
Deep Learning-Based Algorithm for Automatic Detection of Pulmonary Embolism in Chest CT Angiograms

 , , ,
, , ,  , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
2.1. AI Algorithm: General Architecture, Training, and Testing
2.2. Data Selection for Validation
2.3. The Ground Truth
2.4. Post-Processing
2.5. Statistical Analysis
3. Results
3.1. Data Distribution
3.2. Ground Truth Results
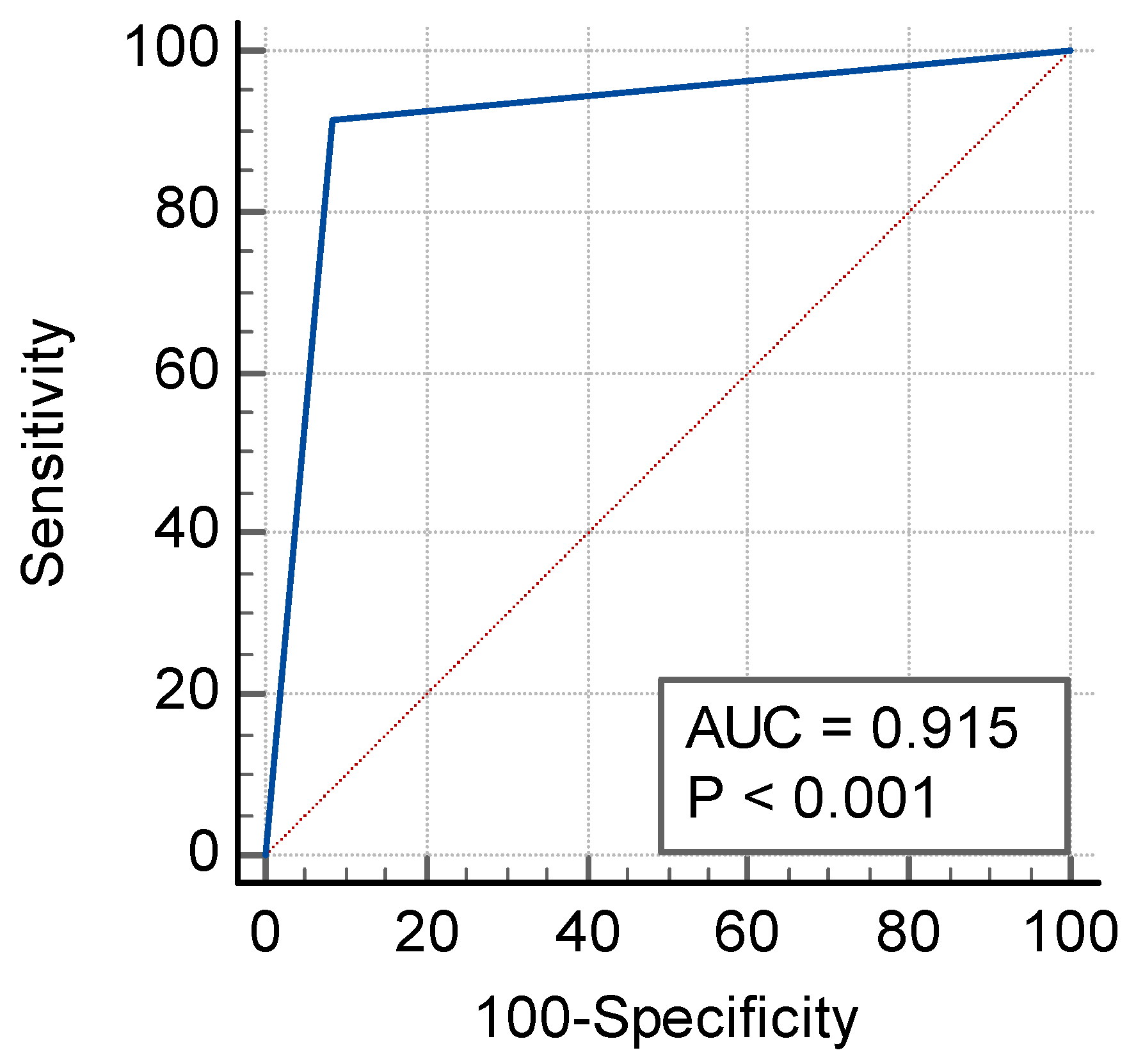
3.3. Sensitivity, Specificity, AUC, Accuracy, and MCC
3.4. Positive and Negative Predictive Values
3.5. Stratified Analysis
3.6. Time-to-Notification
4. Discussion
- To help radiologists to prioritize exams with a high suspicion of pulmonary embolism (PE), a deep learning (DL) algorithm was trained on 4795 CT angiograms from multiple U.S. clinical centers and adequately distributed in terms of vendors, patient age, slice thickness, and kVp.
