
Association of Prognostic Nutritional Index with Severity and Mortality of Hospitalized Patients with COVID-19: A Systematic Review and Meta-Analysis

 , ,
, ,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Searches
2.2. Study Selection and Data Extraction
2.3. Data Extraction
2.4. Outcomes and Definitions
2.5. Assessment of Risks of Bias for the Included Studies
2.6. Data Synthesis and Analysis
3. Results
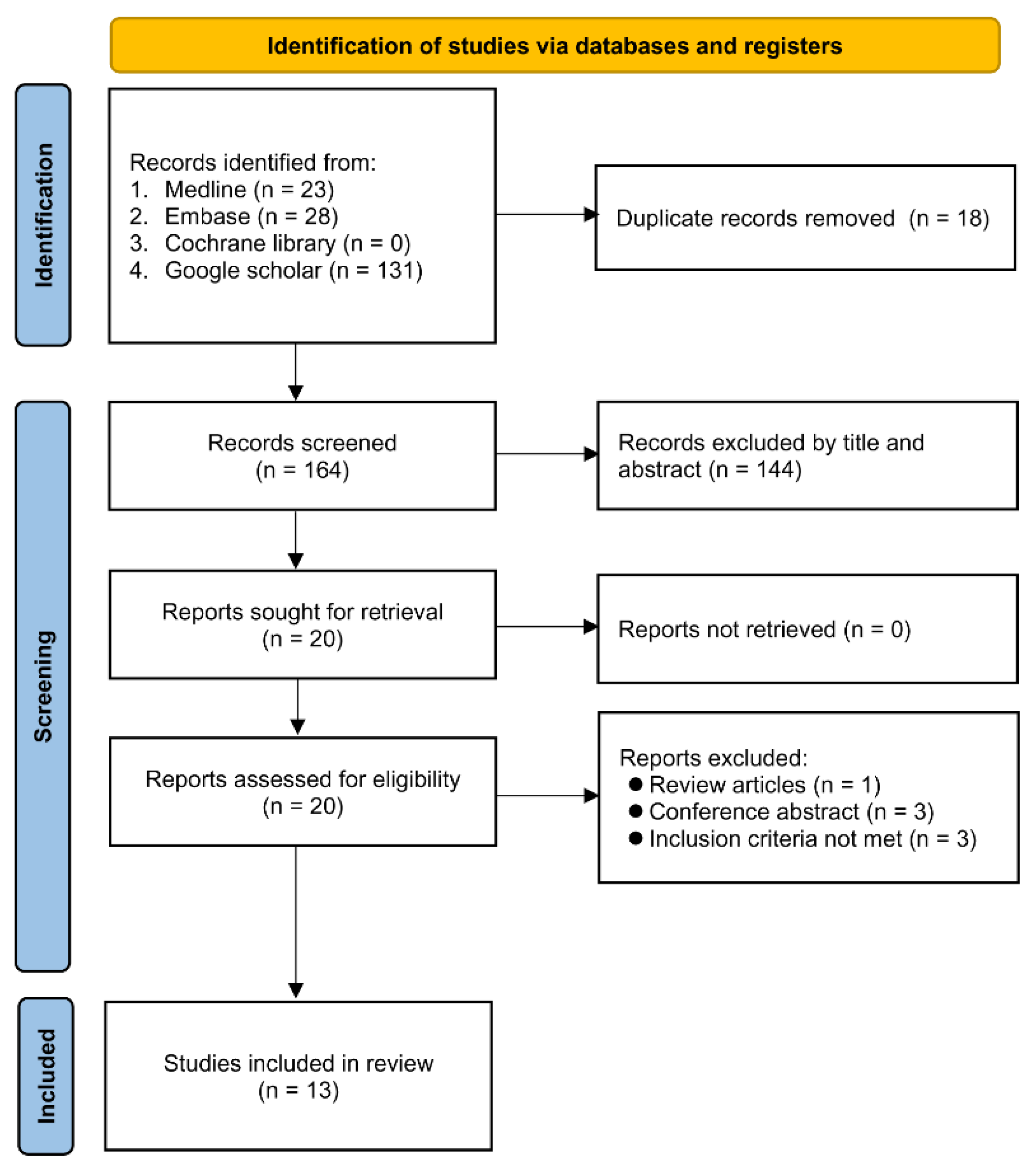
3.1. Study Selection
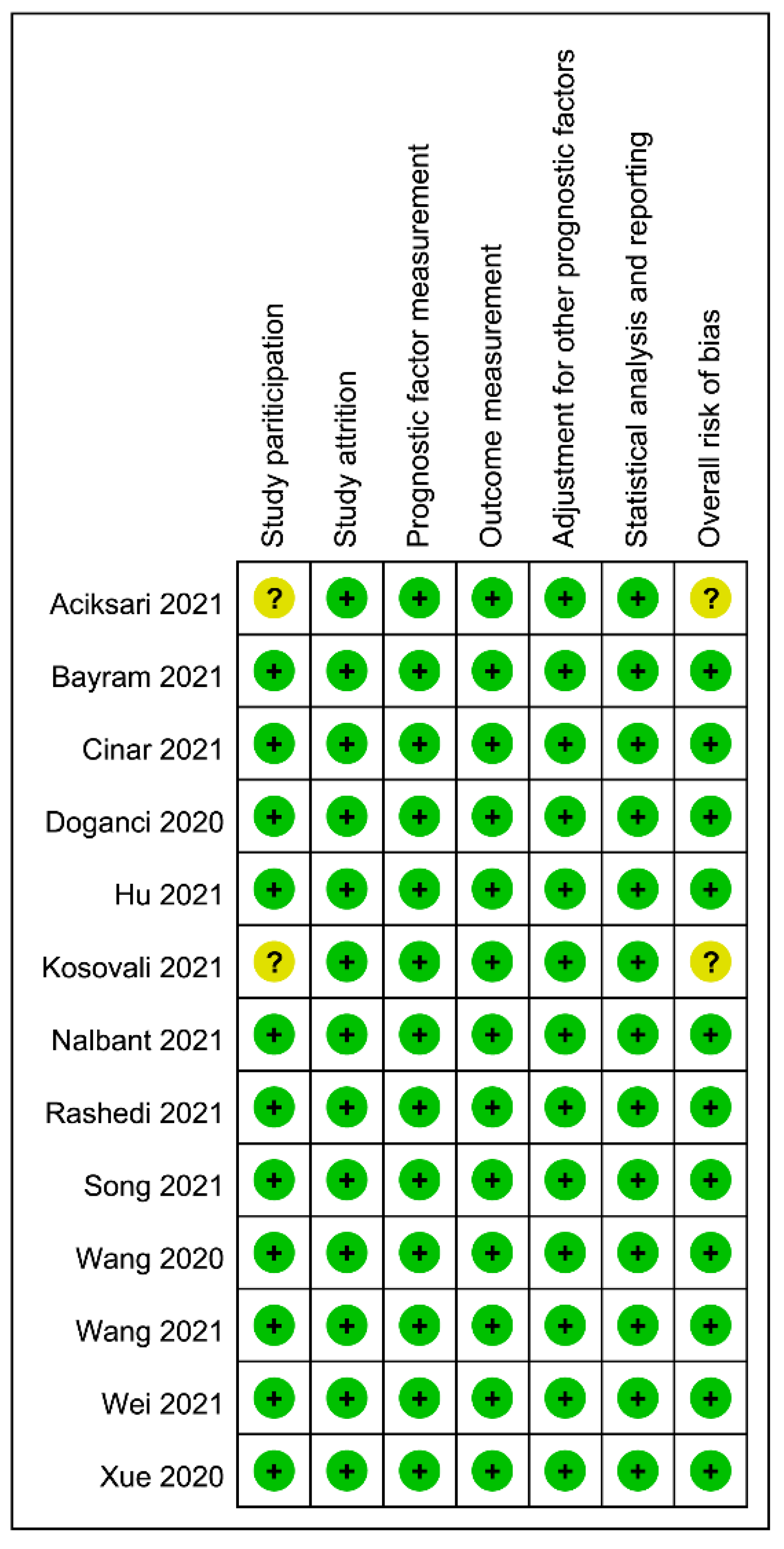
3.2. Study Characteristics and Risk of Bias
3.3. Data Analysis
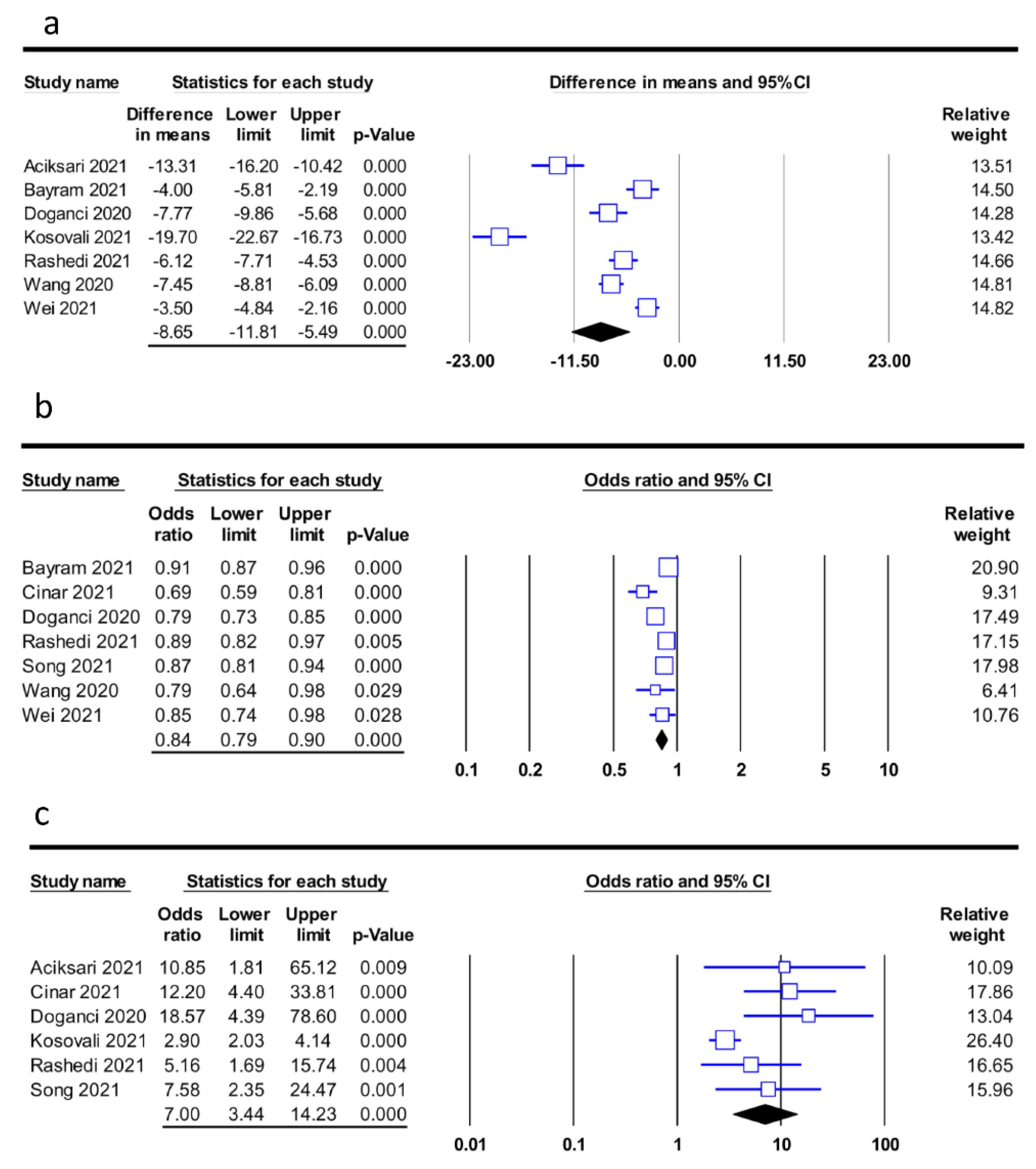
3.3.1. Primary Outcome—Association of PNI with Mortality
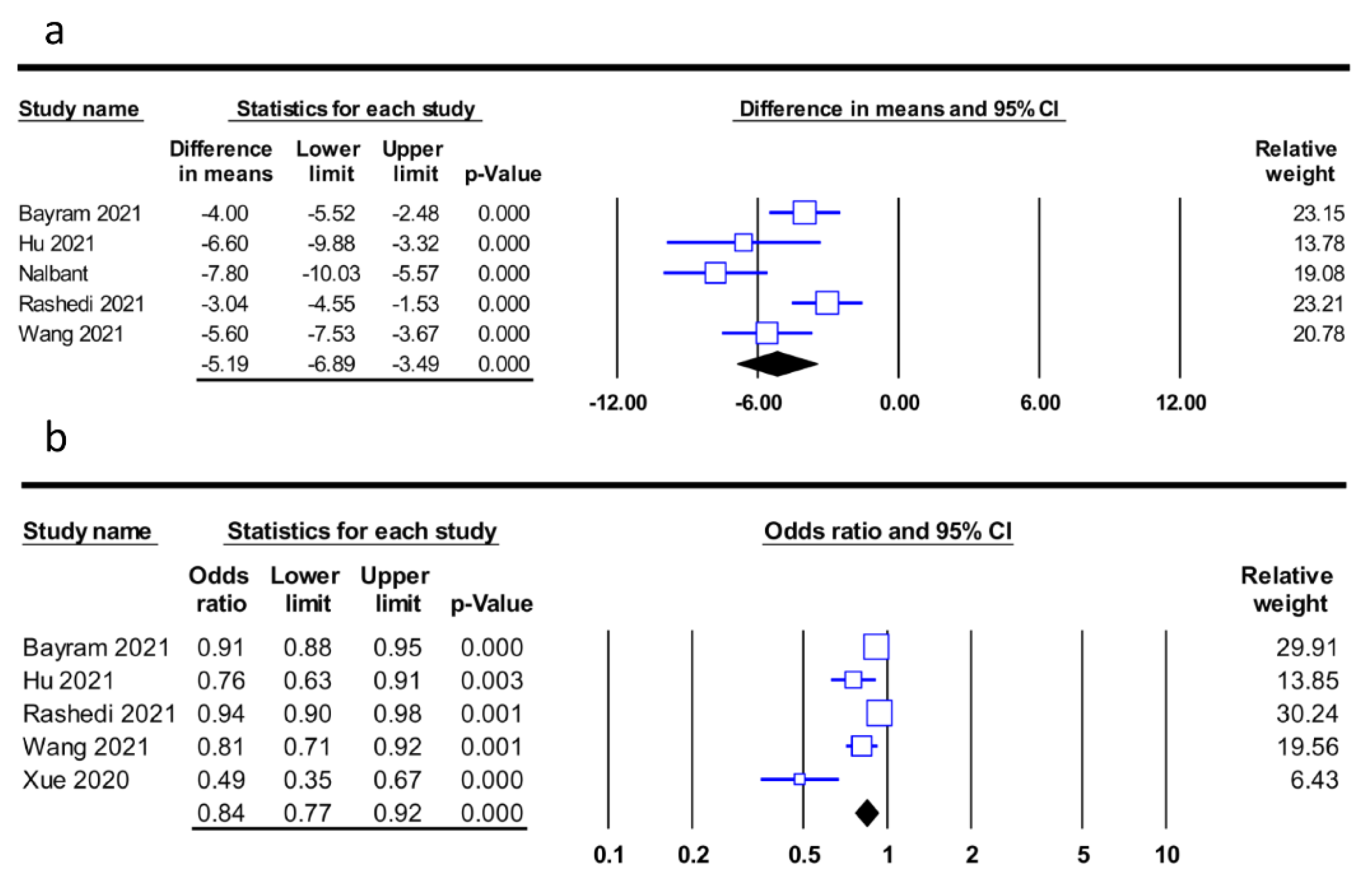
3.3.2. Secondary Outcome—Association of PNI with Disease Severity
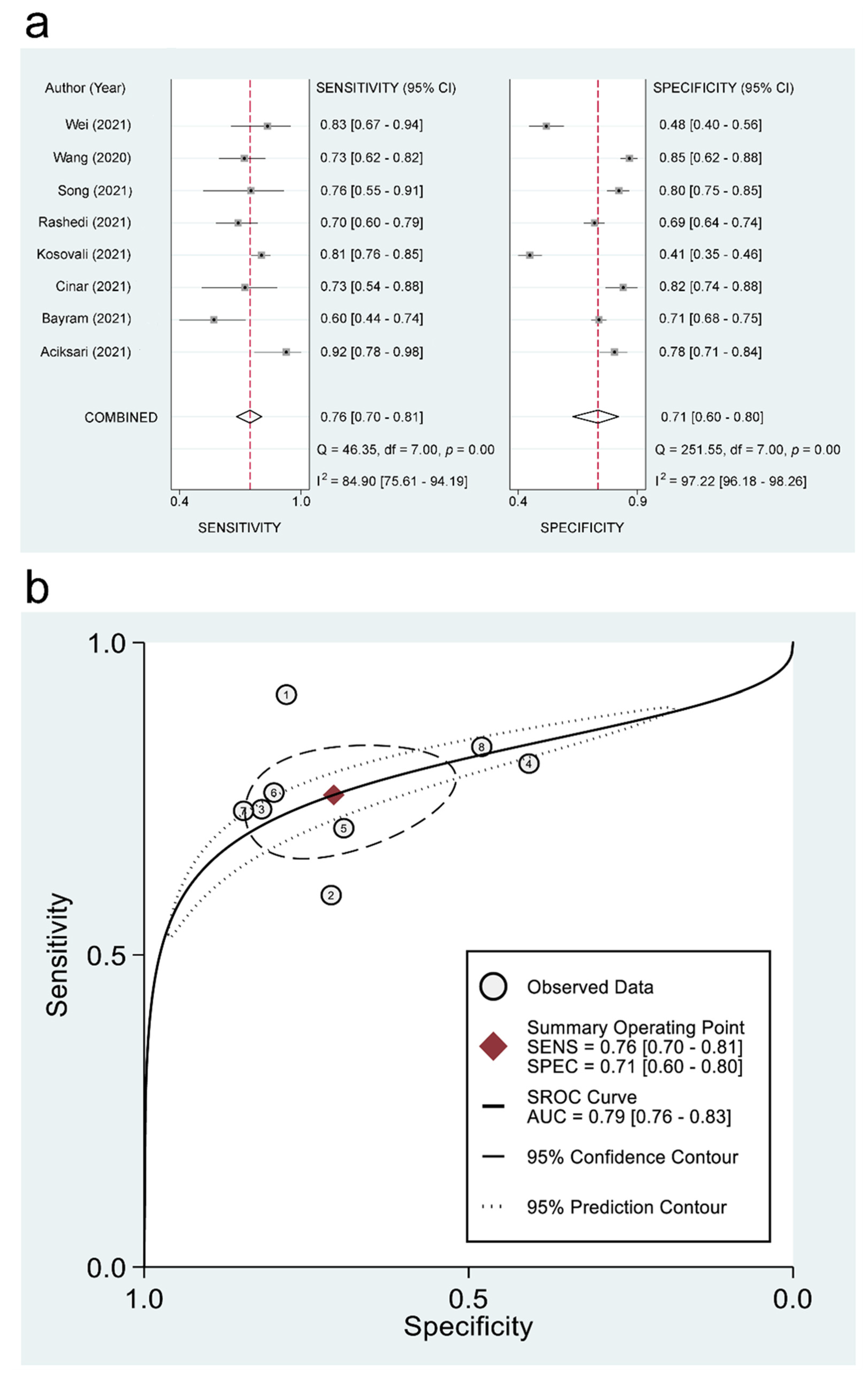
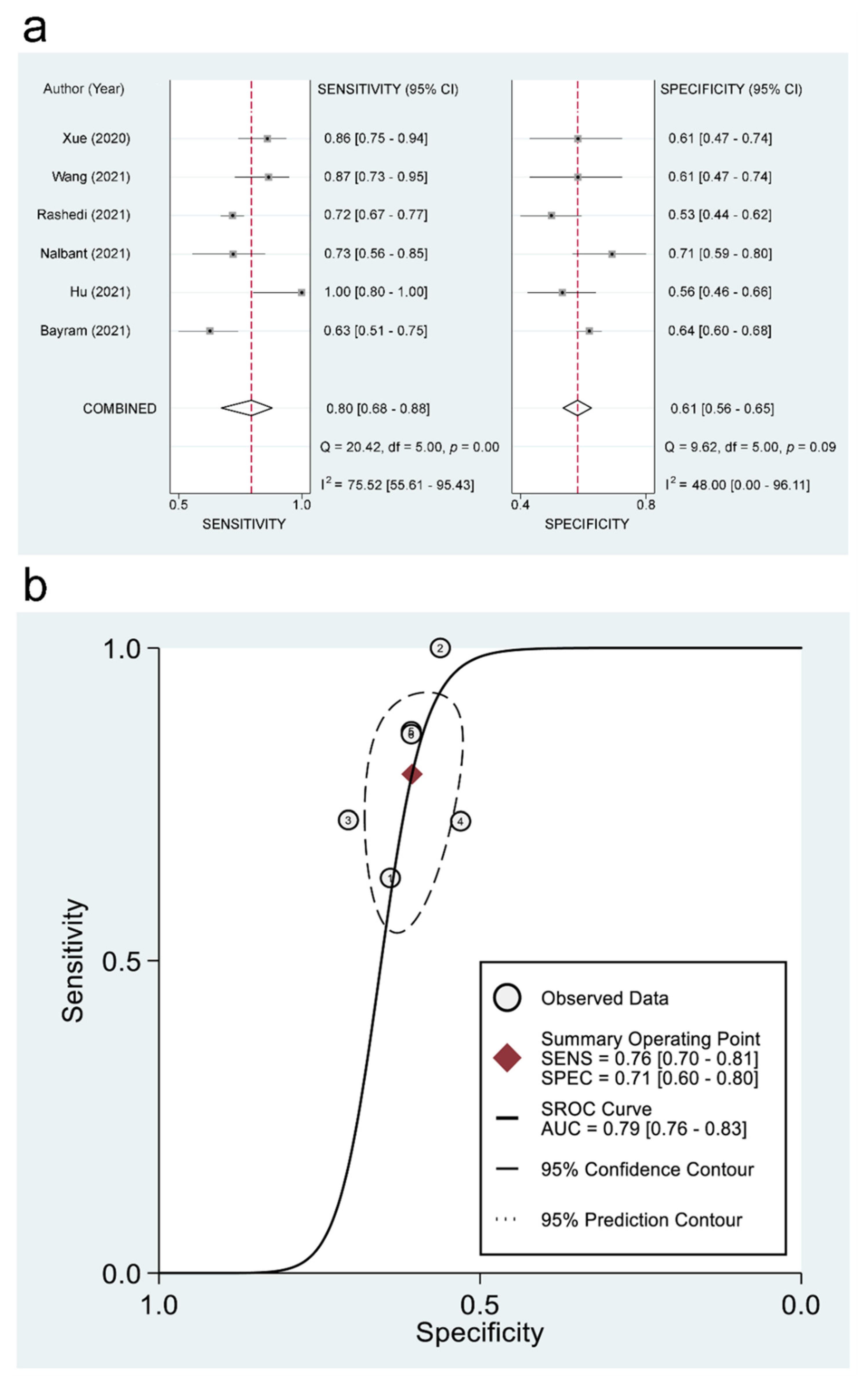
3.3.3. The Use of PNI for Predicting Mortality and Disease Severity: Pooled Estimates of Sensitivity/Specificity and sROC
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chang, D.; Chang, X.; He, Y.; Tan, K.J.K. The determinants of COVID-19 morbidity and mortality across countries. Sci. Rep. 2022, 12, 5888. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Reddy, S.G.K.; Mantena, M.; Garlapati, S.K.P.; Manohar, B.P.; Singh, H.; Bajwa, K.S.; Tiwari, H. COVID-2019-2020-2021: Systematic Review and Meta-Analysis. J. Pharm. Bioallied Sci. 2021, 13, S921–S926. [Google Scholar] [CrossRef]
- Li, L.Q.; Huang, T.; Wang, Y.Q.; Wang, Z.P.; Liang, Y.; Huang, T.B.; Zhang, H.Y.; Sun, W.; Wang, Y. COVID-19 patients’ clinical characteristics, discharge rate, and fatality rate of meta-analysis. J. Med. Virol. 2020, 92, 577–583. [Google Scholar] [CrossRef]
- Hu, H.; Pan, H.; Li, R.; He, K.; Zhang, H.; Liu, L. Increased Circulating Cytokines Have a Role in COVID-19 Severity and Death With a More Pronounced Effect in Males: A Systematic Review and Meta-Analysis. Front. Pharmacol. 2022, 13, 802228. [Google Scholar] [CrossRef]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Hajiasgharzadeh, K.; Jafarlou, M.; Mansoori, B.; Dastmalchi, N.; Baradaran, B.; Khabbazi, A. Inflammatory reflex disruption in COVID-19. Clin. Exp. Neuroimmunol. 2022. [Google Scholar] [CrossRef]
