Cognitive and Neuropsychiatric Profiles in Idiopathic Rapid Eye Movement Sleep Behavior Disorder and Parkinson’s Disease

 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Sociodemografic And Clinical Assessment
2.3. Neuropsychological and Neuropsychiatric Evaluation
2.4. Statistical Analysis
3. Results
3.1. Sociodemographic and Clinical Characteristics
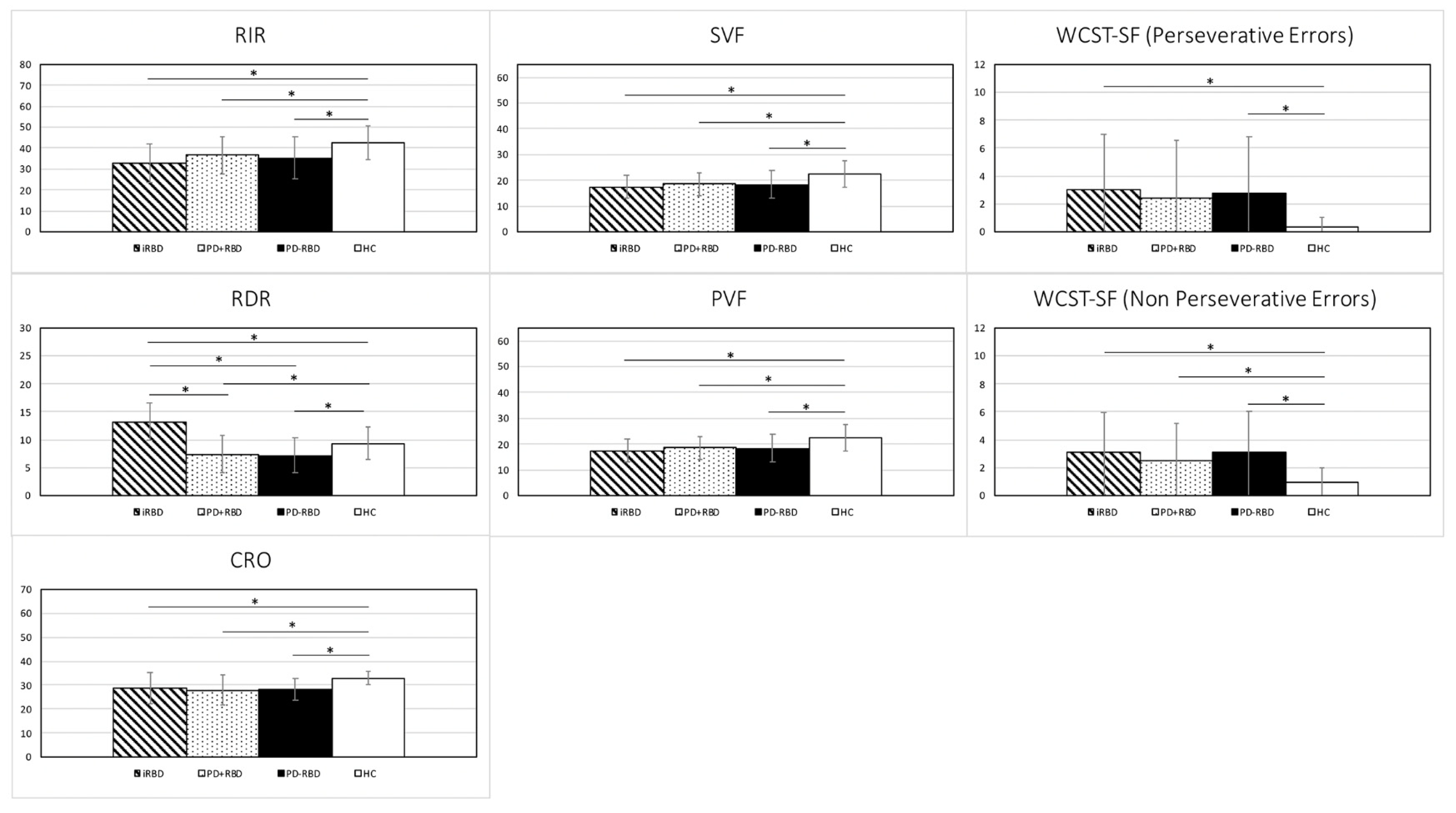
3.2. Neuropsychological Assessment
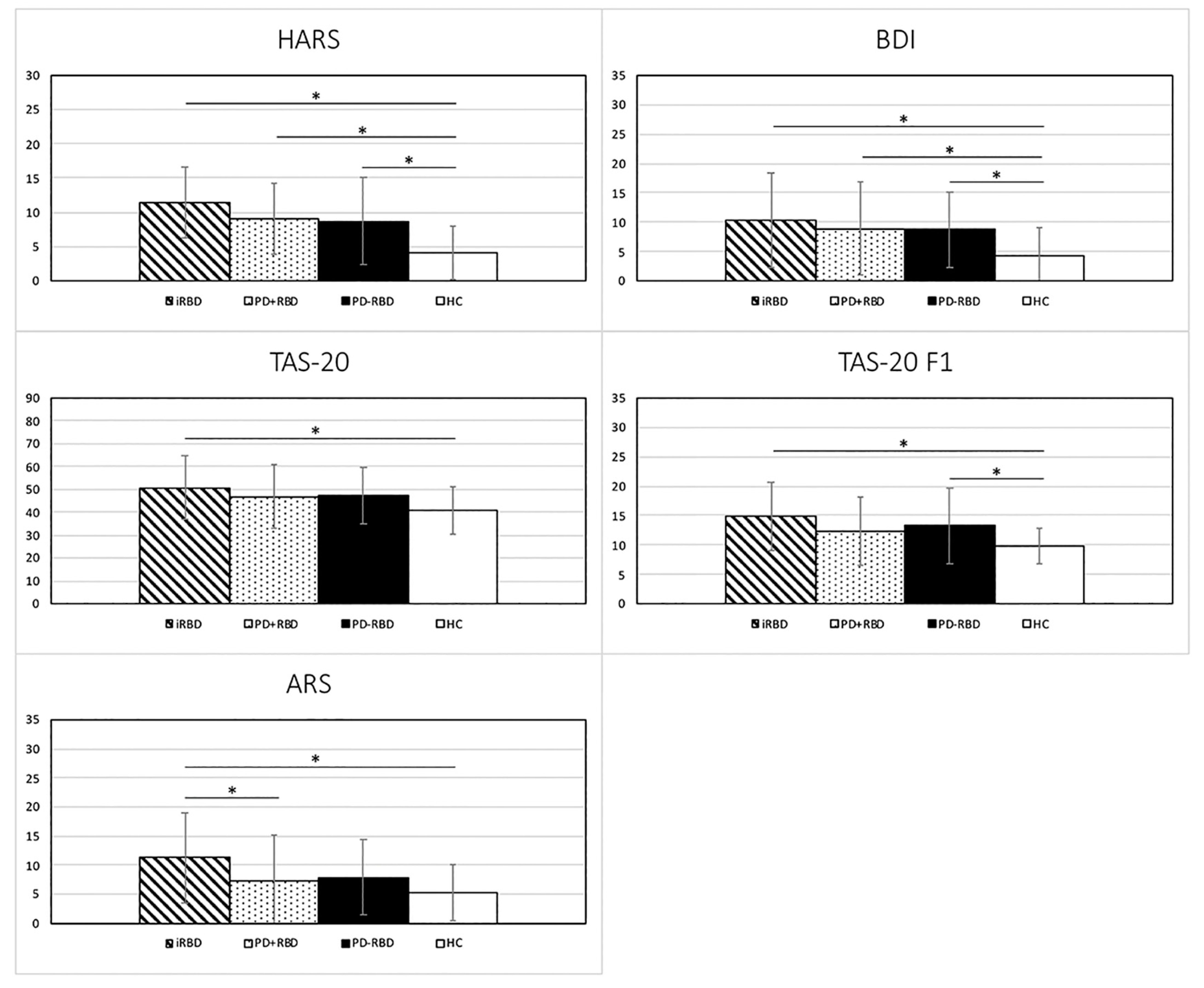
3.3. Neuropsychiatric Assessment
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, Y.; Kim, Y.E.; Park, E.O.; Shin, C.W.; Kim, H.J.; Jeon, B. REM sleep behavior disorder portends poor prognosis in Parkinson’s disease: A systematic review. J. Clin. Neurosci. 2018, 47, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Zhou, Z.; Jia, S.; Hou, C.; Zheng, W.; Rong, P.; Jiao, J. Cognitive study on Chinese patients with idiopathic REM sleep behavior disorder. J. Neurol. Sci. 2016, 366, 82–86. [Google Scholar] [CrossRef] [PubMed]
- Postuma, R.B.; Iranzo, A.; Hu, M.; Högl, B.; Boeve, B.F.; Manni, R.; Oertel, W.H.; Arnulf, I.; Ferini-Strambi, L.; Puligheddu, M.; et al. Risk and predictors of dementia and parkinsonism in idiopathic REM sleep behaviour disorder: A multicentre study. Brain 2019, 142, 744–759. [Google Scholar] [CrossRef] [PubMed]
- Chiu, H.F.; Wing, Y.K.; Lam, L.C.; Li, S.W.; Lum, C.M.; Leung, T.; Ho, C.K. Sleep-related injury in the elderly—An epidemiological study in Hong Kong. Sleep 2000, 23, 513–517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoritaka, A.; Ohizumi, H.; Tanaka, S.; Hattori, N. Parkinson’s disease with and without REM sleep behaviour disorder: Are there any clinical differences? Eur. Neurol. 2009, 61, 164–170. [Google Scholar] [CrossRef]
- Postuma, R.B.; Aarsland, D.; Barone, P.; Burn, D.J.; Hawkes, C.H.; Oertel, W.; Ziemssen, T. Identifying prodromal Parkinson’s disease: Pre-motor disorders in Parkinson’s disease. Mov. Disord. 2012, 27, 617–626. [Google Scholar] [CrossRef]
- Lin, Y.Q.; Chen, S.D. RBD: A red flag for cognitive impairment in Parkinson’s disease? Sleep Med. 2018, 44, 38–44. [Google Scholar] [CrossRef]
- Postuma, R.B.; Gagnon, J.F.; Vendette, M.; Montplaisir, J.Y. Markers of neurodegeneration in idiopathic rapid eye movement sleep behaviour disorder and Parkinson’s disease. Brain 2009, 132, 3298–3307. [Google Scholar] [CrossRef] [Green Version]
- Fantini, M.L.; Gagnon, J.F.; Petit, D.; Rompré, S.; Décary, A.; Carrier, J.; Montplaisir, J. Slowing of electroencephalogram in rapid eye movement sleep behavior disorder. Ann. Neurol. 2003, 53, 774–780. [Google Scholar] [CrossRef]
