
Decreased Levels of SARS-CoV-2 Fusion-Inhibitory Antibodies in the Serum of Aged COVID-19 Patients

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting and Participants
2.2. Recorded Data
2.3. Detection of Total Anti-S Antibodies
2.4. Detection of fiAbs
2.5. Statistical Analysis
3. Results
3.1. Participants
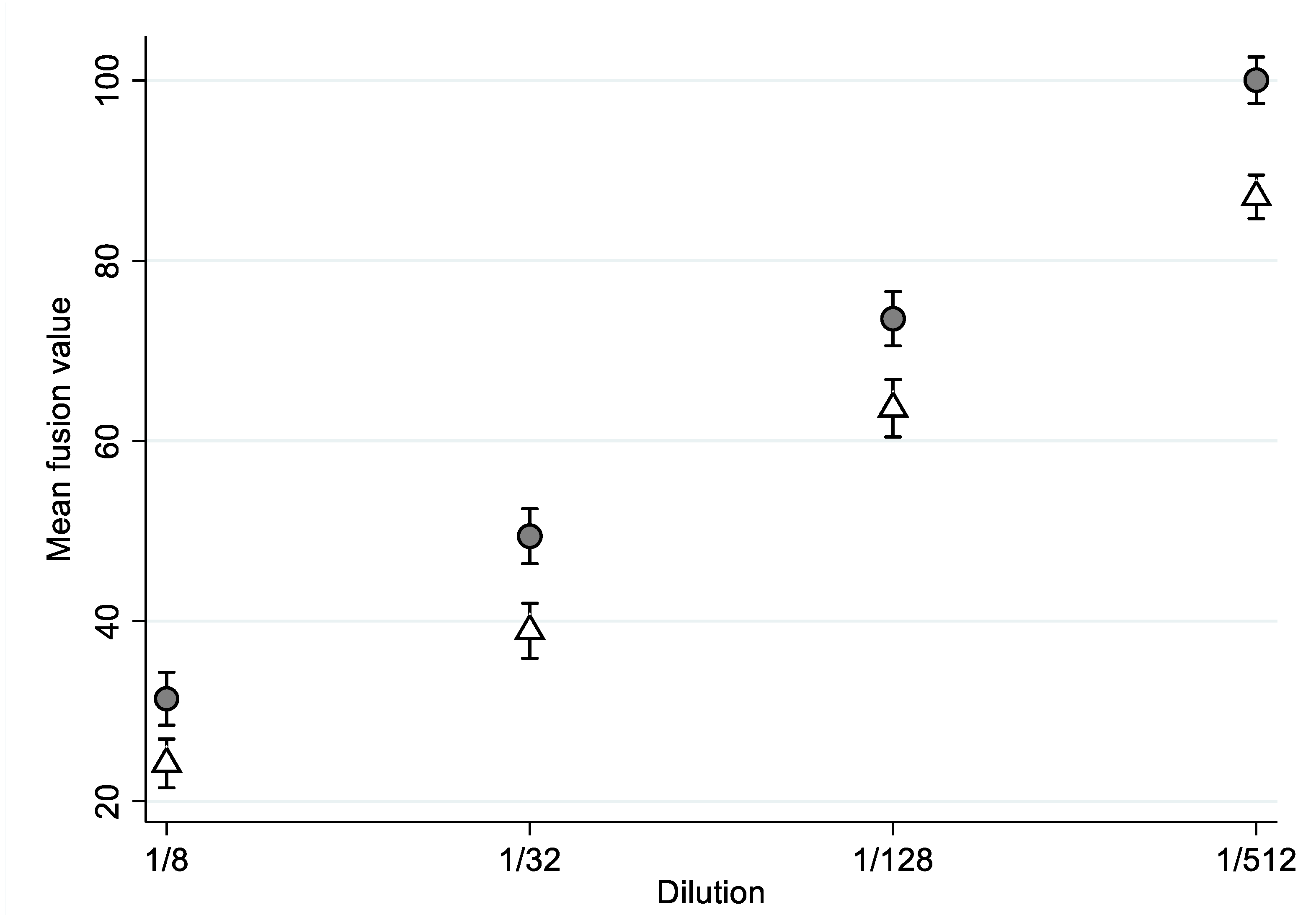
3.2. Detection of SARS-CoV-2 fiAbs
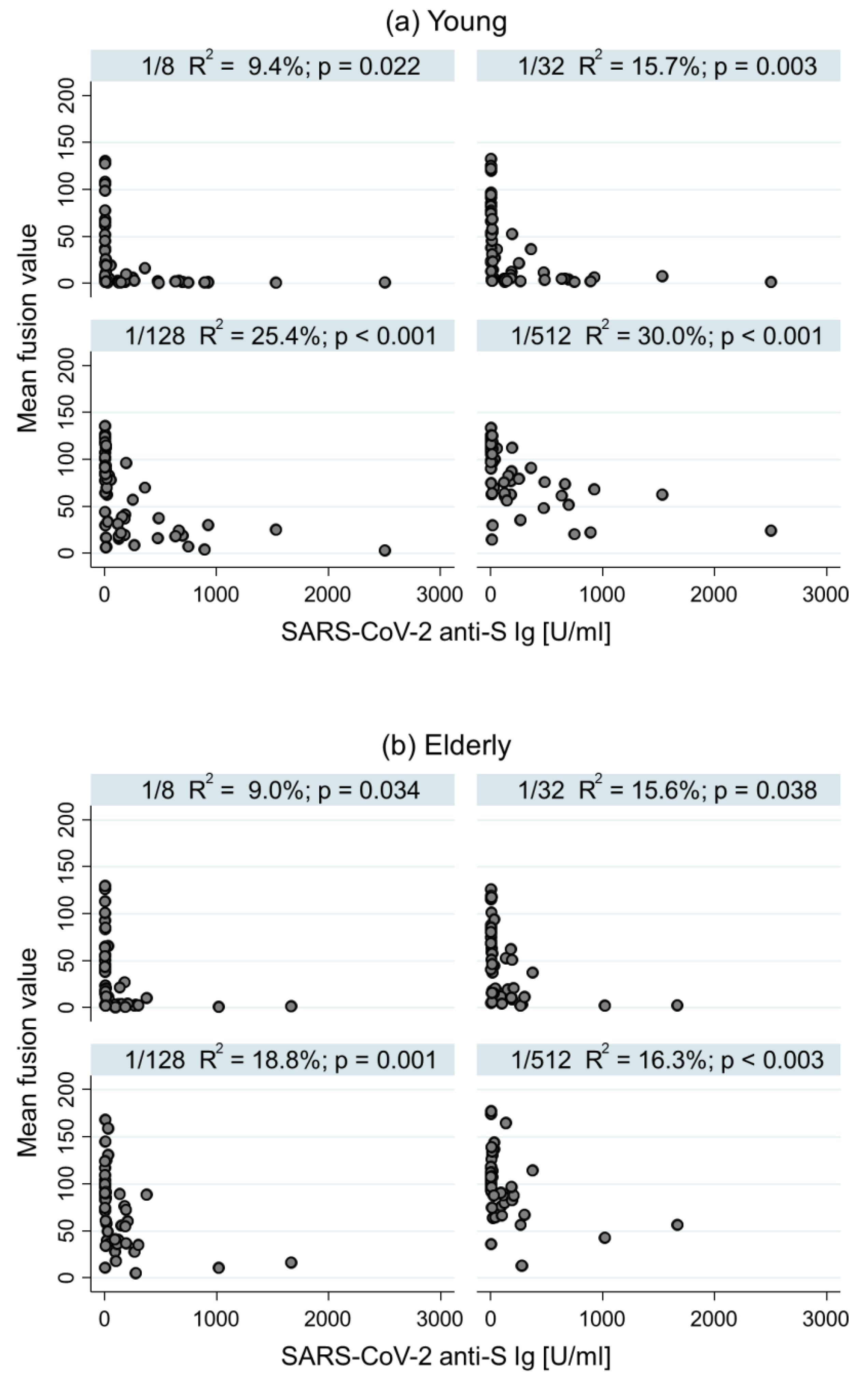
3.3. Comparison between fiAbs and Total Anti-S Ig Antibody Level
3.4. Predictive Factors for the Development of SARS-CoV-2 fiAbs
3.5. Factors Associated with Intra-Hospital Mortality
4. Discussion
4.1. fiAbs Level in the Elderly
4.2. Correlation between Neutralizing/Fusion-Inhibitory Abs and Anti-S Ig Levels
4.3. Frailty and Severity: Factors Associated with Development of fiAbs
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Weekly Epidemiological Update on COVID-19–18 January 2022. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---18-january-2022 (accessed on 30 January 2022).
