
The Pre-Treatment Platelet-to-Lymphocyte Ratio as a Prognostic Factor for Loco-Regional Control in Locally Advanced Rectal Cancer

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Study Design
2.2. Treatment Regime and Follow-Up
2.3. Study Endpoints and Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Benson, A.B.; Venook, A.P.; Al-Hawary, M.M.; Arain, M.A.; Chen, Y.J.; Ciombor, K.K.; Cohen, S.; Cooper, H.S.; Deming, D.; Garrido-Laguna, I.; et al. NCCN Guidelines Insights: Rectal Cancer, Version 6.2020: Featured Updates to the NCCN Guidelines. J. Natl. Compr. Cancer Netw. 2020, 18, 806–815. [Google Scholar]
- Siegel, R.; Miller, K.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Argilés, G.; Tabernero, J.; Labianca, R.; Hochhauser, D.; Salazar, R.; Iveson, T.; Laurent-Puig, P.; Quirke, P.; Yoshino, T.; Taieb, J.; et al. Localised colon cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up†. Ann. Oncol. 2020, 31, 1291–1305. [Google Scholar] [CrossRef] [PubMed]
- Karki, R.; Man, S.; Kanneganti, T.-D. Inflammasomes and Cancer. Cancer Immunol. Res. 2017, 5, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Sciarra, A.; Gentilucci, A.; Salciccia, S.; Pierella, F.; Del Bianco, F.; Gentile, V.; Silvestri, I.; Cattarino, S. Prognostic value of inflammation in prostate cancer progression and response to therapeutic: A critical review. J. Inflamm. 2016, 13, 35. [Google Scholar] [CrossRef]
- Grivennikov, S.I.; Greten, F.; Karin, M. Immunity, inflammation, and cancer. Cell 2010, 140, 883–899. [Google Scholar] [CrossRef]
- Makita, K.; Hamamoto, Y.; Takata, N.; Ishikawa, H.; Tsuruoka, S.; Uwatsu, K.; Hato, N.; Kido, T. Prognostic significance of inflammatory response markers for locally advanced squamous cell carcinoma of the external auditory canal and middle ear. J. Radiat. Res. 2021, 62, 662–668. [Google Scholar] [CrossRef]
