
Drug-Induced Acute Pancreatitis in Hospitalized COVID-19 Patients
 , ,
, , 
Abstract
:1. Introduction
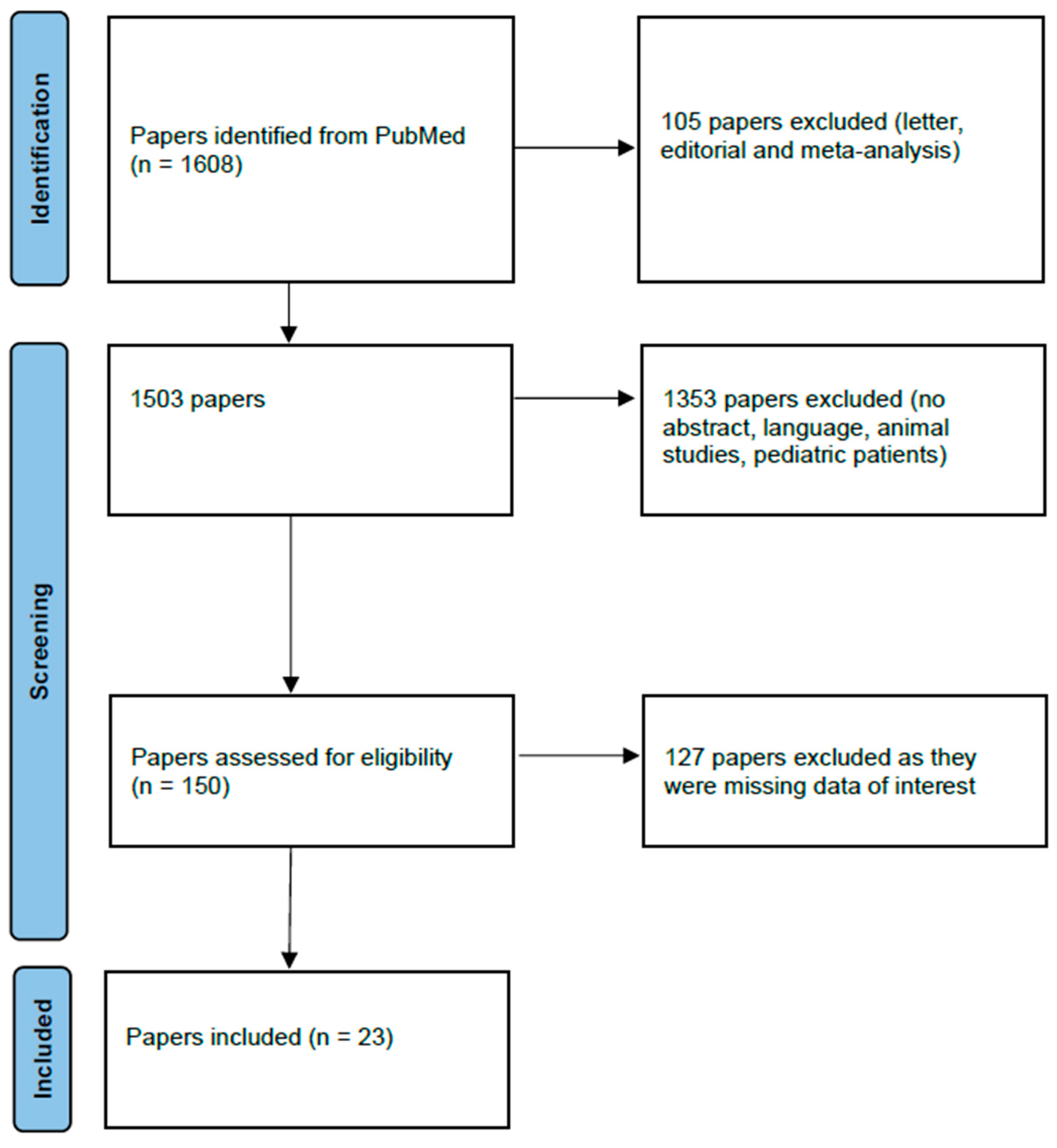
2. Materials and Methods
Results
3. Discussion
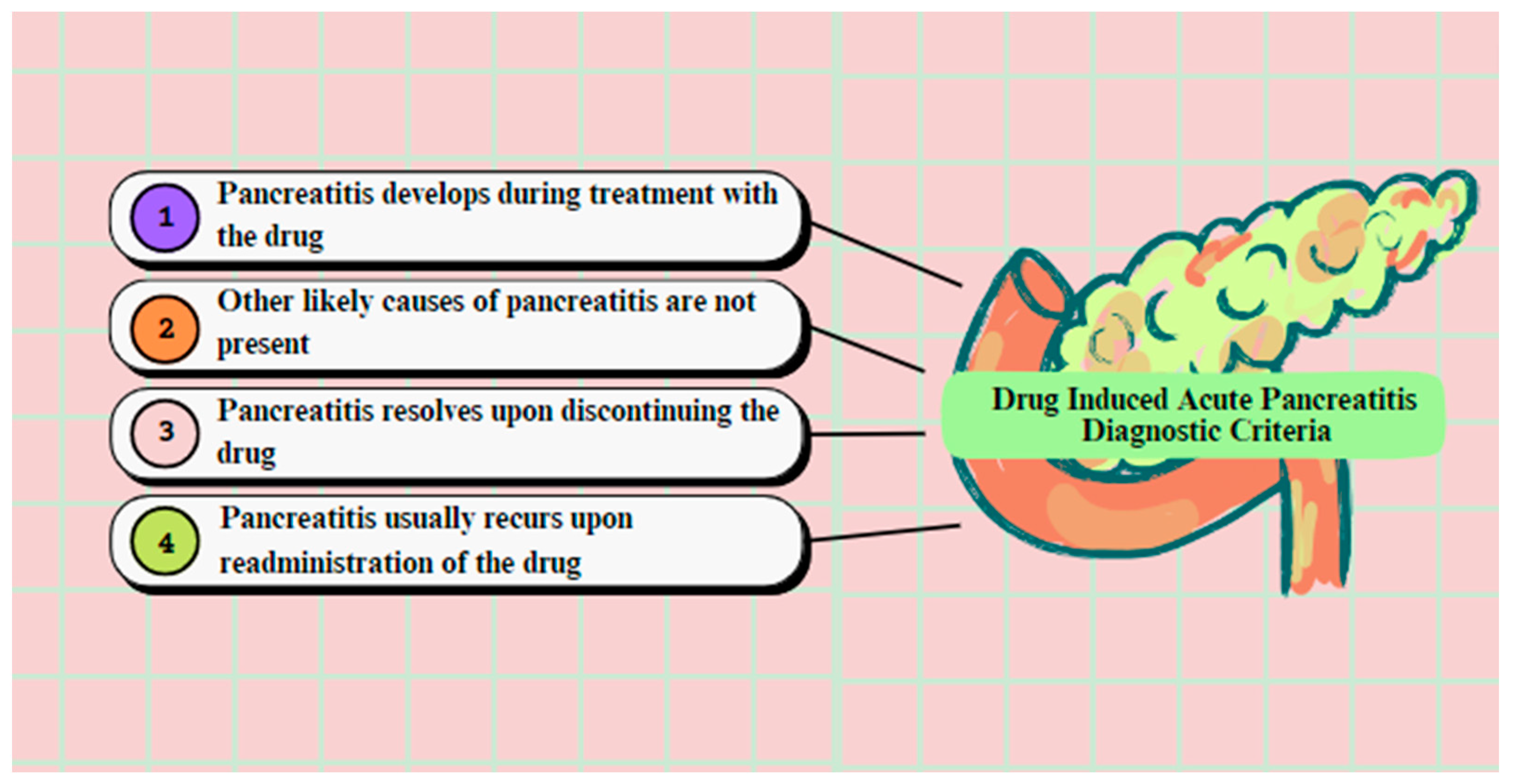
3.1. Diagnosis οf Drug-Induced Acute Pancreatitis
3.2. Risk Factors of Drug-Induced Acute Pancreatitis
3.3. Drug Classification
3.4. Associated Medications
3.4.1. Corticosteroids (Dexamethasone)
3.4.2. Glucocorticosteroids (GCSs)
3.4.3. Non-Steroidal Anti-Inflammatory Drugs (NSAIDs)
3.4.4. Antiviral Agents
Remdesivir
3.4.5. Tocilizumab
3.4.6. Antibiotics
Azithromycin
Ciprofloxacin
Doxycycline
3.4.7. Propofol
3.4.8. Estrogens
3.4.9. Other Medications
3.5. Prophylaxis
3.6. Therapy
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sinagra, E.; Shahini, E.; Crispino, F.; Macaione, I.; Guarnotta, V.; Marasà, M.; Testai, S.; Pallio, S.; Albano, D.; Facciorusso, A.; et al. COVID-19 and the Pancreas: A Narrative Review. Life 2022, 12, 1292. [Google Scholar] [CrossRef] [PubMed]
- Allam, M.M.; El-Zawawy, H.T.; Ahmed, S.M.; Abdelhamid, M.A. COVID-19 treatment: A potential cause of acute pancreatitis. Clin Case Rep. 2022, 10, e6465. [Google Scholar] [CrossRef] [PubMed]
- Stasi, C.; Fallani, S.; Voller, F.; Silvestri, C. Treatment for COVID-19: An overview. Eur. J. Pharmacol. 2020, 889, 173644. [Google Scholar] [CrossRef] [PubMed]
- Somasundaram, N.P.; Ranathunga, I.; Ratnasamy, V.; Wijewickrama, P.S.A.; Dissanayake, H.A.; Yogendranathan, N.; Gamage, K.K.K.; de Silva, N.L.; Sumanatilleke, M.; Katulanda, P.; et al. The Impact of SARS-Cov-2 Virus Infection on the Endocrine System. J. Endocr Soc. 2020, 4, bvaa082. [Google Scholar] [CrossRef]
- Wang, G.J.; Gao, C.F.; Wei, D.; Wang, C.; Ding, S.Q. Acute pancreatitis: Etiology and common pathogenesis. World J. Gastroenterol. 2009, 15, 1427–1430. [Google Scholar] [CrossRef]
- Parkash, O.; Sharko, A.; Farooqi, A.; Ying, G.W.; Sura, P. Acute Pancreatitis: A Possible Side Effect of COVID-19 Vaccine. Cureus 2021, 13, e14741. [Google Scholar] [CrossRef]
- Cappell, M.S. Acute Pancreatitis: Etiology, Clinical Presentation, Diagnosis, and Therapy. Med. Clin. N. Am. 2008, 92, 889–923. [Google Scholar] [CrossRef]
- Mederos, M.A.; Reber, H.A.; Girgis, M.D. Acute Pancreatitis: A Review. JAMA 2021, 325, 382–390. [Google Scholar] [CrossRef]