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Mendes, A.; Serratrice, C.; Herrmann, F.R.; Genton, L.; Périvier, S.; Scheffler, M.; Fassier, T.; Huber, P.; Jacques, M.-C.; Prendki, V.; et al. Predictors of in-hospital mortality in older patients with COVID-19: The COVIDAge Study. J. Am. Med. Dir. Assoc. 2020, 21, 1546–1554. [Google Scholar] [CrossRef]
- Niu, S.; Tian, S.; Lou, J.; Kang, X.; Zhang, L.; Lian, H.; Zhang, J. Clinical characteristics of older patients infected with COVID-19: A descriptive study. Arch. Gerontol. Geriatr. 2020, 89, 104058. [Google Scholar] [CrossRef]
- Castelo-Branco, C.; Soveral, I. The immune system and aging: A review. Gynecol. Endocrinol. 2014, 30, 16–22. [Google Scholar] [CrossRef]
- Murray, M.A.; Chotirmall, S.H. The Impact of Immunosenescence on Pulmonary Disease. Mediators Inflamm. 2015, 2015, 692546. [Google Scholar] [CrossRef]
- Murata, Y.; Walsh, E.E.; Falsey, A.R. Pulmonary complications of interpandemic influenza A in hospitalized adults. J. Infect. Dis. 2007, 195, 1029–1037. [Google Scholar] [CrossRef] [Green Version]
- Kawasuji, H.; Morinaga, Y.; Tani, H.; Kimura, M.; Yamada, H.; Yoshida, Y.; Takegoshi, Y.; Kaneda, M.; Murai, Y.; Kimoto, K.; et al. Delayed neutralizing antibody response in the acute phase correlates with severe progression of COVID-19. Sci. Rep. 2021, 11, 16535. [Google Scholar] [CrossRef]
- Xu, X.; Nie, S.; Wang, Y.; Long, Q.; Zhu, H.; Zhang, X.; Sun, J.; Zeng, Q.; Zhao, J.; Liu, L.; et al. Dynamics of neutralizing antibody responses to SARS-CoV-2 in patients with COVID-19: An observational study. Signal Transduct. Target. Ther. 2021, 6, 197. [Google Scholar] [CrossRef]
- Long, Q.-X.; Liu, B.-Z.; Deng, H.-J.; Wu, G.-C.; Deng, K.; Chen, Y.-K.; Liao, P.; Qiu, J.-F.; Lin, Y.; Cai, X.-F.; et al. Antibody responses to SARS-CoV-2 in patients with COVID-19. Nat. Med. 2020, 26, 845–848. [Google Scholar] [CrossRef]
- Ju, B.; Zhang, Q.; Ge, J.; Wang, R.; Sun, J.; Ge, X.; Yu, J.; Shan, S.; Zhou, B.; Song, S.; et al. Human neutralizing antibodies elicited by SARS-CoV-2 infection. Nature 2020, 584, 115–119. [Google Scholar] [CrossRef]
- Liu, L.; Wang, P.; Nair, M.S.; Yu, J.; Rapp, M.; Wang, Q.; Luo, Y.; Chan, J.F.-W.; Sahi, V.; Figueroa, A.; et al. Potent neutralizing antibodies against multiple epitopes on SARS-CoV-2 spike. Nature 2020, 584, 450–456. [Google Scholar] [CrossRef]
- Boonyaratanakornkit, J.; Morishima, C.; Selke, S.; Zamora, D.; McGuffin, S.; Shapiro, A.E.; Campbell, V.L.; McClurkan, C.L.; Jing, L.; Gross, R.; et al. Clinical, laboratory, and temporal predictors of neutralizing antibodies against SARS-CoV-2 among COVID-19 convalescent plasma donor candidates. J. Clin. Investig. 2021, 131, e144930. [Google Scholar] [CrossRef] [PubMed]
