
Dialectical Behaviour Therapy Improves Emotion Dysregulation Mainly in Binge Eating Disorder and Bulimia Nervosa: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Study Selection
2.2. Eligibility Criteria
2.3. Outcomes and Data Extraction
2.4. Quality Assessment and Risk of Bias in the Included Studies
2.5. Statistical Analysis
3. Results
3.1. Study Selection
3.2. Study Characteristics

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author, Year | Study Design | Sample Size (n) | Population Demographics | ED Type and Diagnostic Manual | Treatment | Key Findings Post-Treatment |
|---|---|---|---|---|---|---|
| Dastan et al., 2019 [41] | RCT Follow-up: - | Total: 40 DBT: 20 WL: 20 | Age (range): 18–50 Females: 100% Nationality: Iranian | ED: BED Criteria: DSM-IV Assessment: SCID-I | Intervention: DBT vs. WL (no intervention) Duration: 20 weeks (2 h session/week) | 1. Emotion regulation -EES global, anger/frustration, anxiety subscales: significantly higher improvements in DBT -EES depression: no significant difference 2. BMI: significantly higher reduction in DBT |
| Hill, 2007 [42] | RCT Follow-up: - | Total: 32 DBT: 18 WL: 14 | Age (SD): 22 (6.3) Females: 100% Nationality: American | ED: BN (n = 26) and sub-clinical BN (n = 6) Criteria: DSM-IV Assessment: SCID-I | Intervention: DBT vs. WL (6-week delayed intervention) Duration: 12 weeks (1 h session/week: the length of the first 6 sessions was increased to 90 min) | 1. Emotion regulation -EES, NMRS, PANAS-NA: no significant differences -PANAS-PA, BDI-II: significantly higher improvements in DBT 2. ED psychopathology -EDE-Q global, restraint, shape, eating concern: significantly higher improvements in DBT -Weight concern: no significant differences -OBE: significantly greater reductions in DBT |
| Masson et al., 2013 [39] | RCT Follow-up: 6 months | Total: 60 DBT: 30 WL: 30 | Age (SD): 42.8 (10.5) Females: 88.3% Males: 11.7% Nationality: Canadian | ED: BED Criteria: DSM-IV Assessment: SCID-I and EDE | Intervention: DBT-guided self-help vs. WL (no intervention) Duration: 13 weeks (6 biweekly 20-min support phone calls) | 1. Emotion regulation -DERS: significantly greater improvements in DBT 2. ED psychopathology -EDE-Q all subscales, except eating concern: significantly higher improvements in DBT -OBE: significantly greater reductions in DBT -EDQLS: significantly greater improvements in DBT |
| Rahmani et al., 2018 [43] | RCT Follow-up: - | Total: 60 DBT: 30 WL: 30 | Age (SD): 30.5 (7.5) Females: 100% Nationality: Iranian | ED: BED Criteria: DSM-IV-TR Assessment: SCID-DSM-IV-TR | Intervention: DBT vs. WL (offered treatment at the end of study) Duration: 10 weeks (2 h session/twice a week) | 1. Emotion regulation -DERS: significantly greater improvements in DBT 2. ED psychopathology -BES: significantly greater reductions in DBT 3. BMI: significantly greater reductions in DBT |
