
Gut Microbiota as Early Predictor of Infectious Complications before Cardiac Surgery: A Prospective Pilot Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
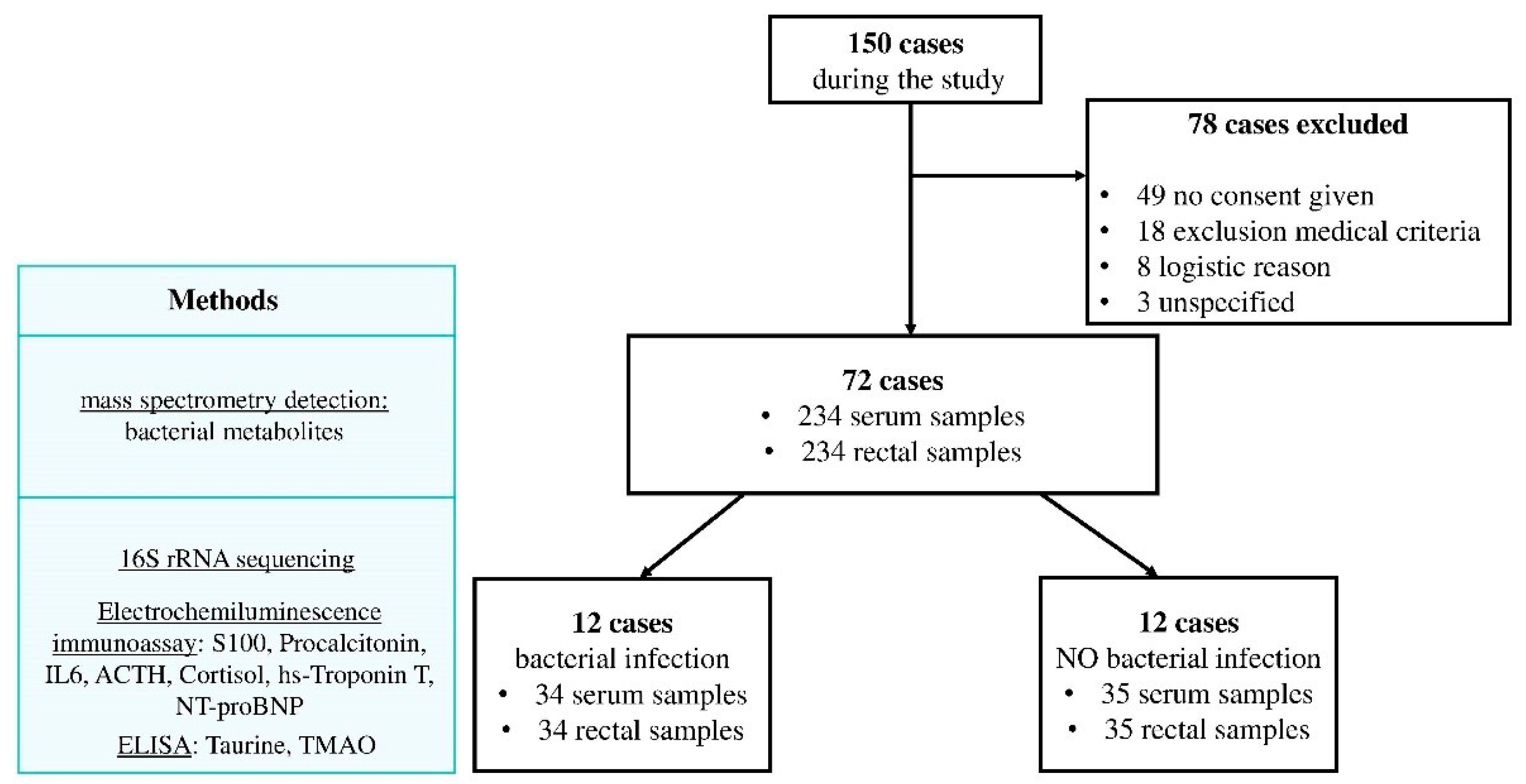
2.1. Study Design
2.2. Patients and Samples
2.3. Analysis of Serum Biomarkers
2.4. Microbiome Sample Preparation
2.5. Microbiome Data Processing
2.6. Statistical Analysis
3. Results
3.1. Patients Characteristics
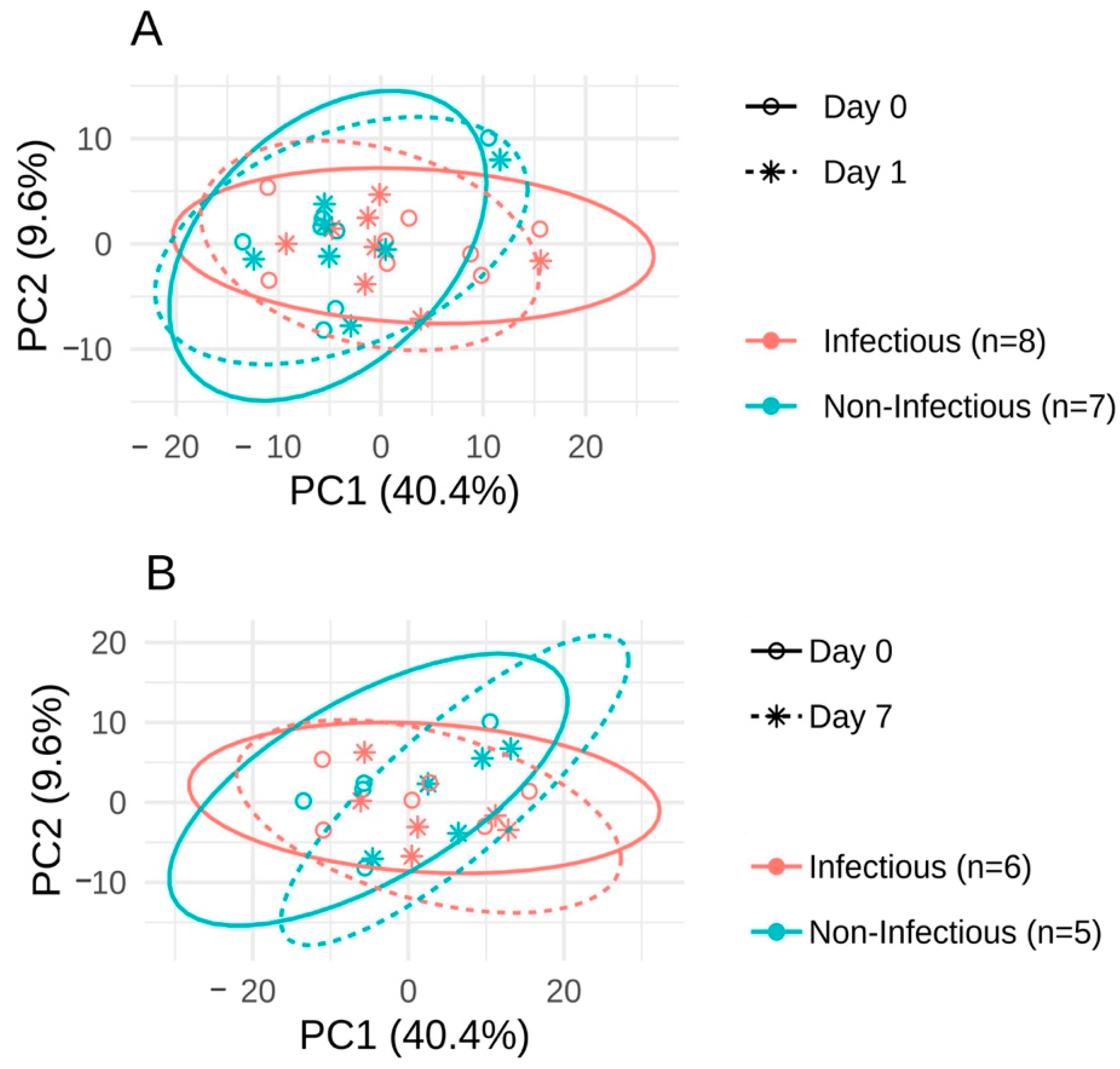
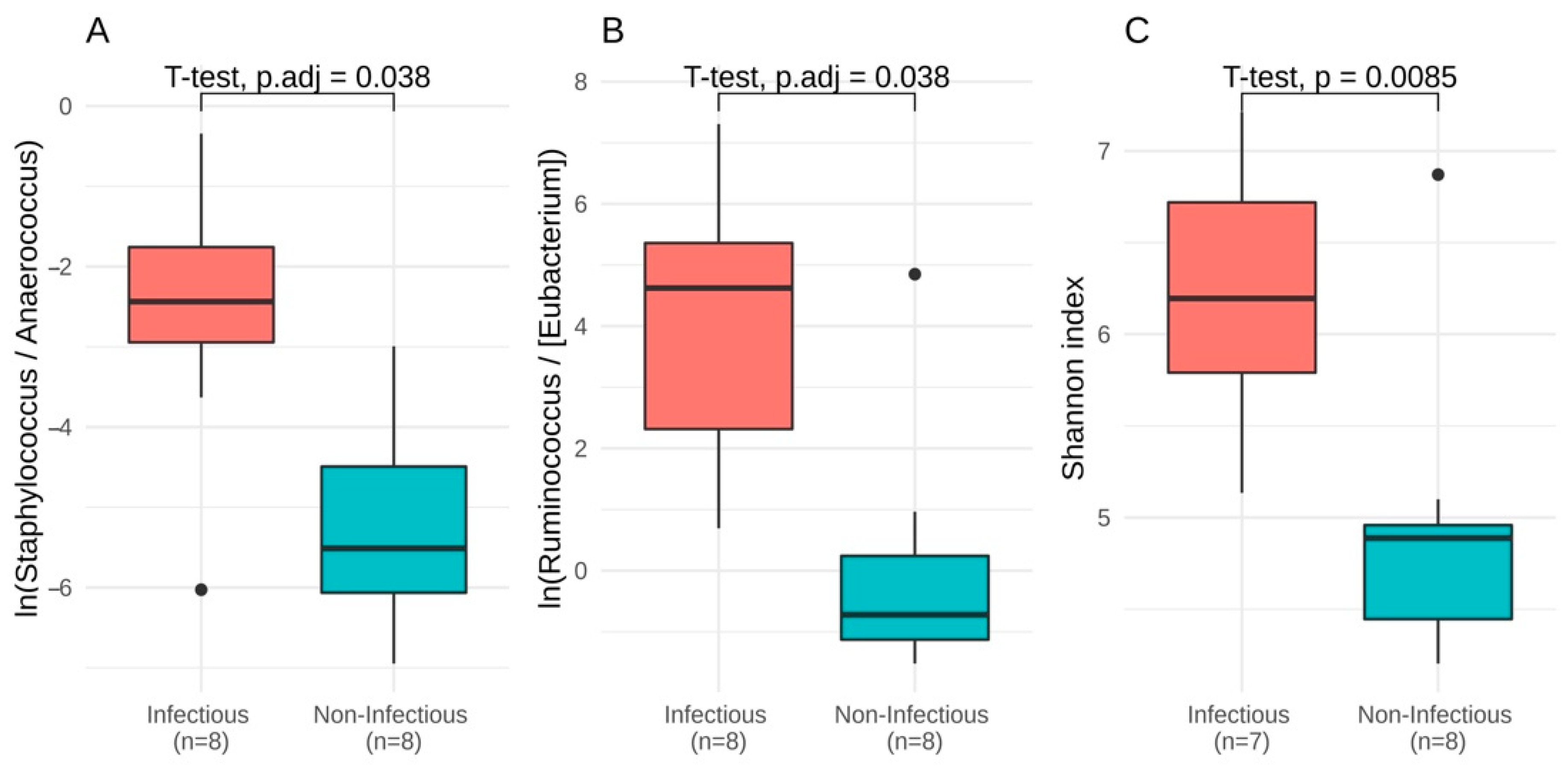
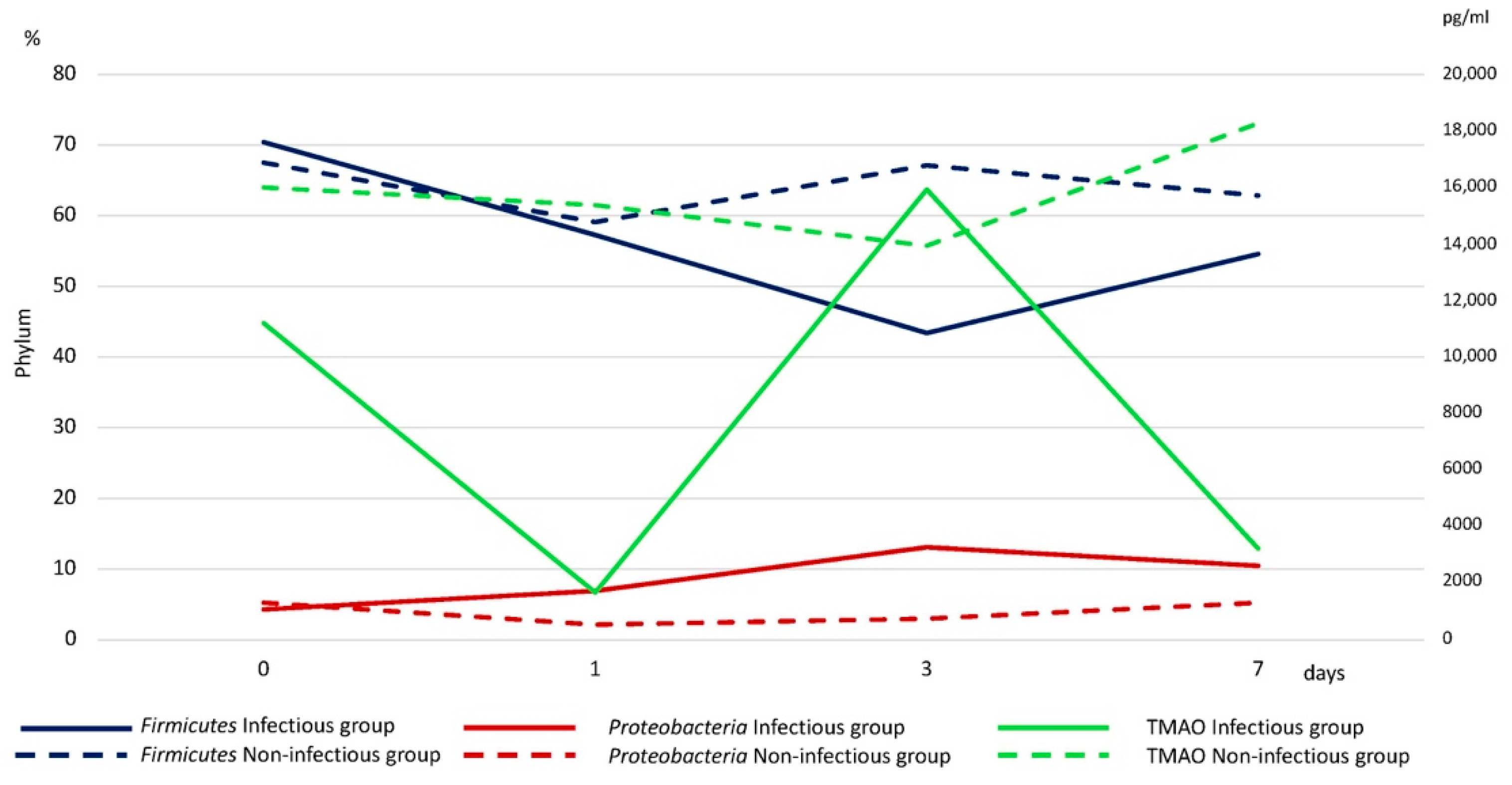
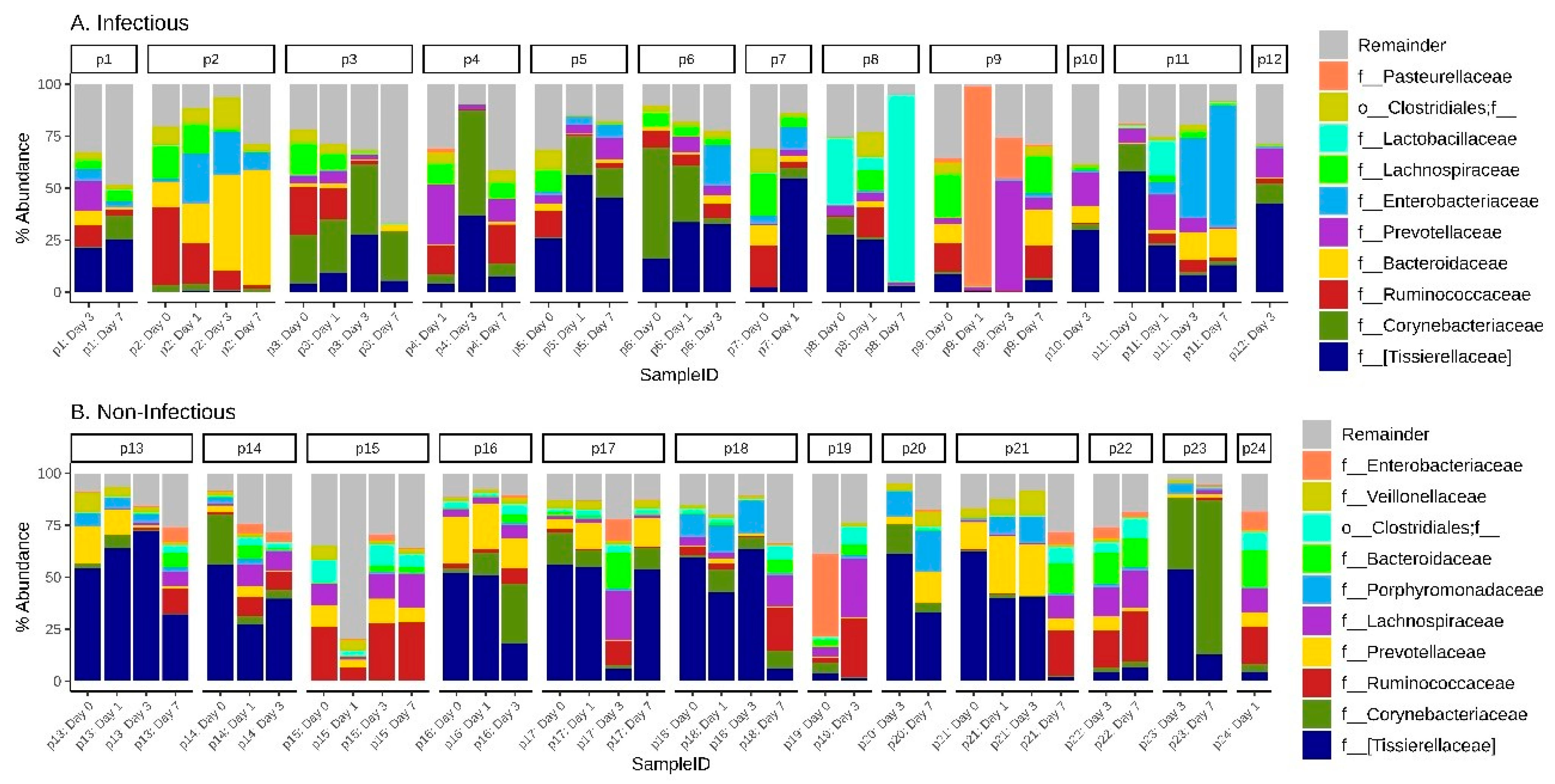
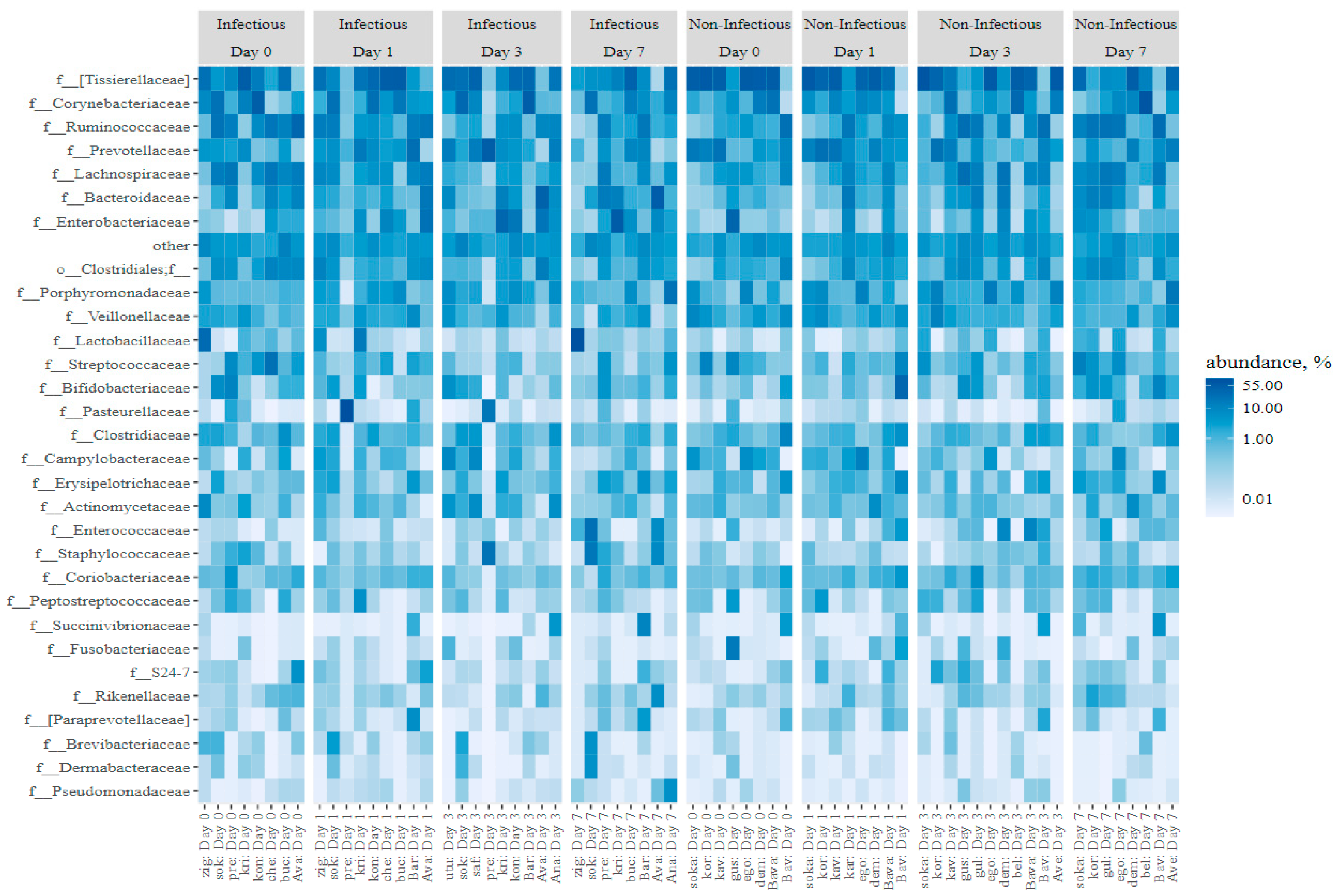
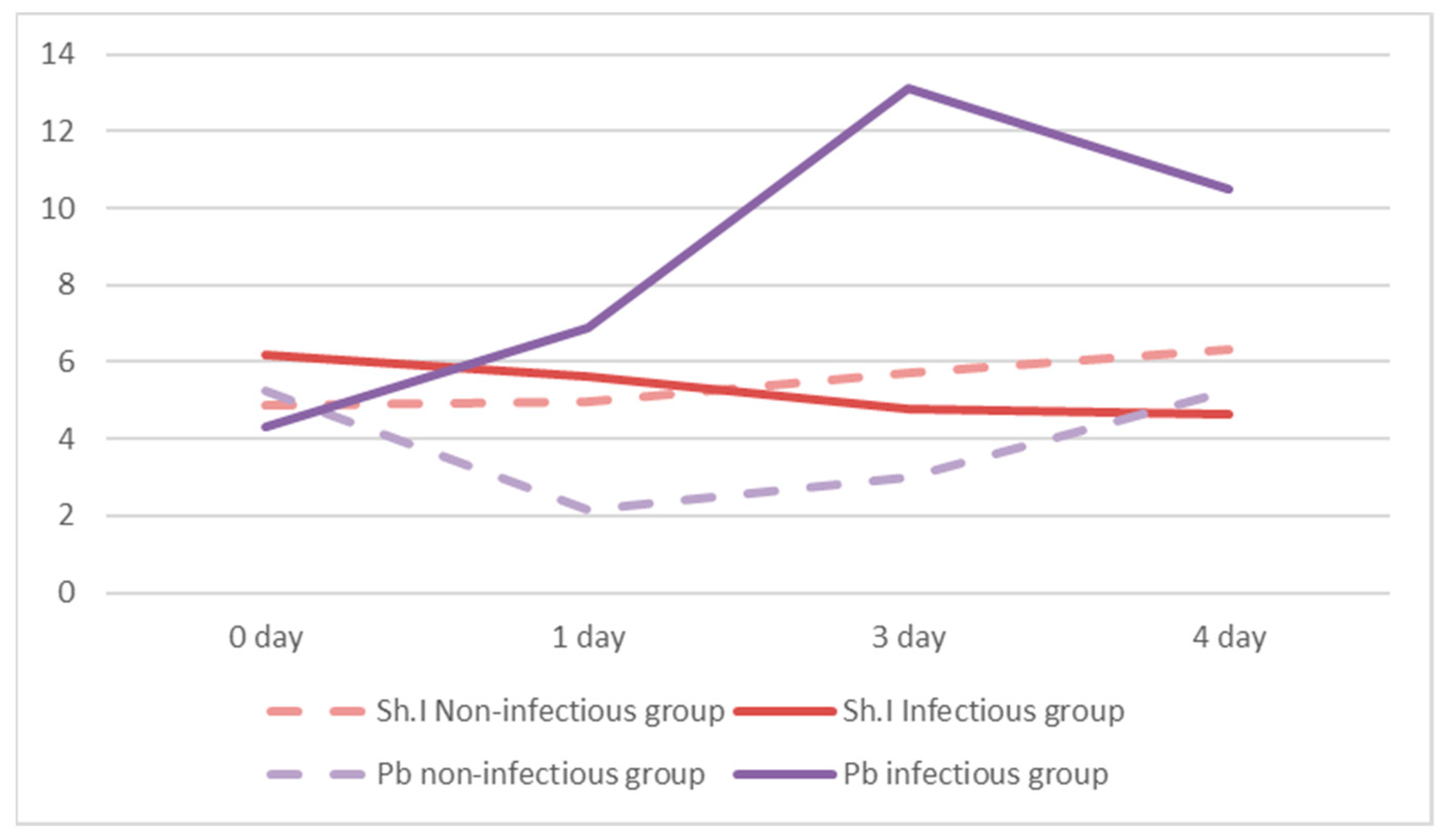
3.2. The Microbiota Composition
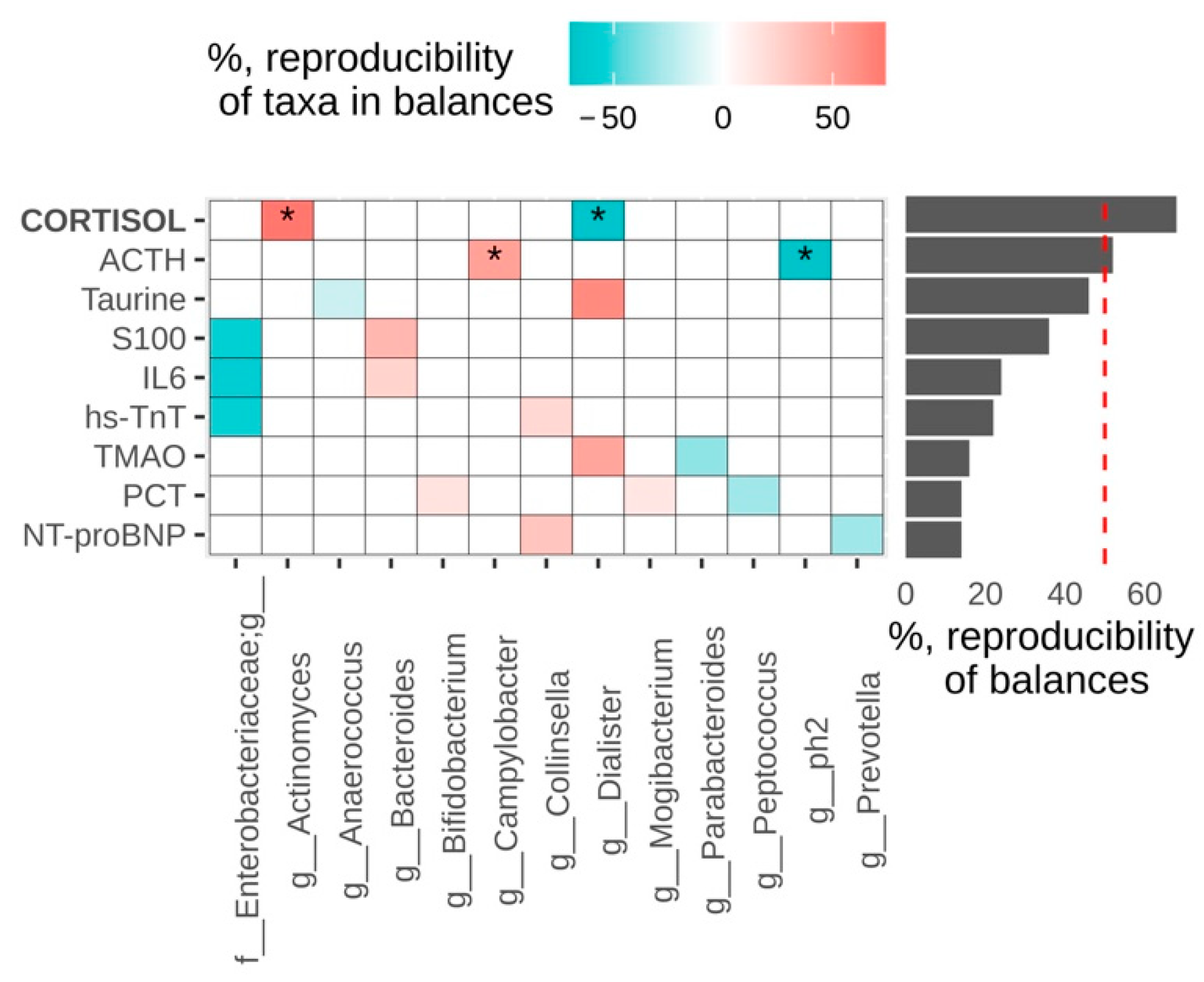
3.3. Biomarkers
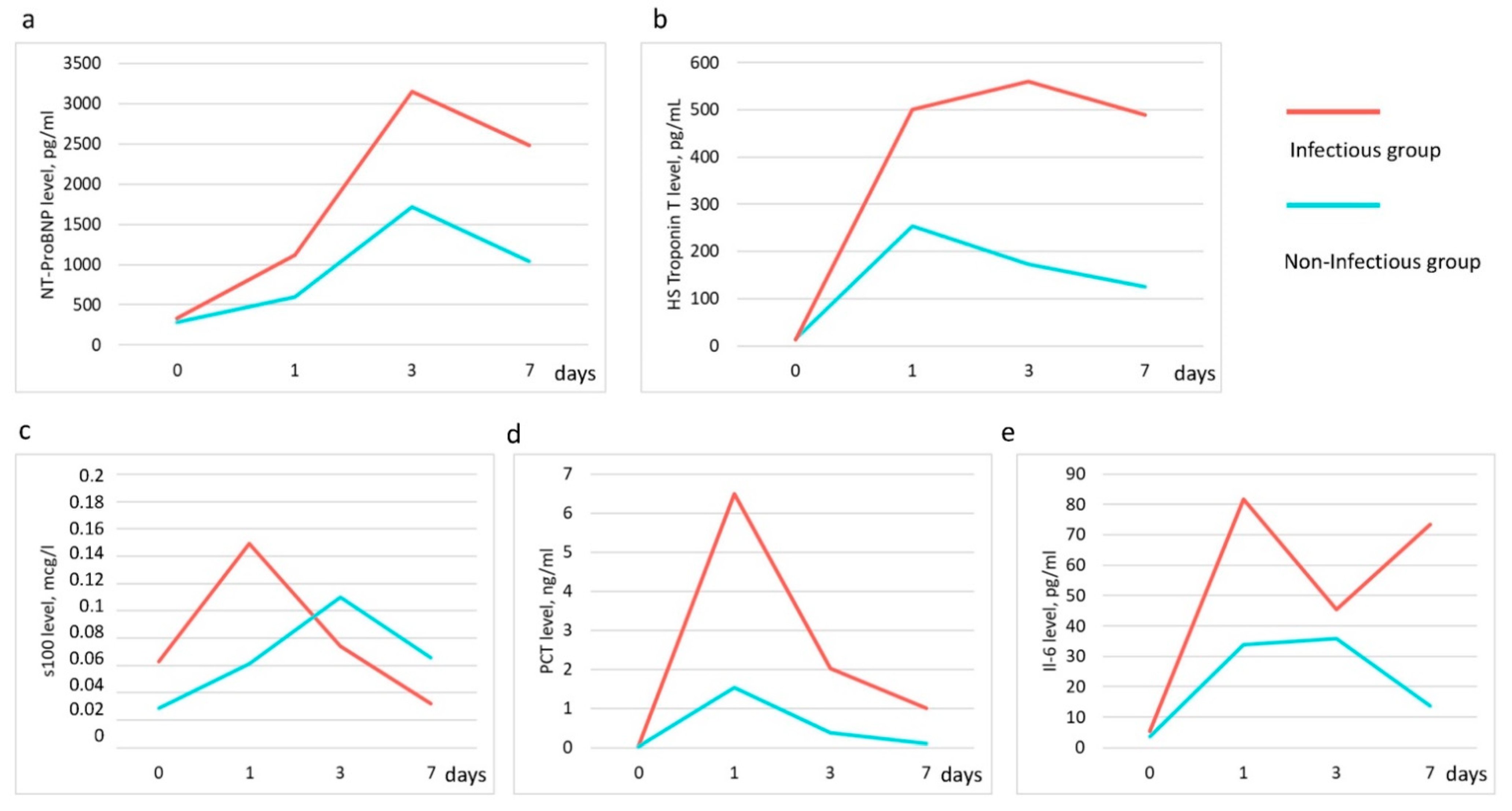
3.3.1. Pro-BNP, HS-Troponin T Levels
3.3.2. S100 Level
3.3.3. Interleukin—6 (IL), Procalcitonin (PCT) Level
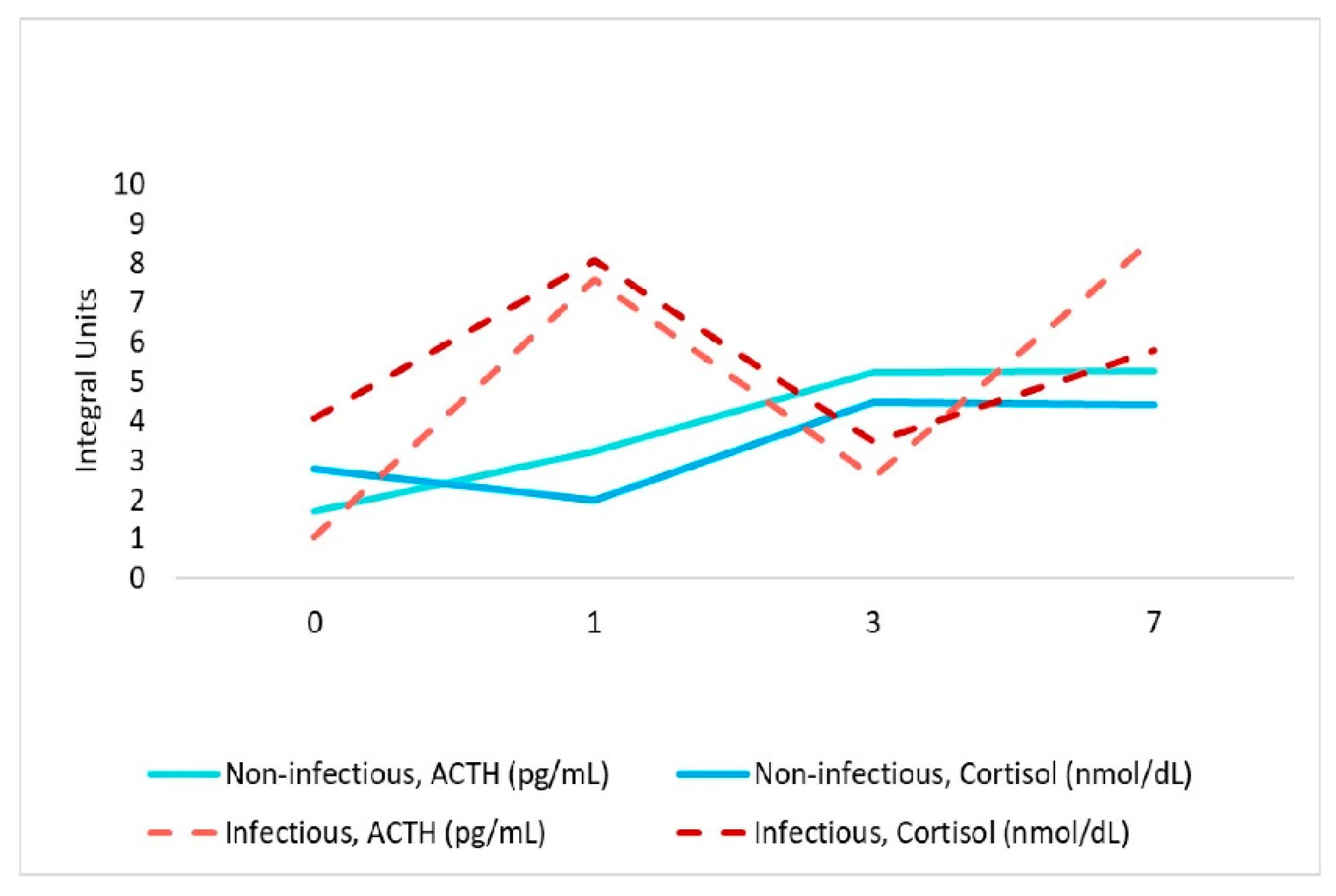
3.3.4. Adrenocorticotropic Hormone (ACTH), Cortisol Level
3.3.5. Taurine, TMAO Level
3.4. Clinical Cases with Microbiological Confirmation of Infection
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Biomarkers | Patients (Median [IQR 25–75%]) | ||||
|---|---|---|---|---|---|
| Infectious Group | Non-Infectious Group | p-Level | |||
| ACTH, pg/mL | 2.59 | (1.26–8.7) | 3.47 | (1.4–7.3) | 1 |
| * Cortisol, nmol/L | 473.2 | (344.1–805.5) | 384.25 | (209.8–482.6) | 0.037 |
| IL-6, pg/mL | 41.84 | (7.7–83.03) | 19.57 | (7.04–37.7) | 0.127 |
| * PCT, ng/mL | 0.924 | (0.27–5.76) | 0.183 | (0.025–0.65) | 0.002 |
| * pro-BNP, pg/mL | 1679 | (674.25–4315.5) | 908 | (462.5–1378) | 0.024 |
| Troponin T-HS, pg/mL | 279.4 | (18.87–628.5) | 126.9 | (19.69–253) | 0.369 |
| S100, μg/L | 0.084 | (0.036–0.1375) | 0.053 | (0.031–0.136) | 0.657 |
| TMAO, pg/mL | 9764 | (1675–19,300) | 15,848 | (11,127–19,844) | 0.052 |
| Taurine, pg/mL | 694 | (379–769) | 455 | (325–720) | 0.101 |


References
- Vesteinsdottir, E.; Helgason, K.O.; Sverrisson, K.O.; Gudlaugsson, O.; Karason, S. Infections and outcomes after cardiac surgery-The impact of outbreaks traced to transesophageal echocardiography probes. Acta Anaesthesiol. Scand. 2019, 63, 871–878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gelijns, A.C.; Moskowitz, A.J.; Acker, M.A.; Argenziano, M.; Geller, N.L.; Puskas, J.D.; Perrault, L.P.; Smith, P.K.; Kron, I.L.; Michler, R.E.; et al. Management practices and major infections after cardiac surgery. J. Am. Coll. Cardiol. 2014, 64, 372–381. [Google Scholar] [CrossRef] [Green Version]
- Hamouda, K.; Oezkur, M.; Sinha, B.; Hain, J.; Menkel, H.; Leistner, M.; Leyh, R.; Schimmer, C. Different duration strategies of perioperative antibiotic prophylaxis in adult patients undergoing cardiac surgery: An observational study. J. Cardiothorac. Surg. 2015, 10, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dixon, L.K.; Di Tommaso, E.; Dimagli, A.; Sinha, S.; Sandhu, M.; Benedetto, U.; Angelini, G.D. Impact of sex on outcomes after cardiac surgery: A systematic review and meta-analysis. Int. J. Cardiol. 2021, 15, 27–34. [Google Scholar] [CrossRef]