- In a retrospective, multicenter, and blinded standalone validation study, the DL algorithm achieved an area under the receiver operating characteristic curve (AUC) of 0.92 [95% CI: 0.88–0.94] (p < 0.0001).
- Both the training and validation of the algorithm on data from multiple clinical sites through the U.S. and acquired on multiple scanner models promotes the generalizability of its use.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Horlander, K.T.; Mannino, D.M.; Leeper, K.V. Pulmonary embolism mortality in the United States, 1979–1998: An analysis using multiple-cause mortality data. Arch. Intern. Med. 2003, 163, 1711–1717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clemens, S.; Leeper, K.V., Jr. Newer modalities for detection of pulmonary emboli. Am. J. Med. 2007, 120, S2–S12. [Google Scholar] [CrossRef] [PubMed]
- Donato, A.A.; Scheirer, J.J.; Atwell, M.S.; Gramp, J.; Duszak, R., Jr. Clinical outcomes in patients with suspected acute pulmonary embolism and negative helical computed tomographic results in whom anticoagulation was withheld. Arch. Intern. Med. 2003, 163, 2033–2038. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dalen, J.E. Pulmonary embolism: What have we learned since Virchow? Natural history, pathophysiology, and diagnosis. Chest 2002, 122, 1440–1456. [Google Scholar] [CrossRef] [Green Version]
- Righini, M.; Robert-Ebadi, H.; Le Gal, G. Diagnosis of acute pulmonary embolism. J. Thromb. Haemost. 2017, 15, 1251–1261. [Google Scholar] [CrossRef] [Green Version]
- Shujaat, A.; Shapiro, J.M.; Eden, E. Utilization of CT Pulmonary Angiography in Suspected Pulmonary Embolism in a Major Urban Emergency Department. Pulm. Med. 2013, 2013, 915213. [Google Scholar] [CrossRef] [PubMed]
- Wittram, C.; Maher, M.M.; Yoo, A.J.; Kalra, M.K.; Shepard, J.A.; McLoud, T.C. CT angiography of pulmonary embolism: Diagnostic criteria and causes of misdiagnosis. Radiographics 2004, 24, 1219–1238. [Google Scholar] [CrossRef]
- Prologo, J.D.; Gilkeson, R.C.; Diaz, M.; Asaad, J. CT pulmonary angiography: A comparative analysis of the utilization patterns in emergency department and hospitalized patients between 1998 and 2003. AJR Am. J. Roentgenol. 2004, 183, 1093–1096. [Google Scholar] [CrossRef]
- Chandra, S.; Sarkar, P.K.; Chandra, D.; Ginsberg, N.E.; Cohen, R.I. Finding an alternative diagnosis does not justify increased use of CT-pulmonary angiography. BMC Pulm. Med. 2013, 13, 9. [Google Scholar] [CrossRef] [Green Version]
- Hutchinson, B.D.; Navin, P.; Marom, E.M.; Truong, M.T.; Bruzzi, J.F. Overdiagnosis of Pulmonary Embolism by Pulmonary CT Angiography. AJR Am. J. Roentgenol. 2015, 205, 271–277. [Google Scholar] [CrossRef]
- McDonald, R.J.; Schwartz, K.M.; Eckel, L.J.; Diehn, F.E.; Hunt, C.H.; Bartholmai, B.J.; Erickson, B.J.; Kallmes, D.F. The effects of changes in utilization and technological advancements of cross-sectional imaging on radiologist workload. Acad. Radiol. 2015, 22, 1191–1198. [Google Scholar] [CrossRef] [PubMed]
- Rohatgi, S.; Hanna, T.N.; Sliker, C.W.; Abbott, R.M.; Nicola, R. After-Hours Radiology: Challenges and Strategies for the Radiologist. AJR Am. J. Roentgenol. 2015, 205, 956–961. [Google Scholar] [CrossRef] [PubMed]
- Hanna, T.N.; Zygmont, M.E.; Peterson, R.; Theriot, D.; Shekhani, H.; Johnson, J.O.; Krupinski, E.A. The Effects of Fatigue From Overnight Shifts on Radiology Search Patterns and Diagnostic Performance. J. Am. Coll. Radiol. 2018, 15, 1709–1716. [Google Scholar] [CrossRef]
- Yavas, U.S.; Calisir, C.; Ozkan, I.R. The interobserver agreement between residents and experienced radiologists for detecting pulmonary embolism and DVT with using CT pulmonary angiography and indirect CT venography. Korean J. Radiol. 2008, 9, 498–502. [Google Scholar] [CrossRef] [Green Version]