- Hung, W.Y.; Abreu Lanfranco, O. Contemporary review of drug-induced pancreatitis: A different perspective. World J. Gastrointest. Pathophysiol. 2014, 5, 405–415. [Google Scholar] [CrossRef]
- AlHarmi, R.A.R.; Fateel, T.; Sayed Adnan, J.; AlAwadhi, K. Acute pancreatitis in a patient with COVID-19. BMJ Case Rep. 2021, 14, e239656. [Google Scholar] [CrossRef]
- Jia, H.P.; Look, D.C.; Shi, L.; Hickey, M.; Pewe, L.; Netland, J.; Farzan, M.; Wohlford-Lenane, C.; Perlman, S.; McCray, P.B., Jr. ACE2 receptor expression and severe acute respiratory syndrome coronavirus infection depend on differentiation of human airway epithelia. J. Virol. 2005, 79, 14614–14621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abramczyk, U.; Nowaczynski, M.; Słomczynski, A.; Wojnicz, P.; Zatyka, P.; Kuzan, A. Consequences of COVID-19 for the Pancreas. Int. J. Mol. Sci. 2022, 23, 864. [Google Scholar] [CrossRef] [PubMed]
- Goyal, H.; Kopel, J.; Ristic, B.; Perisetti, A.; Anastasiou, J.; Chandan, S.; Tharian, B.; Inamdar, S. The pancreas and COVID-19: A clinical conundrum. Am. J. Transl Res. 2021, 13, 11004–11013. [Google Scholar] [PubMed]
- Wang, F.; Wang, H.; Fan, J.; Zhang, Y.; Wang, H.; Zhao, Q. Pancreatic Injury Patterns in Patients With Coronavirus Disease 19 Pneumonia. Gastroenterology 2020, 159, 367–370. [Google Scholar] [CrossRef] [PubMed]
- Muzahim, Y.E.; Parish, D.C.; Goyal, H. Insights into Acute Pancreatitis Associated COVID-19: Literature Review. J. Clin. Med. 2021, 10, 5902. [Google Scholar] [CrossRef]
- Brikman, S.; Denysova, V.; Menzal, H.; Dori, G. Acute pancreatitis in a 61-year-old man with COVID-19. CMAJ 2020, 192, E858–E859. [Google Scholar] [CrossRef]
- Juhász, M.F.; Ocskay, K.; Kiss, S.; Hegyi, P.; Párniczky, A. Insufficient etiological workup of COVID-19-associated acute pancreatitis: A systematic review. World J. Gastroenterol. 2020, 26, 6270–6278. [Google Scholar] [CrossRef]
- Zheng, J.; Yang, Q.J.; Dang, F.T.; Yang, J. Drug-induced pancreatitis: An update. Arab J. Gastroenterol. 2019, 20, 183–188. [Google Scholar] [CrossRef]
- Nitsche, C.; Maertin, S.; Scheiber, J.; Ritter, C.A.; Lerch, M.M.; Mayerle, J. Drug-Induced Pancreatitis. Curr. Gastroenterol. Rep. 2012, 14, 131–138. [Google Scholar] [CrossRef]
