
Artificial Intelligence Based Pain Assessment Technology in Clinical Application of Real-World Neonatal Blood Sampling

 ,
, 
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
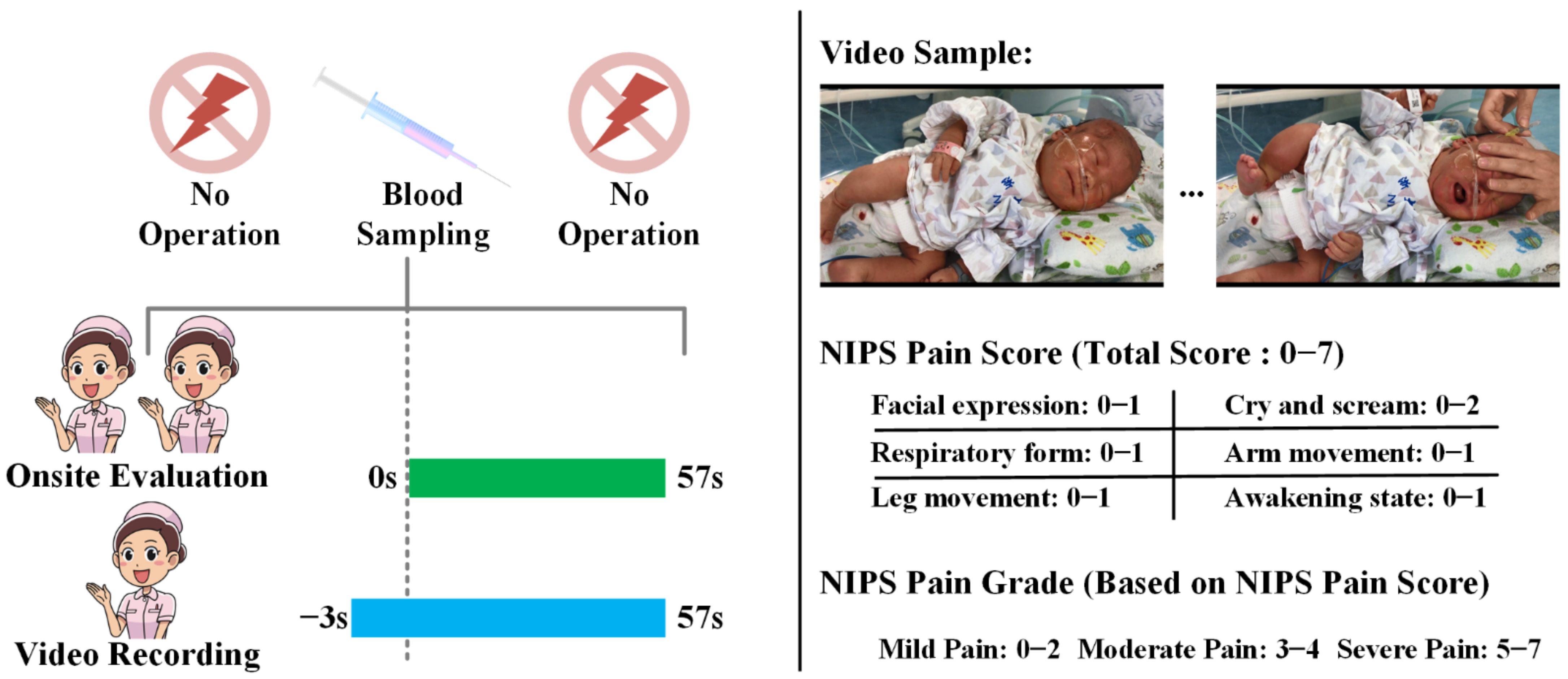
2.1. Study Design
2.2. Inclusion and Exclusion Criteria
2.3. OS-NPA Performed by Nurses
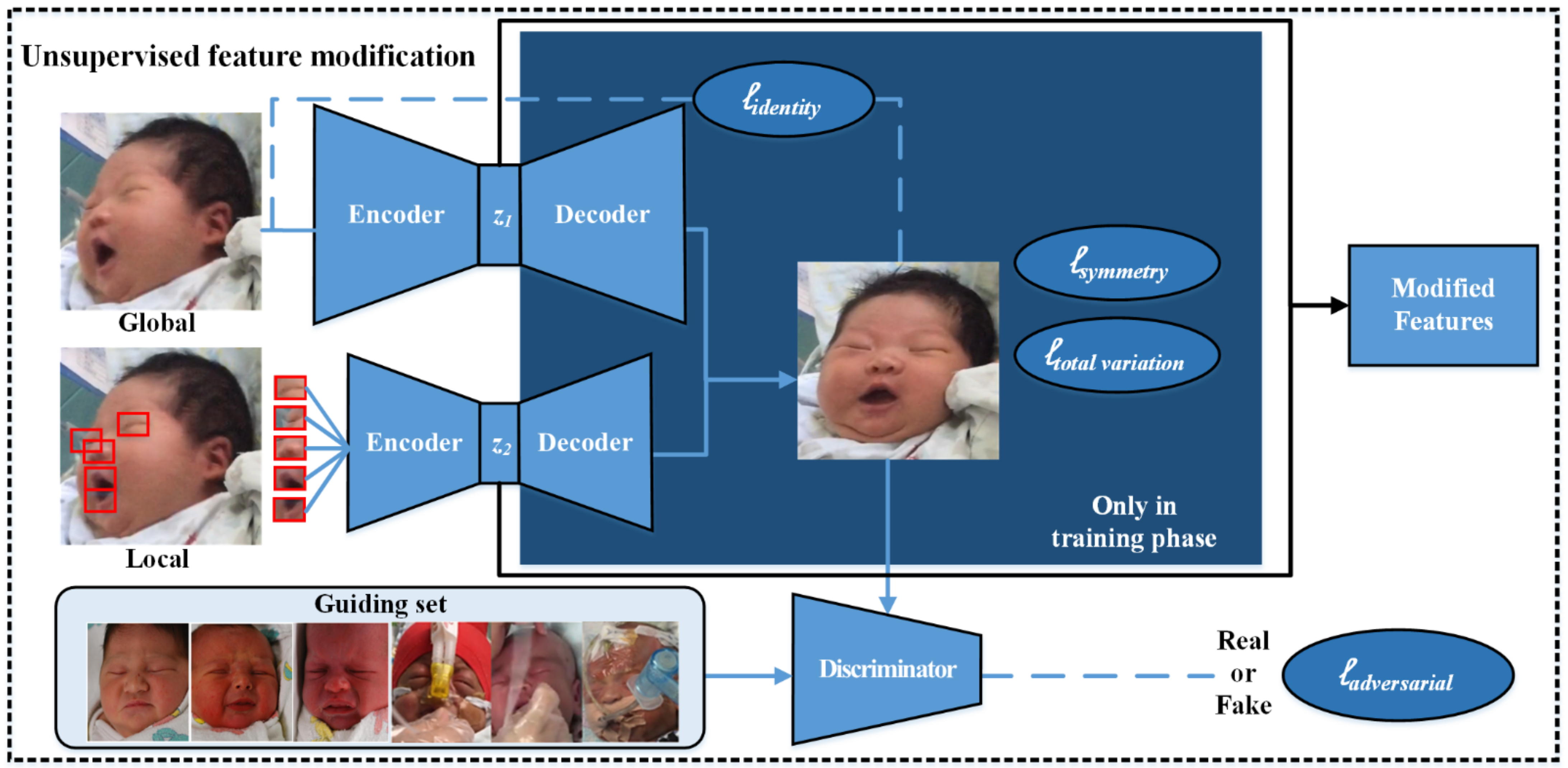
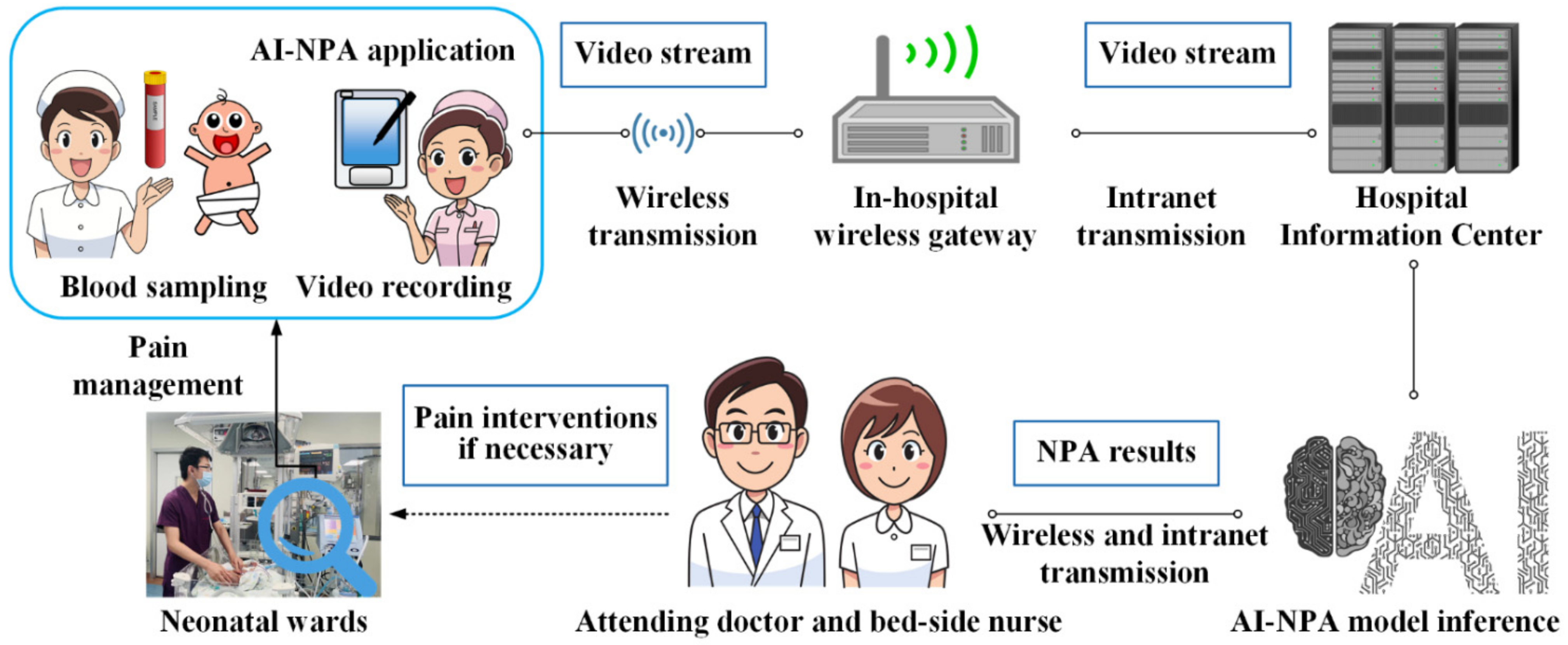
2.4. AI-NPA Performed by the Automated NPA System
2.5. Statistical Analysis
3. Results
3.1. Study Population
3.2. Comparison of NIPS Pain Scores between OS-NPA and AI-NPA
3.3. Comparison of the NIPS Pain Grades between OS-NPA and AI-NPA
4. Discussion
4.1. High Evaluation Consistency of the Automated NPA System
4.2. AI-NPA of Severe Pain
4.3. Strengths and Limitations of the Automated AI-NPA System
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kaur, H.; Mahajan, G. A comprehensive analysis of neonatal pain and measures to reduce pain. J. Pediatric Crit. Care 2019, 6, 43–48. [Google Scholar] [CrossRef]
- Boyle, E.M.; Bradshaw, J.; Blake, K.I. Persistent pain in neonates: Challenges in assessment without the aid of a clinical tool. Acta Paediatr. 2018, 107, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Wan, Y. The Occurrent Status and Influencing Factors of Neonatal Procedural Pain in Neonatal Intensive Care Unit; Chinese Academy of Medical Sciences & Peking Union Medical College: Beijing, China, 2017. [Google Scholar]
- Anand, K.J.; Eriksson, M.; Boyle, E.M.; Avila-Alvarez, A.; Andersen, R.D.; Sarafidis, K.; Polkki, T.; Matos, C.; Lago, P.; Papadouri, T.; et al. Assessment of continuous pain in newborns admitted to NICUs in 18 European countries. Acta Paediatr. 2017, 106, 1248–1259. [Google Scholar] [CrossRef] [Green Version]
