and Realities of a New Standard of Care. Eur. Heart J. 2020, 41, 2393–2396. [Google Scholar] [CrossRef]
- McMurray, J. Empa-Reg—The "Diuretic Hypothesis. J. Diabetes Complicat. 2016, 30, 3–4. [Google Scholar] [CrossRef]
- Rahman, A.; Hitomi, H.; Nishiyama, A. Cardioprotective Effects of Sglt2 Inhibitors Are Possibly Associated with Normalization of the Circadian Rhythm of Blood Pressure. Hypertens Res. 2017, 40, 535–540. [Google Scholar] [CrossRef]
- Hallow, K.M.; Helmlinger, G.; Greasley, P.J.; McMurray, J.J.V.; Boulton, D.W. Why Do Sglt2 Inhibitors Reduce Heart Failure Hospitalization? A Differential Volume Regulation Hypothesis. Diabetes Obes. Metab. 2018, 20, 479–487. [Google Scholar] [CrossRef] [Green Version]
- Bertero, E.; Prates Roma, L.; Ameri, P.; Maack, C. Cardiac Effects of Sglt2 Inhibitors: The Sodium Hypothesis. Cardiovasc. Res. 2018, 114, 12–18. [Google Scholar] [CrossRef] [Green Version]
- Bell, R.M.; Yellon, D.M. Sglt2 Inhibitors: Hypotheses on the Mechanism of Cardiovascular Protection. Lancet Diabetes Endocrinol. 2018, 6, 435–437. [Google Scholar] [CrossRef]
- Verma, S.; Rawat, S.; Ho, K.L.; Wagg, C.S.; Zhang, L.; Teoh, H.; Dyck, J.E.; Uddin, G.M.; Oudit, G.Y.; Mayoux, E.; et al. Empagliflozin Increases Cardiac Energy Production in Diabetes: Novel Translational Insights into the Heart Failure Benefits of Sglt2 Inhibitors. JACC Basic Transl. Sci. 2018, 3, 575–587. [Google Scholar] [CrossRef] [PubMed]
- Yoshihara, F.; Imazu, M.; Hamasaki, T.; Anzai, T.; Yasuda, S.; Ito, S.; Yamamoto, H.; Hashimura, K.; Yasumura, Y.; Mori, K.; et al. An Exploratory Study of Dapagliflozin for the Attenuation of Albuminuria in Patients with Heart Failure and Type 2 Diabetes Mellitus (Dapper). Cardiovasc. Drugs Ther. 2018, 32, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Lopaschuk, G.D.; Verma, S. Mechanisms of Cardiovascular Benefits of Sodium Glucose Co-Transporter 2 (Sglt2) Inhibitors: A State-of-the-Art Review. JACC Basic Transl. Sci. 2020, 5, 632–644. [Google Scholar] [CrossRef] [PubMed]
- Nightingale, B. A Review of the Proposed Mechanistic Actions of Sodium Glucose Cotransporter-2 Inhibitors in the Treatment of Heart Failure. Cardiol. Res. 2021, 12, 60–66. [Google Scholar] [CrossRef]
- Packer, M. Differential Pathophysiological Mechanisms in Heart Failure with a Reduced or Preserved Ejection Fraction in Diabetes. JACC Heart Fail. 2021, 9, 535–549. [Google Scholar] [CrossRef]
- Gupta, M.; Rao, S.; Manek, G.; Fonarow, G.C.; Ghosh, R.K. The Role of Dapagliflozin in the Management of Heart Failure: An Update on the Emerging Evidence. Ther Clin. Risk Manag. 2021, 17, 823–830. [Google Scholar] [CrossRef]
- Fathi, A.; Vickneson, K.; Singh, J.S. Sglt2-Inhibitors; More Than Just Glycosuria and Diuresis. Heart Fail. Rev. 2021, 26, 623–642. [Google Scholar] [CrossRef]
- Metra, M.; O’Connor, C.M.; Davison, B.A.; Cleland, J.G.; Ponikowski, P.; Teerlink, J.R.; Voors, A.A.; Givertz, M.M.; Mansoor, G.A.; Bloomfield, D.M.; et al. Early Dyspnoea Relief in Acute Heart Failure: Prevalence, Association with Mortality, and Effect of Rolofylline in the Protect Study. Eur. Heart J. 2011, 32, 1519–1534. [Google Scholar] [CrossRef] [Green Version]
- Mentz, R.J.; Stevens, S.R.; DeVore, A.D.; Lala, A.; Vader, J.M.; AbouEzzeddine, O.F.; Khazanie, P.; Redfield, M.M.; Stevenson, L.W.; O’Connor, C.M.; et al. Decongestion Strategies and Renin-Angiotensin-Aldosterone System Activation in Acute Heart Failure. JACC Heart Fail. 2015, 3, 97–107. [Google Scholar] [CrossRef]