- Lai, C.C.; Liu, Y.H.; Wang, C.Y.; Wang, Y.H.; Hsueh, S.C.; Yen, M.Y.; Ko, W.C.; Hsueh, P.R. Asymptomatic carrier state, acute respiratory disease, and pneumonia due to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2): Facts and myths. J. Microbiol. Immunol. Infect. 2020, 53, 404–412. [Google Scholar] [CrossRef]
- Laino, M.E.; Ammirabile, A.; Lofino, L.; Lundon, D.J.; Chiti, A.; Francone, M.; Savevski, V. Prognostic findings for ICU admission in patients with COVID-19 pneumonia: Baseline and follow-up chest CT and the added value of artificial intelligence. Emerg. Radiol. 2022, 29, 243–262. [Google Scholar] [CrossRef]
- Song, F.; Ma, H.; Wang, S.; Qin, T.; Xu, Q.; Yuan, H.; Li, F.; Wang, Z.; Liao, Y.; Tan, X. Nutritional screening based on objective indices at admission predicts in-hospital mortality in patients with COVID-19. Nutr. J. 2021, 20, 46. [Google Scholar] [CrossRef]
- Alikiaii, B.; Heidari, Z.; Fazeli, A.; Rahimi Varposhti, M.; Moradi Farsani, D.; Fattahpour, S.; Rafiee, S.; Bagherniya, M. Evaluation of the effectiveness of the Nutritional Risk Screening System 2002 (NRS-2002) in COVID-19 patients admitted to the intensive care unit. Int. J. Clin. Pract. 2021, 75, e14934. [Google Scholar] [CrossRef]
- Pinato, D.J.; North, B.V.; Sharma, R. A novel, externally validated inflammation-based prognostic algorithm in hepatocellular carcinoma: The prognostic nutritional index (PNI). Br. J. Cancer 2012, 106, 1439–1445. [Google Scholar] [CrossRef]
- Wang, C.; He, W.; Yuan, Y.; Zhang, Y.; Li, K.; Zou, R.; Liao, Y.; Liu, W.; Yang, Z.; Zuo, D.; et al. Comparison of the prognostic value of inflammation-based scores in early recurrent hepatocellular carcinoma after hepatectomy. Liver Int. 2020, 40, 229–239. [Google Scholar] [CrossRef]