- Jones, H.G.; Qasem, E.; Dilaver, N.; Egan, R.; Bodger, O.; Kokelaar, R.; Evans, M.D.; Davies, M.; Beynon, J.; Harris, D. Inflammatory cell ratios predict major septic complications following rectal cancer surgery. Int. J. Color. Dis. 2018, 33, 857–862. [Google Scholar] [CrossRef]
- Shen, J.; Zhu, Y.; Wu, W.; Zhang, L.; Ju, H.; Fan, Y.; Zhu, Y.; Luo, J.; Liu, P.; Zhou, N.; et al. Prognostic role of neutrophil-to-lymphocyte ratio in locally advanced rectal cancer treated with neoadjuvant chemoradiotherapy. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2017, 23, 315. [Google Scholar] [CrossRef]
- Zhang, Y.; Liu, X.; Xu, M.; Chen, K.; Li, S.; Guan, G. Prognostic value of pretreatment systemic inflammatory markers in patients with locally advanced rectal cancer following neoadjuvant chemoradiotherapy. Sci. Rep. 2020, 10, 8017. [Google Scholar] [CrossRef]
- Naszai, M.; Kurjan, A.; Maughan, T. The prognostic utility of pre-treatment neutrophil-to-lymphocyte-ratio (NLR) in colorectal cancer: A systematic review and meta-analysis. Cancer Med. 2021, 10, 5983–5997. [Google Scholar] [CrossRef]
- Partl, R.; Lukasiak, K.; Thurner, E.-M.; Renner, W.; Stranzl-Lawatsch, H.; Langsenlehner, T. The Elevated Pre-Treatment C-Reactive Protein Predicts Poor Prognosis in Patients with Locally Advanced Rectal Cancer Treated with Neo-Adjuvant Radiochemotherapy. Diagnostics 2020, 10, 780. [Google Scholar] [CrossRef]
- Toiyama, Y.; Inoue, Y.; Kawamura, M.; Kawamoto, A.; Okugawa, Y.; Hiro, J.; Saigusa, S.; Tanaka, K.; Mohri, Y.; Kusunoki, M. Elevated platelet count as predictor of recurrence in rectal cancer patients undergoing preoperative chemoradiotherapy followed by surgery. Int. Surg. 2015, 100, 199–207. [Google Scholar] [CrossRef]