- Iranzo, A.; Lomeña, F.; Stockner, H.; Valldeoriola, F.; Vilaseca, I.; Salamero, M.; Molinuevo, J.L.; Serradell, M.; Duch, J.; Pavía, J.; et al. Decreased striatal dopamine transporter uptake and substantia nigra hyperechogenicity as risk markers of synucleinopathy in patients with idiopathic rapid-eye-movement sleep behaviour disorder: A prospective study. Lancet Neurol. 2010, 9, 1070–1077. [Google Scholar] [CrossRef]
- Miyamoto, T.; Miyamoto, M.; Inoue, Y.; Usui, Y.; Suzuki, K.; Hirata, K. Reduced cardiac 123I-MIBG scintigraphy in idiopathic REM sleep behavior disorder. Neurology 2006, 67, 2236–2238. [Google Scholar] [CrossRef] [PubMed]
- Plomhause, L.; Dujardin, K.; Boucart, M.; Herlin, V.; Defebvre, L.; Derambure, P.; Charley, C.M. Impaired visual perception in rapid eye movement sleep behavior disorder. Neuropsychology 2014, 28, 388–393. [Google Scholar] [CrossRef] [PubMed]
- Ferini-Strambi, L.; Di Gioia, M.R.; Castronovo, V.; Oldani, A.; Zucconi, M.; Cappa, S.F. Neuropsychological assessment in idiopathic REM sleep behavior disorder (RBD): Does the idiopathic form of RBD really exist? Neurology 2004, 62, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Fantini, M.L.; Farini, E.; Ortelli, P.; Zucconi, M.; Manconi, M.; Cappa, S.; Ferini-Strambi, L. Longitudinal Study of Cognitive Function in Idiopathic REM Sleep Behavior Disorder. Sleep 2011, 34, 619–625. [Google Scholar] [PubMed] [Green Version]
- Massicotte-Marquez, J.; Décary, A.; Gagnon, J.F.; Vendette, M.; Mathieu, A.; Postuma, R.B.; Carrier, J.; Montplaisir, J. Executive dysfunction and memory impairment in idiopathic REM sleep behavior disorder. Neurology 2008, 70, 1250–1257. [Google Scholar] [CrossRef]
- Delazer, M.; Högl, B.; Zamarian, L.; Wenter, J.; Ehrmann, L.; Gschliesser, V.; Brandauer, E.; Poewe, W.; Frauscher, B. Decision Making and Executive Functions in REM Sleep Behavior Disorder. Sleep 2012, 35, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Terzaghi, M.; Sinforiani, E.; Zucchella, C.; Zambrelli, E.; Pasotti, C.; Rustioni, V.; Manni, R. Cognitive performance in REM sleep behaviour disorder: A possible early marker of neurodegenerative disease? Sleep Med. 2008, 9, 343–351. [Google Scholar] [CrossRef]
- Rolinski, M.; Zokaei, N.; Baig, F.; Giehl, K.; Quinnell, T.; Zaiwalla, Z.; Mackay, C.E.; Husain, M.; Hu, M.T. Visual short-term memory deficits in REM sleep behaviour disorder mirror those in Parkinson’s disease. Brain 2016, 139, 47–53. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Wang, K.; Jia, S.; Zhou, Z.; Jin, Y.; Zhang, X.; Hou, C.; Zheng, W.; Rong, P.; Jiao, J. The prospective memory of patients with idiopathic REM sleep behavior disorder. Sleep Med. 2018, 47, 19–24. [Google Scholar] [CrossRef]