- Miyazaki, K.; Yoshimura, Y.; Miyata, N.; Sasaki, H.; Shiba, A.; Aga, M.; Hamakawa, Y.; Taniguchi, Y.; Misumi, Y.; Agemi, Y.; et al. Acute pancreatitis or severe increase in pancreatic enzyme levels following remdesivir administration in COVID 19 patients: An observational study. Sci. Rep. 2022, 12, 5323. [Google Scholar] [CrossRef]
- McArthur, K.E. Review article: Drug-induced pancreatitis. Aliment Pharmacol Ther. 1996, 10, 23–38. [Google Scholar] [CrossRef] [PubMed]
- Mallory, A.; Kern, F., Jr. Drug-Induced Pancreatitis: A critical review. Gastroenterology 1980, 78, 813–820. [Google Scholar] [CrossRef] [PubMed]
- Correia de Sá, T.; Soares, C.; Rocha, M. Acute pancreatitis and COVID-19: A literature review. World J. Gastrointest. Surg. 2021, 13, 574–584. [Google Scholar] [CrossRef] [PubMed]
- Balani, A.R.; Grendell, J.H. Drug-Induced Pancreatitis: Incidence, management and prevention. Drug Saf. 2008, 31, 823–837. [Google Scholar] [CrossRef] [PubMed]
- Badalov, N.; Baradarian, R.; Iswara, K.; Li, J.; Steinberg, W.; Tenner, S. Drug-Induced Acute Pancreatitis: An Evidence-Based Review. Clin. Gastroenterol. Hepatol. 2007, 5, 648–661. [Google Scholar] [CrossRef]
- Tarighi, P.; Eftekhari, S.; Chizari, M.; Sabernavaei, M.; Jafari, D.; Mirzabeigi, P. A review of potential suggested drugs for coronavirus disease (COVID-19) treatment. Eur. J. Pharmacol. 2021, 895, 173890. [Google Scholar] [CrossRef]
- Noreen, S.; Maqbool, I.; Madni, A. Dexamethasone: Therapeutic potential, risks, and future projection during COVID-19 pandemic. Eur. J. Pharmacol. 2021, 894, 173854. [Google Scholar] [CrossRef]
- Chen, F.; Hao, L.; Zhu, S.; Yang, X.; Shi, W.; Zheng, K.; Wang, T.; Chen, H. Potential Adverse Effects of Dexamethasone Therapy on COVID-19 Patients: Review and Recommendations. Infect. Dis. Ther. 2021, 10, 1907–1931. [Google Scholar] [CrossRef]
- RECOVERY Collaborative Group; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef]
- Karlafti, E.; Paramythiotis, D.; Pantazi, K.; Georgakopoulou, V.E.; Kaiafa, G.; Papalexis, P.; Protopapas, A.A.; Ztriva, E.; Fyntanidou, V.; Savopoulos, C. Drug-Induced Liver Injury in Hospitalized Patients during SARS-CoV-2 Infection. Medicina 2022, 58, 1848. [Google Scholar] [CrossRef]
- Bruscoli, S.; Puzzovio, P.G.; Zaimi, M.; Tiligada, K.; Levi-Schaffer, F.; Riccardi, C. Glucocorticoids and COVID-19. Pharmacol. Res. 2022, 185, 106511. [Google Scholar] [CrossRef] [PubMed]
