
Thin Layer Immunoassay: An Economical Approach to Diagnose Helicobacter pylori Infection in Gastroduodenal Ulcer Disease Patients of Pakistan, a Comparative Analysis
Abstract
:1. Introduction
2. Materials and Methods
2.1. Collection, Transport and Processing of Clinical Samples
2.2. Preparation of H. pylori Sonicate Whole Cell Antigen
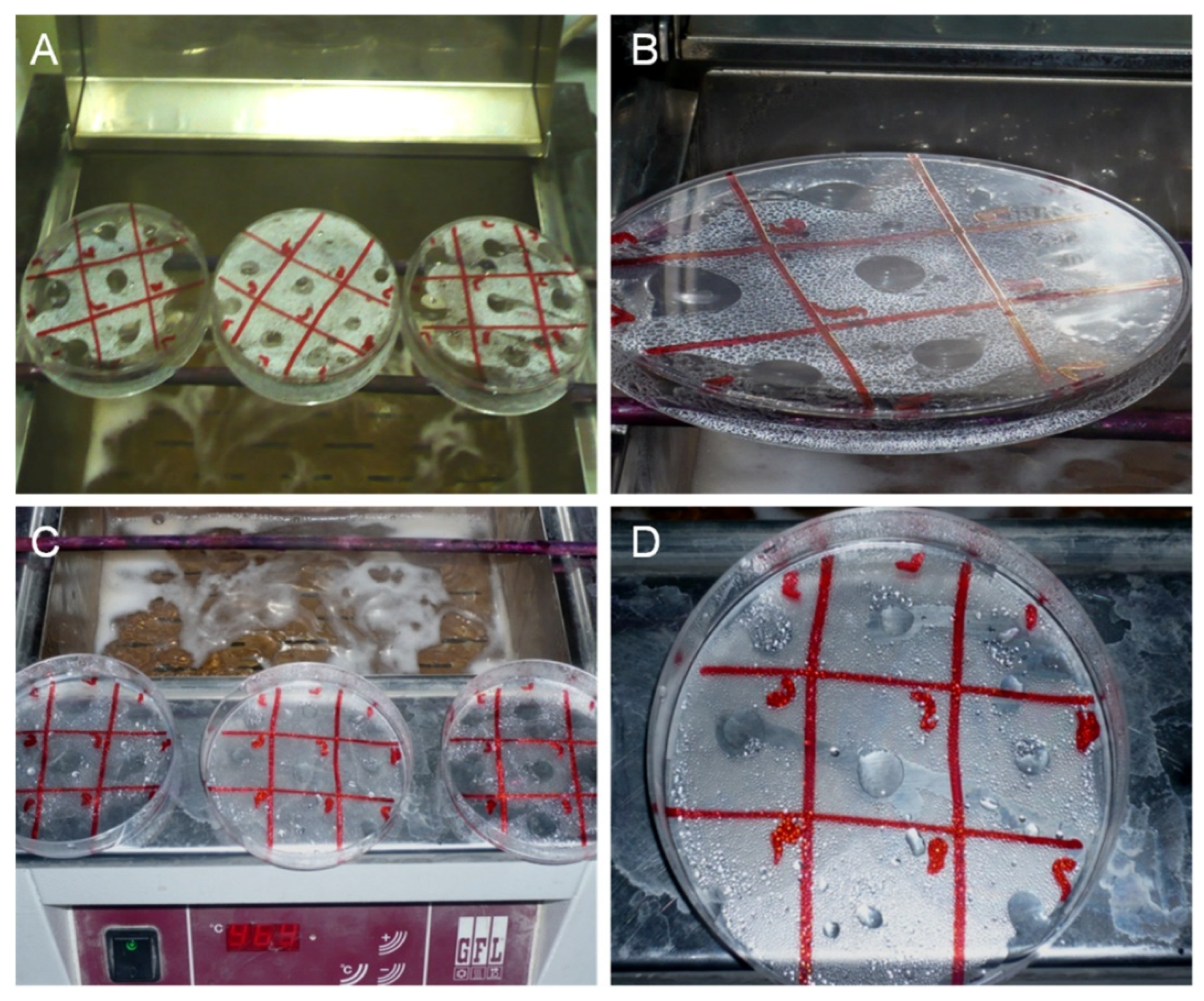
2.3. Thin Layer Immunoassay
2.4. Confirmation of Antigen/Antibody Reaction
2.5. Anti-H. pylori IgG and IgM Titer by Commercial ELISA Kit (kELISA)
2.6. Statistical Analysis
2.7. Ethical Clearance
3. Results
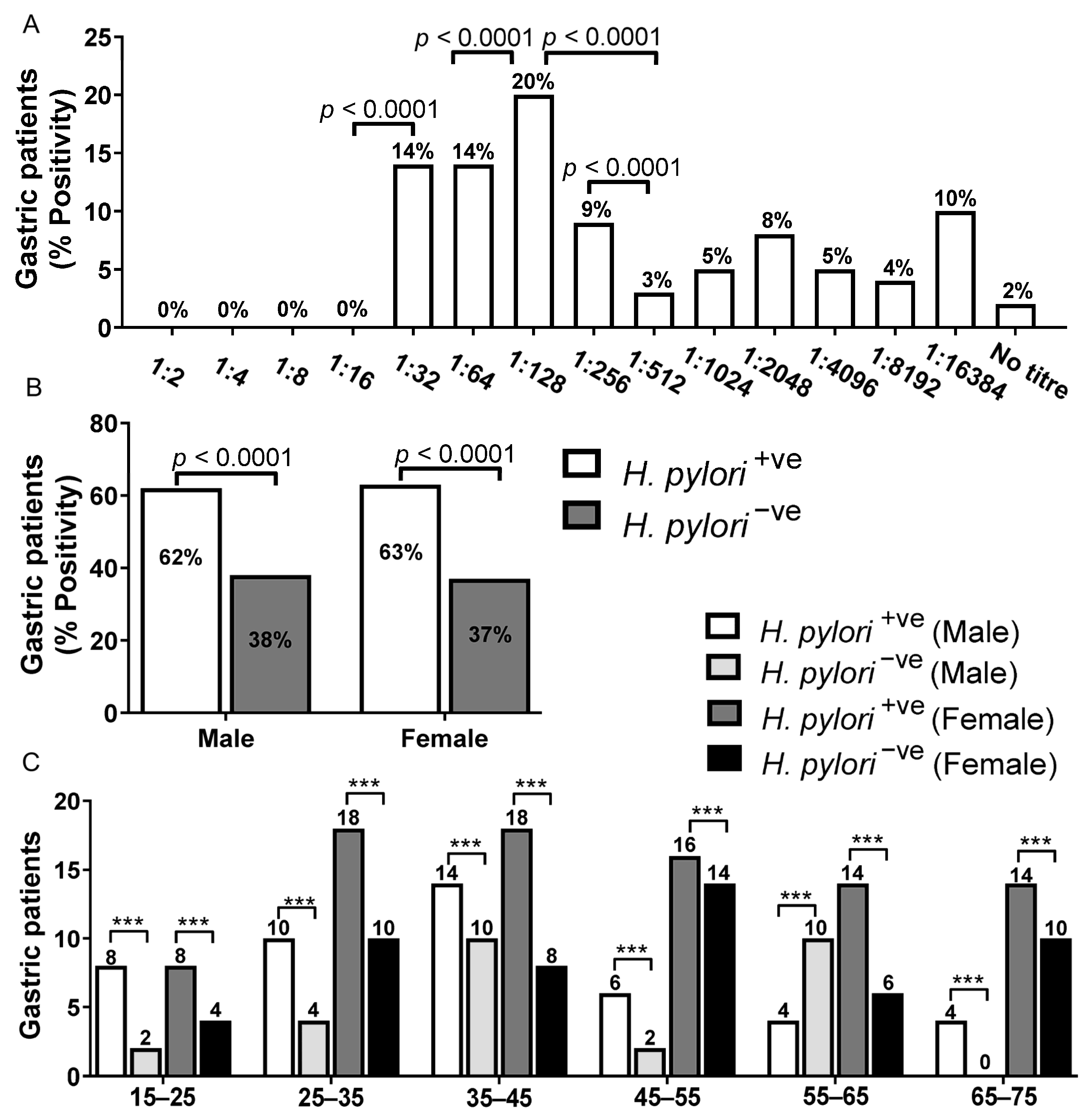
3.1. Analysis of H. pylori Titer by Thin Layer Immunoassay
3.2. Age and Sex Distribution of Gastritis and Gastroduodenal Ulcer Patients by Thin Layer Immunoassay
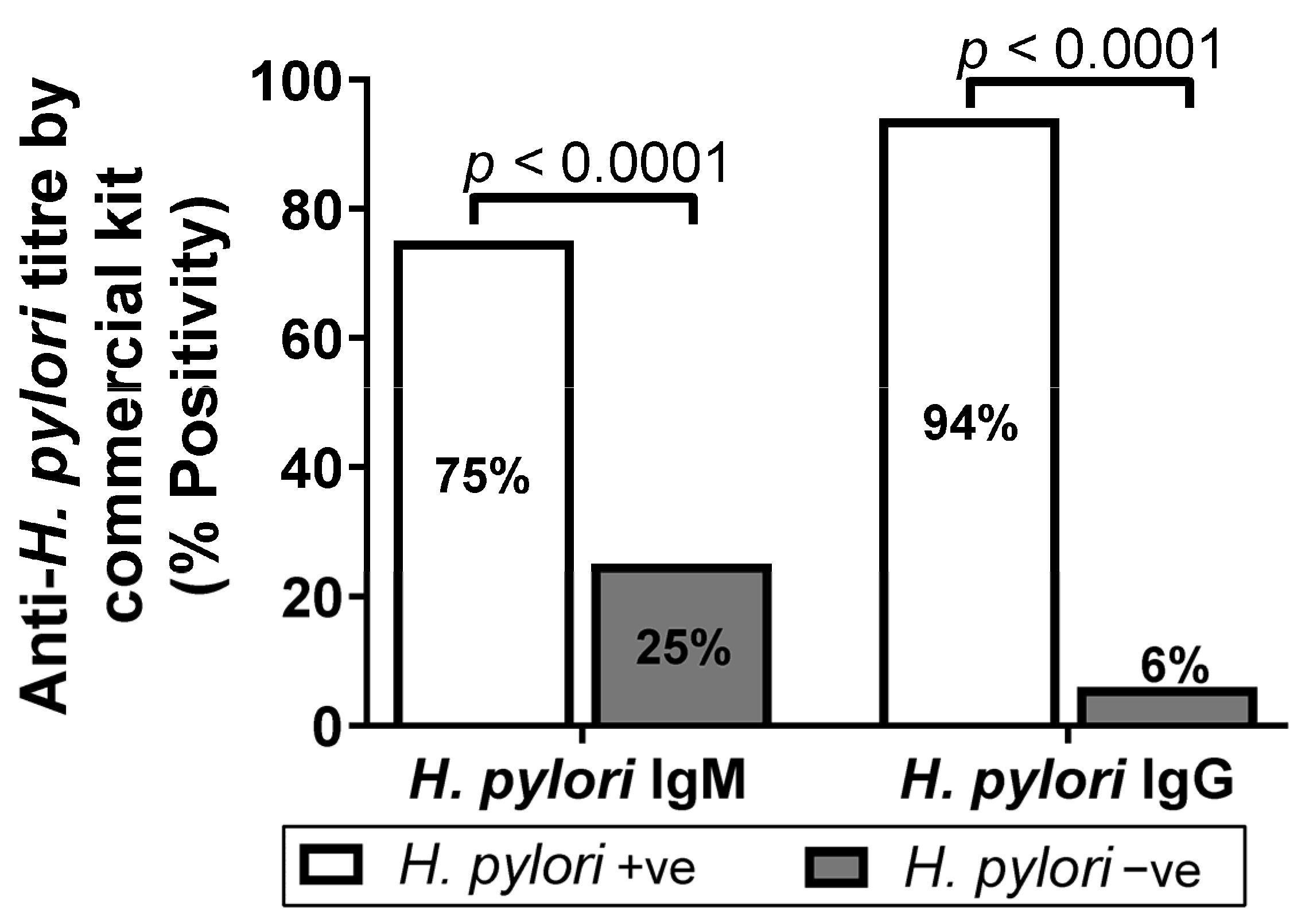
3.3. Analysis of Anti-H. pylori IgM and IgG Titer by Commercial Kit ELISA (kELISA)
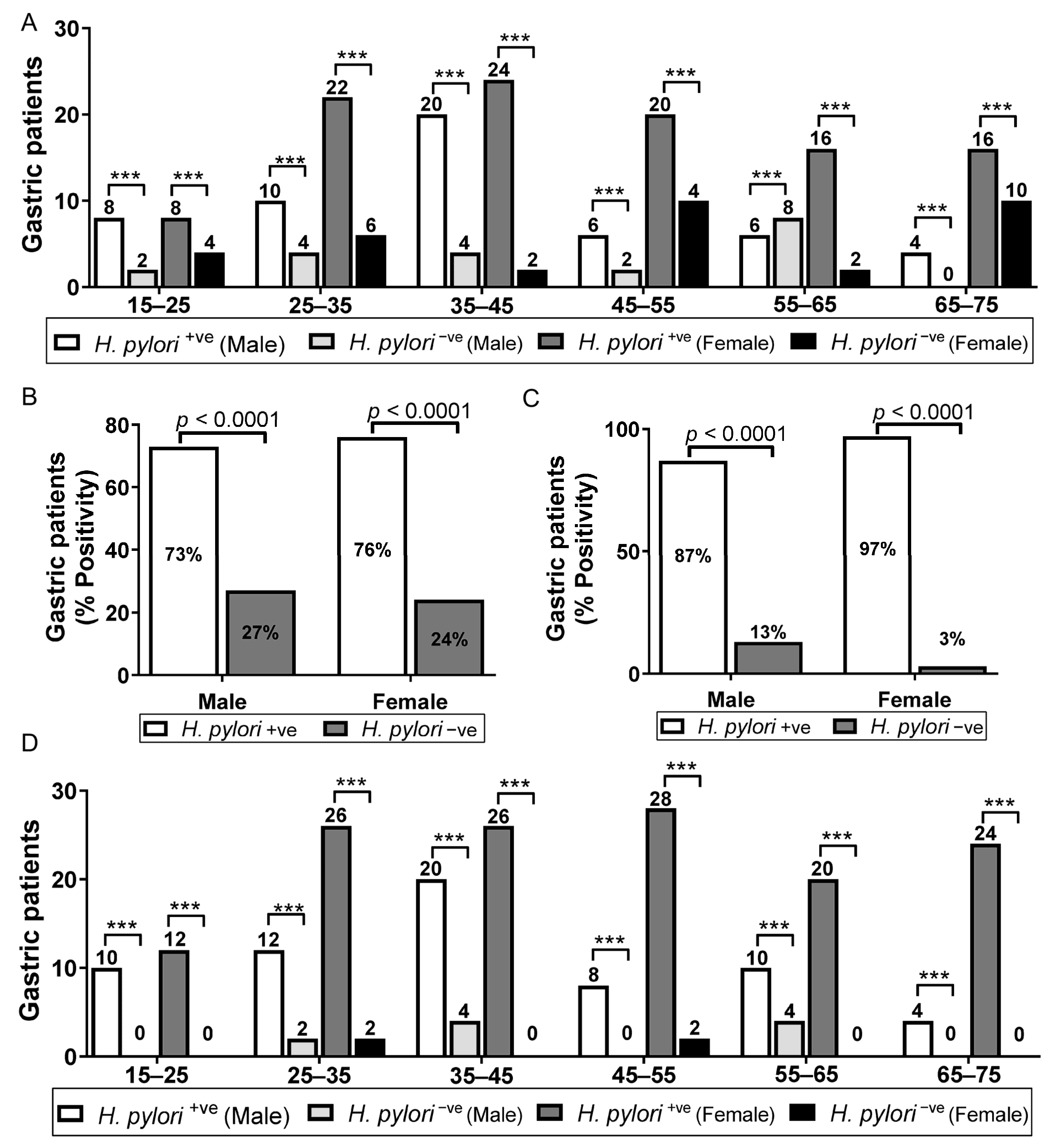
3.4. Age- and Sex-Wise Distribution of Gastric Patients IgM and IgG Titer by Commercial Kit ELISA (kMELISA and kGELISA)
3.5. Evaluation of TLI with Other Serological Assays
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ELISA | Enzyme-linked immunosorbent assay |
| H. pylori | Helicobacter pylori |
| kELISA | ELISA commercial kit |
| OD | Optical density |
| wELISA | In-house ELISA based on H. pylori surface whole cell antigen |
| sELISA | In-house ELISA based on H. pylori sonicate whole cell antigen |
References
- Bühling, F.; Koch, G.; Wex, T.; Heimburg, A.; Vieth, M.; Leodolter, A.; Roessner, A.; Ansorge, S.; Malfertheiner, P. Simultaneous detection and differentiation of anti-Helicobacter pylori antibodies by flow microparticle immunofluorescence assay. Clin. Diagn. Lab. Immunol. 