- Pellicori, P.; Kaur, K.; Clark, A.L. Fluid Management in Patients with Chronic Heart Failure. Card. Fail. Rev. 2015, 1, 90–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melenovsky, V.; Andersen, M.J.; Andress, K.; Reddy, Y.N.; Borlaug, B.A. Lung Congestion in Chronic Heart Failure: Haemodynamic, Clinical, and Prognostic Implications. Eur. J. Heart Fail. 2015, 17, 1161–1171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chioncel, O.; Mebazaa, A.; Harjola, V.P.; Coats, A.J.; Piepoli, M.F.; Crespo-Leiro, M.G.; Laroche, C.; Seferovic, P.M.; Anker, S.D.; Ferrari, R.; et al. Clinical Phenotypes and Outcome of Patients Hospitalized for Acute Heart Failure: The Esc Heart Failure Long-Term Registry. Eur. J. Heart Fail. 2017, 19, 1242–1254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aimo, A.; Vergaro, G.; Giannoni, A.; Emdin, M. Wet Is Bad: Residual Congestion Predicts Worse Prognosis in Acute Heart Failure. Int. J. Cardiol. 2018, 258, 201–202. [Google Scholar] [CrossRef]
- Selvaraj, S.; Claggett, B.; Pozzi, A.; McMurray, J.J.V.; Jhund, P.S.; Packer, M.; Desai, A.S.; Lewis, E.F.; Vaduganathan, M.; Lefkowitz, M.P.; et al. Prognostic Implications of Congestion on Physical Examination among Contemporary Patients with Heart Failure and Reduced Ejection Fraction: Paradigm-Hf. Circulation 2019, 140, 1369–1379. [Google Scholar] [CrossRef] [Green Version]
- Pellicori, P.; Khan, M.J.I.; Graham, F.J.; Cleland, J.G.F. New Perspectives and Future Directions in the Treatment of Heart Failure. Heart Fail. Rev. 2020, 25, 147–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palazzuoli, A.; Evangelista, I.; Nuti, R. Congestion Occurrence and Evaluation in Acute Heart Failure Scenario: Time to Reconsider Different Pathways of Volume Overload. Heart Fail. Rev. 2020, 25, 119–131. [Google Scholar] [CrossRef]
- DeFilippis, E.M.; Van Spall, H.G.C. Improving Health-Related Quality of Life for Women with Acute Heart Failure: Chronically Undertreated. JACC Heart Fail. 2021, 9, 346–348. [Google Scholar] [CrossRef]
- Lombardi, C.M.; Cimino, G.; Pellicori, P.; Bonelli, A.; Inciardi, R.M.; Pagnesi, M.; Tomasoni, D.; Ravera, A.; Adamo, M.; Carubelli, V.; et al. Congestion in Patients with Advanced Heart Failure: Assessment and Treatment. Heart Fail. Clin. 2021, 17, 575–586. [Google Scholar] [CrossRef]
- Gheorghiade, M.; Filippatos, G.; De Luca, L.; Burnett, J. Congestion in Acute Heart Failure Syndromes: An Essential Target of Evaluation and Treatment. Am. J. Med. 2006, 119, S3–S10. [Google Scholar] [CrossRef]
- Pang, P.S.; Cleland, J.G.; Teerlink, J.R.; Collins, S.P.; Lindsell, C.J.; Sopko, G.; Peacock, W.F.; Fonarow, G.C.; Aldeen, A.Z.; Kirk, J.D.; et al. A Proposal to Standardize Dyspnoea Measurement in Clinical Trials of Acute Heart Failure Syndromes: The Need for a Uniform Approach. Eur. Heart J. 2008, 29, 816–824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gheorghiade, M.; Follath, F.; Ponikowski, P.; Barsuk, J.H.; Blair, J.E.; Cleland, J.G.; Dickstein, K.; Drazner, M.H.; Fonarow, G.C.; Jaarsma, T.; et al. Assessing and Grading Congestion in Acute Heart Failure: A Scientific Statement from the Acute Heart Failure Committee of the Heart Failure Association of the European Society of Cardiology and Endorsed by the European Society of Intensive Care Medicine. Eur. J. Heart Fail. 2010, 12, 423–433. [Google Scholar] [CrossRef] [PubMed]