- Nango, D.; Hirose, Y.; Goto, M.; Echizen, H. Analysis of the Association of Administration of various glucocorticoids with development of acute pancreatitis using US Food and Drug Administration adverse event reporting system (FAERS). J. Pharm. Health Care Sci. 2019, 5, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Capuano, A.; Scavone, C.; Racagni, G.; Scaglione, F.; Italian Society of Pharmacology. NSAIDs in patients with viral infections, including Covid-19: Victims or perpetrators? Pharmacol. Res. 2020, 157, 104849. [Google Scholar] [CrossRef]
- Pezzilli, R.; Morselli-Labate, A.M.; Corinaldesi, R. NSAIDs and Acute Pancreatitis: A Systematic Review. Pharmaceuticals 2010, 3, 558–571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samanta, J.; Gupta, R.; Singh, M.P.; Patnaik, I.; Kumar, A.; Kochhar, R. Coronavirus disease 2019 and the pancreas. Pancreatology 2020, 20, 1567–1575. [Google Scholar] [CrossRef]
- Qomara, W.F.; Primanissa, D.N.; Amalia, S.H.; Purwadi, F.V.; Zakiyah, N. Effectiveness of Remdesivir, Lopinavir/Ritonavir, and Favipiravir for COVID-19 Treatment: A Systematic Review. Int. J. Gen. Med. 2021, 14, 8557–8571. [Google Scholar] [CrossRef]
- Meini, S.; Pagotto, A.; Longo, B.; Vendramin, I.; Pecori, D.; Tascini, C. Role of Lopinavir/Ritonavir in the Treatment of Covid-19: A Review of Current Evidence, Guideline Recommendations, and Perspectives. J. Clin. Med. 2020, 9, 2050. [Google Scholar] [CrossRef]
- Rubel, A.R.; Chong, P.L.; Abdullah, M.S.; Asli, R.; Momin, R.N.; Mani, B.I.; Chong, V.H. Lipemic serum in patients with Coronavirus Disease 2019 (COVID-19) undergoing treatment. J. Med. Virol. 2020, 92, 1810–1811. [Google Scholar] [CrossRef]
- Kurihara, Y.; Maruhashi, T.; Wada, T.; Osada, M.; Oi, M.; Yamaoka, K.; Asari, Y. Pancreatitis in a Patient with Severe Coronavirus Disease Pneumonia Treated with Veno-venous Extracorporeal Membrane Oxygenation. Intern. Med. 2020, 59, 2903–2906. [Google Scholar] [CrossRef]
- Flaig, T.; Douros, A.; Bronder, E.; Klimpel, A.; Kreutz, R.; Garbe, E. Tocilizumab-induced pancreatitis: Case report and review of data from the FDA Adverse Event Reporting System. J. Clin. Pharm. Ther. 2016, 41, 718–721. [Google Scholar] [CrossRef]