- Relland, L.M.; Gehred, A.; Maitre, N.L. Behavioral and physiological signs for pain assessment in preterm and term neonates during a nociception-specific response: A systematic review. Pediatric Neurol. 2019, 90, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Walker, S.M. Translational studies identify long-term impact of prior neonatal pain experience. Pain 2017, 158, S29–S42. [Google Scholar] [CrossRef]
- Grunau, R.E.; Oberlander, T.; Holsti, L.; Whitfield, M.F. Bedside application of the neonatal facial coding system in pain assessment of premature infants. Pain 1998, 76, 277–286. [Google Scholar] [CrossRef]
- Büttner, W.; Finke, W. Analysis of behavioural and physiological parameters for the assessment of postoperative analgesic demand in newborns, infants and young children: A comprehensive report on seven consecutive studies. Pediatric Anesth. 2000, 90, 13–23. [Google Scholar] [CrossRef]
- Stevens, B.; Johnston, C.; Petryshen, P.; Taddio, A. Premature infant pain profile: Development and initial validation. Clin. J. Pain 1996, 12, 13–22. [Google Scholar] [CrossRef]
- Lawrence, J.; Alcock, D.; McGrath, P.; Kay, J.; MacMurray, S.B.; Dulberg, C. The development of a tool to assess neonatal pain. Neonatal Netw. 1993, 12, 59–66. [Google Scholar] [CrossRef]
- Cong, X.; McGrath, J.M.; Delaney, C.; Liang, S.; Vazquez, V.; Keating, L.; Chang, K.; Dejong, A. Neonatal nurses’ perceptions of pain management: Survey of the United States and China. Pain Manag. Nurs. 2014, 15, 834–844. [Google Scholar] [CrossRef]
- Guinsburg, R.; de Araújo Peres, C.; de Almeida, M.F.B.; Balda, R.D.C.X.; Berenguel, R.C.; Tonelotto, J.; Kopelman, B.I. Differences in pain expression between male and female newborn infants. Pain 2000, 85, 127–133. [Google Scholar] [CrossRef]