- O’Keefe, S.; Williams, K.; Legare, J.-F. Hospital-Acquired Infections after Cardiac Surgery and Current Physician Practices: A Retrospective Cohort Study. J. Clin. Med. Res. 2017, 9, 10–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Q.; Gao, B.; Siqin, B.; He, Q.; Zhang, R.; Meng, X.; Naiheng, Z.; Zhang, N.; Li, M. Gut Microbiota: A Novel Regulator of Cardiovascular Disease and Key Factor in the Therapeutic Effects of Flavonoids. Front. Pharmacol. 2021, 12, 651926. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.H.W.; Kitai, T.; Hazen, S.L. Gut Microbiota in Cardiovascular Health and Disease. Circ. Res. 2017, 120, 1183–1196. [Google Scholar] [CrossRef] [Green Version]
- Piccioni, A.; Saviano, A.; Cicchinelli, S.; Franza, L.; Rosa, F.; Zanza, C.; Rosa, F.; Zanza, C.; Santoro, M.C.; Candelli, M.; et al. Microbiota and Myopericarditis: The New Frontier in the Car-Diological Field to Prevent or Treat Inflammatory Cardiomyo-Pathies in COVID-19 Outbreak. Biomedicines 2021, 9, 1234. [Google Scholar] [CrossRef]
- Yamashita, T.; Emoto, T.; Sasaki, N.; Hirata, K.-I. Gut Microbiota and Coronary Artery Disease. Int. Heart J. 2016, 57, 663–671. [Google Scholar] [CrossRef] [Green Version]
- Xu, H.; Wang, X.; Feng, W.; Liu, Q.; Zhou, S.; Liu, Q.; Cai, L. The gut microbiota and its interactions with cardiovascular disease. Microb. Biotechnol. 2020, 13, 637–656. [Google Scholar] [CrossRef] [Green Version]
- Suslov, A.V.; Chairkina, E.; Shepetovskaya, M.D.; Suslova, I.S.; Khotina, V.A.; Kirichenko, T.V.; Postnov, A.Y. The neuroimmune role of intestinal Microbiota in the pathogenesis of cardiovascular disease. J. Clin. Med. Res. 2021, 10, 1995. [Google Scholar]
- Chen, X.; Li, H.-Y.; Hu, X.-M.; Zhang, Y.; Zhang, S.-Y. Current understanding of gut microbiota alterations and related therapeutic intervention strategies in heart failure. Chin. Med. J. 2019, 132, 1843–1855. [Google Scholar] [CrossRef]
- Jia, Q.; Li, H.; Zhou, H.; Zhang, X.; Zhang, A.; Xie, Y.; Li, Y.; Lv, S.; Zhang, J. Role and Effective Therapeutic Target of Gut Microbiota in Heart Failure. Cardiovasc. Ther. 2019, 2019, 5164298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piccioni, A.; de Cunzo, T.; Valletta, F.; Covino, M.; Rinninella, E.; Raoul, P.; Zanza, C.; Mele, M.C.; Franceschi, F. Gut Microbiota and Environment in Coronary Artery Disease. Int. J. Environ. Res. Public Health 2021, 18, 4242. [Google Scholar] [CrossRef]
- Aardema, H.; Lisotto, P.; Kurilshikov, A.; Diepeveen, J.R.J.; Friedrich, A.W.; Sinha, B.; de Smet, A.M.G.A.; Harmsen, H.J.M. Marked Changes in Gut Microbiota in Cardio-Surgical Intensive Care Patients: A Longitudinal Cohort Study. Front. Cell Infect. Microbiol. 2019, 9, 467. [Google Scholar] [CrossRef] [Green Version]
