
Isolated Severe Dysphonia as a Presentation of Post-COVID-19 Syndrome

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Methods
2.3. Subjective Voice Assessment
2.4. Instrumental Voice Assessment
2.5. Treatment
3. Results
3.1. Patients’ Symptoms
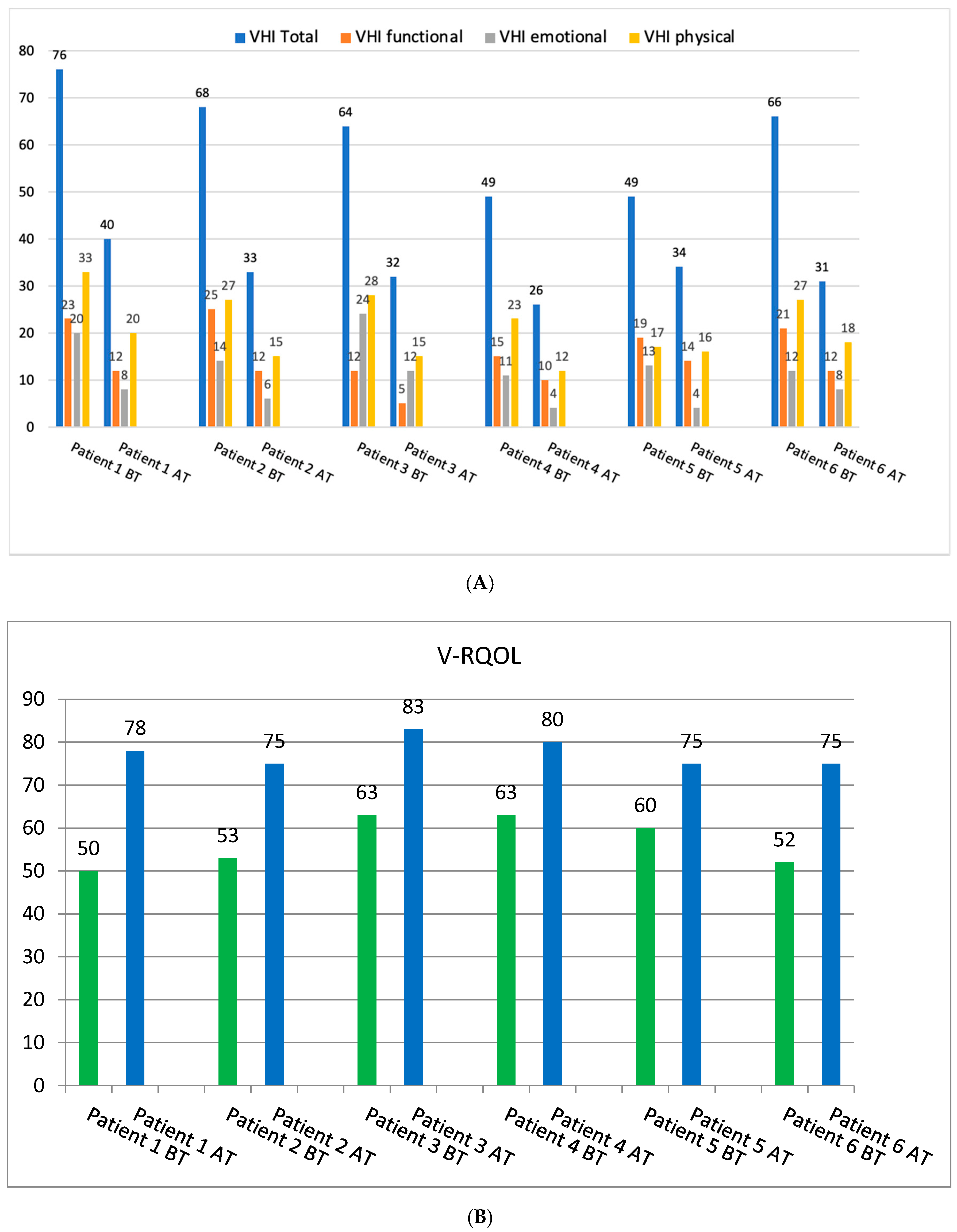
3.2. Subjective Voice Assessment
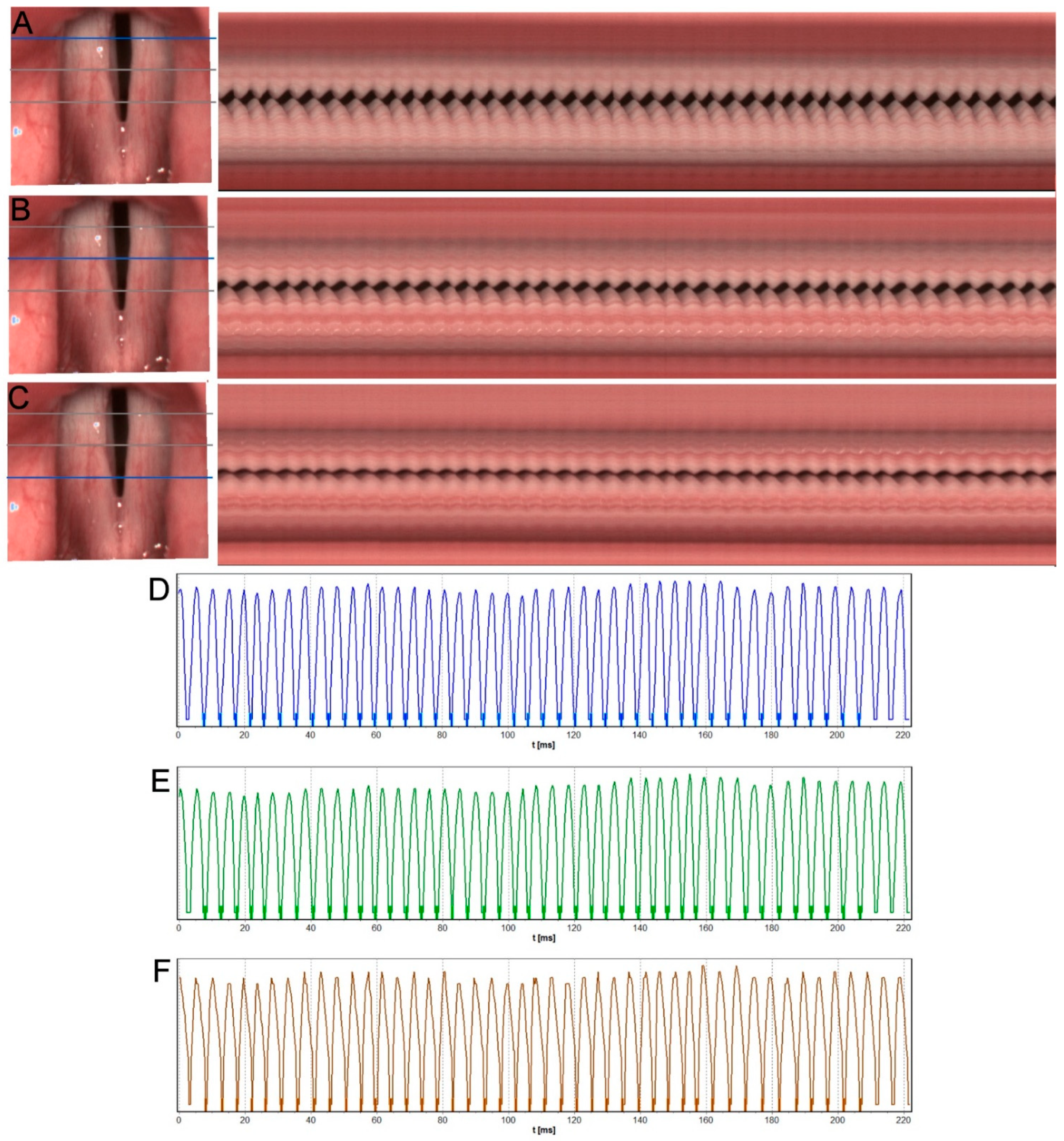
3.3. ENT Examination with Instrumental Assessment including VLS and HSV
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lechien, J.R.; Chiesa-Estomba, C.M.; Cabaraux, P.; Mat, Q.; Huet, K.; Harmegnies, B.; Horoi, M.; Le Bon, S.D.; Rodriguez, A.; Dequanter, D.; et al. Features of Mild-to-Moderate COVID-19 Patients with Dysphonia. J. Voice 2022, 36, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Elibol, E. Otolaryngological symptoms in COVID-19. Eur. Arch. Oto-Rhino-Laryngol. 2021, 278, 1233–1236. [Google Scholar] [CrossRef] [PubMed]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Tahir, E.; Kavaz, E.; Çengel Kurnaz, S.; Temoçin, F.; Atilla, A. Patient reported voice handicap and auditory-perceptual voice assessment outcomes in patients with COVID-19. Logop. Phoniatr. Vocology 2021, 15, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Saki, N.; Zamani, P.; Bayat, A.; Nikakhlagh, S.; Moghateli, N.; Salmanzadeh, S. Auditory-Perceptual Evaluation of Vocal Characteristics in Patients with the New Coronavirus Disease 2019. Folia Phoniatr. Logop. 2022, 74, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Singhal, T. A Review of Coronavirus Disease-2019 (COVID-19). Indian J. Pediatr. 2020, 87, 281–286. [Google Scholar] [CrossRef] [Green Version]
- Al-Ani, R.M.; Rashid, R.A. Prevalence of General and Otorhinolaryngological Symptoms Post-COVID-19 Regarding the Time of Presentation. Indian J. Otolaryngol. Head Neck Surg. 2021, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Organisation, W.H. A Clinical Case Definition of Post COVID-19 Condition by a Delphi Consensus (6 October 2021). Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Post_COVID-19_condition-Clinical_case_definition-2021.1 (accessed on 12 July 2022).