- Zamzmi, G.; Kasturi, R.; Goldgof, D.; Zhi, R.; Ashmeade, T.; Sun, Y. A review of automated pain assessment in infants: Features, classification tasks, and databases. IEEE Rev. Biomed. Eng. 2017, 11, 77–96. [Google Scholar] [CrossRef] [PubMed]
- Gholami, B.; Haddad, W.M.; Tannenbaum, A.R. Relevance vector machine learning for neonate pain intensity assessment using digital imaging. IEEE Trans. Biomed. Eng. 2010, 57, 1457–1466. [Google Scholar] [CrossRef] [Green Version]
- Brahnam, S.; Nanni, L.; Sexton, R. Introduction to neonatal facial pain detection using common and advanced face classification techniques. In Advanced Computational Intelligence Paradigms in Healthcare; Springer: Berlin/Heidelberg, Germany, 2007; pp. 225–253. [Google Scholar] [CrossRef]
- Lu, G.; Li, X.; Li, H. Research on recognition for facial expression of pain in neonates. Acta Opt. Sin. 2008, 28, 2109. [Google Scholar]
- Brahnam, S.; Nanni, L.; McMurtrey, S.; Lumini, A.; Brattin, R.; Slack, M.; Barrier, T. Neonatal pain detection in videos using the iCOPEvid dataset and an ensemble of descriptors extracted from Gaussian of Local Descriptors. Appl. Comput. Inform. 2019, in press. [Google Scholar] [CrossRef]
- Egede, J.; Valstar, M.; Torres, M.T.; Sharkey, D. Automatic neonatal pain estimation: An acute pain in neonates database. In Proceedings of the 2019 8th International Conference on Affective Computing and Intelligent Interaction, Cambridge, UK, 3–6 September 2019. [Google Scholar] [CrossRef]
- Zamzmi, G.; Paul, R.; Salekin, M.S.; Goldgof, D.; Kasturi, R.; Ho, T.; Sun, Y. Convolutional neural networks for neonatal pain assessment. IEEE Trans. Biom. Behav. Identity Sci. 2019, 1, 192–200. [Google Scholar] [CrossRef]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016. [Google Scholar] [CrossRef] [Green Version]