2004, 11, 131–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Algood, H.M.; Cover, T.L. Helicobacter pylori persistence: An overview of interactions between H. pylori and host immune defenses. Clin. Microbiol. Rev. 2006, 19, 597–613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faisal, A.; Yang, X.; Wen, Q.; Yan, Q. A method for establishing human primary gastric epithelial cells culture from gastric tissue with continuous trace medium. Mol. Med. Rep. 2015, 12, 2939–2944. [Google Scholar]
- Faisal, A.; Gao, W.; Qiu, Y. Fucosyltransferase-4 and Oligosaccharide LewisY Antigen as potentially Correlative Biomarkers of H. pylori CagA Associated Gastric Cancer. Pathol. Oncol. Res. 2017, 23, 179. [Google Scholar]
- Faisal, A.; Yan, Q. Ginsenoside Rg3 induces FUT4-mediated apoptosis in H. pylori CagA-treated gastric cancer cells by regulating SP1 and HSF1 expressions. Toxicol. In-Vitro 2016, 31, 158–166. [Google Scholar]
- Faisal, A.; Yang, X.; Wang, X.; Yan, Q. Anti-LeY antibody enhances celecoxib efficacy to treat gastric cancer through downregulation of MAPK/COX-2 signaling pathway, correlation with clinical study. J. Cancer Res. Clin. Oncol. 2015, 141, 1221–1235. [Google Scholar]
- Faisal, A.; Yan, Q. The role of anti-LeY antibody in the downregulation of MAPKs/COX-2 pathway in gastric cancer. Curr. Drug. Targets 2014, 15, 469–476. [Google Scholar]
- Faisal, A.; Imran K and Shruti, S. Partners in crime: The Lewis Y antigen and fucosyltransferase IV in Helicobacter pylori-induced gastric cancer. Pharmacol. Ther. 2021, 24, 107994. [Google Scholar]
- Ghose, C.; Perez-Perez, G.I.; Torres, V.J.; Crosatti, M.; Nomura, A.; Peek, R.M., Jr.; Cover, T.L.; Francois, F.; Blaser, M.J. Serological assays for identification of human gastric colonization by Helicobacter pylori strains expressing VacA m1 or m2. Clin. Vaccine Immunol. 2007, 14, 442–450. [Google Scholar] [CrossRef] [Green Version]