| Safer et al., 2001 [44] | RCT Follow-up: - | Total: 29 DBT: 14 WL: 15 | Age (SD): 34 (11) Females: 100% Nationality: American | ED: BN (80.6%) and sub-clinical BN (19.4%) Criteria: DSM-IV Assessment: EDE | Intervention: DBT vs. WL (offered treatment at the end of study) Duration: 20 weeks | 1. Emotion regulation -EES global and subscales, PANAS-NA, NMRS, BDI: significantly greater improvements in DBT -PANAS-PA: no significant differences 2. ED psychopathology -OBE: significantly greater reductions in DBT |
| Telch et al., 2001 [45] | RCT Follow-up: - | Total: 44 DBT: 22 WL: 22 | Age (SD): 50 (6.1) Females: 100% Nationality: American | ED: BED Criteria:DSM-IV Assessment: SCID-I and SCID-II | Intervention: DBT vs. WL (no intervention) Duration: 20 weeks (2 h session/week) | 1. Emotion regulation -EES global, anxiety and depression: no significant differences -EES anger: greater improvements in DBT (borderline significant) -PANAS, NMRS, BDI: no significant differences 2. ED psychopathology -OBE, BES: significantly greater reductions in DBT -EDE-Q weight, shape, eating concern: significantly higher improvements in DBT -EDE-Q global and restraint concern: no significant differences |
| First Author, Year | Study Design | Sample Size (n) | Population Demographics | ED Type and Diagnostic Manual | Treatment | Key Findings Post-Treatment |
|---|---|---|---|---|---|---|
| Adler, 2008 [35] | RCT Follow-up: 18 weeks | Total: 17 DBT: 8 BTP: 9 | Age (SD): 49.4 (11.4) Females: 88.2% Males: 11.8% Nationality: American | ED: BED (subthreshold: n = 4) Criteria: DSM-IV Assessment: EDE | Intervention: DBT + Alli (weight loss drug) vs. BTP + Alli Duration: 12 weeks (2 h session/week) | 1. Emotion regulation -EES, BDI: no significant differences 2. ED psychopathology -OBE: no significant differences -BES: significantly greater reductions in DBT |
| Hoffman, 2006 [38] | RCT Follow-up: - | Total: 101 DBT: 50 SGT: 51 | Age (SD): 51.6 (11.2) Females: 85.1% Males: 14.9% Nationality: American | ED: BED Criteria: DSM-IV Assessment: SCID-I and SCID-II | Intervention: DBT vs. SGT Duration: 20 weeks (2 h session/week) | 1. Emotion regulation -DERS: no significant difference -BDI: significantly greater reductions in DBT 2. ED psychopathology -OBE: significantly greater reductions 3. BMI: no significant differences in DBT |