- Özçelik Korkmaz, M.; Eğilmez, O.K.; Özçelik, M.A.; Güven, M. Otolaryngological manifestations of hospitalised patients with confirmed COVID-19 infection. Eur. Arch. Oto-Rhino-Laryngol. 2021, 278, 1675–1685. [Google Scholar] [CrossRef] [PubMed]
- Cantarella, G.; Aldè, M.; Consonni, D.; Zuccotti, G.; Di Berardino, F.; Barozzi, S.; Bertoli, S.; Battezzati, A.; Zanetti, D.; Pignataro, L. Prevalence of Dysphonia in Non hospitalized Patients with COVID-19 in Lombardy, the Italian Epicenter of the Pandemic. J. Voice 2021, 2, 6–10. [Google Scholar] [CrossRef] [PubMed]
- Azzam, A.A.A.; Samy, A.; Sefein, I.; ElRouby, I. Vocal Disorders in Patients with COVID 19 in Egypt. Indian J. Otolaryngol. Head Neck Surg. 2021, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Zamzam, S.M.; Hanafy, R.G. Correction to: Impact of COVID-19 on vocal cord mobility: A case series study. Egypt. J. Otolaryngol. 2021, 37, 116. [Google Scholar] [CrossRef]
- Naunheim, M.R.; Zhou, A.S.; Puka, E.; Franco, R.A.; Carroll, T.L.; Teng, S.E.; Mallur, P.S.; Song, P.C. Laryngeal complications of COVID-19. Laryngoscope Investig. Otolaryngol. 2020, 5, 1117–1124. [Google Scholar] [CrossRef] [PubMed]
- Miles, A.; McRae, J.; Clunie, G.; Gillivan-Murphy, P.; Inamoto, Y.; Kalf, H.; Pillay, M.; Pownall, S.; Ratcliffe, P.; Richard, T.; et al. An International Commentary on Dysphagia and Dysphonia during the COVID-19 Pandemic. Dysphagia 2022, 1–26. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, B.H.; Benninger, M.S.; Newman, C.W.; Cleveland, T.; Foundation, C. The Voice Handicap Index (VHI): Development and Validation. Am. J. Speech-Lang. Pathol. 1997, 6, 66–70. [Google Scholar] [CrossRef]
- Hogikyan, N.D.; Sethuraman, G. Validation of an instrument to measure voice-related quality of life (V- RQOL). J. Voice 1999, 13, 557–569. [Google Scholar] [CrossRef]