- Bielanski, M.P.; Konturek, W.S.J.; Targosz, A.; Sliwowski, Z.; Dobrzanska, M.; Kaminska, A.; Sito, E.; Konturek, P.C.; Brzozowski, T. Helicobacter pylori infection and serum gastrin, ghrelin and leptin in children of Polish shepherds. Dig. Liner Dis. 2006, 38, 91–97. [Google Scholar]
- Amjad, M. Diagnosis, Immune Response and Role of Cytokines in Helicobacter pylori Associated Gastroduodenal Ulcer Disease; IIDRL, Department of Microbiology, University of Karachi: Karachi, Pakistan, 1997. [Google Scholar]
- Faisal, A.; Li, X.; Chakraborty, A.; Zheng, Y.; Xin, M.; Liu, K.; Dong, Z. Ubiquitination of ADRα1d/SerpinA1 complex stimulates hypoxia to induce gastric tumorigenesis with a combination of Helicobacter pylori and chronic stress through IL-1α. Gastric Cancer 2022, 25, 4. [Google Scholar]
- Faisal, A.; Abhijit, C.; Zigang, D. Gastric tumorigenesis induced by Helicobacter pylori infection and chronic alcohol consumption in mice through IL-10 inhibition. Carcinogenesis 2021, 2021, bgab114. [Google Scholar]
- Faisal, A.; Xin, M.; Gao, Y.; Monts, J.; Monson, K.; Wang, Q.; Bode, A.M.; Dong, Z. Induction and prevention of gastric cancer with combined Helicobacter pylori and capsaicin administration and DFMO treatment, respectively. Cancers 2020, 12, 4. [Google Scholar]
- Czinn, S.J. Helicobacter pylori infection: Detection, investigation, and management. J. Pediatrics 2005, 146.3, S21–S26. [Google Scholar] [CrossRef] [PubMed]
- Suerbaum, S.; Michetti, P. Helicobacter pylori infection. N. Engl. J. Med. 2002, 34711, 75–86. [Google Scholar]