- Gagnon, J.F.; Vendette, M.; Postuma, R.B.; Desjardins, C.; Massicotte-Marquez, J.; Panisset, M.; Montplaisir, J. Mild cognitive impairment in rapid eye movement sleep behavior disorder and Parkinson’s disease. Ann. Neurol. 2009, 66, 39–47. [Google Scholar] [CrossRef]
- Marques, A.; Dujardin, K.; Boucart, M.; Pins, D.; Delliaux, M.; Defebvre, L.; Derambure, P.; Monaca, C. REM sleep behaviour disorder and visuoperceptive dysfunction: A disorder of the ventral visual stream? J. Neurol. 2010, 257, 383–391. [Google Scholar] [CrossRef] [PubMed]
- Vendette, M.; Gagnon, J.F.; Décary, A.; Massicotte-Marquez, J.; Postuma, R.B.; Doyon, J.; Panisset, M.; Montplaisir, J. REM sleep behavior disorder predicts cognitive impairment in Parkinson disease without dementia. Neurology 2007, 69, 1843–1849. [Google Scholar] [CrossRef] [PubMed]
- Barber, T.R.; Muhammed, K.; Drew, D.; Lawton, M.; Crabbe, M.; Rolinski, M.; Quinnell, T.; Zaiwalla, Z.; Ben-Shlomo, Y.; Husain, M.; et al. Apathy in rapid eye movement sleep behaviour disorder is common and under-recognized. Eur. J. Neurol. 2018, 25, 469-e32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barber, T.R.; Lawton, M.; Rolinski, M.; Evetts, S.; Baig, F.; Ruffmann, C.; Gornall, A.; Klein, J.C.; Lo, C.; Dennis, G.; et al. Prodromal Parkinsonism and Neurodegenerative Risk Stratification in REM Sleep Behavior Disorder. Sleep 2017, 40, zsx071. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Zhu, X.Y.; Zhang, X.J.; Kuo, S.H.; Ondo, W.G.; Wu, Y.C. Clinical features of Parkinson’s disease with and without rapid eye movement sleep behavior disorder. Transl. Neurodegener. 2017, 6, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neikrug, A.B.; Avanzino, J.A.; Liu, L.; Maglione, J.E.; Natarajan, L.; Corey-Bloom, J.; Palmer, B.W.; Loredo, J.S.; Ancoli-Israel, S. Parkinson’s disease and REM sleep behavior disorder result in increased non-motor symptoms. Sleep Med. 2014, 15, 959–966. [Google Scholar] [CrossRef] [Green Version]
- Bargiotas, P.; Ntafouli, M.; Lachenmayer, M.L.; Krack, P.; Schüpbach, W.M.M.; Bassetti, C.L.A. Apathy in Parkinson’s disease with REM sleep behavior disorder. J. Neurol. Sci. 2019, 399, 194–198. [Google Scholar] [CrossRef]
- Daniel, S.E.; Lees, A.J. Parkinson’s Disease Society Brain Bank, London: Overview and research. J. Neural Transm. Suppl. 1993, 39, 165–172. [Google Scholar]
- American Academy of Sleep Medicine. International Classification of Sleep Disorders, 3rd ed.; American Academy of Sleep Medicine: Darien, IL, USA, 2014. [Google Scholar]