- Wu, F.; Liu, M.; Wang, A.; Lu, L.; Wang, Q.; Gu, C.; Chen, J.; Wu, Y.; Xia, S.; Ling, Y.; et al. Evaluating the Association of Clinical Characteristics with Neutralizing Antibody Levels in Patients Who Have Recovered from Mild COVID-19 in Shanghai, China. JAMA Intern. Med. 2020, 180, 1356–1362. [Google Scholar] [CrossRef] [PubMed]
- Kalkan Yazıcı, M.; Koç, M.M.; Çetin, N.S.; Karaaslan, E.; Okay, G.; Durdu, B.; Sümbül, B.; Doymaz, M.Z. Discordance between Serum Neutralizing Antibody Titers and the Recovery from COVID-19. J. Immunol. 2020, 205, 2719–2725. [Google Scholar] [CrossRef] [PubMed]
- Abdul, F.; Ribaux, P.; Caillon, A.; Malézieux-Picard, A.; Prendki, V.; Zhukovsky, N.; Delhaes, F.; Krause, K.-H.; Preynat-Seauve, O. A cellular assay for spike/ACE2 fusion: Quantification of fusion-inhibitory antibodies after COVID-19 and vaccination. bioRxiv 2022. [Google Scholar] [CrossRef]
- Vernaz, N.; Agoritsas, T.; Calmy, A.; Gayet-Ageron, A.; Gold, G.; Perrier, A.; Picard, F.; Prendki, V.; Reny, J.-L.; Samer, C.; et al. Early experimental COVID-19 therapies: Associations with length of hospital stay, mortality and related costs. Swiss Med. Wkly. 2020, 150, w20446. [Google Scholar] [CrossRef]
- Co-Medications Administered with Hydroxychloroquine in COVID-19 Inpatients: Prevalence and Ethical Implications. Swiss Medical Weekly. Available online: https://smw.ch/op-eds/post/co-medications-administered-with-hydroxychloroquine-in-covid-19-inpatients (accessed on 18 March 2022).
- Rockwood, K.; Song, X.; MacKnight, C.; Bergman, H.; Hogan, D.B.; McDowell, I.; Mitnitski, A. A global clinical measure of fitness and frailty in elderly people. CMAJ 2005, 173, 489–495. [Google Scholar] [CrossRef] [Green Version]
- Fine, M.J.; Auble, T.E.; Yealy, D.M.; Hanusa, B.H.; Weissfeld, L.A.; Singer, D.E.; Coley, C.M.; Marrie, T.J.; Kapoor, W.N. A prediction rule to identify low-risk patients with community-acquired pneumonia. N. Engl. J. Med. 1997, 336, 243–250. [Google Scholar] [CrossRef]
- COVID-19 Clinical Management: Living Guidance. Available online: https://www.who.int/publications-detail-redirect/WHO-2019-nCoV-clinical-2021-1 (accessed on 4 June 2021).
- Riester, E.; Findeisen, P.; Hegel, J.K.; Kabesch, M.; Ambrosch, A.; Rank, C.M.; Pessl, F.; Laengin, T.; Niederhauser, C. Performance evaluation of the Roche Elecsys Anti-SARS-CoV-2 S immunoassay. J. Virol. Methods 2021, 297, 114271. [Google Scholar] [CrossRef]
- Müller, L.; Andrée, M.; Moskorz, W.; Drexler, I.; Walotka, L.; Grothmann, R.; Ptok, J.; Hillebrandt, J.; Ritchie, A.; Rabl, D.; et al. Age-dependent immune response to the Biontech/Pfizer BNT162b2 COVID-19 vaccination. Clin. Infect. Dis. 2021, 73, 2065–2072. [Google Scholar] [CrossRef]