- Girerd, N.; Seronde, M.F.; Coiro, S.; Chouihed, T.; Bilbault, P.; Braun, F.; Kenizou, D.; Maillier, B.; Nazeyrollas, P.; Roul, G.; et al. Integrative Assessment of Congestion in Heart Failure Throughout the Patient Journey. JACC Heart Fail. 2018, 6, 273–285. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, R.D.; Mehta, R.M.; Tripathi, R.; Gladysheva, I.P.; Reed, G.L. Normalizing Plasma Renin Activity in Experimental Dilated Cardiomyopathy: Effects on Edema, Cachexia, and Survival. Int. J. Mol. Sci. 2019, 20, 3886. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tripathi, R.; Sullivan, R.D.; Fan, T.M.; Mehta, R.M.; Gladysheva, I.P.; Reed, G.L. A Low-Sodium Diet Boosts Ang (1-7) Production and No-Cgmp Bioavailability to Reduce Edema and Enhance Survival in Experimental Heart Failure. Int. J. Mol. Sci. 2021, 22, 4035. [Google Scholar] [CrossRef]
- Pirrotta, F.; Mazza, B.; Gennari, L.; Palazzuoli, A. Pulmonary Congestion Assessment in Heart Failure: Traditional and New Tools. Diagnostics 2021, 11, 1306. [Google Scholar] [CrossRef]
- Reed, G.L.; Gladysheva, I.P.; Sullivan, R.D.; Mehta, R.M. Method of Personalized Treatment for Cardiomyopathy and Heart Failure and Associated Diseases by Measuring Edema and Cachexia/Sarcopenia. U.S. Patent 17/313,904, 6 May 2021. Available online: https://www.freepatentsonline.com/y2021/0263120.html (accessed on 26 February 2022).
- Takeuchi, T.; Dohi, K.; Omori, T.; Moriwaki, K.; Sato, Y.; Nakamori, S.; Fujimoto, N.; Fujii, E.; Yamada, N.; Ito, M. Diuretic Effects of Sodium-Glucose Cotransporter 2 Inhibitor in Patients with Type 2 Diabetes Mellitus and Heart Failure. Int. J. Cardiol. 2015, 201, 1–3. [Google Scholar] [CrossRef]
- Lee, H.C.; Shiou, Y.L.; Jhuo, S.J.; Chang, C.Y.; Liu, P.L.; Jhuang, W.J.; Dai, Z.K.; Chen, W.Y.; Chen, Y.F.; Lee, A.S. The Sodium-Glucose Co-Transporter 2 Inhibitor Empagliflozin Attenuates Cardiac Fibrosis and Improves Ventricular Hemodynamics in Hypertensive Heart Failure Rats. Cardiovasc. Diabetol. 2019, 18, 45. [Google Scholar] [CrossRef]
- Packer, M. Activation and Inhibition of Sodium-Hydrogen Exchanger Is a Mechanism That Links the Pathophysiology and Treatment of Diabetes Mellitus with That of Heart Failure. Circulation 2017, 136, 1548–1559. [Google Scholar] [CrossRef]
- Lambers Heerspink, H.J.; de Zeeuw, D.; Wie, L.; Leslie, B.; List, J. Dapagliflozin a Glucose-Regulating Drug with Diuretic Properties in Subjects with Type 2 Diabetes. Diabetes Obes. Metab. 2013, 15, 853–862. [Google Scholar] [CrossRef] [Green Version]
- Eickhoff, M.K.; Dekkers, C.C.J.; Kramers, B.J.; Laverman, G.D.; Frimodt-Moller, M.; Jorgensen, N.R.; Faber, J.; Danser, A.H.J.; Gansevoort, R.T.; Rossing, P.; et al. Effects of Dapagliflozin on Volume Status When Added to Renin-Angiotensin System Inhibitors. J. Clin. Med. 2019, 8, 779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masuda, T.; Muto, S.; Fukuda, K.; Watanabe, M.; Ohara, K.; Koepsell, H.; Vallon, V.; Nagata, D. Osmotic Diuresis by Sglt2 Inhibition Stimulates Vasopressin-Induced Water Reabsorption to Maintain Body Fluid Volume. Physiol. Rep. 2020, 8, e14360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marx, N.; McGuire, D.K. Sodium-Glucose Cotransporter-2 Inhibition for the Reduction of Cardiovascular Events in High-Risk Patients with Diabetes Mellitus. Eur. Heart J. 2016, 37, 3192–3200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rossignol, P.; Hernandez, A.F.; Solomon, S.D.; Zannad, F. Heart Failure Drug Treatment. Lancet 2019, 393, 1034–1044. [Google Scholar] [CrossRef]