- Pietruszewska, W.; Just, M.; Morawska, J.; Malinowski, J.; Hoffman, J.; Racino, A.; Barańska, M.; Kowalczyk, M.; Niebudek-Bogusz, E. Comparative analysis of high-speed videolaryngoscopy images and sound data simultaneously acquired from rigid and flexible laryngoscope: A pilot study. Sci. Rep. 2021, 11, 20480. [Google Scholar] [CrossRef] [PubMed]
- Sielska-Badurek, E.M.; Jędra, K.; Sobol, M.; Niemczyk, K.; Osuch-Wójcikiewicz, E. Laryngeal stroboscopy—Normative values for amplitude, open quotient, asymmetry and phase difference in young adults. Clin. Otolaryngol. 2019, 44, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Malinowski, J.; Niebudek-Bogusz, E.; Just, M.; Morawska, J.; Racino, A.; Hoffman, J.; Barańska, M.; Kowalczyk, M.; Pietruszewska, W. Laryngeal High-Speed Videoendoscopy with Laser Illumination: A Preliminary Report. Otolaryngol. Pol. 2021, 75, 1–10. [Google Scholar] [CrossRef]
- Leis-Cofiño, C.; Arriero-Sánchez, P.; González-Herranz, R.; Arenas-Brítez, Ó.; Hernández-García, E.; Plaza, G. Persistent Dysphonia in Hospitalized COVID-19 Patients. J. Voice 2021. [Google Scholar] [CrossRef]
- Aghaz, A.; Shahriyari, A.; Panahiaboozar, S.; Jadidi, H.; Khoshgoftar, M.; Choupani, E.; Hemmati, E. Prevalence of Dysphonia in Patients with COVID-19: A Systematic Review and Meta-Analysis. J. Mod. Rehabil. 2022, 16, 130–136. [Google Scholar] [CrossRef]
- Lechien, J.R.; Saussez, S.; Vaira, L.A.; Hans, S. Post-COVID-19 Dysphonia may have Several Origins. Indian J. Otolaryngol. Head Neck Surg. 2021, 2, 9–10. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, K.; Yan, Y.; Bless, D.M. Vocal fold vibratory characteristics in normal female speakers from high-speed digital imaging. J. Voice 2012, 26, 239–253. [Google Scholar] [CrossRef] [PubMed]
- Mohd Khairuddin, K.A.; Ahmad, K.; Mohd Ibrahim, H.; Yan, Y. Analysis Method for Laryngeal High-Speed Videoendoscopy: Development of the Criteria for the Measurement Input. J. Voice 2021, 35, 636–645. [Google Scholar] [CrossRef] [PubMed]
- Schlegel, P.; Stingl, M.; Kunduk, M.; Kniesburges, S.; Bohr, C.; Döllinger, M. Dependencies and Ill-designed Parameters Within High-speed Videoendoscopy and Acoustic Signal Analysis. J. Voice 2019, 33, 811.e1–811.e12. [Google Scholar] [CrossRef] [PubMed]