- Emre, M.; Aarsland, D.; Brown, R.; Burn, D.J.; Duyckaerts, C.; Mizuno, Y.; Broe, G.A.; Cummings, J.; Dickson, D.W.; Gauthier, S.; et al. Clinical diagnostic criteria for dementia associated with Parkinson’s disease. Mov. Disord. 2007, 22, 1689–1707. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Iorio, M.; Spalletta, G.; Chiapponi, C.; Luccichenti, G.; Cacciari, C.; Orfei, M.D.; Caltagirone, C.; Piras, F. White matter hyperintensities segmentation: A new semi-automated method. Front. Aging Neurosci. 2013, 5, 76. [Google Scholar] [CrossRef] [Green Version]
- Assogna, F.; Pellicano, C.; Cravello, L.; Savini, C.; Pierantozzi, M.; Mercuri, B.; Caltagirone, C.; Pontieri, F.E.; Spalletta, G.; Stefani, A. Psychiatric profile of motor subtypes of de novo drug-naïve Parkinson’s disease patients. Brain Behav. 2018, 8, e01094. [Google Scholar] [CrossRef] [PubMed]
- Marelli, S.; Rancoita, P.M.; Giarrusso, F.; Galbiati, A.; Zucconi, M.; Oldani, A.; Di Serio, C.; Ferini-Strambi, L. National validation and proposed revision of REM sleep behavior disorder screening questionnaire (RBDSQ). J. Neurol. 2016, 263, 2470–2475. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.; Steer, R.A. Beck Depression Inventory Manual; The Psychological Corporation: San Antonio, TX, USA, 1987. [Google Scholar]
- Fernández-Arcos, A.; Iranzo, A.; Serradell, M.; Gaig, C.; Santamaria, J. The Clinical Phenotype of Idiopathic Rapid Eye Movement Sleep Behavior Disorder at Presentation: A Study in 203 Consecutive Patients. Sleep 2016, 39, 121–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kehagia, A.A.; Barker, R.A.; Robbins, T.W. Cognitive impairment in Parkinson’s disease: The dual syndrome hypothesis. Neurodegener. Dis. 2012, 11, 79–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scherfler, C.; Frauscher, B.; Schocke, M.; Iranzo, A.; Gschliesser, V.; Seppi, K.; Santamaria, J.; Tolosa, E.; Högl, B.; Poewe, W.; et al. White and gray matter abnormalities in idiopathic rapid eye movement sleep behavior disorder: A diffusion-tensor imaging and voxel-based morphometry study. Ann. Neurol. 2011, 69, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Pellicano, C.; Niccolini, F.; Wu, K.; O’Sullivan, S.S.; Lawrence, A.D.; Lees, A.J.; Piccini, P.; Politis, M. Morphometric changes in the reward system of Parkinson’s disease patients with impulse control disorders. J. Neurol. 2015, 262, 2653–2661. [Google Scholar] [CrossRef] [PubMed]
- Mazza, S.; Soucy, J.P.; Gravel, P.; Michaud, M.; Postuma, R.; Massicotte-Marquez, J.; Decary, A.; Montplaisir, J. Assessing whole brain perfusion changes in patients with REM sleep behavior disorder. Neurology 2006, 67, 1618–1622. [Google Scholar] [CrossRef]