- Torres, J.; Leal-Herrera, Y.; Perez-Perez, G.; Gomez, A.; Camorlinga-Ponce, M.; Cedillo-Rivera, R.; Tapia-Conyer, R.; Muñoz, O. A community-based seroepidemiologic study of Helicobacter pylori infection in Mexico. J. Infect. Dis. 1998, 178, 1089–1094. [Google Scholar] [CrossRef] [Green Version]
- Faisal, A.; Chen, X.; Yang, X.; Yan, Q. Prevalence and correlation with clinical diseases of Helicobacter pylori cagA and vacA genotype among gastric patients from Northeast China. Biomed. Res. Int. 2014, 2014, 142980. [Google Scholar]
- Dehesa, M.; Dooley, C.P.; Cohen, H.; Fitzgibbons, P.L.; Perez-Perez, G.I.; Blaser, M.J. High prevalence of Helicobacter pylori infection and histologic gastritis in asymptomatic Hispanics. J. Clin. Microbiol. 1991, 29, 1128–1131. [Google Scholar] [CrossRef] [Green Version]
- Yeung, O.; Aziz, F.; Arguelles, S. Signalling pathways in inflammation and anti-inflammatory therapies. Curr. Pharm. Des. 2018, 21, 449–1484. [Google Scholar]
- Me’graud, F.; Lehours, P. Helicobacter pylori detection and antimicrobial susceptibility testing. Clin. Microbiol. 2007, 20, 280–322. [Google Scholar] [CrossRef] [Green Version]
- Gómez-Priego, A.; Crecencio-Rosales, L.; de-La-Rosa, J.L. Serlogical evaluation of thin layer immunoassay enzyme-linked ummunosorbent assay for antibody detection in human trichinellosis. Clin. Diagn. Lab. Immunol. 2000, 7, 810–812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ricci, C.; Holton, J.; Vaira, D. Diagnosis of Helicobacter pylori: Invasive and non-invasive tests. Clin. Gastroenterol. 2007, 21, 299–313. [Google Scholar] [CrossRef] [PubMed]