| Lammers et al., 2020 [37] | Quasi-randomised control trial Follow-up: 6 months | Total: 74 DBT: 41 CBT+: 33 | Age (SD): 37.3 (11.8) Females: 89.2% Males: 10.8% Nationality: Dutch | ED: BED Criteria: DSM-V Assessment: DEBQ and SCID | Intervention: DBT-BED vs. CBT+ Duration: 20 weeks (2 h session/week) | 1. Emotion regulation -DEBQ, EDI-3 (emotion dysregulation), BDI-II: no significant difference 2. ED psychopathology -EDE-Q, EDI-3 (self-esteem), SCL-90: no significant differences -OBE: significantly greater reductions in CBT+ 3. BMI: no significant differences in DBT |
| Navarro-Haro et al., 2020 [36] | Non-randomised control trial Follow-up: 4 and 6 years | Total: 109 DBT: 64 TAU-CBT: 45 | Age (SD): 27.3 (8.1) Females: 100% Nationality: Spanish Comorbidity: BPD | ED: BN, AN or EDNOS Criteria: DSM-IV Assessment: SCID-I | Intervention: DBT vs. TAU-CBT Duration: 6 months (2 h session/week) | 1. Emotion regulation -EES: significantly greater improvements in TAU-CBT -ERQ, BDI-II, PANAS-PA: no significant difference -PANAS-NA: borderline significant |
| Safer et al., 2010 [40] | RCT Follow-up: 3, 6 and 12 months | Total: 101 DBT: 50 ACGT: 51 | Age (SD): 52.2 (10.6) Females: 86% Males: 14% Nationality: American | ED: BED Criteria: DSM-IV Assessment: SCID-I | Intervention: DBT-BED vs. ACGT Duration: 21 weeks (2 h session/week) | 1. Emotion regulation -NMRS, EES, PANAS, DERS: no significant difference -BDI: significantly greater reductions in DBT 2. ED psychopathology -EDE-Q global and eating concern: significantly greater improvements in DBT -Restraint, weight and shape concern: no significant improvements in DBT -OBE: significantly reduced in DBT 3. BMI: no significant differences |
3.3. Quality Assessment
3.4. Effectiveness of DBT
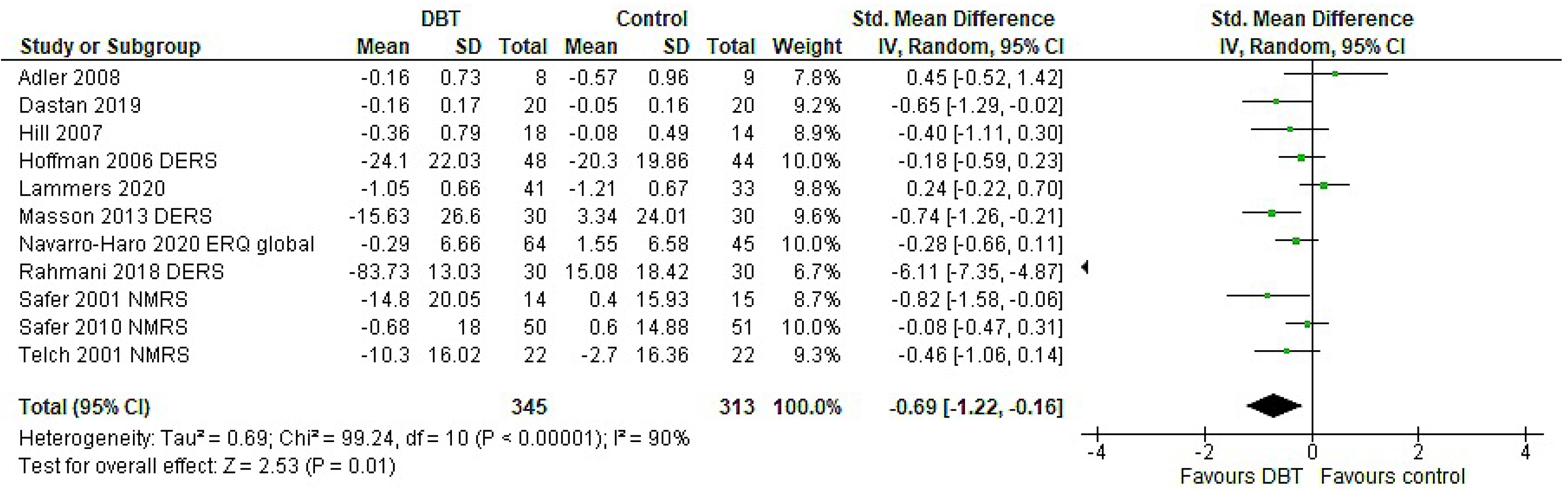
3.4.1. Emotion Regulation (ER)
Subgroup Analyses
3.4.2. ED Psychopathology
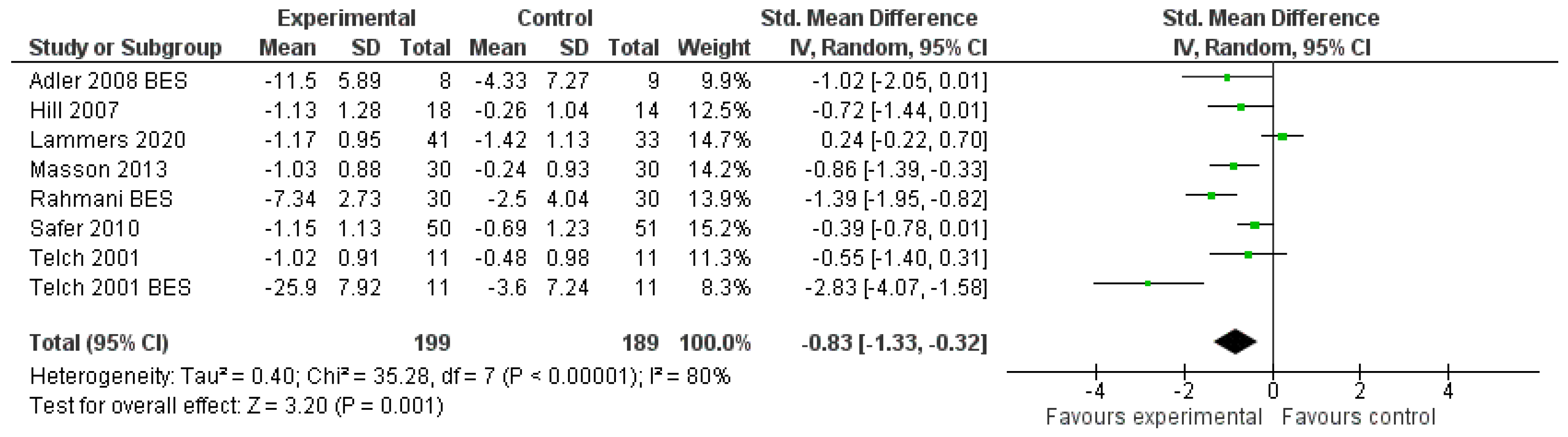
Severity of Symptoms
Objective Binge Episodes (OBE)
Subgroup Analyses
3.4.3. Body Mass Index (BMI)
Subgroup Analyses
3.5. Meta-Regression Analysis
3.6. Publication Bias
4. Discussion
4.1. Emotion Regulation (ER)
4.2. ED Psychopathology
4.3. Body Mass Index (BMI)
4.4. Subgroup Analyses
4.5. Strengths and Limitations
Quality of the Included Studies and Heterogeneity
4.6. Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ACGT | Active Comparison Group Therapy |
| AN | Anorexia Nervosa |
| BDI | Beck Depression inventory |
| BED | Binge Eating Disorder |
| BES | Binge Eating Scale |
| BMI | Body Mass Index |
| BN | Bulimia Nervosa |
| BPD | Borderline Personality Disorder |
| BTP | Behavioural Treatment Plan |
| CBT | Cognitive Behaviour Therapy |
| CBT-E | Enhanced CBT |
| CI | Confidence Interval |
| DBT | Dialectical Behaviour Therapy |
| DEBQ | Dutch Eating Behaviour Questionnaire |
| DERS | Difficulties in Emotion Regulation Scale |
| DSM | The Diagnostic and Statistical Manual of Mental Disorders |
| ED | Eating Disorder(s) |