- Kawai, K.; Kitayama, J.; Tsuno, N.H.; Sunami, E.; Watanabe, T. Thrombocytosis before pre-operative chemoradiotherapy predicts poor response and shorter local recurrence-free survival in rectal cancer. Int. J. Color. Dis. 2013, 28, 527–535. [Google Scholar] [CrossRef]
- Lin, R.J.; Afshar-Kharghan, V.; Schafer, A. Paraneoplastic thrombocytosis: The secrets of tumor self-promotion. Blood 2014, 124, 184–187. [Google Scholar] [CrossRef]
- Wang, C.; Tong, J.; Tang, M.; Lu, Y.; Liang, G.; Zhang, Z.; Chen, T. Pretreatment Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio as Prognostic Factors and Reference Markers of Treatment Options for Locally Advanced Squamous Cell Carcinoma Located in the Middle and Upper Esophagus. Cancer Manag. Res 2021, 13, 1075–1085. [Google Scholar] [CrossRef]
- Tesfamariam, B. Involvement of platelets in tumor cell metastasis. Pharmacol. Ther. 2016, 157, 112–119. [Google Scholar] [CrossRef]
- Nieswandt, B.; Hafner, M.; Echtenacher, B.; Männel, D.N. Lysis of tumor cells by natural killer cells in mice is impeded by platelets. Cancer Res. 1999, 59, 1295–1300. [Google Scholar]
- Peterson, J.E.; Zurakowski, D.; Italiano, J.E., Jr.; Michel, L.V.; Connors, S.; Oenick, M.; D’Amato, R.J.; Klement, G.L.; Folkman, J. VEGF, PF4 and PDGF are elevated in platelets of colorectal cancer patients. Angiogenesis 2012, 15, 265–273. [Google Scholar] [CrossRef]
- Kisucka, J.; Butterfield, C.E.; Duda, D.G.; Eichenberger, S.C.; Saffaripour, S.; Ware, J.; Ruggeri, Z.M.; Jain, R.K.; Folkman, J.; Wagner, D.D. Platelets and platelet adhesion support angiogenesis while preventing excessive hemorrhage. Proc. Natl. Acad. Sci. USA 2006, 103, 855–860. [Google Scholar] [CrossRef]