- Yu, H.; Basu, S.; Hallow, K.M. Cardiac and Renal Function Interactions in Heart Failure with Reduced Ejection Fraction: A Mathematical Modeling Analysis. PLoS Comput. Biol. 2020, 16, e1008074. [Google Scholar] [CrossRef] [PubMed]
- Rangaswami, J.; Bhalla, V.; Blair, J.E.A.; Chang, T.I.; Costa, S.; Lentine, K.L.; Lerma, E.V.; Mezue, K.; Molitch, M.; Mullens, W.; et al. Cardiorenal Syndrome: Classification, Pathophysiology, Diagnosis, and Treatment Strategies: A Scientific Statement from the American Heart Association. Circulation 2019, 139, e840–e878. [Google Scholar] [CrossRef] [PubMed]
- Merrill, A.J. Edema and Decreased Renal Blood Flow in Patients with Chronic Congestive Heart Failure: Evidence of “Forward Failure” as the Primary Cause of Edema. J. Clin. Invest. 1946, 25, 389–400. [Google Scholar] [CrossRef] [Green Version]
- Kilcoyne, M.M.; Schmidt, D.H.; Cannon, P.J. Intrarenal Blood Flow in Congestive Heart Failure. Circulation 1973, 47, 786–797. [Google Scholar] [CrossRef] [Green Version]
- Verbrugge, F.H.; Guazzi, M.; Testani, J.M.; Borlaug, B.A. Altered Hemodynamics and End-Organ Damage in Heart Failure: Impact on the Lung and Kidney. Circulation 2020, 142, 998–1012. [Google Scholar] [CrossRef]
- Nespoux, J.; Vallon, V. Renal Effects of Sglt2 Inhibitors: An Update. Curr. Opin. Nephrol. Hypertens. 2020, 29, 190–198. [Google Scholar] [CrossRef]
- Kuriyama, S. A Potential Mechanism of Cardio-Renal Protection with Sodium-Glucose Cotransporter 2 Inhibitors: Amelioration of Renal Congestion. Kidney Blood Press. Res. 2019, 44, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Cotton, J.M.; Kearney, M.T.; Shah, A.M. Nitric Oxide and Myocardial Function in Heart Failure: Friend or Foe? Heart 2002, 88, 564–566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ibebuogu, U.N.; Gladysheva, I.P.; Houng, A.K.; Reed, G.L. Decompensated Heart Failure Is Associated with Reduced Corin Levels and Decreased Cleavage of Pro-Atrial Natriuretic Peptide. Circ. Heart Fail. 2011, 4, 114–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dries, D.L. Process Matters: Emerging Concepts Underlying Impaired Natriuretic Peptide System Function in Heart Failure. Circ. Heart Fail. 2011, 4, 107–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sayer, G.; Bhat, G. The Renin-Angiotensin-Aldosterone System and Heart Failure. Cardiol. Clin. 2014, 32, 21–32. [Google Scholar] [CrossRef]
- Volpe, M.; Carnovali, M.; Mastromarino, V. The Natriuretic Peptides System in the Pathophysiology of Heart Failure: From Molecular Basis to Treatment. Clin. Sci. 2016, 130, 57–77. [Google Scholar] [CrossRef] [Green Version]
- Zaidi, S.S.; Ward, R.D.; Ramanathan, K.; Yu, X.; Gladysheva, I.P.; Reed, G.L. Possible Enzymatic Downregulation of the Natriuretic Peptide System in Patients with Reduced Systolic Function and Heart Failure: A Pilot Study. BioMed Res. Int. 2018, 2018, 7279036. [Google Scholar] [CrossRef] [Green Version]
- Tripathi, R.; Wang, D.; Sullivan, R.; Fan, T.H.; Gladysheva, I.P.; Reed, G.L. Depressed Corin Levels Indicate Early Systolic Dysfunction before Increases of Atrial Natriuretic Peptide/B-Type Natriuretic Peptide and Heart Failure Development. Hypertension 2016, 67, 362–367. [Google Scholar] [CrossRef] [Green Version]