| EDE-Q | Eating Disorder Examination Questionnaire |
| EDI-3 | Eating Disorder Inventory |
| EDNOS | Eating Disorder Not Otherwise Specified |
| EDQLS | The Eating Disorder Quality of Life Scale |
| EES | Emotional Eating Scale |
| ER | Emotion Regulation |
| IPT | Interpersonal Psychotherapy |
| MD | Mean Difference |
| NMRS | Negative Mood Regulation Scale |
| OBE | Objective Binge Episode(s) |
| OMI | Outcome Measure Instrument(s) |
| OSFED | Other Specified Eating Disorders |
| PANAS | Positive and Negative Affect Schedule |
| RCT | Randomised controlled trial(s) |
| ROB 2 | Risk of Bias |
| ROBINS-I | Risk of Bias in Non-randomised Studies |
| SCID | Structural Clinical Interview for DSM |
| SCL-90 | The Symptom Checklist |
| SGT | Supportive Group Therapy |
| SD | Standard Deviation |
| TAU | Treatment as Usual |
Appendix A
| Outcome | DBT (n) | Control (n) | MD/g | 95 CI% | p | I sq. | p for I sq. |
|---|---|---|---|---|---|---|---|
| Primary ER | 345 | 313 | −0.69 | [−1.22; −0.16] | 0.01 | 90% | <0.00001 |
| Overall ER | 1206 | 1071 | −0.46 | [−0.67; −0.26] | <0.00001 | 81% | <0.00001 |
| General ER | 408 | 368 | −0.66 | [−1.13; −0.19] | 0.006 | 89% | <0.00001 |
| Eating ER | 237 | 209 | −0.15 | [−0.51; 0.21] | 0.41 | 69% | 0.002 |
| Depressive symptoms | 588 | 533 | −0.33 | [−0.45; −0.20] | <0.00001 | 9% | 0.35 |
| Severity of symptoms | 221 | 211 | −0.9 | [−1.45; −0.34] | 0.002 | 86% | <0.00001 |
| OBEs | 232 | 218 | −0.27 | [−0.45; −0.09] | 0.003 | 85% | <0.00001 |
| BMI | 204 | 195 | −1.93 | [−3.42; −0.44] | 0.01 | 32% | 0.2 |
| Outcome | DBT (n) | Control (n) | MD/g | 95 CI% | p | I sq. | p for I sq. |
|---|---|---|---|---|---|---|---|
| Overall ER | 346 | 292 | −0.42 | [−0.68; −0.16] | 0.001 | 53% | <0.0001 |
| General ER | 317 | 284 | −0.70 | [−1.23; −0.18] | 0.009 | 89% | <0.00001 |
| Depressive symptoms | 286 | 253 | −0.28 | [−0.46; −0.11] | 0.001 | 0% | 0.93 |
| Severity of symptoms | 199 | 189 | −0.83 | [−1.33; −0.32] | 0.001 | 80% | 0.00001 |
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar] [CrossRef]
- Galmiche, M.; Déchelotte, P.; Lambert, G.; Tavolacci, M.P. Prevalence of eating disorders over the 2000–2018 period: A systematic literature review. Am. J. Clin. Nutr. 2019, 109, 1402–1413. [Google Scholar] [CrossRef]
- Arcelus, J.; Mitchell, A.J.; Wales, J.; Nielsen, S. Mortality rates in patients with anorexia nervosa and other eating disorders: A meta-analysis of 36 studies. Arch. Gen. Psychiatry 2011, 68, 724–731. [Google Scholar] [CrossRef] [Green Version]
- Dobrescu, S.R.; Dinkler, L.; Gillberg, C.; Råstam, M.; Gillberg, C.; Wentz, E. Anorexia nervosa: 30-year outcome. Br. J. Psychiatry 2020, 216, 97–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steinhausen, H.C.; Weber, S. The Outcome of Bulimia Nervosa: Findings From One-Quarter Century of Research. Am. J. Psychiatry 2009, 166, 1331–1341. [Google Scholar] [CrossRef] [PubMed]