- Peng, J.C.; Nie, F.; Li, Y.J.; Xu, Q.Y.; Xing, S.P.; Gao, Y. Prognostic Nutritional Index as a Predictor of 30-Day Mortality Among Patients Admitted to Intensive Care Unit with Acute Exacerbation of Chronic Obstructive Pulmonary Disease: A Single-Center Retrospective Cohort Study. Med. Sci. Monit. 2022, 28, e934687. [Google Scholar] [CrossRef]
- Yao, C.; Liu, X.; Tang, Z. Prognostic role of neutrophil-lymphocyte ratio and platelet-lymphocyte ratio for hospital mortality in patients with AECOPD. Int. J. Chron. Obstruct. Pulmon. Dis. 2017, 12, 2285–2290. [Google Scholar] [CrossRef] [Green Version]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Vong, T.; Yanek, L.R.; Wang, L.; Yu, H.; Fan, C.; Zhou, E.; Oh, S.J.; Szvarca, D.; Kim, A.; Potter, J.J.; et al. Malnutrition Increases Hospital Length of Stay and Mortality among Adult Inpatients with COVID-19. Nutrients 2022, 14, 1310. [Google Scholar] [CrossRef]
- Bayram, M.; Yildirim, O.; Ozmen, R.S.; Soylu, B.; Dundar, A.S.; Koksal, A.R.; Ekinci, I.; Akarsu, M.; Tabak, O. Prognostic Nutritional Index and CRP, age, platelet count, albumin level score in predicting mortality and intensive care unit admission for COVID-19. Biomark. Med. 2021, 15, 1733–1740. [Google Scholar] [CrossRef]
- Çınar, T.; Hayıroğlu, M.İ.; Çiçek, V.; Kılıç, Ş.; Asal, S.; Yavuz, S.; Selçuk, M.; Yalçınkaya, E.; Keser, N.; Orhan, A.L. Is prognostic nutritional index a predictive marker for estimating all-cause in-hospital mortality in COVID-19 patients with cardiovascular risk factors? Heart Lung 2021, 50, 307–312. [Google Scholar] [CrossRef]
- Wang, R.; He, M.; Yin, W.; Liao, X.; Wang, B.; Jin, X.; Ma, Y.; Yue, J.; Bai, L.; Liu, D.; et al. The Prognostic Nutritional Index is associated with mortality of COVID-19 patients in Wuhan, China. J. Clin. Lab. Anal. 2020, 34, e23566. [Google Scholar] [CrossRef] [PubMed]
- Gómez, C.A.; Sun, C.K.; Tsai, I.T.; Chang, Y.P.; Lin, M.C.; Hung, I.Y.; Chang, Y.J.; Wang, L.K.; Lin, Y.T.; Hung, K.C. Mortality and risk factors associated with pulmonary embolism in coronavirus disease 2019 patients: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 16025. [Google Scholar] [CrossRef]