- Asiaee, M.; Vahedian-azimi, A.; Atashi, S.S.; Keramatfar, A.; Nourbakhsh, M. Voice Quality Evaluation in Patients with COVID-19: An Acoustic Analysis. J. Voice 2020. [Google Scholar] [CrossRef]
- Okba, N.M.A.; Müller, M.A.; Li, W.; Wang, C.; GeurtsvanKessel, C.H.; Corman, V.M.; Lamers, M.M.; Sikkema, R.S.; de Bruin, E.; Chandler, F.D.; et al. Severe Acute RespiratorySyndrome Coronavirus 2–Specific Antibody Responses in Coronavirus Disease Patients. Emerg. Infect. Dis. 2020, 26, 1478–1488. [Google Scholar] [CrossRef]
- Sato, K.; Sinclair, J.E.; Sadeghirad, H.; Fraser, J.F.; Short, K.R.; Kulasinghe, A. Cardiovascular disease in SARS-CoV-2 infection. Clin. Transl. Immunol. 2021, 10, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Li, L.; Zhang, Y.; Wang, X. An Investigation of the Expression of 2019 Novel Coronavirus Cell Receptor Gene ACE2 in a Wide Variety of Human Tissues. Infect. Dis. Poverty 2020, 9, 1–7. [Google Scholar]
- Schlegel, P.; Kunduk, M.; Stingl, M.; Semmler, M.; Döllinger, M.; Bohr, C.; Schützenberger, A. Influence of spatial camera resolution in highspeed videoendoscopy on laryngeal parameters. PLoS ONE 2019, 14, e0215168. [Google Scholar] [CrossRef] [PubMed]
- Maertens, K.; De Jong, F.I.C.R.S. The voice handicap index as a tool for assessment of the biopsychosocial impact of voice problems. B-ENT 2007, 3, 61–66. [Google Scholar] [PubMed]
- Buselli, R.; Corsi, M.; Necciari, G.; Pistolesi, P.; Baldanzi, S.; Chiumiento, M.; Del Lupo, E.; Del Guerra, P.; Cristaudo, A. Sudden and persistent dysphonia within the framework of COVID-19: The case report of a nurse. Brain Behav. Immun.-Health 2020, 9, 100160. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | BR Subject 1 | KU Subject 2 | KM Subject 3 | MT Subject 4 | NM Subject 5 | OM Subject 6 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post | |
| F0Avg [Hz] | 183.5 | 150 | 245.7 | 212 | 335.1 | 536.1 | 427.8 | 286.8 | 295.7 | 215.5 | 280.9 | 323.5 |
| PPF [%] | 4.13 | 4.1 | 1.18 | 4.86 | 0.63 | 5.29 | 7.56 | 0.31 | 3.92 | 1.76 | 1.88 | 2.02 |