- Tripathi, R.; Sullivan, R.; Fan, T.M.; Wang, D.; Sun, Y.; Reed, G.L.; Gladysheva, I.P. Enhanced Heart Failure, Mortality and Renin Activation in Female Mice with Experimental Dilated Cardiomyopathy. PLoS ONE 2017, 12, e0189315. [Google Scholar] [CrossRef] [Green Version]
- Santos-Gallego, C.G.; Requena-Ibanez, J.A.; San Antonio, R.; Ishikawa, K.; Watanabe, S.; Picatoste, B.; Flores, E.; Garcia-Ropero, A.; Sanz, J.; Hajjar, R.J.; et al. Empagliflozin Ameliorates Adverse Left Ventricular Remodeling in Nondiabetic Heart Failure by Enhancing Myocardial Energetics. J. Am. Coll. Cardiol. 2019, 73, 1931–1944. [Google Scholar] [CrossRef]
- Ansary, T.M.; Nakano, D.; Nishiyama, A. Diuretic Effects of Sodium Glucose Cotransporter 2 Inhibitors and Their Influence on the Renin-Angiotensin System. Int. J. Mol. Sci. 2019, 20, 629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maggioni, A.P.; Dahlstrom, U.; Filippatos, G.; Chioncel, O.; Leiro, M.C.; Drozdz, J.; Fruhwald, F.; Gullestad, L.; Logeart, D.; Metra, M.; et al. Eurobservational Research Programme: The Heart Failure Pilot Survey (Esc-Hf Pilot). Eur. J. Heart Fail. 2010, 12, 1076–1084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubio-Gracia, J.; Demissei, B.G.; Ter Maaten, J.M.; Cleland, J.G.; O’Connor, C.M.; Metra, M.; Ponikowski, P.; Teerlink, J.R.; Cotter, G.; Davison, B.A.; et al. Prevalence, Predictors and Clinical Outcome of Residual Congestion in Acute Decompensated Heart Failure. Int. J. Cardiol. 2018, 258, 185–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Drazner, M.H.; Fonarow, G.C.; Geraci, S.A.; Horwich, T.; Januzzi, J.L.; et al. 2013 Accf/Aha Guideline for the Management of Heart Failure: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2013, 62, e147–e239. [Google Scholar] [CrossRef] [Green Version]
- Santos-Gallego, C.G.; Vargas-Delgado, A.P.; Requena-Ibanez, J.A.; Garcia-Ropero, A.; Mancini, D.; Pinney, S.; Macaluso, F.; Sartori, S.; Roque, M.; Sabatel-Perez, F.; et al. Randomized Trial of Empagliflozin in Nondiabetic Patients with Heart Failure and Reduced Ejection Fraction. J. Am. Coll. Cardiol. 2021, 77, 243–255. [Google Scholar] [CrossRef]
- Wiviott, S.D.; Raz, I.; Sabatine, M.S. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes. Reply. N. Engl. J. Med. 2019, 380, 1881–1882. [Google Scholar] [CrossRef]
- Jhund, P.S.; Ponikowski, P.; Docherty, K.F.; Gasparyan, S.B.; Bohm, M.; Chiang, C.E.; Desai, A.S.; Howlett, J.; Kitakaze, M.; Petrie, M.C.; et al. Dapagliflozin and Recurrent Heart Failure Hospitalizations in Heart Failure with Reduced Ejection Fraction: An Analysis of Dapa-Hf. Circulation 2021, 143, 1962–1972. [Google Scholar] [CrossRef]
- Curtain, J.P.; Docherty, K.F.; Jhund, P.S.; Petrie, M.C.; Inzucchi, S.E.; Kober, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; et al. Effect of Dapagliflozin on Ventricular Arrhythmias, Resuscitated Cardiac Arrest, or Sudden Death in Dapa-Hf. Eur. Heart J. 2021, 42, 3727–3738. [Google Scholar] [CrossRef]
- Butt, J.H.; Docherty, K.F.; Petrie, M.C.; Schou, M.; Kosiborod, M.N.; O’Meara, E.; Katova, T.; Ljungman, C.E.A.; Diez, M.; Ogunniyi, M.O.; et al. Efficacy and Safety of Dapagliflozin in Men and Women with Heart Failure with Reduced Ejection Fraction: A Prespecified Analysis of the Dapagliflozin and Prevention of Adverse Outcomes in Heart Failure Trial. JAMA Cardiol. 2021, 6, 678–689. [Google Scholar] [CrossRef]