- Hayden, J.A.; van der Windt, D.A.; Cartwright, J.L.; Côté, P.; Bombardier, C. Assessing bias in studies of prognostic factors. Ann. Intern. Med. 2013, 158, 280–286. [Google Scholar] [CrossRef]
- Hung, K.C.; Wang, L.K.; Lin, Y.T.; Yu, C.H.; Chang, C.Y.; Sun, C.K.; Chen, J.Y. Association of preoperative vitamin D deficiency with the risk of postoperative delirium and cognitive dysfunction: A meta-analysis. J. Clin. Anesth. 2022, 79, 110681. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Takwoingi, Y.; Riley, R.D.; Deeks, J.J. Meta-analysis of diagnostic accuracy studies in mental health. Evid. Based Ment. Health 2015, 18, 103–109. [Google Scholar] [CrossRef]
- Li, Y.; Li, H.; Song, C.; Lu, R.; Zhao, Y.; Lin, F.; Han, D.; Chen, L.; Pan, P.; Dai, M. Early Prediction of Disease Progression in Patients with Severe COVID-19 Using C-Reactive Protein to Albumin Ratio. Dis. Markers 2021, 2021, 6304189. [Google Scholar] [CrossRef]
- Açıksarı, G.; Koçak, M.; Çağ, Y.; Altunal, L.N.; Atıcı, A.; Çelik, F.B.; Bölen, F.; Açıksarı, K.; Çalışkan, M. Prognostic value of inflammatory biomarkers in patients with severe COVID-19: A single-center retrospective study. Biomark. Insights 2021, 16, 11772719211027022. [Google Scholar] [CrossRef]
- Doganci, S.; Ince, M.; Ors, N.; Yildirim, A.; Sir, E.; Karabacak, K.; Eksert, S.; Ozgurtas, T.; Tasci, C.; Dogan, D. A new COVID-19 prediction scoring model for in-hospital mortality: Experiences from Turkey, single center retrospective cohort analysis. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 10247–10257. [Google Scholar]
- Wang, Z.-H.; Lin, Y.-W.; Wei, X.-B.; Li, F.; Liao, X.-L.; Yuan, H.-Q.; Huang, D.-Z.; Qin, T.-H.; Geng, H.; Wang, S.-H. Predictive value of prognostic nutritional index on COVID-19 severity. Front. Nutr. 2021, 7, 582736. [Google Scholar] [CrossRef]
- Xue, G.; Gan, X.; Wu, Z.; Xie, D.; Xiong, Y.; Hua, L.; Zhou, B.; Zhou, N.; Xiang, J.; Li, J. Novel serological biomarkers for inflammation in predicting disease severity in patients with COVID-19. Int. Immunopharmacol. 2020, 89, 107065. [Google Scholar] [CrossRef] [PubMed]