- Huang, G.; Liu, Z.; van der Maaten, L.; Weinberger, K.Q. Densely connected convolutional networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 22–25 July 2017. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y.; Hu, J.; Wang, W.; He, M.; de With, P.H.N. Camera-based discomfort detection using multi-channel attention 3D-CNN for hospitalized infants. Quant. Imaging Med. Surg. 2011, 11, 3059. [Google Scholar] [CrossRef]
- Chen, S.; Luo, F.; Chen, X.; Yan, J.; Zhong, Y.; Pan, Y. A video database of neonatal facial expression based on painful clinical procedures. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Berlin, Germany, 23–27 July 2019. [Google Scholar] [CrossRef]
- Huang, R.; Zhang, S.; Li, T.; He, R. Beyond face rotation: Global and local perception GAN for photorealistic and identity preserving frontal view synthesis. In Proceedings of the IEEE International Conference on Computer Vision, Venice, Italy, 22–29 October 2017. [Google Scholar] [CrossRef] [Green Version]
- Wang, F.; Jiang, M.; Qian, C.; Yang, S.; Li, C.; Zhang, H.; Wang, X.; Tang, X. Residual attention network for image classification. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 22–25 July 2017. [Google Scholar] [CrossRef] [Green Version]
- Li, S.; Deng, W. Reliable crowdsourcing and deep locality-preserving learning for unconstrained facial expression recognition. IEEE Trans. Image Process. 2018, 28, 356–370. [Google Scholar] [CrossRef]
- Witt, N.; Coynor, S.; Edwards, C.; Bradshaw, H. A guide to pain assessment and management in the neonate. Curr. Emerg. Hosp. Med. Rep. 2016, 4, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Grunau, R.; Craig, K. Pain expression in neonates: Facial action and cry. Pain 1987, 28, 395–410. [Google Scholar] [CrossRef]