- Huynh, A.; Arnold, D.M.; Smith, J.W.; Moore, J.C.; Zhang, A.; Chagla, Z.; Harvey, B.J.; Stacey, H.D.; Ang, J.C.; Clare, R.; et al. Characteristics of Anti-SARS-CoV-2 Antibodies in Recovered COVID-19 Subjects. Viruses 2021, 13, 697. [Google Scholar] [CrossRef] [PubMed]
- Rockstroh, A.; Wolf, J.; Fertey, J.; Kalbitz, S.; Schroth, S.; Lübbert, C.; Ulbert, S.; Borte, S. Correlation of humoral immune responses to different SARS-CoV-2 antigens with virus neutralizing antibodies and symptomatic severity in a German COVID-19 cohort. Emerg. Microbes Infect. 2021, 10, 774–781. [Google Scholar] [CrossRef]
- Zhou, C.; Zhang, T.; Ren, H.; Sun, S.; Yu, X.; Sheng, J.; Shi, Y.; Zhao, H. Impact of age on duration of viral RNA shedding in patients with COVID-19. Aging 2020, 12, 22399–22404. [Google Scholar] [CrossRef]
- Chen, W.; Zhang, J.; Qin, X.; Wang, W.; Xu, M.; Wang, L.-F.; Xu, C.; Tang, S.; Liu, P.; Zhang, L.; et al. SARS-CoV-2 neutralizing antibody levels are correlated with severity of COVID-19 pneumonia. Biomed. Pharmacother. 2020, 130, 110629. [Google Scholar] [CrossRef]
- Lucas, C.; Klein, J.; Sundaram, M.E.; Liu, F.; Wong, P.; Silva, J.; Mao, T.; Oh, J.E.; Mohanty, S.; Huang, J.; et al. Delayed production of neutralizing antibodies correlates with fatal COVID-19. Nat. Med. 2021, 27, 1178–1186. [Google Scholar] [CrossRef]
- Vetrano, D.L.; Triolo, F.; Maggi, S.; Malley, R.; Jackson, T.A.; Poscia, A.; Bernabei, R.; Ferrucci, L.; Fratiglioni, L. Fostering healthy aging: The interdependency of infections, immunity and frailty. Ageing Res. Rev. 2021, 69, 101351. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Young | Elderly | Total | p-Value | |
|---|---|---|---|---|
| N; Mean ± SD | N; Mean ± SD | N; Mean ± SD | ||
| Number | 56 | 52 | 108 | |
| Age (years) | 56; 52.3 ± 9.9 | 52; 85.3 ± 6.9 | 108; 68.4 ± 18.6 | <0.001 |
| Gender (male) | 46 (82.1%) | 20 (38.5%) | 66 (61.1%) | <0.001 |
| Place of living (home) | 56 (100.0%) | 46 (88.7%) | 102 (94.4%) | 0.021 |
| Number of comorbidities | <0.001 | |||
| 0 | 27 (48.2%) | 0 (0.0%) | 27 (25.0%) | |
| 1 | 19 (33.9%) | 46 (88.5%) | 65 (60.2%) | |
| 2 | 7 (12.5%) | 2 (3.8%) | 9 (8.3%) | |
| 3 | 3 (5.4%) | 2 (3.8%) | 5 (4.6%) | |
| 4 | 0 (0.0%) | 2 (3.8%) | 2 (1.9%) | |
| Clinical frailty scale | <0.001 | |||
| 1 | 36 (64.3%) | 0 (0.0%) | 36 (33.3%) | |
| 2 | 11 (19.6%) | 0 (0.0%) | 11 (10.2%) | |
| 3 | 6 (10.7%) | 4 (7.7%) | 10 (9.3%) | |
| 4 | 1 (1.8%) | 14 (26.9%) | 15 (13.9%) | |
| 5 | 1 (1.8%) | 8 (15.4%) | 9 (8.3%) | |
| 6 | 0 (0.0%) | 17 (32.7%) | 17 (15.7%) | |
| 7 | 1 (1.8%) | 8 (15.4%) | 9 (8.3%) | |
| 8 | 0 (0.0%) | 1 (1.9%) | 1 (0.9%) | |
| 9 | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| COPD | 0 (0.0%) | 8 (13.5%) | 8 (7.4%) | 0.010 |