- Working Group of the Clinical Practice Guideline for Eating Disorders. Clinical Practice Guideline for Eating Disorders; Catalan Agency for Health Technology Assessment and Research: Spain, 2009. [Google Scholar]
- Brockmeyer, T.; Skunde, M.; Wu, M.; Bresslein, E.; Rudofsky, G.; Herzog, W.; Friederich, H.C. Difficulties in emotion regulation across the spectrum of eating disorders. Compr. Psychiatry 2014, 55, 565–571. [Google Scholar] [CrossRef] [PubMed]
- Gross, J.J. The Emerging Field of Emotion Regulation: An Integrative Review. Rev. Gen. Psychol. 1998, 2, 271–299. [Google Scholar] [CrossRef]
- Thompson, R.A. Emotional regulation and emotional development. Educ. Psychol. Rev. 1991, 3, 269–307. [Google Scholar] [CrossRef]
- Federici, A.; Wisniewski, L.; Ben-Porath, D. Description of an Intensive Dialectical Behavior Therapy Program for Multidiagnostic Clients With Eating Disorders. J. Couns. Dev. 2012, 90, 330–338. [Google Scholar] [CrossRef]
- Monell, E.; Clinton, D.; Birgegård, A. Self-directed behaviors differentially explain associations between emotion dysregulation and eating disorder psychopathology in patients with or without objective binge-eating. J. Eat. Disord. 2020, 8, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, S.G.; Asnaani, A.; Vonk, I.J.; Sawyer, A.T.; Fang, A. The efficacy of cognitive behavioral therapy: A review of meta-analyses. Cogn. Ther. Res. 2012, 36, 427–440. [Google Scholar] [CrossRef] [Green Version]
- Murphy, R.; Straebler, S.; Basden, S.; Cooper, Z.; Fairburn, C.G. Interpersonal psychotherapy for eating disorders. Clin. Psychol. Psychother. 2012, 19, 150–158. [Google Scholar] [CrossRef] [Green Version]
- Kass, A.E.; Kolko, R.P.; Wilfley, D.E. Psychological treatments for eating disorders. Curr. Opin. Psychiatry 2013, 26, 549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lipsitz, J.D.; Markowitz, J.C. Mechanisms of change in interpersonal therapy (IPT). Clin. Psychol. Rev. 2013, 33, 1134–1147. [Google Scholar] [CrossRef] [Green Version]
- Linehan, M.M. Cognitive-Behavioral Treatment of Borderline Personality Disorder; Cognitive-Behavioral Treatment of Borderline Personality disorder; Guilford Press: New York, NY, USA, 1993; p. 558. [Google Scholar]
- Crowell, S.E.; Beauchaine, T.P.; Linehan, M.M. A biosocial developmental model of borderline personality: Elaborating and extending linehan’s theory. Psychol. Bull. 2009, 135, 495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swales, M.; Dunkley, C. Principles of skills assessment in dialectical behavior therapy. Cogn. Behav. Pract. 2020, 27, 18–29. [Google Scholar] [CrossRef]