- Ismail, M.; Draper, C.; Ouchterlony, O.; Nilsson, L.A.; Terry, R. A comparison between a new serological method, thin layer immunoassay (TIA), and the enzyme-linked immunosorbent assay (ELISA) for the detection of antibodies in schistosomiasis. Parasite Immunol. 1979, 3, 1251–1258. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, L.A.; Petchclai, B.; Elwing, H. Application of thin layer immunoassay (TIA) for demonstration of antibodies against Entamoeba histolytica. Am. J. Trop. Med. Hyg. 1980, 29, 524–529. [Google Scholar] [CrossRef] [PubMed]
- Elwing, H.; Nilson, L.A.; Ouchterlony, O. A simple spot technique for thin layer immunoassays (TIA) on plastic surfaces. J. Immunol. Methods 1977, 17, 131–145. [Google Scholar] [CrossRef]
- Nilsson, L.A.; Björck, L.; Elwing, H.; Ouchterlony, O. Determination of rheumatoid factor by means of thin layer immunoassay. Int. Arch. Allergy Appl. Immunol. 1980, 63, 294–302. [Google Scholar] [CrossRef]
- Faisal, A.; Sherwani, S.K.; Akhtar, S.S.; Kazmi, S.U. Development of an in-house enzyme linked immunosorbent assay based on surface whole cell antigen for diagnosis of Helicobacter pylori infection in patients with gastroduodenal ulcer disease. World J. Microbiol. Biotechnol. 2014, 30, 305–315. [Google Scholar]
- Faisal, A.; Yasmeen, T.; Akhtar, S.S.; Kazmi, S.U. In-House Enzyme-Linked Immunosorbent Assay Based on Helicobacter Pylori sonicate whole cell antigen for diagnosis of Helicobacter Pylori Infection in Karachi, Pakistan. Int. J. Microbiol. Immunol. 2013, 1, 1–10. [Google Scholar]
- Islam, K.; Khalil, I.; Ahsan, C.R.; Yasmin, M.; Nessa, J. Analysis of immune responses against H. pylori in rabbits. World J. Gastroenterol. 2007, 13, 600–606. [Google Scholar] [CrossRef] [Green Version]
- Rahman, S.H.; Azam, M.G.; Rahman, M.A.; Arfin, M.S.; Alam, M.M.; Bhuiyan, T.M.; Ahmed, N.; Rahman, M.; Nahar, S.; Hassan, M.S. Noninvasive diagnosis of H. pylori infection: Evaluation of serological tests with and without current infection marker CIM. World J. Gastroenterol. 2008, 14, 1231–1236. [Google Scholar] [CrossRef]