| BMI | 39; 29.4 ± 6.8 | 50; 24.1 ± 5.5 | 89; 26.4 ± 6.6 | <0.001 |
| Immunosuppression | 4 (7.1%) | 3 (5.8%) | 7 (6.5%) | 1.000 |
| Diabetes | 9 (16.1%) | 8 (15.4%) | 17 (15.7%) | 1.000 |
| Chronic cardiac failure | 1 (1.8%) | 11 (21.6%) | 12 (11.2%) | 0.001 |
| Hypertension | 12 (21.4%) | 4 (7.7%) | 16 (14.8%) | 0.059 |
| Kidney disease | 2 (3.6%) | 9 (17.3%) | 11 (10.2%) | 0.025 |
| Cognitive disorders | 1 (1.8%) | 9 (17.3%) | 10 (9.2%) | 0.007 |
| Active neoplasia-solid cancer or lymphoma | 2 (3.6%) | 3 (5.8%) | 5 (4.6%) | 0.670 |
| Symptoms at admission (new or increasing)or biological markers | ||||
| Delay PSO—admission (days) | 56; 9.2 ± 4.0 | 52; 3.7 ± 6.3 | 108; 6.5 ± 5.9 | <0.001 |
| Delay PSO—antibody testing (days) | 56; 13.2 ± 3.9 | 52; 15.2 ± 5.5 | 108; 14.2 ± 4.8 | 0.030 |
| Cough | 46 (82.1%) | 30 (61.2%) | 76 (72.4%) | 0.014 |
| Sputum production | 14 (25.0%) | 7 (14.3%) | 21 (20.0%) | 0.155 |
| Myalgia | 23 (41.1%) | 4 (8.2%) | 27 (25.7%) | <0.001 |
| Tiredness | 20 (35.7%) | 23 (46.9%) | 43 (41.0%) | 0.264 |
| Delirium | 4 (7.1%) | 7 (14.3%) | 11 (10.5%) | 0.224 |
| Headache | 19 (33.9%) | 4 (8.2%) | 23 (21.9%) | 0.001 |
| Ageusia | 8 (14.3%) | 1 (2.0%) | 9 (8.6%) | 0.046 |
| Anosmia | 8 (14.3%) | 0 (0.0%) | 8 (7.6%) | 0.006 |
| Rhinorrhea | 10 (17.9%) | 4 (8.2%) | 14 (13.3%) | 0.139 |
| Diarrhea | 15 (26.8%) | 12 (24.5%) | 27 (25.7%) | 0.583 |
| Dyspnea | 43 (76.8%) | 27 (56.3%) | 70 (67.3%) | 0.036 |
| Fall | 1 (1.8%) | 11 (22.4%) | 12 (11.5%) | 0.001 |
| PSI | 56; 75.7 ± 26.9 | 52; 11.4 ± 32.1 | 108; 44.8 ± 43.7 | <0.001 |
| C-reactive protein at admission (mg/L) | 55; 101.9 ± 72.2 | 52; 50.2 ± 51.0 | 107; 76.7 ± 67.7 | <0.001 |
| Creatinine (µmol/L) | 55; 105.1 ± 95.5 | 52; 87.8 ± 38.4 | 107; 96.5 ± 73.3 | <0.001 |
| During the hospitalization | ||||
| Respiratory distress syndrome | <0.001 | |||
| No | 15 (26.8%) | 36 (69.2%) | 51 (47.2%) | |
| At admission | 31 (55.4%) | 11 (21.2%) | 42 (38.9%) | |
| During stay | 10 (17.9%) | 5 (9.6%) | 15 (13.9%) | |
| Transfer to intermediate care unit | 18 (34.6%) | 7 (13.5%) | 25 (24.0%) | 0.021 |
| Transfer to intensive care unit | 22 (39.3%) | 0 (0.0%) | 22 (20.4%) | <0.001 |
| Intra-hospital death | 7 (12.7%) | 6 (11.8%) | 13 (12.3%) | 1.000 |
| Number of days with fever | 54; 7.6 ± 8.7 | 51; 6.4 ± 9.9 | 105; 7.0 ± 9.3 | 0.029 |
| Number of days with O2 | 56; 11.4 ± 10.9 | 50; 8.9 ± 11.1 | 106; 10.2 ± 11.0 | <0.001 |
| C-reactive protein higher value (mg/L) | 55; 178.3 ± 113.9 | 43; 88.4 ± 63.9 | 98; 138.8 ± 104.9 | <0.001 |
| Length of hospital stay | 56; 18.2 ± 17.8 | 51; 31.5 ± 24.7 | 107; 24.5 ± 22.2 | <0.001 |
| WHO severity score | 0.001 | |||
| Asymptomatic | 0 (0.0%) | 2 (3.8%) | (1.9%) | |