- Peters, J.; Koot, H.; Grunau, R.; de Boer, J.; van Druenen, M.; Tibboel, D.; Duivenvoorden, H. Neonatal facial coding system for assessing postoperative pain in infants: Item reduction is valid and feasible. Clin. J. Pain 2003, 19, 353–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zamzmi, G.; Pai, C.; Goldgof, D.; Kasturi, R.; Sun, Y.; Ashmeade, T. Automated pain assessment in neonates. In Proceedings of the 20th Scandinavian Conference on Image Analysis, Tromsø, Norway, 12–14 June 2017. [Google Scholar] [CrossRef]
- Zamzmi, G.; Pai, C.; Goldgof, D.; Kasturi, R.; Ashmeade, T.; Sun, Y. A comprehensive and context-sensitive neonatal pain assessment using computer vision. IEEE Trans. Affect. Comput. 2019, 13, 28–45. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Metrics | Number of Cases | Composition Ratio (%) | |
|---|---|---|---|
| Sex | Male | 86 | 37.07 |
| Female | 146 | 62.93 | |
| Delivery mode | Spontaneous delivery | 95 | 41.13 |
| Cesarean section | 136 | 58.87 | |
| Main diagnosis | Respiratory disorders | 113 | 48.71 |
| Digestive disorders | 63 | 27.15 | |
| Nervous-system disorders | 22 | 9.48 | |
| Infection disease | 34 | 14.66 | |
| Operation type | Venous blood sampling | 36 | 15.52 |
| Arterial blood sampling | 75 | 32.33 | |
| Heel blood sampling | 75 | 32.33 | |
| Fingertip blood sampling | 46 | 19.82 | |
| OS-NPA | AI-NPA Given by the Automated NPA System | |||||||
|---|---|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | |
| 0 | 5 | 1 | 0 | 0 | 0 | 0 | 0 | 0 |
| 1 | 1 | 5 | 0 | 0 | 0 | 0 | 0 | 0 |
| 2 | 0 | 0 | 13 | 1 | 0 | 1 | 0 | 0 |
| 3 | 0 | 0 | 0 | 15 | 1 | 1 | 1 | 0 |
| 4 | 0 | 0 | 1 | 1 | 21 | 4 | 2 | 0 |
| 5 | 0 | 0 | 0 | 0 | 0 | 37 | 2 | 4 |
| 6 | 0 | 0 | 0 | 0 | 0 | 2 | 47 | 2 |
| 7 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 63 |