- Dos Santos Viana, I.; Cordeiro Santos, M.L.; Santos Marques, H.; Lima de Souza Gonçalves, V.; Bittencourt de Brito, B.; França da Silva, F.A.; Oliveira, E.; Silva, N.; Dantas Pinheiro, F.; Fernandes Teixeira, A.; et al. Vaccine development against Helicobacter pylori: From ideal antigens to the current landscape. Expert Rev. Vaccines 2021, 20, 989–999. [Google Scholar] [CrossRef]
- Sunnerstam, B.; Kjerstadius, T.; Jansson, L.; Giesecke, J.; Bergstro¨m, M.; Ejderhamn, J. Detection of Helicobacter pylori antibodies in a pediatric population: Comparison of three commercially available serological tests and one in-house enzyme immunoassal. J. Clin. Microbiol. 1999, 37, 3328–3331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Namyalo, E.; Nyakarahuka, L.; Afayoa, M.; Baziira, J.; Tamale, A.; Atuhaire, G.C.; Kungu, J.M. Prevalence of Helicobacter pylori among Patients with Gastrointestinal Tract (GIT) Symptoms: A Retrospective Study at Selected Africa Air Rescue (AAR) Clinics in Kampala, Uganda, from 2015 to 2019. J. Trop. Med. 2021, 2021, 9935142. [Google Scholar] [CrossRef] [PubMed]
- Breckan, R.K.; Paulssen, E.J.; Asfeldt, A.M.; Kvamme, J.M.; Straume, B.; Florholmen, J. The All-Age Prevalence of Helicobacter pylori Infection and Potential Transmission Routes. A Population-Based Study. Helicobacter 2016, 21, 586–595. [Google Scholar] [CrossRef] [Green Version]
- Rowland, M.; Daly, L.; Vaughan, M.; Higgins, A.; Bourke, B.; Drumm, B. Age-Specific Incidence of Helicobacter pylori. Gastroenterology 2006, 130, 65–72. [Google Scholar] [CrossRef]
- Park, J.S.; Jun, J.S.; Seo, J.H.; Youn, H.S.; Rhee, K.H. Changing prevalence of Helicobacter pylori infection in children and adolescents. Clin. Exp. Pediatr. 2021, 64, 21–25. [Google Scholar] [CrossRef] [PubMed]