- Iapichino, G.; Callegari, M.L.; Marzorati, S.; Cigada, M.; Corbella, D.; Ferrari, S.; Morelli, M. Impact of antibiotics on the gut microbiota of critically ill patients. J. Med. Microbiol. 2008, 57, 1007–1014. [Google Scholar] [CrossRef]
- McDonald, D.; Ackermann, G.; Khailova, L.; Baird, C.; Heyland, D.; Kozar, R.; Lemieux, M.; Derenski, K.; King, J.; Vis-Kampen, C.; et al. Extreme Dysbiosis of the Microbiome in Critical Illness. Msphere 2016, 1. [Google Scholar] [CrossRef] [Green Version]
- Ojima, M.; Motooka, D.; Shimizu, K.; Gotoh, K.; Shintani, A.; Yoshiya, K.; Nakamura, S.; Ogura, H.; Iida, D.; Shimazu, T. Metagenomic Analysis Reveals Dynamic Changes of Whole Gut Microbiota in the Acute Phase of Intensive Care Unit Patients. Dig. Dis. Sci. 2016, 61, 1628–1634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chernevskaya, E.; Beloborodova, N.; Klimenko, N.; Pautova, A.; Shilkin, D.; Gusarov, V.; Tyakht, A. Serum and fecal profiles of aromatic microbial metabolites reflect gut microbiota disruption in critically ill patients: A prospective observational pilot study. Crit. Care 2020, 24, 312. [Google Scholar] [CrossRef]
- Sekirov, I.; Russell, S.L.; Antunes, L.C.M.; Finlay, B.B. Gut microbiota in health and disease. Physiol. Rev. 2010, 90, 859–904. [Google Scholar] [CrossRef] [Green Version]
- Chernevskaya, E.; Klimenko, N.; Pautova, A.; Buyakova, I.; Tyakht, A.; Beloborodova, N. Host-Microbiome Interactions Mediated by Phenolic Metabolites in Chronically Critically Ill Patients. Metabolites 2021, 11, 122. [Google Scholar] [CrossRef]
- Piccioni, A.; Valletta, F.; Zanza, C.; Esperide, A.; Franceschi, F. Novel biomarkers to assess the risk for acute coronary syndrome: Beyond troponins. Intern. Emerg. Med. 2020, 15, 1193–1199. [Google Scholar] [CrossRef] [PubMed]
- Klimenko, N.; Tyakht, A.; Popenko, A.; Vasiliev, A.; Altukhov, I.; Ischenko, D.; Shashkova, T.I.; Efimova, D.A.; Nikogosov, D.A.; Osipenko, D.A.; et al. Microbiome Responses to an Uncontrolled Short-Term Diet Intervention in the Frame of the Citizen Science Project. Nutrients 2018, 10, 576. [Google Scholar] [CrossRef] [Green Version]
- Efimova, D.; Tyakht, A.; Popenko, A.; Vasilyev, A.; Altukhov, I.; Dovidchenko, N.; Odintsova, V.; Klimenko, N.; Loshkarev, R.; Pashkova, M.; et al. Knomics-Biota—A system for exploratory analysis of human gut microbiota data. BioData Min. 2018, 11, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Callahan, B.J.; McMurdie, P.J.; Rosen, M.J.; Han, A.W.; Johnson, A.J.A.; Holmes, S.P. DADA2: High-resolution sample inference from Illumina amplicon data. Nat. Methods 2016, 13, 581–583. [Google Scholar] [CrossRef] [Green Version]