- Kosovali, B.D.; Kucuk, B.; Balkiz Soyal, O.; Mehmet Mutlu, N. Can prognostic nutritional index predict mortality in intensive care patients with COVID-19? Int. J. Clin. Pract. 2021, 75, e14800. [Google Scholar] [CrossRef] [PubMed]
- Nalbant, A.; Demirci, T.; Kaya, T.; Aydın, A.; Altındiş, M.; Güçlü, E. Can prognostic nutritional index and systemic immune-inflammatory index predict disease severity in COVID-19? Int. J. Clin. Pract. 2021, 75, e14544. [Google Scholar] [CrossRef] [PubMed]
- Wei, W.; Wu, X.; Jin, C.; Mu, T.; Gu, G.; Min, M.; Mu, S.; Han, Y. Predictive significance of the prognostic nutritional index (PNI) in patients with severe COVID-19. J. Immunol. Res. 2021, 2021, 9917302. [Google Scholar] [CrossRef]
- Hu, X.; Deng, H.; Wang, Y.; Chen, L.; Gu, X.; Wang, X. Predictive value of the prognostic nutritional index for the severity of coronavirus disease 2019. Nutrition 2021, 84, 111123. [Google Scholar] [CrossRef]
- Rashedi, S.; Keykhaei, M.; Pazoki, M.; Ashraf, H.; Najafi, A.; Kafan, S.; Peirovi, N.; Najmeddin, F.; Jazayeri, S.A.; Kashani, M. Clinical significance of prognostic nutrition index in hospitalized patients with COVID-19: Results from single-center experience with systematic review and meta-analysis. Nutr. Clin. Pract. 2021, 36, 970–983. [Google Scholar] [CrossRef]
- Onodera, T.; Goseki, N.; Kosaki, G. Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients. Nihon Geka Gakkai Zasshi 1984, 85, 1001–1005. [Google Scholar]
- McGovern, J.; Al-Azzawi, Y.; Kemp, O.; Moffitt, P.; Richards, C.; Dolan, R.D.; Laird, B.J.; McMillan, D.C.; Maguire, D. The relationship between frailty, nutritional status, co-morbidity, CT-body composition and systemic inflammation in patients with COVID-19. J. Transl. Med. 2022, 20, 98. [Google Scholar] [CrossRef]
- Meng, Y.; Wang, J.; Wen, K.; Da, W.; Yang, K.; Zhou, S.; Tao, Z.; Liu, H.; Tao, L. Clinical Features and Laboratory Examination to Identify Severe Patients with COVID-19: A Systematic Review and Meta-Analysis. Biomed. Res. Int. 2021, 2021, 6671291. [Google Scholar] [CrossRef]