- McNulty, C.A.; Nair, P.; Watson, B.E.; Uff, J.S.; Valori, R.M. A comparison of six commercial kits for Helicobacter pylori detection. Commun. Dis. Public Health 1999, 2, 59–63. [Google Scholar]
- Alem, M.; Wojdani, A. Anti-Campylobacter antibodies as an indication for diagnosis of peptic ulcer. In Proceedings of the International Conference on Gastroenteric Biology, Oxnard, CA, USA, 1998. [Google Scholar]
- Obata, Y.; Kikuchi, S.; Miwa, H.; Yagyu, K.; Lin, Y.; Ogihara, A. Diagnostic accuracy of serological kits for Helicobacter pylori infection with the same assaysystem but different antigens in a Japanese patient population. J. Med. Microbiol. 2003, 52, 889–892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Safaei, H.G.; Fazeli, A.; Tamizifar, H.; Rashidi, N. Comparison of salivary anti Helicobacter pylori IgG with serum IgG and bacteriological tests in detecting Helicobacter pylori infections. J. Res. Med. Sci. 2005, 10, 1–5. [Google Scholar]
- Shughart, L.C.; Lappas, N.T. Detection of opiates in blood by thin-layer immunoassay. J. Anal. Toxicol. 1983, 7, 209–212. [Google Scholar] [CrossRef]
- Gómez-Morales, A.; Cherchi, S.; Ludovisi, A. Serological testing for Trichinella infection in animals and man: Current status and opportunities for advancements. Food Waterborne Parasitol. 2022, 27, e00165. [Google Scholar] [CrossRef] [PubMed]
- Ambroise-Thomas, P.; Castro, B. Le test à la vapeur. Thin layer immunoassay (TIA). A rapid and simple method for the serodiagno sis of echinococcosis. Ann. Biol. Clin. 1982, 40, 29–35. [Google Scholar]