- Jia, W.; Yuan, L.; Ni, H.; Xu, B.; Zhao, P. Prognostic Value of Platelet-to-Lymphocyte Ratio, Neutrophil-to-Lymphocyte Ratio, and Lymphocyte-to-White Blood Cell Ratio in Colorectal Cancer Patients Who Received Neoadjuvant Chemotherapy. Technol. Cancer Res. Treat. 2021, 20, 15330338211034291. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zhang, H.-Y.; Li, J.; Shao, X.-Y.; Zhang, C.-X. The elevated NLR, PLR and PLT may predict the prognosis of patients with colorectal cancer: A systematic review and meta-analysis. Oncotarget 2017, 8, 68837–68846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, D.; Fu, Y.; Su, Q.; Wang, H. Prognostic role of platelet-lymphocyte ratio in colorectal cancer: A systematic review and meta-analysis. Medicine 2016, 95, e3837. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Du, Y.; Huang, Z.; Xu, J.; Qiu, T.; Wang, J.; Wang, T.; Zhu, W.; Liu, P. Prognostic value of PLR in various cancers: A meta-analysis. PLoS ONE 2014, 9, e101119. [Google Scholar] [CrossRef] [PubMed]
- Ding, N.; Pang, Z.; Shen, H.; Ni, Y.; Du, J.; Liu, Q. The Prognostic Value of PLR in Lung Cancer, a Meta-analysis Based on Results from a Large Consecutive Cohort. Sci. Rep. 2016, 6, 34823. [Google Scholar] [CrossRef]
- Langsenlehner, T.; Pichler, M.; Thurner, E.-M.; Krenn-Pilko, S.; Stojakovic, T.; Gerger, A.; Langsenlehner, U. Evaluation of the platelet-to-lymphocyte ratio as a prognostic indicator in a European cohort of patients with prostate cancer treated with radiotherapy. Urol. Oncol. Semin. Orig. Investig. 2015, 33, e9–e201. [Google Scholar] [CrossRef]
- Zhou, K.; Cao, J.; Lin, H.; Liang, L.; Shen, Z.; Wang, L.; Peng, Z.; Mei, J. Prognostic role of the platelet to lymphocyte ratio (PLR) in the clinical outcomes of patients with advanced lung cancer receiving immunotherapy: A systematic review and meta-analysis. Front. Oncol. 2022, 12, 9. [Google Scholar] [CrossRef]
- Chen, H.; Wu, X.; Wen, Z.; Zhu, Y.; Liao, L.; Yang, J. The Clinicopathological and Prognostic Value of NLR, PLR and MLR in Non-Muscular Invasive Bladder Cancer. Arch. Esp. Urol. 2022, 75, 467–471. [Google Scholar] [CrossRef]