- Cheng, Y.; Luo, R.; Wang, K.; Zhang, M.; Wang, Z.; Dong, L.; Li, J.; Yao, Y.; Ge, S.; Xu, G. Kidney disease is associated with in-hospital death of patients with COVID-19. Kidney Int. 2020, 97, 829–838. [Google Scholar] [CrossRef]
- Shi, C.; Wang, L.; Ye, J.; Gu, Z.; Wang, S.; Xia, J.; Xie, Y.; Li, Q.; Xu, R.; Lin, N. Predictors of mortality in patients with coronavirus disease 2019: A systematic review and meta-analysis. BMC Infect. Dis. 2021, 21, 663. [Google Scholar] [CrossRef]
- Wang, Y.; Zhao, J.; Yang, L.; Hu, J.; Yao, Y. Value of the Neutrophil-Lymphocyte Ratio in Predicting COVID-19 Severity: A Meta-analysis. Dis. Markers 2021, 2021, 2571912. [Google Scholar] [CrossRef]
- Tirupathi, R.; Muradova, V.; Shekhar, R.; Salim, S.A.; Al-Tawfiq, J.A.; Palabindala, V. COVID-19 disparity among racial and ethnic minorities in the US: A cross sectional analysis. Travel. Med. Infect. Dis. 2020, 38, 101904. [Google Scholar] [CrossRef]
- Mackey, K.; Ayers, C.K.; Kondo, K.K.; Saha, S.; Advani, S.M.; Young, S.; Spencer, H.; Rusek, M.; Anderson, J.; Veazie, S.; et al. Racial and Ethnic Disparities in COVID-19-Related Infections, Hospitalizations, and Deaths: A Systematic Review. Ann. Intern. Med. 2021, 174, 362–373. [Google Scholar] [CrossRef]
- Gao, Z.; Xu, Y.; Sun, C.; Wang, X.; Guo, Y.; Qiu, S.; Ma, K. A systematic review of asymptomatic infections with COVID-19. J. Microbiol. Immunol. Infect. 2021, 54, 12–16. [Google Scholar] [CrossRef]
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2021, 19, 141–154. [Google Scholar] [CrossRef]
- Attaway, A.H.; Scheraga, R.G.; Bhimraj, A.; Biehl, M.; Hatipoğlu, U. Severe covid-19 pneumonia: Pathogenesis and clinical management. BMJ 2021, 372, n436. [Google Scholar] [CrossRef]
- Higuera-de-la-Tijera, F.; Servín-Caamaño, A.; Reyes-Herrera, D.; Flores-López, A.; Robiou-Vivero, E.J.A.; Martínez-Rivera, F.; Galindo-Hernández, V.; Rosales-Salyano, V.H.; Casillas-Suárez, C.; Chapa-Azuela, O.; et al. The Age-AST-D Dimer (AAD) Regression Model Predicts Severe COVID-19 Disease. Dis. Markers 2021, 2021, 6658270. [Google Scholar] [CrossRef]