- DeSantis, T.Z.; Hugenholtz, P.; Larsen, N.; Rojas, M.; Brodie, E.L.; Keller, K.; Huber, T.; Dalevi, D.; Hu, P.; Andersen, G.L. Greengenes, a chimera-checked 16S rRNA gene database and workbench compatible with ARB. Appl. Environ. Microbiol. 2006, 72, 5069–5072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrianova, N.V.; Popkov, V.A.; Klimenko, N.S.; Tyakht, A.V.; Baydakova, G.V.; Frolova, O.Y.; Zorova, L.D.; Pevzner, I.P.; Zorov, D.B.; Plotnikov, E.Y. Microbiome-Metabolome Signature of Acute Kidney Injury. Metabolites 2020, 10, 142. [Google Scholar] [CrossRef] [Green Version]
- Brandt, B.W.; Bonder, M.J.; Huse, S.M.; Zaura, E. TaxMan: A server to trim rRNA reference databases and inspect taxonomic coverage. Nucleic Acids Res. 2012, 40, W82–W87. [Google Scholar] [CrossRef] [Green Version]
- Fu, L.; Niu, B.; Zhu, Z.; Wu, S.; Li, W. CD-HIT: Accelerated for clustering the next-generation sequencing data. Bioinformatics 2012, 28, 3150–3152. [Google Scholar] [CrossRef]
- Shen, S.-M. The Statistical Analysis of Compositional Data; Open Dissertation Press: Pokfulam, Kong Kong, 2017. [Google Scholar]
- Aitchison, J. The Statistical Analysis of Compositional Data. J. R. Stat. Soc. 1986, 44, 139–177. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Quinn, T.P.; Erb, I. Interpretable Log Contrasts for the Classification of Health Biomarkers: A New Approach to Balance Selection. Msystems 2020, 5. [Google Scholar] [CrossRef] [Green Version]
- Palarea-Albaladejo, J.; Martín-Fernández, J.A. zCompositions—R package for multivariate imputation of left-censored data under a compositional approach. Chemom. Intell. Lab. Systems. 2015, 143, 85–96. [Google Scholar] [CrossRef]
- Dixon, P. VEGAN, a package of R functions for community ecology. J. Veg. Sci. 2003, 927–930. [Google Scholar] [CrossRef]
- Kuznetsova, A.; Brockhoff, P.B.; Christensen, R.H.B. lmerTest Package: Tests in Linear Mixed Effects Models. J. Stat. Softw. 2017, 82. [Google Scholar] [CrossRef] [Green Version]
- Rivera-Pinto, J.; Egozcue, J.J.; Pawlowsky-Glahn, V.; Paredes, R.; Noguera-Julian, M.; Calle, M.L. Balances: A New Perspective for Microbiome Analysis. Msystems 2018, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gloor, G.B.; Macklaim, J.M.; Pawlowsky-Glahn, V.; Egozcue, J.J. Microbiome Datasets Are Compositional: And This Is Not Optional. Front. Microbiol. 2017, 8, 2224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanafani, Z.A.; Arduino, J.M.; Muhlbaier, L.H.; Kaye, K.S.; Allen, K.B.; Carmeli, Y.; Corey, G.R.; Cosgrove, S.E.; Fraser, T.G.; Harris, A.D.; et al. Incidence of and preoperative risk factors for Staphylococcus aureus bacteremia and chest wound infection after cardiac surgery. Infect. Control. Hosp. Epidemiol. 2009, 30, 242–248. [Google Scholar] [CrossRef]