- Wisniewski, L.; Kelly, E. The application of dialectical behavior therapy to the treatment of eating disorders. Cogn. Behav. Pract. 2003, 10, 131–138. [Google Scholar] [CrossRef]
- Bankoff, S.M.; Karpel, M.G.; Forbes, H.E.; Pantalone, D.W. A Systematic Review of Dialectical Behavior Therapy for the Treatment of Eating Disorders. Eat. Disord. 2012, 20, 196–215. [Google Scholar] [CrossRef]
- Brown, T.A.; Wisniewski, L.; Anderson, L.K. Dialectical Behavior Therapy for Eating Disorders: State of the Research and New Directions. Eat. Disord. 2020, 28, 97–100. [Google Scholar] [CrossRef]
- Ben-Porath, D.; Duthu, F.; Luo, T.; Gonidakis, F.; Compte, E.J.; Wisniewski, L. Dialectical behavioral therapy: An update and review of the existing treatment models adapted for adults with eating disorders. Eat. Disord. 2020, 28, 101–121. [Google Scholar] [CrossRef]
- Claudat, K.; Brown, T.A.; Anderson, L.; Bongiorno, G.; Berner, L.A.; Reilly, E.; Luo, T.; Orloff, N.; Kaye, W.H. Correlates of co-occurring eating disorders and substance use disorders: A case for dialectical behavior therapy. Eat. Disord. 2020, 28, 142–156. [Google Scholar] [CrossRef]
- Hill, D.M.; Craighead, L.W.; Safer, D.L. Appetite-focused dialectical behavior therapy for the treatment of binge eating with purging: A preliminary trial. Int. J. Eat. Disord. 2011, 44, 249–261. [Google Scholar] [CrossRef]
- Safer, D.L.; Couturier, J.L.; Lock, J. Dialectical behavior therapy modified for adolescent binge eating disorder: A case report. Cogn. Behav. Pract. 2007, 14, 157–167. [Google Scholar] [CrossRef]
- Telch, C.F.; Agras, W.S.; Linehan, M.M. Group dialectical behavior therapy for binge-eating disorder: A preliminary, uncontrolled trial. Behav. Ther. 2000, 31, 569–582. [Google Scholar] [CrossRef]
- Salbach-Andrae, H.; Bohnekamp, I.; Pfeiffer, E.; Lehmkuhl, U.; Miller, A.L. Dialectical behavior therapy of anorexia and bulimia nervosa among adolescents: A case series. Cogn. Behav. Pract. 2008, 15, 415. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372. [Google Scholar] [CrossRef]
- Higgins, J. Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1. 0 [updated March 2011]; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- The Endnote Team. Endnote 20. Available online: https://endnote.com/product-details?fbclid=IwAR3u61_oF_pdAD_XuIxvAjB-HdUGCimo9NKFsGQBmLhyv6rwlqKjHRh6b48 (accessed on 15 September 2021).
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- the Cochrane Collaboration. RevMan 5.4.1. Available online: https://training.cochrane.org/online-learning/core-software-cochrane-reviews/revman/revman-5-download (accessed on 15 September 2021).