- Lu, Y.; Li, F.; Fan, Y.; Yang, Y.; Chen, M.; Xi, J. Effect of Sglt-2 Inhibitors on Cardiovascular Outcomes in Heart Failure Patients: A Meta-Analysis of Randomized Controlled Trials. Eur. J. Intern. Med. 2021, 87, 20–28. [Google Scholar] [CrossRef]
- Requena-Ibanez, J.A.; Santos-Gallego, C.G.; Rodriguez-Cordero, A.; Vargas-Delgado, A.P.; Mancini, D.; Sartori, S.; Atallah-Lajam, F.; Giannarelli, C.; Macaluso, F.; Lala, A.; et al. Mechanistic Insights of Empagliflozin in Nondiabetic Patients with Hfref: From the Empa-Tropism Study. JACC Heart Fail. 2021, 9, 578–589. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.M.Y.; Brooksbank, K.J.M.; Wetherall, K.; Mangion, K.; Roditi, G.; Campbell, R.T.; Berry, C.; Chong, V.; Coyle, L.; Docherty, K.F.; et al. Effect of Empagliflozin on Left Ventricular Volumes in Patients with Type 2 Diabetes, or Prediabetes, and Heart Failure with Reduced Ejection Fraction (Sugar-Dm-Hf). Circulation 2021, 143, 516–525. [Google Scholar] [CrossRef] [PubMed]
- Hundertmark, M.J.; Agbaje, O.F.; Coleman, R.; George, J.T.; Grempler, R.; Holman, R.R.; Lamlum, H.; Lee, J.; Milton, J.E.; Niessen, H.G.; et al. Design and Rationale of the Empa-Vision Trial: Investigating the Metabolic Effects of Empagliflozin in Patients with Heart Failure. ESC Heart Fail. 2021, 8, 2580–2590. [Google Scholar] [CrossRef] [PubMed]
- Tanajak, P.; Sa-Nguanmoo, P.; Sivasinprasasn, S.; Thummasorn, S.; Siri-Angkul, N.; Chattipakorn, S.C.; Chattipakorn, N. Cardioprotection of Dapagliflozin and Vildagliptin in Rats with Cardiac Ischemia-Reperfusion Injury. J. Endocrinol. 2018, 236, 69–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, P.C.; Ganguly, S.; Goh, S.Y. Weight Loss Associated with Sodium-Glucose Cotransporter-2 Inhibition: A Review of Evidence and Underlying Mechanisms. Obes. Rev. 2018, 19, 1630–1641. [Google Scholar] [CrossRef]
- Tromp, J.; Ponikowski, P.; Salsali, A.; Angermann, C.E.; Biegus, J.; Blatchford, J.; Collins, S.P.; Ferreira, J.P.; Grauer, C.; Kosiborod, M.; et al. Sodium-Glucose Co-Transporter 2 Inhibition in Patients Hospitalized for Acute Decompensated Heart Failure: Rationale for and Design of the Empulse Trial. Eur. J. Heart Fail. 2021, 23, 826–834. [Google Scholar] [CrossRef]
- Ibrahim, N.E.; Januzzi, J.L. Sodium-Glucose Co-Transporter 2 Inhibitors and Insights from Biomarker Measurement in Heart Failure Patients. Clin. Chem. 2021, 67, 79–86. [Google Scholar] [CrossRef]
- Butt, J.H.; Adamson, C.; Docherty, K.F.; de Boer, R.A.; Petrie, M.C.; Inzucchi, S.E.; Kosiborod, M.N.; Maria Langkilde, A.; Lindholm, D.; Martinez, F.A.; et al. Efficacy and Safety of Dapagliflozin in Heart Failure with Reduced Ejection Fraction According to N-Terminal Pro-B-Type Natriuretic Peptide: Insights from the Dapa-Hf Trial. Circ. Heart Fail. 2021, 14, 1305–1318. [Google Scholar] [CrossRef]
- Sezai, A.; Sekino, H.; Unosawa, S.; Taoka, M.; Osaka, S.; Tanaka, M. Canagliflozin for Japanese Patients with Chronic Heart Failure and Type Ii Diabetes. Cardiovasc. Diabetol. 2019, 18, 76. [Google Scholar] [CrossRef] [Green Version]
- Takase, H.; Dohi, Y. Kidney Function Crucially Affects B-Type Natriuretic Peptide (Bnp), N-Terminal Probnp and Their Relationship. Eur. J. Clin. Investig. 2014, 44, 303–308. [Google Scholar] [CrossRef]