| OS-NPA | AI-NPA | Kappa Value and 95%CI | p Value | ||
|---|---|---|---|---|---|
| Mild | Moderate | Severe | |||
| Mild | 25 | 1 | 1 | 0.90 [0.84, 0.96] | < 0.001 |
| Moderate | 1 | 38 | 8 | ||
| Severe | 0 | 0 | 158 | ||
| Operation Type | Number of Subjects with Severe Pain (Proportion %) | Kappa Value and 95% CI | AUC and 95% CI | p Value | |
|---|---|---|---|---|---|
| OS-NPA | AI-NPA | ||||
| Venous blood sampling | 32 (88.8) | 32 (88.8) | 1.00 [1.00, 1.00] | 1.000 [1.000, 1.000] | <0.001 |
| Arterial blood sampling | 57 (76.0) | 60 (80.0) | 0.88 [0.76, 1.00] | 0.967 [0.924, 1.000] | <0.001 |
| Heel blood sampling | 43 (57.3) | 46 (61.3) | 0.92 [0.83, 1.00] | 0.984 [0.959, 1.000] | <0.001 |
| Fingertip blood sampling | 26 (56.5) | 29 (63.3) | 0.86 [0.72, 1.00] | 0.957 [0.899, 1.000] | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, X.; Zhu, H.; Mei, L.; Luo, F.; Chen, X.; Zhao, Y.; Chen, S.; Pan, Y. Artificial Intelligence Based Pain Assessment Technology in Clinical Application of Real-World Neonatal Blood Sampling. Diagnostics 2022, 12, 1831. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12081831
Cheng X, Zhu H, Mei L, Luo F, Chen X, Zhao Y, Chen S, Pan Y. Artificial Intelligence Based Pain Assessment Technology in Clinical Application of Real-World Neonatal Blood Sampling. Diagnostics. 2022; 12(8):1831. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12081831
Chicago/Turabian StyleCheng, Xiaoying, Huaiyu Zhu, Linli Mei, Feixiang Luo, Xiaofei Chen, Yisheng Zhao, Shuohui Chen, and Yun Pan. 2022. "Artificial Intelligence Based Pain Assessment Technology in Clinical Application of Real-World Neonatal Blood Sampling" Diagnostics 12, no. 8: 1831. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12081831