- Kinney, A.R.; Eakman, A.M.; Graham, J.E. Novel effect size interpretation guidelines and an evaluation of statistical power in rehabilitation research. Arch. Phys. Med. Rehabil. 2020, 101, 2219–2226. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adler, S. Orlistat/alli as Compared to Orlistat/alli Plus Dialectical Behavior Therapy in Overweight Binge Eaters: A Randomized Control Trial. Ph.D. Thesis, Pacific Graduate School of Psychology, Palo Alto, CA, USA, 2008. [Google Scholar]
- Navarro-Haro, M.V.; Botella, V.G.; Badenes-Ribera, L.; Borao, L.; García-Palacios, A. Dialectical Behavior Therapy in the Treatment of Comorbid Borderline Personality Disorder and Eating Disorder in a Naturalistic Setting: A Six-Year Follow-up Study. Cogn. Ther. Res. 2020, 45, 480–493. [Google Scholar] [CrossRef]
- Lammers, M.W.; Vroling, M.S.; Crosby, R.D.; Strien, T.V. Dialectical behavior therapy adapted for binge eating compared to cognitive behavior therapy in obese adults with binge eating disorder: A controlled study. J. Eat. Disord. 2020, 8, 1–11. [Google Scholar] [CrossRef]
- Hoffman, J.E. Alliance as a Predictor of Outcome in Group Psychotherapy for Binge Eating Disorder: Making the Most Predictive Model through Exploration of Mediation and Moderation. Ph.D. Thesis, PGSP-Stanford PsyD Consortium, Palo Alto, CA, USA, 2006. [Google Scholar]
- Masson, P.C.; Von Ranson, K.M.; Wallace, L.M.; Safer, D.L. A randomized wait-list controlled pilot study of dialectical behaviour therapy guided self-help for binge eating disorder. Behav. Res. Ther. 2013, 51, 723–728. [Google Scholar] [CrossRef]
- Safer, D.L.; Robinson, A.H.; Jo, B. Outcome From a Randomized Controlled Trial of Group Therapy for Binge Eating Disorder: Comparing Dialectical Behavior Therapy Adapted for Binge Eating to an Active Comparison Group Therapy. Behav. Ther. 2010, 41, 106–120. [Google Scholar] [CrossRef] [Green Version]
- Dastan, B.; Zanjani, S.A.; Adl, A.F.; Habibi, M. The effectiveness of dialectical behaviour therapy for treating women with obesity suffering from BED: A feasibility and pilot study. Clin. Psychol. 2019, 24, 133–142. [Google Scholar] [CrossRef]
- Hill, D.M. Appetite-Focused Dialectical Behavior Therapy for the Treatment of Binge Eating with Purging: A Randomized Controlled Trial. Ph.D. Thesis, University of Colorado, Boulder, CO, USA, 2007. [Google Scholar]
- Rahmani, M.; Omidi, A.; Asemi, Z.; Akbari, H. The effect of dialectical behaviour therapy on binge eating, difficulties in emotion regulation and BMI in overweight patients with binge-eating disorder: A randomized controlled trial. Ment. Health Prev. 2018, 9, 13–18. [Google Scholar] [CrossRef]
- Safer, D.L.; Telch, C.F.; Agras, W.S. Dialectical Behavior Therapy for Bulimia Nervosa. Am. J. Psychiatry 2001, 158, 632–634. [Google Scholar] [CrossRef] [Green Version]
- Telch, C.F.; Agras, W.S.; Linehan, M.M. Dialectical behavior therapy for binge eating disorder. J. Consult. Clin. Psychol. 2001, 69, 1061–1065. [Google Scholar] [CrossRef]
- Harvey, L.J.; Hunt, C.; White, F.A. Dialectical Behaviour Therapy for Emotion Regulation Difficulties: A Systematic Review. Behav. Chang. 2019, 36, 143–164. [Google Scholar] [CrossRef] [Green Version]
- Benzerouk, F.; Djerada, Z.; Bertin, E.; Barrière, S.; Gierski, F.; Kaladjian, A. Contributions of Emotional Overload, Emotion Dysregulation, and Impulsivity to Eating Patterns in Obese Patients with Binge Eating Disorder and Seeking Bariatric Surgery. Nutrition 2020, 12, 3099. [Google Scholar] [CrossRef] [PubMed]
- Stapleton, P.; Whitehead, M. Dysfunctional Eating in an Australian Community Sample: The Role of Emotion Regulation, Impulsivity, and Reward and Punishment Sensitivity. Aust. Psychol. 2014, 49, 358–368. [Google Scholar] [CrossRef] [Green Version]
- Braden, A.; Musher-Eizenman, D.; Watford, T.; Emley, E. Eating when depressed, anxious, bored, or happy: Are emotional eating types associated with unique psychological and physical health correlates? Appetite 2018, 125, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Barnhart, W.R.; Braden, A.L.; Price, E. Emotion regulation difficulties interact with negative, not positive, emotional eating to strengthen relationships with disordered eating: An exploratory study. Appetite 2021, 158, 105038. [Google Scholar] [CrossRef] [PubMed]
- Lenz, A.S.; Taylor, R.; Fleming, M.; Serman, N. Effectiveness of dialectical behavior therapy for treating eating disorders. J. Couns. Dev. 2014, 92, 26–35. [Google Scholar] [CrossRef]
- deloitte Access Economics. Social and Economic Cost of Eating Disorders in the United States of America Report for the Strategic Training Initiative for the Prevention of Eating Disorders and the Academy for Eating Disorders. Available online: https://www.hsph.harvard.edu/striped/report-economic-costs-of-eating-disorders/ (accessed on 15 September 2021).