- Paling, F.P.; Olsen, K.; Ohneberg, K.; Wolkewitz, M.; Fowler, V.G., Jr.; DiNubile, M.J.; Jafri, H.S.; Sifakis, F.; Bonten, M.J.M.; Harbarth, S.J.; et al. Risk prediction for Staphylococcus aureus surgical site infection following cardiothoracic surgery; A secondary analysis of the V710-P003 trial. PLoS ONE 2018, 13, e0193445. [Google Scholar] [CrossRef] [PubMed]
- Dunyach-Remy, C.; Salipante, F.; Lavigne, J.-P.; Brunaud, M.; Demattei, C.; Yahiaoui-Martinez, A.; Bastide, S.; Palayer, C.; Sotto, A.; Gélis, A. Pressure ulcers microbiota dynamics and wound evolution. Sci. Rep. 2021, 11, 18506. [Google Scholar] [CrossRef]
- Fan, X.; Chen, Y.; Liu, Y.; Hu, L. First Case of Bloodstream Infection Caused by Ruminococcus gnavus in an 85 Year Old Man in China. Lab. Med. 2021, e0–e4. [Google Scholar] [CrossRef]
- Yamakawa, H.; Hagiwara, E.; Hayashi, M.; Katano, T.; Isomoto, K.; Otoshi, R.; Shintani, R.; Ikeda, S.; Tanaka, K.; Ogura, T. A case of relapsed lung abscess caused by infection following an initial diagnosis of pulmonary actinomycosis. Respir. Med. Case Rep. 2017, 22, 171–174. [Google Scholar] [CrossRef]
- Kanwal, A.; Avgeropoulos, D.; Kaplan, J.G.; Saini, A. Idiopathic Purulent Pericarditis: A Rare Diagnosis. Am. J. Case Rep. 2020, 21, e921633. [Google Scholar] [CrossRef]
- Nesbitt, W.E.; Fukushima, H.; Leung, K.P.; Clark, W.B. Coaggregation of Prevotella intermedia with oral Actinomyces species. Infect. Immun. 1993, 61, 2011–2014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedersen, P.U.; Tracey, A.; Sindby, J.E.; Bjerrum, M. Preoperative oral hygiene recommendation before open-heart surgery: Patients’ adherence and reduction of infections: A quality improvement study. BMJ Open Qual. 2019, 8, e000512. [Google Scholar] [CrossRef] [Green Version]
- Yuzefpolskaya, M.; Bohn, B.; Nasiri, M.; Zuver, A.M.; Onat, D.D.; Royzman, E.A.; Nwokocha, J.; Mabasa, M.; Pinsino, A.; Brunjes, D.; et al. Gut microbiota, endotoxemia, inflammation, and oxidative stress in patients with heart failure, left ventricular assist device, and transplant. J. Heart Lung Transplant. 2020, 39, 880–890. [Google Scholar] [CrossRef] [PubMed]
- Stacy, A.; Andrade-Oliveira, V.; McCulloch, J.A.; Hild, B.; Oh, J.H.; Perez-Chaparro, P.J.; Sim, C.K.; Lim, A.I.; Link, V.M.; Enamorado, M.; et al. Infection trains the host for microbiota-enhanced resistance to pathogens. Cell 2021, 184, 615–627. [Google Scholar] [CrossRef]
- Forte, E.; Borisov, V.B.; Falabella, M.; Colaço, H.G.; Tinajero-Trejo, M.; Poole, R.K.; Vicente, J.B.; Sarti, P.; Giuffrèet, A. The Terminal Oxidase Cytochrome bd Promotes Sulfide-resistant Bacterial Respiration and Growth. Sci. Rep. 2016, 6, 23788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neumann-Schaal, M.; Jahn, D.; Schmidt-Hohagen, K. Metabolism the Difficile Way: The Key to the Success of the Pathogen. Front. Microbiol. 2019, 10, 219. [Google Scholar] [CrossRef] [Green Version]