- Morrison, A.R.; Johnson, J.M.; Ramesh, M.; Bradley, P.; Jennings, J.; Smith, Z.R. Acute hypertriglyceridemia in patients with COVID-19 receiving tocilizumab. J. Med. Virol. 2020, 2, 1791–1792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Popp, M.; Stegemann, M.; Riemer, M.; Metzendorf, M.I.; Romero, C.S.; Mikolajewska, A.; Kranke, P.; Meybohm, P.; Skoetz, N.; Weibel, S. Antibiotics for the treatment of COVID-19. Cochrane Database Syst. Rev. 2021, 10, CD015025. [Google Scholar] [CrossRef] [PubMed]
- Valle, C.; Martin, B.; Touret, F.; Shannon, A.; Canard, B.; Guillemot, J.C.; Coutard, B.; Decroly, E. Drugs against SARS-CoV-2: What do we know about their mode of action? Rev. Med. Virol. 2020, 30, 1–10. [Google Scholar] [CrossRef]
- Poschet, J.F.; Perkett, E.A.; Timmins, G.S.; Deretic, V. Azithromycin and ciprofloxacin have a chloroquine-like effect on respiratory epithelial cells. bioRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Ehsan, P.; Haseeb, M.; Khan, Z.; Rehan, A.; Singh, R. Coronavirus Disease 2019 Pneumonia and Acute Pancreatitis in a Young Girl. Cureus 2021, 13, e15374. [Google Scholar] [CrossRef]
- Marciniec, K.; Beberok, A.; Pecak, P.; Boryczka, S.; Wrześniok, D. Ciprofloxacin and moxifloxacin could interact with SARS-CoV-2 protease: Preliminary in silico analysis. Pharmacol. Rep. 2020, 72, 1553–1561. [Google Scholar] [CrossRef]
- Thai, T.; Salisbury, B.H.; Zito, P.M. Ciprofloxacin; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Karampela, I.; Dalamaga, M. Could Respiratory Fluoroquinolones, Levofloxacin and Moxifloxacin, Prove to be Beneficial as an Adjunct Treatment in COVID-19? Arch. Med. Res. 2020, 51, 741–742. [Google Scholar] [CrossRef]
- Malek, A.E.; Granwehr, B.P.; Kontoyiannis, D.P. Doxycycline as a potential partner of COVID-19 therapies. IDCases 2020, 21, e00864. [Google Scholar] [CrossRef]
- Yates, P.A.; Newman, S.A.; Oshry, L.J.; Glassman, R.H.; Leone, A.M.; Reichel, E. Doxycycline treatment of high-risk COVID-19-positive patients with comorbid pulmonary disease. Ther. Adv. Respir. Dis. 2020, 14, 1753466620951053. [Google Scholar] [CrossRef]
- Shah, N.; Razzano, A.; Grendell, J. Doxycycline Induced Severe Acute Pancreatitis: A Rare Finding To A Common Medication. BMJ Case Rep. 2021, 14, e239640. [Google Scholar] [CrossRef]