| Mild disease | 5 (8.9%) | 11 (21.2%) | 16 (14.8%) | |
| Moderate disease | 10 (17.9%) | 16 (30.8%) | 26 (24.1%) | |
| Severe disease | 19 (33.9%) | 19 (36.5%) | 38 (35.2%) | |
| Critical disease | 22 (39.3%) | 4 (7.7%) | 26 (24.1%) |
| Coefficient (%) (IC 95%) | p-Value | |
|---|---|---|
| Elderly group | 6.49 (−6.49–19.48) | 0.327 |
| Dilution | ||
| 1/32 | 14.71 (10.99–18.44) | <0.001 |
| 1/128 | 39.42 (35.70–43.15) | <0.001 |
| 1/512 | 62.88 (59.16–66.61) | <0.001 |
| Group*dilution | ||
| Elderly-1/32 | 4.02 (−1.39–9.42) | 0.145 |
| Elderly-1/128 | 3.78 (−1.63–9.20) | 0.171 |
| Elderly-1/512 | 6.47 (1.06–11.87) | 0.019 |
| Bivariate Analysis | Multivariable Analysis | |||
|---|---|---|---|---|
| Coefficient (IC95%) | p-Value | Coefficient (IC95%) | p-Value | |
| Dilution | ||||
| 1/32 | 16.40 (13.68–19.12) | <0.001 | 16.40 (13.68–19.12) | <0.001 |
| 1/128 | 41.20 (38.49–43.91) | <0.001 | 40.98 (38.25–43.70) | <0.001 |
| 1/512 | 65.95 (63.25–68.66) | <0.001 | 66.02 (63.30–68.74) | <0.001 |
| Age (years) | 0.08 (−0.26–0.42) | 0.470 | −0.40 (−0.87–0.07) | 0.092 |
| Gender (male) | 8.25 (−4.66–21.16) | 0.210 | 2.20 (−10.76–15.16) | 0.740 |
| LOS | 0.11 (−0.17–0.40) | 0.436 | 0.06 (−0.26–0.38) | 0.711 |
| Delay PSO- antibody testing (d) | −2.41 (−3.64–−1.16) | <0.001 | −2.69 (−3.85–−1.53) | <0.001 |
| Arterial hypertension | −9.12 (−26.87–8.64) | 0.313 | −8.98 (−24.99–7.03) | 0.272 |
| Immunosuppression | 9.14 (−16.54–34.82) | 0.485 | 3.04 (−20.34–26.42) | 0.799 |
| Clinical Frailty Scale | 2.70 (−0.16–5.57) | 0.064 | 4.71 (0.34–9.10) | 0.035 |
| WHO severity score | −6.07 (−11.96–−0.18) | 0.043 | −6.01 (−11.97–−0.06) | 0.048 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malézieux-Picard, A.; Abdul, F.; Herrmann, F.R.; Caillon, A.; Ribaux, P.; Cambet, Y.; Yerly, S.; Baggio, S.; Vernaz, N.; Zekry, D.; et al. Decreased Levels of SARS-CoV-2 Fusion-Inhibitory Antibodies in the Serum of Aged COVID-19 Patients. Diagnostics 2022, 12, 1813. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12081813
Malézieux-Picard A, Abdul F, Herrmann FR, Caillon A, Ribaux P, Cambet Y, Yerly S, Baggio S, Vernaz N, Zekry D, et al. Decreased Levels of SARS-CoV-2 Fusion-Inhibitory Antibodies in the Serum of Aged COVID-19 Patients. Diagnostics. 2022; 12(8):1813. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12081813
Chicago/Turabian StyleMalézieux-Picard, Astrid, Fabien Abdul, François R. Herrmann, Aurélie Caillon, Pascale Ribaux, Yves Cambet, Sabine Yerly, Stéphanie Baggio, Nathalie Vernaz, Dina Zekry, and et al. 2022. "Decreased Levels of SARS-CoV-2 Fusion-Inhibitory Antibodies in the Serum of Aged COVID-19 Patients" Diagnostics 12, no. 8: 1813. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12081813