- Massicotte-Marquez, J.; Carrier, J.; Décary, A.; Mathieu, A.; Vendette, M.; Petit, D.; Montplaisir, J. Slow-wave sleep and delta power in rapid eye movement sleep behavior disorder. Ann. Neurol. 2005, 57, 277–282. [Google Scholar] [CrossRef]
- Klinzing, J.G.; Niethard, N.; Born, J. Mechanisms of systems memory consolidation during sleep. Nat. Neurosci. 2019, 22, 1598–1610. [Google Scholar] [CrossRef]
- Schrag, A.; Taddei, R.N. Depression and Anxiety in Parkinson’s Disease. Int. Rev. Neurobiol. 2017, 133, 623–655. [Google Scholar]
- Goodarzi, Z.; Mele, B.; Guo, S.; Hanson, H.; Jette, N.; Patten, S.; Pringsheim, T.; Holroyd-Leduc, J. Guidelines for dementia or Parkinson’s disease with depression or anxiety: A systematic review. BMC Neurol. 2016, 16, 244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Godin, I.; Montplaisir, J.; Gagnon, J.-F.; Nielsen, T. Alexithymia Associated with Nightmare Distress in Idiopathic REM Sleep Behavior Disorder. Sleep 2013, 36, 1957–1962. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.J.; Kim, S.J.; Lee, S.-A. Severity of Idiopathic Rapid Eye Movement Sleep Behavior Disorder Correlates with Depression and Alexithymia. Sleep Med. 2020, 74, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Assogna, F.; Palmer, K.; Pontieri, F.E.; Pierantozzi, M.; Stefani, A.; Gianni, W.; Caltagirone, C.; Spalletta, G. Alexithymia is a non-motor symptom of Parkinson disease. Am. J. Geriatr. Psychiatry 2012, 20, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Siderowf, A.; Jennings, D. Cardiac denervation in rapid eye movement sleep behavior disorder and Parkinson’s disease: Getting to the heart of the matter. Mov. Disord. 2010, 25, 2269–2271. [Google Scholar] [CrossRef] [PubMed]
- David, R.; Koulibaly, M.; Benoit, M.; Garcia, R.; Caci, H.; Darcourt, J.; Robert, P. Striatal dopamine transporter levels correlate with apathy in neurodegenerative diseases. A SPECT study with partial volume effect correction. Clin. Neurol. Neurosurg. 2008, 110, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Roselli, F.; Pisciotta, N.M.; Perneczky, R.; Pennelli, M.; Aniello, M.S.; De Caro, M.F.; Ferrannini, E.; Tartaglione, B.; Defazio, G.; Rubini, G.; et al. Severity of neuropsychiatric symptoms and dopamine transporter levels in dementia with lewy bodies: A123I-FP-CIT SPECT study. Mov. Disord. 2009, 24, 2097–2103. [Google Scholar] [CrossRef]
- Saper, C.; Schmidt, P.; Siegel, J.M.; Singer, C.; St Louis, E.; Videnovic, A.; Oertel, W. Rapid eye movement sleep behavior disorder: Devising controlled active treatment studies for symptomatic and neuroprotective therapy-a consensus statement from the International Rapid Eye Movement Sleep Behavior Disorder Study Group. Sleep Med. 2013, 14, 795–806. [Google Scholar]