- Levy, M.; Thaiss, C.A.; Zeevi, D.; Dohnalová, L.; Zilberman-Schapira, G.; Mahdi, J.A.; David, E.; Savidor, A.; Korem, T.; Herzig, Y.; et al. Microbiota-Modulated Metabolites Shape the Intestinal Microenvironment by Regulating NLRP6 Inflammasome Signaling. Cell 2015, 163, 1428–1443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, S.; Ilyas, I.; Little, P.J.; Li, H.; Kamato, D.; Zheng, X.; Luo, S.; Li, Z.; Liu, P.; Han, J.; et al. Endothelial Dysfunction in Atherosclerotic Cardiovascular Diseases and Beyond: From Mechanism to Pharmacotherapies. Pharmacol. Rev. 2021, 73, 924–967. [Google Scholar] [CrossRef] [PubMed]
- Abebe, W.; Mozaffari, M.S. Role of taurine in the vasculature: An overview of experimental and human studies. Am. J. Cardiovasc. Dis. 2011, 1, 293–311. [Google Scholar]
- Bkaily, G.; Jazzar, A.; Normand, A.; Simon, Y.; Al-Khoury, J.; Jacques, D. Taurine and cardiac disease: State of the art and perspectives. Can. J. Physiol. Pharmacol. 2020, 98, 67–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manor, O.; Zubair, N.; Conomos, M.P.; Xu, X.; Rohwer, J.E.; Krafft, C.E.; Lovejoy, J.C.; Magis, A.T. A Multi-omic Association Study of Trimethylamine N-Oxide. Cell Rep. 2018, 24, 935–946. [Google Scholar] [CrossRef] [Green Version]
- Cho, C.E.; Taesuwan, S.; Malysheva, O.V.; Bender, E.; Tulchinsky, N.F.; Yan, J.; Sutter, J.L.; Caudill, M.A. Trimethylamine-N-oxide (TMAO) response to animal source foods varies among healthy young men and is influenced by their gut microbiota composition: A randomized controlled trial. Mol. Nutr. Food Res. 2017, 61. [Google Scholar] [CrossRef]
- Romano, K.A.; Vivas, E.; Amador-Noguez, D.; Rey, F.E. Intestinal Microbiota Composition Modulates Choline Bioavailability from Diet and Accumulation of the Proatherogenic Metabolite Trimethylamine-N-Oxide. Mbio 2015, 6, e02481. [Google Scholar] [CrossRef] [Green Version]
- Rath, S.; Heidrich, B.; Pieper, D.H.; Vital, M. Uncovering the trimethylamine-producing bacteria of the human gut microbiota. Microbiome 2017, 5, 54. [Google Scholar] [CrossRef] [Green Version]
- Tang, T.W.H.; Chen, H.-C.; Chen, C.-Y.; Yen, C.Y.T.; Lin, C.-J.; Prajnamitra, R.P.; Chen, L.L.; Ruan, S.C.; Lin, J.H.; Lin, P.J.; et al. Loss of Gut Microbiota Alters Immune System Composition and Cripples Postinfarction Cardiac Repair. Circulation 2019, 139, 647–659. [Google Scholar] [CrossRef] [PubMed]
- Sponholz, C.; Sakr, Y.; Reinhart, K.; Brunkhorst, F. Diagnostic value and prognostic implications of serum procalcitonin after cardiac surgery: A systematic review of the literature. Crit. Care 2006, 10, R145. [Google Scholar] [CrossRef] [Green Version]