- Szkandera, J.; Pichler, M.; Absenger, G.; Stotz, M.; Arminger, F.; Weissmueller, M.; Schaberl-Moser, R.; Samonigg, H.; Kornprat, P.; Stojakovic, T.; et al. The elevated preoperative platelet to lymphocyte ratio predicts decreased time to recurrence in colon cancer patients. Am. J. Surg. 2014, 208, 210–214. [Google Scholar] [CrossRef]
- Acikgoz, O.; Cakan, B.; Demir, T.; Bilici, A.; Oven, B.B.; Hamdard, J.; Olmuscelik, O.; Olmez, O.F.; Seker, M.; Yildiz, O. Platelet to lymphocyte ratio is associated with tumor localization and outcomes in metastatic colorectal cancer. Medicine 2021, 100, e27712. [Google Scholar] [CrossRef]
- Mori, K.; Toiyama, Y.; Saigusa, S.; Fujikawa, H.; Hiro, J.; Kobayashi, M.; Ohi, M.; Araki, T.; Inoue, Y.; Tanaka, K.; et al. Systemic Analysis of Predictive Biomarkers for Recurrence in Colorectal Cancer Patients Treated with Curative Surgery. Dig. Dis. Sci. 2015, 60, 477–2487. [Google Scholar] [CrossRef]
- Duque-Santana, V.; López-Campos, F.; Martin-Martin, M.; Valero, M.; Zafra-Martín, J.; Couñago, F.; Sancho, S. Neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio as prognostic factors in locally advanced rectal cancer. Oncology 2022. Online ahead of print. [Google Scholar] [CrossRef]
- Li, B.; Zhou, P.; Liu, Y.; Wei, H.; Yang, X.; Chen, T.; Xiao, J. Platelet-to-lymphocyte ratio in advanced Cancer: Review and meta-analysis. Clin. Chim. Acta 2018, 483, 48–56. [Google Scholar] [CrossRef]
- Ozawa, T.; Ishihara, S.; Nishikawa, T.; Tanaka, T.; Tanaka, J.; Kiyomatsu, T.; Hata, K.; Kawai, K.; Nozawa, H.; Kazama, S.; et al. The preoperative platelet to lymphocyte ratio is a prognostic marker in patients with stage II colorectal cancer. Int. J. Color. Dis. 2015, 30, 1165–1171. [Google Scholar] [CrossRef]