- Rufener, S.L.; Patel, S.; Kazerooni, E.A.; Schipper, M.; Kelly, A.M. Comparison of on-call radiology resident and faculty interpretation of 4- and 16-row multidetector CT pulmonary angiography with indirect CT venography. Acad. Radiol. 2008, 15, 71–76. [Google Scholar] [CrossRef]
- Joshi, R.; Wu, K.; Kaicker, J.; Choudur, H. Reliability of on-call radiology residents’ interpretation of 64-slice CT pulmonary angiography for the detection of pulmonary embolism. Acta Radiol. 2014, 55, 682–690. [Google Scholar] [CrossRef]
- Kligerman, S.J.; Mitchell, J.W.; Sechrist, J.W.; Meeks, A.K.; Galvin, J.R.; White, C.S. Radiologist Performance in the Detection of Pulmonary Embolism: Features that Favor Correct Interpretation and Risk Factors for Errors. J. Thorac. Imaging 2018, 33, 350–357. [Google Scholar] [CrossRef]
- Das, M.; Mühlenbruch, G.; Helm, A.; Bakai, A.; Salganicoff, M.; Stanzel, S.; Liang, J.; Wolf, M.; Günther, R.W.; Wildberger, J.E. Computer-aided detection of pulmonary embolism: Influence on radiologists’ detection performance with respect to vessel segments. Eur. Radiol. 2008, 18, 1350–1355. [Google Scholar] [CrossRef] [PubMed]
- Eng, J.; Krishnan, J.A.; Segal, J.B.; Bolger, D.T.; Tamariz, L.J.; Streiff, M.B.; Jenckes, M.W.; Bass, E.B. Accuracy of CT in the diagnosis of pulmonary embolism: A systematic literature review. AJR Am. J. Roentgenol. 2004, 183, 1819–1827. [Google Scholar] [CrossRef]
- Huang, S.C.; Pareek, A.; Seyyedi, S.; Banerjee, I.; Lungren, M.P. Fusion of medical imaging and electronic health records using deep learning: A systematic review and implementation guidelines. NPJ Digit. Med. 2020, 3, 136. [Google Scholar] [CrossRef]
- Tajbakhsh, N.; Shin, J.Y.; Gotway, M.B.; Liang, J. Computer-aided detection and visualization of pulmonary embolism using a novel, compact, and discriminative image representation. Med. Image Anal. 2019, 58, 101541. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Liu, M.; Guo, X.; Zhang, P.; Zhang, L.; Zhang, R.; Kang, H.; Zhai, Z.; Tao, X.; Wan, J.; et al. Evaluation of acute pulmonary embolism and clot burden on CTPA with deep learning. Eur. Radiol. 2020, 30, 3567–3575. [Google Scholar] [CrossRef] [PubMed]
- Weikert, T.; Winkel, D.J.; Bremerich, J.; Stieltjes, B.; Parmar, V.; Sauter, A.W.; Sommer, G. Automated detection of pulmonary embolism in CT pulmonary angiograms using an AI-powered algorithm. Eur. Radiol. 2020, 30, 6545–6553. [Google Scholar] [CrossRef] [PubMed]
- Huhtanen, H.; Nyman, M.; Mohsen, T.; Virkki, A.; Karlsson, A.; Hirvonen, J. Automated detection of pulmonary embolism from CT-angiograms using deep learning. BMC Med. Imaging 2022, 22, 43. [Google Scholar] [CrossRef]
- Ajmera, P.; Kharat, A.; Seth, J.; Rathi, S.; Pant, R.; Gawali, M.; Kulkarni, V.; Maramraju, R.; Kedia, I.; Botchu, R.; et al. A deep learning approach for automated diagnosis of pulmonary embolism on computed tomographic pulmonary angiography. BMC Med. Imaging 2022, 22, 195. [Google Scholar] [CrossRef]
- Soffer, S.; Klang, E.; Shimon, O.; Barash, Y.; Cahan, N.; Greenspana, H.; Konen, E. Deep learning for pulmonary embolism detection on computed tomography pulmonary angiogram: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 15814. [Google Scholar] [CrossRef]
- Cheikh, A.; Gorincour, G.; Nivet, H.; May, J.; Seux, M.; Calame, P.; Thomson, V.; Delabrousse, E.; Crombé, A. How artificial intelligence improves radiological interpretation in suspected pulmonary embolism. Eur. Radiol. 2022, 32, 5831–5842. [Google Scholar] [CrossRef]
- Carrier, M.; Klok, F.A. Symptomatic subsegmental pulmonary embolism: To treat or not to treat? Hematol. Am. Soc. Hematol. Educ. Program. 2017, 1, 237–241. [Google Scholar] [CrossRef] [Green Version]
- Sherk, W.; Stojanovska, J. Role of Clinical Decision Tools in the Diagnosis of Pulmonary Embolism. AJR Am. J. Roentgenol. 2017, 208, W60–W70. [Google Scholar] [CrossRef]