- Jiao, J.; Wang, M.; Zhang, J.; Shen, K.; Liao, X.; Zhou, X. Procalcitonin as a diagnostic marker of ventilator-associated pneumonia in cardiac surgery patients. Exp. Ther. Med. 2015, 1051–1057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sander, M.; von Heymann, C.; von Dossow, V.; Spaethe, C.; Konertz, W.F.; Jain, U.; Spies, C.D. Increased interleukin-6 after cardiac surgery predicts infection. Anesth. Analg. 2006, 102, 1623–1629. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D. Fourth Universal Definition of Myocardial Infarction. Circulation 2018, 138, e618–e651. [Google Scholar] [CrossRef]
- Gu, Y.; Shan, L.; Liu, B.; Lv, M.; Chen, X.; Yan, T.; Shi, Y.; Chen, J.; Li, Z.; Zhang, Y. Release Profile of Cardiac Troponin T and Risk Factors of Postoperative Myocardial Injury in Patients Undergoing CABG. Int. J. Gen. Med. 2021, 14, 2541–2551. [Google Scholar] [CrossRef]
- Singh, N.; Anchan, R.K.; Besser, S.A.; Belkin, M.N.; Cruz, M.D.; Lee, L.; Yu, D.; Mehta, N.; Nguyen, A.B.; Alenghat, F.J. High sensitivity Troponin-T for prediction of adverse events in patients with COVID-19. Biomarkers 2020, 25, 626–633. [Google Scholar] [CrossRef] [PubMed]
- Nellipudi, J.A.; Baker, R.A.; Dykes, L.; Krieg, B.M.; Bennetts, J.S. Prognostic Value of High-Sensitivity Troponin T After On-Pump Coronary Artery Bypass Graft Surgery. Heart Lung Circ. 2021, 30, 1562–1569. [Google Scholar] [CrossRef]
- Janigro, D.; Bailey, D.M.; Lehmann, S.; Badaut, J.; O’Flynn, R.; Hirtz, C.; Marchi, N. Peripheral Blood and Salivary Biomarkers of Blood-Brain Barrier Permeability and Neuronal Damage: Clinical and Applied Concepts. Front. Neurol. 2020, 11, 577312. [Google Scholar] [CrossRef] [PubMed]
- Silva, F.P.; Schmidt, A.P.; Valentin, L.S.; Pinto, K.O.; Zeferino, S.P.; Oses, J.P.; Wiener, C.D.; Otsuki, D.A.; Tort, A.B.L.; Portela, L.V.; et al. S100B protein and neuron-specific enolase as predictors of cognitive dysfunction after coronary artery bypass graft surgery: A prospective observational study. Eur. J. Anaesthesiol. 2016, 33, 681–689. [Google Scholar] [CrossRef] [PubMed]
- Al Tmimi, L.; van de Velde, M.; Meyns, B.; Meuris, B.; Sergeant, P.; Milisen, K.; Pottel, H.; Poesen, K.; Rex, S. Serum protein S100 as marker of postoperative delirium after off-pump coronary artery bypass surgery: Secondary analysis of two prospective randomized controlled trials. Clin. Chem. Lab. Med. 2016, 54, 1671–1680. [Google Scholar] [CrossRef]
- Wang, J.; Wu, X.; Tian, Y.; Li, X.; Zhao, X.; Zhang, M. Dynamic changes and diagnostic and prognostic significance of serum PCT, hs-CRP and s-100 protein in central nervous system infection. Exp. Ther. Med. 2018, 16, 5156–5160. [Google Scholar] [CrossRef] [Green Version]
- Wu, L.; Feng, Q.; Ai, M.-L.; Deng, S.-Y.; Liu, Z.-Y.; Huang, L.; Ai, Y.H.; Zhang, L. The dynamic change of serum S100B levels from day 1 to day 3 is more associated with sepsis-associated encephalopathy. Sci. Rep. 2020, 10, 7718. [Google Scholar] [CrossRef]








| Characteristic | Infectious Group | Non-Infectious Group | p |