- Aiolfi, R.; Sitia, G. Chronic hepatitis B: Role of anti-platelet therapy in inflammation control. Cell. Mol. Immunol. 2015, 12, 264–268. [Google Scholar] [CrossRef]
- Davi, G.; Patrono, C. Platelet activation and atherothrombosis. N. Engl. J. Med. 2007, 357, 2482–2494. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| Number of patients | 603 |
| Sex | |
| Male Female | 406 (67.3%) 197 (32.7%) |
| Age; median (mean ± SD) | 66.6 (65.6 ± 10.5) |
| Smoking status | |
| Current Former* or never Missing | 84 (13.9%) 370 (61.4%) 149 (24.7%) |
| Tumor site | |
| <6 cm ab ano 6–12 cm ab ano 12–16 cm ab ano | 344 (57.0%) 241 (40.0%) 18 (3.0%) |
| Tumor grade | |
| G 1 G 2 G 3 Missing | 41 (6.8%) 515 (85.4%) 42 (7.0%) 5 (0.8%) |
| Clinical tumor stage | |
| T2 T3 T4 | 16 (2.7%) 522 (86.6%) 65 (10.7%) |
| Clinical nodal involvement | |
| Yes No | 370 (61.4%) 233 (38.6%) |
| Clinical stage | |
| Stage II Stage III/IV | 228 (37.8%) 375 (62.2%) |
| Chemotherapy | |
| 5-Fluoruracil Cabecitabine Missing | 451 (74.8%) 151 (25.0%) 1 (0.2%) |
| LDH, median (mean ± SD) | 178.5 (193.4 ± 67.0) |
| CEA, median (mean ± SD) | 3.5 (9.9 ± 39.2) |
| CA 19-9, median (mean ± SD) | 8.1 (27.0 ± 84.5) |
| NLR, median (mean ± SD) | 3.1 (3.6 ± 2.1) |
| PLR, median (mean ± SD) | 173.9 (193.9 ± 95.9) |
| Loco-Regional Control | Metastases-Free Survival | Overall Survival | ||||
|---|---|---|---|---|---|---|
| Criterion | HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value |
| Sex | ||||||
| Male Female | 1 0.656 (0.309–1.390) | 0.271 | 1 1.191 (0.799–1.775) | 0.392 | 1 1.782 (0.492–1.241) | 0.296 |
| Age (continuous) | 0.987 (0.957–1.017) | 0.390 | 1 1.008 ((0.989–1.028) | 0.389 | 1.041 (1.019–1.064) | < 0.001 |
| Smoking status | ||||||
| Current Former/Never | 1 0.449 (0.211–0.953) | 0.037 | 1 0.791 (0.455–1.373) | 0.404 | 1 1.216 (0.621–2.238) | 0.568 |