- Docherty, A.B.; Harrison, E.M.; Green, C.A.; Hardwick, H.E.; Pius, R.; Norman, L.; Holden, K.A.; Read, J.M.; Dondelinger, F.; Carson, G.; et al. Features of 20 133 UK patients in hospital with covid-19 using the ISARIC WHO Clinical Characterisation Protocol: Prospective observational cohort study. BMJ 2020, 369, m1985. [Google Scholar] [CrossRef]
- Liu, G.; Zhang, S.; Mao, Z.; Wang, W.; Hu, H. Clinical significance of nutritional risk screening for older adult patients with COVID-19. Eur. J. Clin. Nutr. 2020, 74, 876–883. [Google Scholar] [CrossRef]
- Corish, C.A.; Bardon, L.A. Malnutrition in older adults: Screening and determinants. Proc. Nutr. Soc. 2019, 78, 372–379. [Google Scholar] [CrossRef] [PubMed]
- Luan, C.W.; Tsai, Y.T.; Yang, H.Y.; Chen, K.Y.; Chen, P.H.; Chou, H.H. Pretreatment prognostic nutritional index as a prognostic marker in head and neck cancer: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 17117. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Gao, P.; Song, Y.; Sun, J.; Chen, X.; Zhao, J.; Ma, B.; Wang, Z. The prognostic nutritional index is a predictive indicator of prognosis and postoperative complications in gastric cancer: A meta-analysis. Eur. J. Surg. Oncol. 2016, 42, 1176–1182. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Zhou, H.; Zhou, Y.; Wu, X.; Zhao, Y.; Lu, Y.; Tan, W.; Yuan, M.; Ding, X.; Zou, J.; et al. Risk factors associated with disease severity and length of hospital stay in COVID-19 patients. J. Infect. 2020, 81, e95–e97. [Google Scholar] [CrossRef]
- Satici, M.O.; Islam, M.M.; Satici, C.; Uygun, C.N.; Ademoglu, E.; Altunok, İ.; Aksel, G.; Eroglu, S.E. The role of a noninvasive index ‘Spo2/Fio2’ in predicting mortality among patients with COVID-19 pneumonia. Am. J. Emerg. Med. 2022, 57, 54–59. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Studies | Patient Enrollment Period (2020) | Age (Years) | Male (%) | Patient Number (n = 4204) | Definition of Severity | Outcomes | Country |
|---|---|---|---|---|---|---|---|
| Aciksari 2021 | March–August † | 60 | 53 | 223 | a | Mortality/severity | Turkey |