- Nilsson, L.A.; Voller, A. A comparison of thin layer immunoassay (TIA) and enzyme-linked immunosorbent assay (ELISA) for the detection of antibodies to Trypanosoma cruzi L. Trans. R Soc. Trop. Med. Hyg. 1982, 76, 95–97. [Google Scholar] [CrossRef] [PubMed]
- Fredenburg, M.E.; Lappas, N.T. Detection of opiates in urine by means of thin layer immunoassay. J. Anal. Toxicol. 1982, 6, 127–130. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Standard Assays | Sensitivity % | Specificity % | Accuracy % | PPV % | NPV % | FPV | FNV | OA | EA | AABC | PABC | KAPPA |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| H. pylori Thin Layer Immunoassay | ||||||||||||
| wELISA | 72 | 100 | 76 | 100 | 35 | 0.0 | 0.28 | 0.757 | 0.52 | 0.237 | 0.480 | 0.493 |
| sELISA | 68 | 100 | 71 | 100 | 22.5 | 0.0 | 0.316 | 0.710 | 0.52 | 0.190 | 0.480 | 0.396 |
| kELISA | 67 | 100 | 69 | 100 | 18 | 0.0 | 0.33 | 0.691 | 0.52 | 0.17 | 0.480 | 0.357 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aziz, F.; Kazmi, S.U. Thin Layer Immunoassay: An Economical Approach to Diagnose Helicobacter pylori Infection in Gastroduodenal Ulcer Disease Patients of Pakistan, a Comparative Analysis. Diagnostics 2023, 13, 517. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics13030517
Aziz F, Kazmi SU. Thin Layer Immunoassay: An Economical Approach to Diagnose Helicobacter pylori Infection in Gastroduodenal Ulcer Disease Patients of Pakistan, a Comparative Analysis. Diagnostics. 2023; 13(3):517. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics13030517
Chicago/Turabian StyleAziz, Faisal, and Shahana Urooj Kazmi. 2023. "Thin Layer Immunoassay: An Economical Approach to Diagnose Helicobacter pylori Infection in Gastroduodenal Ulcer Disease Patients of Pakistan, a Comparative Analysis" Diagnostics 13, no. 3: 517. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics13030517