- Jung, Y.; Boot, B.P.; Mielke, M.M.; Ferman, T.J.; Geda, Y.E.; McDade, E.; Christianson, T.J.H.; Knopman, D.S.; St Louis, E.K.; Silber, M.H.; et al. Phenoconversion from probable rapid eye movement sleep behavior disorder to mild cognitive impairment to dementia in a population-based sample. Alzheimers Dement. 2017, 8, 127–130. [Google Scholar] [CrossRef]
- Nomura, T.; Inoue, Y.; Kagimura, T.; Uemura, Y.; Nakashima, K. Utility of the REM sleep behavior disorder screening questionnaire (RBDSQ) in Parkinson’s disease patients. Sleep Med. 2011, 12, 711–713. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | iRBD | PD + RBD | PD-RBD | HC | F-value | df | P-value | Cohen’s f | post-hoc *** | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (n = 38) | (n = 38) | (n = 38) | (n = 38) | iRBD vs. HC (Cohen’s f) | iRBD vs. PD + RBD (Cohen’s f) | iRBD vs. PD-RBD (Cohen’s f) | HC vs. PD + RBD (Cohen’s f) | HC vs. PD-RBD (Cohen’s f) | PD + RBD vs. PD-RBD (Cohen’s f) | |||||
| Age ** (Years) | 67.61 ± 6.99 | 67.16 ± 7.38 | 67.26 ± 7.18 | 67.47 ± 7.40 | 0.030 | 3 | 0.9931 | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. |
| Education ** (Years) | 11.87 ± 4.02 | 12.18 ± 3.99 | 11.29 ± 3.72 | 12.03 ± 4.00 | 0.0374 | 3 | 0.7719 | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. |
| MMSE ** | 28.19 ± 1.67 | 28.58 ± 1.39 | 28.63 ± 1.48 | 29.32 ± 0.93 | 4.343 | 3 | 0.0058* | 0.2919 | 0.0005 * (0.2867) | 0.2178 | 0.1628 | 0.0223 * (0.1877) | 0.0336 * (0.1750) | 0.8691 |
| Disease duration (Years) | ~ | 4.68 ± 3.57 | 3.96 ± 3.12 | ~ | 0.917 | 1 | 0.3413 | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. |
| Time from symptoms onset (Years) | 5.08 ± 6.64 | ~ | ~ | ~ | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. |
| UPDRS-III score | 2.37 ± 2.43 | 19.26 ± 10.30 | 16.66 ± 10.13 | ~ | 17.360 | 2 | < 0.0001 * | 0.8779 | n.a. | < 0.0001 * (0.8152) | < 0.0001 * (0.6898) | n.a. | n.a. | 0.2123 |
| Hoehn &Yahr stage | ~ | 1.97 ± 0.60 | 1.82 ± 0.60 | ~ | 1.314 | 1 | 0.2554 | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. |
| Daily Levodopa Equivalent Dose (mg) | ~ | 486.18 ± 370,66 | 388.12 ± 363.01 | ~ | 1.358 | 1 | 0.2477 | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. |
| Characteristic | iRBD | PD + RBD | PD-RBD | HC | Chi | df | P-value | Cohen’s f | post-hoc | |||||
| (n = 38) | (n = 38) | (n = 38) | (n = 38) | iRBD vs. HC | iRBD vs. PD + RBD | iRBD vs. PD-RBD | HC vs. PD + RBD | HC vs. PD-RBD | PD + RBD vs. PD-RBD | |||||
| Sex (n. Male/n. Female) | 31/7 | 31/7 | 31/7 | 31/7 | 0 | 3 | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. |