- Bhatt, A.S.; Cooper, L.B.; Ambrosy, A.P.; Clare, R.M.; Coles, A.; Joyce, E.; Krishnamoorthy, A.; Butler, J.; Felker, G.M.; Ezekowitz, J.A.; et al. Interaction of Body Mass Index on the Association between N-Terminal-Pro-B-Type Natriuretic Peptide and Morbidity and Mortality in Patients with Acute Heart Failure: Findings from Ascend-Hf (Acute Study of Clinical Effectiveness of Nesiritide in Decompensated Heart Failure). J. Am. Heart Assoc. 2018, 7, e006740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiig, H. Pathophysiology of Tissue Fluid Accumulation in Inflammation. J. Physiol. 2011, 589, 2945–2953. [Google Scholar] [CrossRef] [PubMed]
- Van Linthout, S.; Tschope, C. Inflammation - Cause or Consequence of Heart Failure or Both? Curr. Heart Fail. Rep. 2017, 14, 251–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, S.P.; Kakkar, R.; McCarthy, C.P.; Januzzi, J.L., Jr. Inflammation in Heart Failure: Jacc State-of-the-Art Review. J. Am. Coll. Cardiol. 2020, 75, 1324–1340. [Google Scholar] [CrossRef] [PubMed]
- Heerspink, H.J.L.; Perco, P.; Mulder, S.; Leierer, J.; Hansen, M.K.; Heinzel, A.; Mayer, G. Canagliflozin Reduces Inflammation and Fibrosis Biomarkers: A Potential Mechanism of Action for Beneficial Effects of Sglt2 Inhibitors in Diabetic Kidney Disease. Diabetologia 2019, 62, 1154–1166. [Google Scholar] [CrossRef] [Green Version]
- Alshnbari, A.S.; Millar, S.A.; O’Sullivan, S.E.; Idris, I. Effect of Sodium-Glucose Cotransporter-2 Inhibitors on Endothelial Function: A Systematic Review of Preclinical Studies. Diabetes Ther. 2020, 11, 1947–1963. [Google Scholar] [CrossRef]
- Ugusman, A.; Kumar, J.; Aminuddin, A. Endothelial Function and Dysfunction: Impact of Sodium-Glucose Cotransporter 2 Inhibitors. Pharmacol. Ther. 2021, 224, 107832. [Google Scholar] [CrossRef]
- Dyck, J.R.B.; Sossalla, S.; Hamdani, N.; Coronel, R.; Weber, N.C.; Light, P.E.; Zuurbier, C.J. Cardiac Mechanisms of the Beneficial Effects of Sglt2 Inhibitors in Heart Failure: Evidence for Potential Off-Target Effects. J. Mol. Cell. Cardiol. 2022, 167, 17–31. [Google Scholar] [CrossRef]
- Schefold, J.C.; Filippatos, G.; Hasenfuss, G.; Anker, S.D.; von Haehling, S. Heart Failure and Kidney Dysfunction: Epidemiology, Mechanisms and Management. Nat. Rev. Nephrol. 2016, 12, 610–623. [Google Scholar] [CrossRef]
- Damman, K.; Masson, S.; Lucci, D.; Gorini, M.; Urso, R.; Maggioni, A.P.; Tavazzi, L.; Tarantini, L.; Tognoni, G.; Voors, A.; et al. Progression of Renal Impairment and Chronic Kidney Disease in Chronic Heart Failure: An Analysis from Gissi-Hf. J. Card Fail. 2017, 23, 2–9. [Google Scholar] [CrossRef] [Green Version]
- Adamska-Welnicka, A.; Welnicki, M.; Mamcarz, A.; Gellert, R. Chronic Kidney Disease and Heart Failure-Everyday Diagnostic Challenges. Diagnostics 2021, 11, 2164. [Google Scholar] [CrossRef] [PubMed]
- Jhund, P.S.; Solomon, S.D.; Docherty, K.F.; Heerspink, H.J.L.; Anand, I.S.; Bohm, M.; Chopra, V.; de Boer, R.A.; Desai, A.S.; Ge, J.; et al. Efficacy of Dapagliflozin on Renal Function and Outcomes in Patients with Heart Failure with Reduced Ejection Fraction: Results of Dapa-Hf. Circulation 2021, 143, 298–309. [Google Scholar] [CrossRef] [PubMed]
- Green, C.P.; Porter, C.B.; Bresnahan, D.R.; Spertus, J.A. Development and Evaluation of the Kansas City Cardiomyopathy Questionnaire: A New Health Status Measure for Heart Failure. J. Am. Coll. Cardiol. 2000, 35, 1245–1255. [Google Scholar] [CrossRef] [Green Version]