- Roy, P.M.; Meyer, G.; Vielle, B.; Le Gall, C.; Verschuren, F.; Carpentier, F.; Leveau, P.; Furber, A.; EMDEPU Study Group. Appropriateness of diagnostic management and outcomes of suspected pulmonary embolism. Ann. Intern. Med. 2006, 144, 157–164. [Google Scholar] [CrossRef] [Green Version]
- Donohoo, J.H.; Mayo-Smith, W.W.; Pezzullo, J.A.; Egglin, T.K. Utilization patterns and diagnostic yield of 3421 consecutive multidetector row computed tomography pulmonary angiograms in a busy emergency department. J. Comput. Assist. Tomogr. 2008, 32, 421–425. [Google Scholar] [CrossRef] [PubMed]
- Mountain, D.; Keijzers, G.; Chu, K.; Joseph, A.; Read, C.; Blecher, G.; Furyk, J.; Bharat, C.; Velusamy, K.; Munro, A.; et al. Rates of Pulmonary Emboli (PE) and Sub-Segmental PE with Modern Computed Tomographic Pulmonary Angiograms in Emergency Departments: A Multi-Center Observational Study Finds Significant Yield Variation, Uncorrelated with Use or Small PE Rates. PLoS ONE 2016, 11, e0166483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dalen, J.E.; Waterbrook, A.L. Why Are Nearly All CT Pulmonary Angiograms for Suspected Pulmonary Embolism Negative? Am. J. Med. 2017, 130, 247–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, X.; Ferguson, E.; Jiang, X.; Savitz, S.I.; Shams, S. A multitask deep learning approach for pulmonary embolism detection and identification. Sci. Rep. 2022, 12, 13087. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.C.; Pareek, A.; Zamanian, R.; Barnejee, I.; Lungren, M.P. Multimodal fusion with deep neural networks for leveraging CT imaging and electronic health record: A case-study in pulmonary embolism detection. Sci. Rep. 2020, 10, 22147. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Acquisition Parameters |
|---|
| Matrix size ≥ 512 × 512 (rectangular matrix accepted) |
| Axial acquisition only |
| Slice thickness ≤ 2.5 mm with no gap between successive slices |
| Radiation dose parameters: 60 kVp to 160 kVp |
| Reconstruction diameter above 200 mm |
| Contrast intensity: Minimum opacification the in the main pulmonary artery (mPA) = 180 HU (Hounsfield units) |
| Contrast timing: Minimum opacification ratio between the mPA and the ascending aorta = 0.95 |
| Soft tissue reconstruction kernel |
| Statistical Findings | |||
|---|---|---|---|
| TP | 170 | Sensitivity [95% CI] | 91.4% [86.4–95.0%] |
| FN | 16 | Specificity [95% CI] | 91.5% [86.8–95.0%] |
| TN | 184 | Accuracy [95% CI] | 91.5% [88.2–94.1%] |
| FP | 17 | AUC [95% CI] | 0.92 * [0.88–0.94] |
| Prevalence (%) | CINA—PE Positive Predictive Value (%) | CINA—PE Negative Predictive Value (%) |
|---|---|---|
| 10 | 54.6 | 99.0 |
| 15 | 65.6 | 98.4 |
| 20 | 73.0 | 97.7 |
| 25 | 78.3 | 97.0 |
| 30 | 82.2 | 96.1 |
| 35 | 85.3 | 95.2 |
| 40 | 87.8 | 94.1 |
| 45 | 89.8 | 92.9 |
| 50 | 91.5 | 91.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grenier, P.A.; Ayobi, A.; Quenet, S.; Tassy, M.; Marx, M.; Chow, D.S.; Weinberg, B.D.; Chang, P.D.; Chaibi, Y. Deep Learning-Based Algorithm for Automatic Detection of Pulmonary Embolism in Chest CT Angiograms. Diagnostics 2023, 13, 1324. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics13071324
Grenier PA, Ayobi A, Quenet S, Tassy M, Marx M, Chow DS, Weinberg BD, Chang PD, Chaibi Y. Deep Learning-Based Algorithm for Automatic Detection of Pulmonary Embolism in Chest CT Angiograms. Diagnostics. 2023; 13(7):1324. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics13071324
Chicago/Turabian StyleGrenier, Philippe A., Angela Ayobi, Sarah Quenet, Maxime Tassy, Michael Marx, Daniel S. Chow, Brent D. Weinberg, Peter D. Chang, and Yasmina Chaibi. 2023. "Deep Learning-Based Algorithm for Automatic Detection of Pulmonary Embolism in Chest CT Angiograms" Diagnostics 13, no. 7: 1324. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics13071324