| Variables | iRBD | PD + RBD | PD-RBD | HC | F-value | df | P-value | Cohen’s f | post-hoc *** | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (n = 38) | (n = 38) | (n = 38) | (n = 38) | iRBD vs. HC (Cohen’s f) | iRBD vs. PD + RBD (Cohen’s f) | iRBD vs. PD-RBD (Cohen’s f) | HC vs. PD + RBD (Cohen’s f) | HC vs. PD-RBD (Cohen’s f) | PD + RBD vs. PD-RBD (Cohen’s f) | |||||
| RIR | 32.74 ± 9.00 | 36.55 ± 8.57 | 35.37 ± 10.14 | 42.66 ± 8.14 | 8.291 | 3 | < 0.0001 * | 0.4045 | < 0.0001 ** (0.3900) | 0.0664 (0.1498) | 0.2041 (0.1034) | 0.0036 ** (0.2402) | 0.0005 ** (0.2866) | 0.5668 (0.0464) |
| RDR | 13.21 ± 3.35 | 7.37 ± 2.79 | 7.24 ± 3.03 | 9.34 ± 2.88 | 32.315 | 3 | < 0.0001 * | 0.7986 | < 0.0001 ** (0.4531) | < 0.0001 ** (0.6838) | < 0.0001 ** (0.6990) | 0.0050 ** (0.2307) | 0.0028 ** (0.2459) | 0.8497 (0.0152) |
| CRO | 28.64 ± 6.39 | 27.82 ± 5.12 | 28.32 ± 4.61 | 32.88 ± 2.72 | 8.675 | 3 | < 0.0001 * | 0.4134 | 0.0002 ** (0.3065) | 0.4611 (0.0593) | 0.7698 (0.0231) | < 0.0001 ** (0.3658) | < 0.0001 ** (0.3296) | 0.6565 (0.0361) |
| SWCT (Word Reading) | 15.92 ± 3.61 | 15.58 ± 4.40 | 15.74 ± 3.77 | 14.05 ± 3.09 | 1.993 | 3 | 0.1176 | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. |
| SWCT (Color Naming) | 21.82 ± 5.18 | 22.10 ± 5.87 | 21.63 ± 5.66 | 19.37 ± 3.79 | 2.23 | 3 | 0.0875 | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. |
| SWCT (Interference) | 50.63 ± 26.23 | 49.79 ± 30.14 | 43.34 ± 12.48 | 38.24 ± 10.69 | 2.773 | 3 | 0.0436 | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. |
| PVF | 30.90 ± 11.23 | 31.55 ± 9.11 | 28.13 ± 7.44 | 38.97 ± 11.40 | 8.273 | 3 | <0.0001 * | 0.4040 | 0.0005 ** (0.2873) | 0.7732 | 0.2271 | 0.0014 ** (0.2642) | < 0.0001 ** (0.3860) | 0.1353 |
| SVF | 17.53 ± 4.48 | 18.66 ± 5.03 | 18.37 ± 5.27 | 22.40 ± 5.00 | 7.228 | 3 | 0.0001 * | 0.3777 | < 0.0001 ** (0.3476) | 0.3208 | 0.4596 | 0.0013** (0.2670) | 0.0005 ** (0.2877) | 0.7992 |
| WCST-SF (Categories) | 5.42 ± 1.18 | 5.58 ± 1.00 | 5.37 ± 1.10 | 6.00 ± 0.00 | 3.456 | 3 | 0.0181 | n.a. | 0.0087 | 0.4696 | 0.8094 | 0.0551 | 0.0043 | 0.3353 |
| WCST-SF (Perseverative Errors) | 3.03 ± 3.98 | 2.42 ± 4.14 | 2.79 ± 4.07 | 0.37 ± 0.71 | 4.480 | 3 | 0.0048 * | 0.2974 | 0.0013** (0.2659) | 0.4569 | 0.7708 | 0.0125 | 0.0033 ** (0.2419) | 0.6505 |
| WCST-SF (Non perseverative Errors) | 3.10 ± 2.86 | 2.55 ± 2.64 | 3.08 ± 2.96 | 0.95 ± 1.01 | 6.299 | 3 | 0.0005 * | 0.3513 | 0.0002** (0.3045) | 0.3354 | 0.9634 | 0.0057 ** (0.2266) | 0.0003 ** (0.3017) | 0.3554 |
| Variables | iRBD | PD + RBD | PD-RBD | HC | F-value | df | P-value | Cohen’s f | post-hoc *** | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (n = 38) | (n = 38) | (n = 38) | (n = 38) | iRBD vs. HC (Cohen’s f) | iRBD vs. PD + RBD (Cohen’s f) | iRBD vs. PD-RBD (Cohen’s f) | HC vs. PD + RBD (Cohen’s f) | HC vs. PD-RBD (Cohen’s f) | PD + RBD vs. PD-RBD (Cohen’s f) | |||||