- Kenes, M.T.; McSparron, J.I.; Marshall, V.D.; Renius, K.; Hyzy, R.C. Propofol-Associated Hypertriglyceridemia in Coronavirus Disease 2019 Versus Noncoronavirus Disease 2019 Acute Respiratory Distress Syndrome. Crit. Care Expl. 2020, 2, e0303. [Google Scholar] [CrossRef] [PubMed]
- Kermad, A.; Speltz, J.; Danziger, G.; Mertke, T.; Bals, R.; Volk, T.; Lepper, P.M.; Meiser, A. Comparison of isoflurane and propofol sedation in critically ill COVID 19 patients—A retrospective chart review. J. Anesth. 2021, 35, 625–632. [Google Scholar] [CrossRef] [PubMed]
- Ghajarzadeh, K.; Fard, M.M.; Otaghvar, H.A.; Faiz, S.R.F.; Dabbagh, A.; Mohseni, M.; Kashani, S.S.; Fard, A.M.M.; Alebouyeh, M.R. Effects of Dexmedetomidine and Propofol on Hemodynamic Stability and Ventilation Time in Patients Suffering COVID-19 Admitting to Intensive Care Units. Ann. Rom. Soc. Cell Biol. 2021, 25, 2457–2465. [Google Scholar]
- Elkhouly, M.A.; Salazar, M.J.; Simons-Linares, C.R. Hypertriglyceridemia-Associated Drug-Induced Acute Pancreatitis. Pancreas 2019, 48, 22–35. [Google Scholar] [CrossRef]
- Coelingh Bennink, H.J.T.; Foidart, J.M.; Debruyne, F.M.J. Treatment of Serious COVID-19 with Testosterone Suppression and High-dose Estrogen Therapy. Eur. Urol. 2021, 80, 523–525. [Google Scholar] [CrossRef]
- Youn, J.Y.; Zhang, Y.; Wu, Y.; Cannesson, M.; Cai, H. Therapeutic application of estrogen for COVID-19: Attenuation of SARS-CoV-2 spike protein and IL-6 stimulated, ACE2-dependent NOX2 activation, ROS production and MCP-1 upregulation in endothelial cells. Redox Biol. 2021, 46, 102099. [Google Scholar] [CrossRef]
- Fallahzadeh, M.; Pourhoseingholi, M.A.; Boroujeni, M.G.; Besharati, S.; Mardani, M.; Shabani, M.; Shokouhi, S.; Amirdosara, M.; Hajiesmaeili, M.; Gachkar, L.; et al. Study of the effects of interferon β-1a on hospitalized patients with COVID-19: SBMU Taskforce on the COVIFERON study. J. Med. Virol. 2022, 94, 1488–1493. [Google Scholar] [CrossRef]
- Rahmani, H.; Davoudi-Monfared, E.; Nourian, A.; Khalili, H.; Hajizadeh, N.; Jalalabadi, N.Z.; Fazeli, M.R.; Ghazaeian, M.; Yekaninejad, M.S. Interferon β-1b in treatment of severe COVID-19: A randomized clinical trial. Int. Immunopharmacol. 2020, 88, 106903. [Google Scholar] [CrossRef] [PubMed]
- Sestili, P.; Fimognari, C. Paracetamol use in COVID-19: Friend or enemy? Preprints 2020, 2020080186. Available online: https://www.preprints.org/manuscript/202008.0186/v1 (accessed on 20 December 2022).