|---|---|---|---|
| Age | 66 (63; 71) | 65 (62; 68) | 0.378 |
| Ejection Fraction | 58 (43; 64) | 60 (50; 66) | 0.630 |
| EuroScore 2 | 1.2 (0.7; 1.6) | 0.9(0.7; 1.27) | 0.318 |
| The total duration of the extracorporeal circulation | 90 (83; 107) | 85 (66; 138) | 0.630 |
| 1st day | |||
| WBC (at the end of the 1st day) | 17.3 (14.3; 24.8) | 14.6 (11.7; 16.3) | 0.178 |
| Lactate max, during the 1st day, including EC | 7.4 (3.5; 9.4) | 4.5 (2.7; 5.9) | 0.03 |
| SOFA | 6 (5; 9) | 5 (2; 6) | 0.03 |
| 3rd day | |||
| WBC (at the end of the 3rd day) | 16.5 (13.3; 22.5) | 10.5 (8.7; 13.8) | 0.01 |
| SOFA | 8 (6; 10) | 1 (1; 3) | 0.0001 |
| 7th day | |||
| WBC (at the end of the 7st day) | 11.9 (8.1; 16.3) | 7.1 (5.9; 9.7) | 0.01 |
| SOFA | 3 (1; 6) | 0 (0; 0) | 0.00001 |
| Length of hospital stay, days | 20 (15; 35) | 13 (13; 14) | 0.001 |
| Day 1, Balance (p. adj) | Day 3, Balance (p. adj) | Day 7, Balance (p. adj) | ||
|---|---|---|---|---|
| Infectious | ||||
| Day 0 | Prevotella/Actinomyces (0.043) | Porphyromonas/Streptococcus (0.039) u_Clostrideacea/Blautia (0.039) Bacteroides/Faecalibacterium (0.039) Corynebacterium/Peptococcus (0.039) Parabacteroides/u_Lachnospiraceae (0.039) | u_Lachnospiraceae/[Eubacterium] (0.013) Bacteroides/Ruminococcus (0.013) | |
| Day 1 | - | - | - | |
| Day 3 | - | - | - | |
| Non-Infectious | ||||
| Day 0 | - | u_Lachnospiraceae/Faecalibacterium (0.04) Dorea/[Ruminococcus] (0.032) | Clostridium/Oscillospira (0.049) Bacteroides/u_Mogibacteriaceae (0.049) [Ruminococcus]/Dialister (0.049) | |
| Day 1 | - | Lactobacillus/u_[Mogibacteriaceae] (0.045) Finegoldia/Peptoniphilus (0.045) Porphyromonas/Campylobacter (0.045) Faecalibacterium/Sutterella (0.009) | u_Clostridiaceae/Oscillospira (0.029) Bacteroides/u_[Mogibacteriaceae] (0.04) Collinsella/Dialister (0.029) [Ruminococcus]/Sutterella (0.018) | |
| Day 3 | - | - | - | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chernevskaya, E.; Zuev, E.; Odintsova, V.; Meglei, A.; Beloborodova, N. Gut Microbiota as Early Predictor of Infectious Complications before Cardiac Surgery: A Prospective Pilot Study. J. Pers. Med. 2021, 11, 1113. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11111113
Chernevskaya E, Zuev E, Odintsova V, Meglei A, Beloborodova N. Gut Microbiota as Early Predictor of Infectious Complications before Cardiac Surgery: A Prospective Pilot Study. Journal of Personalized Medicine. 2021; 11(11):1113. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11111113
Chicago/Turabian StyleChernevskaya, Ekaterina, Evgenii Zuev, Vera Odintsova, Anastasiia Meglei, and Natalia Beloborodova. 2021. "Gut Microbiota as Early Predictor of Infectious Complications before Cardiac Surgery: A Prospective Pilot Study" Journal of Personalized Medicine 11, no. 11: 1113. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11111113