| Tumor site (ab ano) | ||||||
| <6 cm 6–12 cm 12–16 cm | 1 0.707 (0.360–1.389) 0 (0–1.358) | 0.314 0.974 | 1 1.191 (0.807–1.757) 0.593 (0.145–2.436) | 0.379 0.469 | 1 1.127 (0.740–1.718) 0.712 (0.173–2.933) | 0.577 0.638 |
| Tumor grade | ||||||
| G 1 G 2 G 3 | 1 2.664 (0.364–19.488) 2.015 (0.183–22.226) | 0.334 0.567 | 1 1.470 (0.597–3.618) 1.794 (0.601–5.355) | 0.402 0.295 | 1 1.035 (0.451–2.378) 1.209 (0.406–3.599) | 0.935 0.733 |
| Tumor stage | ||||||
| T 1-3 T 4 | 1 1.585 (0.617–4.072) | 0.338 | 1 1.468 (0.820–2.625) | 0.196 | 1 1.583 (0.861–2.910) | 0.139 |
| Nodal involvement | ||||||
| No Yes | 1 1.634 (0.807–3.309) | 0.172 | 1 1.201 (0.805–1.790) | 0.369 | 1 0.871 (0.573–1.323) | 0.517 |
| Clinical stage | ||||||
| II III/IV | 1 1.414 (0.710–2.816) | 0.324 | 1 1.305 (0.871–1.955) | 0.197 | 1 0.989 (0.649–1.508) | 0.959 |
| Chemotherapy | ||||||
| 5-Fluoruracil Cabecitabine | 1 0.970 (0.458–2.057) | 0.938 | 1 0.854 (0.538–1.358) | 0.505 | 1 1.111 (0.696–1.774) | 0.660 |
| LDH (continuous) | 0.996 (0.990–1.003) | 0.263 | 1.003 (1.001–1.006) | 0.007 | 1.002 (1.000–1.005) | 0.108 |
| CEA (continuous) | 1.003 (0.997–1.009) | 0.407 | 1.007 (1.004–1.009) | < 0.001 | 1.005 (1.003–1.008) | < 0.001 |
| CA 19-9 (continuous) | 1.002 (0.999–1.004) | 0.147 | 1.001 (0.999–1.003) | 0.375 | 1.000 (0.998–1.003) | 0.819 |
| NLR (continuous) | 1.083 (0.966–1.214) | 0.173 | 1.034 (0.951–1.124) | 0.436 | 1.104 (1.027–1.186) | 0.007 |
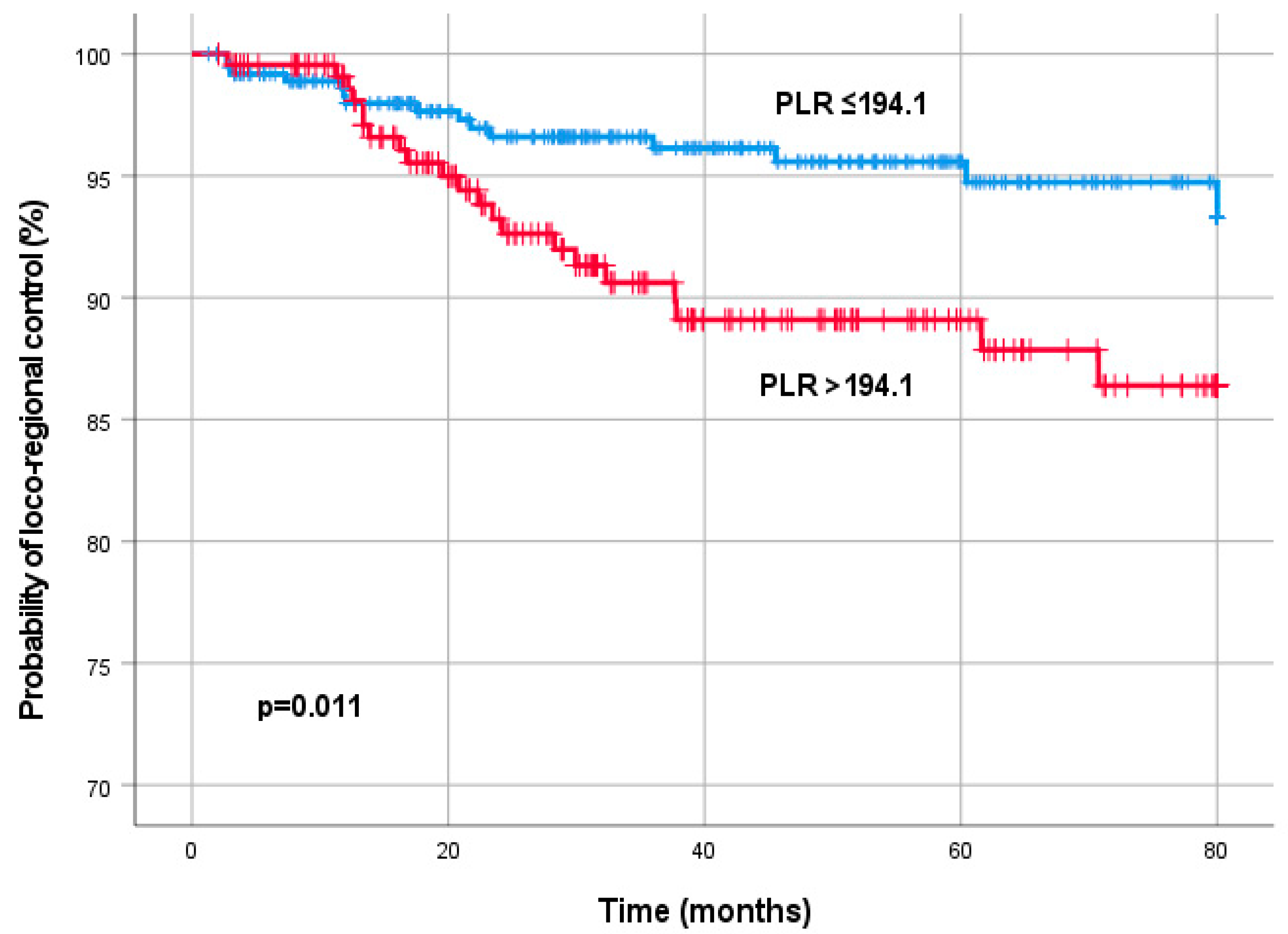
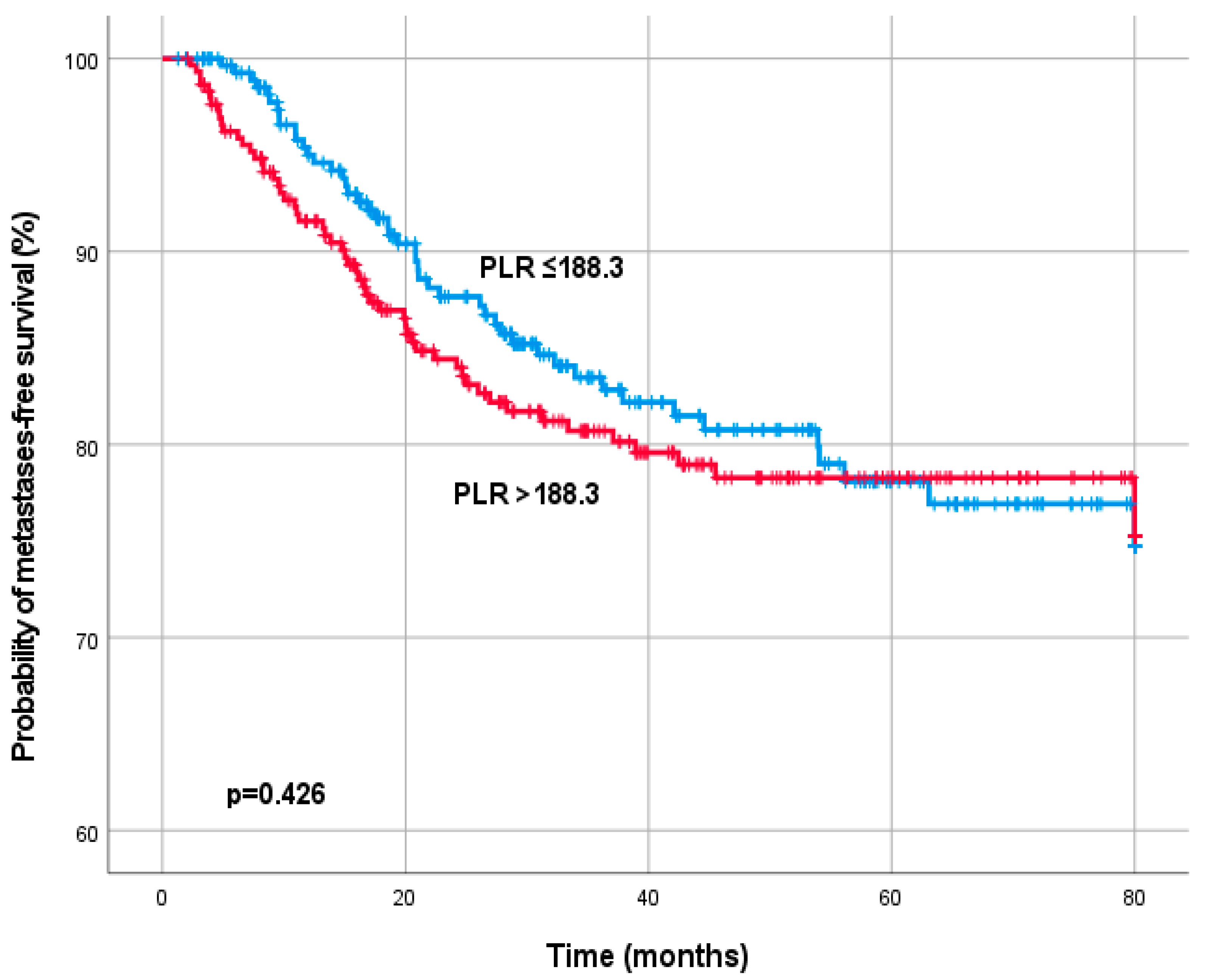
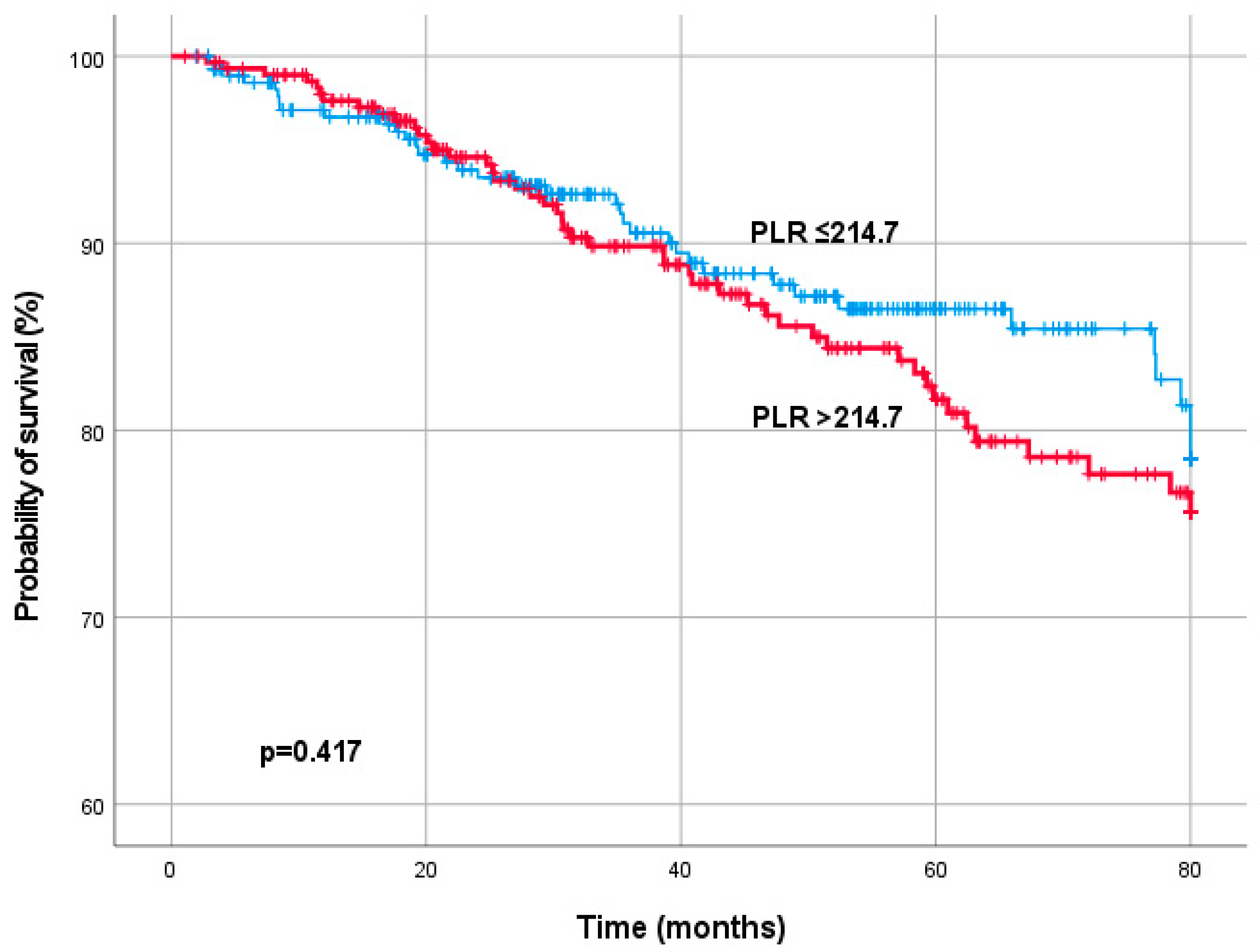
| PLR (continuous) | 1.003 (1.001–1.006) | 0.017 | 1.001 (0.999–1.003) | 0.446 | 1.002 (1.001–1.004) | 0.008 |
| Loco-Regional Control | Metastases-Free Survival | Overall Survival | ||||
|---|---|---|---|---|---|---|
| Criterion | HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value |