| Bayram 2021 | September–December | 74 vs. 61 | 54.8 | 748 | ICU admission | Mortality/severity | Turkey |
| Cinar 2021 | March–August | 62 vs. 50 | 59.2 | 196 | NA | Mortality | Turkey |
| Doganci 2020 | March–May | 57 | 50 | 397 | NA | Mortality | Turkey |
| Hu 2021 | January–February | 44 | 55.7 | 122 | a | Severity | China |
| Kosovali 2021 | March–July ¶ | 69 | 54.9 | 690 | NA | Mortality | Turkey |
| Nalbant 2021 | January–April | 58 vs. 70 | 50.8 | 118 | ICU admission | Severity | Turkey |
| Rashedi 2021 | February–November | 61 | 61.5 | 504 | b | Mortality/severity | Iran |
| Song 2021 | January–May § | 58 | 52.5 | 295 | a | Mortality/severity | China |
| Wang 2020 | January–February | 58 | 45.8 | 450 | NA | Mortality | China |
| Wang 2021 | January–March | 65 vs. 49 | 42.3 | 111 | c | Severity | China |
| Wei 2021 | NA § | 74 vs. 55 | 49.2 | 236 | d | Mortality/severity | China |
| Xue 2020 | February–March | 62 | 56.1 | 114 | a | Severity | China |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hung, K.-C.; Ko, C.-C.; Wang, L.-K.; Liu, P.-H.; Chen, I.-W.; Huang, Y.-T.; Sun, C.-K. Association of Prognostic Nutritional Index with Severity and Mortality of Hospitalized Patients with COVID-19: A Systematic Review and Meta-Analysis. Diagnostics 2022, 12, 1515. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12071515
Hung K-C, Ko C-C, Wang L-K, Liu P-H, Chen I-W, Huang Y-T, Sun C-K. Association of Prognostic Nutritional Index with Severity and Mortality of Hospitalized Patients with COVID-19: A Systematic Review and Meta-Analysis. Diagnostics. 2022; 12(7):1515. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12071515
Chicago/Turabian StyleHung, Kuo-Chuan, Ching-Chung Ko, Li-Kai Wang, Ping-Hsin Liu, I-Wen Chen, Yen-Ta Huang, and Cheuk-Kwan Sun. 2022. "Association of Prognostic Nutritional Index with Severity and Mortality of Hospitalized Patients with COVID-19: A Systematic Review and Meta-Analysis" Diagnostics 12, no. 7: 1515. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12071515