- Butler, J.; Anker, S.D.; Filippatos, G.; Khan, M.S.; Ferreira, J.P.; Pocock, S.J.; Giannetti, N.; Januzzi, J.L.; Pina, I.L.; Lam, C.S.P.; et al. Empagliflozin and Health-Related Quality of Life Outcomes in Patients with Heart Failure with Reduced Ejection Fraction: The Emperor-Reduced Trial. Eur. Heart J. 2021, 42, 1203–1212. [Google Scholar] [CrossRef]
- Spertus, J.A.; Birmingham, M.C.; Nassif, M.; Damaraju, C.V.; Abbate, A.; Butler, J.; Lanfear, D.E.; Lingvay, I.; Kosiborod, M.N.; Januzzi, J.L. The Sglt2 Inhibitor Canagliflozin in Heart Failure: The Chief-Hf Remote, Patient-Centered Randomized Trial. Nat. Med. 2022, 1–5. [Google Scholar] [CrossRef]
- Teo, Y.H.; Teo, Y.N.; Syn, N.L.; Kow, C.S.; Yoong, C.S.Y.; Tan, B.Y.Q.; Yeo, T.C.; Lee, C.H.; Lin, W.; Sia, C.H. Effects of Sodium/Glucose Cotransporter 2 (Sglt2) Inhibitors on Cardiovascular and Metabolic Outcomes in Patients without Diabetes Mellitus: A Systematic Review and Meta-Analysis of Randomized-Controlled Trials. J. Am. Heart Assoc. 2021, 10, e019463. [Google Scholar] [CrossRef]
- Heerspink, H.J.L.; Kohan, D.E.; de Zeeuw, D. New Insights from Sonar Indicate Adding Sodium Glucose Co-Transporter 2 Inhibitors to an Endothelin Receptor Antagonist Mitigates Fluid Retention and Enhances Albuminuria Reduction. Kidney Int. 2021, 99, 346–349. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| HF Clinical Trial | Study Population Inclusion Criteria | Major Outcome Measures | Summary |
|---|---|---|---|
| DAPA-HF Dapagliflozin: 10 mg or 5 mg tablets given once daily/up to 27.8 months. McMurray et al., 2019 [24] |
| Dapagliflozin vs. pacebo groups:
| Dapagliflozin reduced HHF and CV death |
| EMPEROR-REDUCED Empagliflozin: 10 mg/once daily/up to 1040 days Packer et al., 2020 [27] |
| Empagliflozin vs. placebo group:
| Empagliflozin reduced HHF and CV death; preserved renal function |
| EMPA-TROPISM Empagliflozin: 10mg/once daily/6 months Santos-Gallegos et al., 2021 [96] |
| Empagliflozin vs. placebo group from baseline to 6 months:
| Empagliflozin improved cardiac function (suggesting cardiac pressure overload improvement) and patient exercise capacity |
| EMPA-RESPONSE-AHF Empagliflozin: 10 mg/daily/30 days Damman et al., 2020 [29] |
| Empagliflozin vs. placebo group:
| Empagliflozin reduced HHF; acute setting and small sample size limited results |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernandez, M.; Sullivan, R.D.; McCune, M.E.; Reed, G.L.; Gladysheva, I.P. Sodium-Glucose Cotransporter-2 Inhibitors Improve Heart Failure with Reduced Ejection Fraction Outcomes by Reducing Edema and Congestion. Diagnostics 2022, 12, 989. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12040989
Hernandez M, Sullivan RD, McCune ME, Reed GL, Gladysheva IP. Sodium-Glucose Cotransporter-2 Inhibitors Improve Heart Failure with Reduced Ejection Fraction Outcomes by Reducing Edema and Congestion. Diagnostics. 2022; 12(4):989. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12040989
Chicago/Turabian StyleHernandez, Michelle, Ryan D. Sullivan, Mariana E. McCune, Guy L. Reed, and Inna P. Gladysheva. 2022. "Sodium-Glucose Cotransporter-2 Inhibitors Improve Heart Failure with Reduced Ejection Fraction Outcomes by Reducing Edema and Congestion" Diagnostics 12, no. 4: 989. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12040989