| Age (continuous) | 1.052 (1.023–1.081) | <0.001 | ||||
| Smoking status | ||||||
| Current Former/Never | 1 0.720 (0.250–2.077) | 0.544 | ||||
| Tumor stage | ||||||
| T 1-3 T 4 | 1 1.574 (0.786–3.150) | 0.200 | 1 1.581 (0.703–3.557) | 0.268 | ||
| Nodal involvement | ||||||
| No Yes | 1 1.275 (0.505–3.219) | 0.607 | ||||
| Clinical stage | ||||||
| II III/IV | 1 1.353 (0.814–2.249) | 0.243 | ||||
| LDH (continuous) | 1.005 (1.002–1.008) | <0.001 | 1.003 (1.000–1.007) | 0.029 | ||
| CEA (continuous) | 1.006 (1.003–1.009) | <0.001 | 1.006 (1.003–1.009) | <0.001 | ||
| CA 19-9 (continuous) | 1.002 (0.999–1.004) | 0.196 | ||||
| NLR (continuous) | 0.947 (0.741–1.210) | 0.662 | 0.938 (0.798–1.102) | 0.435 | ||
| PLR (continuous) | 1.005 (1.000–1.009) | 0.050 | 1.002 (0.999–1.006) | 0.205 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Partl, R.; Paal, K.; Stranz, B.; Hassler, E.; Magyar, M.; Brunner, T.B.; Langsenlehner, T. The Pre-Treatment Platelet-to-Lymphocyte Ratio as a Prognostic Factor for Loco-Regional Control in Locally Advanced Rectal Cancer. Diagnostics 2023, 13, 679. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics13040679
Partl R, Paal K, Stranz B, Hassler E, Magyar M, Brunner TB, Langsenlehner T. The Pre-Treatment Platelet-to-Lymphocyte Ratio as a Prognostic Factor for Loco-Regional Control in Locally Advanced Rectal Cancer. Diagnostics. 2023; 13(4):679. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics13040679
Chicago/Turabian StylePartl, Richard, Katarzyna Paal, Bettina Stranz, Eva Hassler, Marton Magyar, Thomas Baptist Brunner, and Tanja Langsenlehner. 2023. "The Pre-Treatment Platelet-to-Lymphocyte Ratio as a Prognostic Factor for Loco-Regional Control in Locally Advanced Rectal Cancer" Diagnostics 13, no. 4: 679. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics13040679