| HARS | 11.42 ± 5.12 | 9.05 ± 5.07 | 8.71 ± 6.41 | 4.10 ± 3.94 | 13.114 | 3 | < 0.0001 * | 0.5089 | < 0.0001 ** (0.4968) | 0.0493 | 0.0247 | < 0.0001 ** (0.3360) | 0.0002 ** (0.3129) | 0.7750 |
| TAS-20 | 50.55 ± 13.84 | 46.87 ± 11.27 | 47.34 ± 12.07 | 40.76 ± 10.17 | 4.474 | 3 | 0.0049 * | 0.2972 | 0.0005 ** (0.2906) | 0.1797 | 0.2420 | 0.0270 | 0.0173 | 0.8626 |
| TAS-20 F1 | 14.97 ± 5.79 | 12.32 ± 5.16 | 13.29 ± 6.37 | 9.79 ± 3.06 | 6.491 | 3 | 0.0004 * | 0.3575 | < 0.0001 ** (0.3491) | 0.0287 | 0.1636 | 0.0374 | 0.004 ** (0.2359) | 0.4196 |
| TAS-20 F2 | 14.10 ± 6.11 | 13.71 ± 5.70 | 14.05 ± 5.93 | 11.76 ± 5.14 | 1.426 | 3 | 0.2377 | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. |
| TAS-20 F3 | 21.47 ± 5.97 | 20.84 ± 5.01 | 20 ± 5.91 | 19.21 ± 5.19 | 1.207 | 3 | 0.3092 | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. |
| ARS | 11.24 ± 7.77 | 7.32 ± 5.55 | 7.90 ± 6.42 | 5.24 ± 4.73 | 6.081 | 3 | 0.0006 * | 0.3464 | < 0.0001 ** (0.3411) | 0.0067 ** (0.2228) | 0.0205 | 0.1472 | 0.0644 | 0.6855 |
| SHAPS | 0.32 ± 0.78 | 0.29 ± 0.57 | 0.40 ± 0.68 | 0.24 ± 0.43 | 0.420 | 3 | 0.7390 | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. |
| BDI Total score | 10.37 ± 7.99 | 8.92 ± 5.76 | 8.82 ± 6.40 | 4.32 ± 4.69 | 6.543 | 3 | 0.0003 * | 0.3591 | < 0.0001 ** (0.3382) | 0.3200 | 0.2862 | 0.0018 ** (0.2572) | 0.0023 ** (0.2516) | 0.9423 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Assogna, F.; Liguori, C.; Cravello, L.; Macchiusi, L.; Belli, C.; Placidi, F.; Pierantozzi, M.; Stefani, A.; Mercuri, B.; Izzi, F.; et al. Cognitive and Neuropsychiatric Profiles in Idiopathic Rapid Eye Movement Sleep Behavior Disorder and Parkinson’s Disease. J. Pers. Med. 2021, 11, 51. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11010051
Assogna F, Liguori C, Cravello L, Macchiusi L, Belli C, Placidi F, Pierantozzi M, Stefani A, Mercuri B, Izzi F, et al. Cognitive and Neuropsychiatric Profiles in Idiopathic Rapid Eye Movement Sleep Behavior Disorder and Parkinson’s Disease. Journal of Personalized Medicine. 2021; 11(1):51. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11010051
Chicago/Turabian StyleAssogna, Francesca, Claudio Liguori, Luca Cravello, Lucia Macchiusi, Claudia Belli, Fabio Placidi, Mariangela Pierantozzi, Alessandro Stefani, Bruno Mercuri, Francesca Izzi, and et al. 2021. "Cognitive and Neuropsychiatric Profiles in Idiopathic Rapid Eye Movement Sleep Behavior Disorder and Parkinson’s Disease" Journal of Personalized Medicine 11, no. 1: 51. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11010051