- Ceranowicz, P.; Dembinski, A.; Warzecha, Z.; Dembinski, M.; Cieszkowski, J.; Rembiasz, K.; Konturek, S.J.; Kusnierz-Cabala, B.; Tomaszewska, R.; Pawlik, W.W. Protective and therapeutic effect of heparin in acute pancreatitis. J. Physiol. Pharmacol. 2008, 59, 103–125. [Google Scholar]
- Ketwaroo, G.; Sealock, R.J.; Freedman, S.; Hart, P.A.; Othman, M.; Wassef, W.; Banks, P.; Vege, S.S.; Gardner, T.; Yadav, D.; et al. Quality of Care Indicators in Patients with Acute Pancreatitis. Dig. Dis. Sci. 2019, 64, 2514–2526. [Google Scholar] [CrossRef] [PubMed]
- Vivian, E.; Cler, L.; Conwell, D.; Coté, G.A.; Dickerman, R.; Freeman, M.; Gardner, T.B.; Hawes, R.H.; Kedia, P.; Krishnamoorthi, R.; et al. Acute Pancreatitis Task Force on Quality: Development of Quality Indicators for Acute Pancreatitis Management. Am. J. Gastroenterol. 2019, 114, 1322–1342. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Medication | Type | Badalov Classification | References |
|---|---|---|---|
| Dexamethasone | Corticosteroids | Ib | [25,26] |
| Glucocorticosteroids | Corticosteroids | N/A | [26] |
| Non-steroidal anti-inflammatory drugs (NSAIDs) | Non-steroidal anti-inflammatory drugs (NSAIDs) | N/A | [15] |
| Lopinavir/ritonavir | Antiviral drug | IV | [3,12] |
| Remdesivir | Antiviral drug | N/A | [3,26] |
| Tocilizumab | Monoclonal antibody | N/A | [3] |
| Azithromycin | Antibiotic | N/A | [26] |
| Ciprofloxacin | Antibiotic | III | [16] |
| Doxycycline | Antibiotic | III | [10,16] |
| Propofol | Anesthetic agent | II | [25] |
| Estrogens | Hormones | Ib | [25] |
| Interferons | Antiviral agent | III | [25,26] |
| Acetaminophen | Antipyretic | II | [25] |
| Enalapril | Antihypertensive agent | Ia | [25] |
| Lisinopril | Antihypertensive agent | III | [25] |
| Asparginase | Enzyme | II | [25] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paramythiotis, D.; Karlafti, E.; Veroplidou, K.; Fafouti, M.; Kaiafa, G.; Netta, S.; Michalopoulos, A.; Savopoulos, C. Drug-Induced Acute Pancreatitis in Hospitalized COVID-19 Patients. Diagnostics 2023, 13, 1398. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics13081398
Paramythiotis D, Karlafti E, Veroplidou K, Fafouti M, Kaiafa G, Netta S, Michalopoulos A, Savopoulos C. Drug-Induced Acute Pancreatitis in Hospitalized COVID-19 Patients. Diagnostics. 2023; 13(8):1398. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics13081398
Chicago/Turabian StyleParamythiotis, Daniel, Eleni Karlafti, Kalliopi Veroplidou, Maria Fafouti, Georgia Kaiafa, Smaro Netta, Antonios Michalopoulos, and Christos Savopoulos. 2023. "Drug-Induced Acute Pancreatitis in Hospitalized COVID-19 Patients" Diagnostics 13, no. 8: 1398. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics13081398