| Jitt [%] | 4.14 | 3.96 | 1.18 | 4.73 | 0.63 | 5.08 | 7.37 | 0.31 | 3.77 | 1.68 | 1.88 | 2.03 |
| APF [%] | 4.05 | 1.96 | 9.54 | 3.96 | 6.58 | 3.5 | 26.93 | 1.64 | 1.27 | 3.41 | 2.92 | 2.04 |
| Shimmer [%] | 4.11 | 1.94 | 8.87 | 4 | 6.49 | 3.55 | 19.29 | 1.64 | 1.27 | 3.44 | 2.94 | 2.04 |
| PPQ3 [%] | 2.22 | 2.48 | 0.5 | 2.61 | 0.35 | 3.08 | 3.79 | 0.17 | 2.19 | 0.92 | 1.19 | 1.25 |
| APQ3 [%] | 2.19 | 1.15 | 2.4 | 1.97 | 4.25 | 2.04 | 10.41 | 0.93 | 0.5 | 2.11 | 1.41 | 1.17 |
| AmpAvg [%FL] | 8.6 | 8.2 | 5.7 | 4.1 | 6.7 | 3.8 | 3.8 | 4.5 | 3.8 | 4 | 6.1 | 8.4 |
| AmpAvg 2/3 [%FL] | 8.3 | 11.4 | 6 | 3.4 | 8.5 | 4.6 | 3.5 | 5 | 4.1 | 5.5 | 6.6 | 9.6 |
| RGGA [%] | 0 | 0 | 10.7 | 0 | 5.9 | 33.7 | 0 | 11.3 | 0 | 1.9 | 0 | 0 |
| OQAvg [%] | 57.8 | 53.9 | 73.6 | 53.2 | 86.1 | 99.5 | 49 | 89.7 | 55.7 | 35.8 | 65.4 | 58.5 |
| AmplAsymAvg [%] | 13.1 | 12.2 | 21.7 | 6.8 | 7.3 | 10.7 | 19.2 | 5 | 9.8 | 17.4 | 19.9 | 6.4 |
| AmplAsym Avg_2/3 [%] | 16.3 | 10.5 | 14.5 | 4.8 | 7.1 | 6.6 | 18.5 | 5.5 | 7 | 15.1 | 19.3 | 6.3 |
| AbsPhase DiffAvg [°] | 34.3 | 49 | 115.1 | 96.2 | 28.9 | 24 | 107 | 71.8 | 56.4 | 53.6 | 29.3 | 34.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeleniewska, J.; Niebudek-Bogusz, E.; Malinowski, J.; Morawska, J.; Miłkowska-Dymanowska, J.; Pietruszewska, W. Isolated Severe Dysphonia as a Presentation of Post-COVID-19 Syndrome. Diagnostics 2022, 12, 1839. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12081839
Jeleniewska J, Niebudek-Bogusz E, Malinowski J, Morawska J, Miłkowska-Dymanowska J, Pietruszewska W. Isolated Severe Dysphonia as a Presentation of Post-COVID-19 Syndrome. Diagnostics. 2022; 12(8):1839. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12081839
Chicago/Turabian StyleJeleniewska, Joanna, Ewa Niebudek-Bogusz, Jakub Malinowski, Joanna Morawska, Joanna Miłkowska-Dymanowska, and Wioletta Pietruszewska. 2022. "Isolated Severe Dysphonia as a Presentation of Post-COVID-19 Syndrome" Diagnostics 12, no. 8: 1839. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12081839