- Youssef, G.; Plancherel, B.; Laget, J.; Corcos, M.; Flament, M.F.; Halfon, O. Personality trait risk factors for attempted suicide among young women with eating disorders. Eur. Psychiatry 2004, 19, 131–139. [Google Scholar] [CrossRef]
- Harley, R.; Sprich, S.; Safren, S.; Jacobo, M.; Fava, M. Adaptation of dialectical behavior therapy skills training group for treatment-resistant depression. J. Nerv. Ment. Dis. 2008, 196, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Tylka, T.L. The Relation between Body Dissatisfaction and Eating Disorder Symptomatology: An Analysis of Moderating Variables. J. Couns. Psychol. 2004, 51. [Google Scholar] [CrossRef] [Green Version]
- Winkler, L.A.D.; Christiansen, E.; Lichtenstein, M.B.; Hansen, N.B.; Bilenberg, N.; Støving, R.K. Quality of life in eating disorders: A meta-analysis. Psychiatry Res. 2014, 219, 1–9. [Google Scholar] [CrossRef]
- Roosen, M.A.; Safer, D.; Adler, S.; Cebolla, A.; van Strien, T.; van Strien, T. Group dialectical behavior therapy adapted for obese emotional eaters; a pilot study. Nutr. Hosp. 2012, 27, 1141–1147. [Google Scholar] [CrossRef] [PubMed]
- Ricca, V.; Castellini, G.; Lo Sauro, C.; Ravaldi, C.; Lapi, F.; Mannucci, E.; Rotella, C.M.; Faravelli, C. Correlations between binge eating and emotional eating in a sample of overweight subjects. Appetite 2009, 53, 418–421. [Google Scholar] [CrossRef] [PubMed]
- Van Strien, T.V.; Engels, R.C.M.E.; Leeuwe, J.V.; Snoek, H.M. The Stice model of overeating: Tests in clinical and non-clinical samples. Appetite 2005, 45, 205–213. [Google Scholar] [CrossRef]
- Barnes, R.D.; Boeka, A.G.; McKenzie, K.C.; Genao, I.; Garcia, R.L.; Ellman, M.S.; Ellis, P.J.; Masheb, R.M.; Grilo, C.M. Metabolic syndrome in obese patients with binge-eating disorder in primary care clinics: A cross-sectional study. Prim. Care Companion J. Clin. Psychiatry 2011, 13. [Google Scholar] [CrossRef]
- Fairburn, C.G.; Cooper, Z.; Doll, H.A.; Norman, P.; O’Connor, M. The natural course of bulimia nervosa and binge eating disorder in young women. Arch. Gen. Psychiatry 2000, 57. [Google Scholar] [CrossRef] [PubMed]
- Field, A.E.; Sonneville, K.R.; Micali, N.; Crosby, R.D.; Swanson, S.A.; Laird, N.M.; Treasure, J.; Solmi, F.; Horton, N.J. Prospective Association of Common Eating Disorders and Adverse Outcomes. Pediatrics 2012, 130, e289–e295. [Google Scholar] [CrossRef] [Green Version]
- Sonneville, K.R.; Horton, N.J.; Micali, N.; Crosby, R.D.; Swanson, S.A.; Solmi, F.; Field, A.E. Longitudinal Associations between Binge Eating and Overeating and Adverse Outcomes Among Adolescents and Young Adults: Does Loss of Control Matter? JAMA Pediatr. 2013, 167, 149–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Channon, S.; De Silva, P.; Hemsley, D.; Perkins, R. A controlled trial of cognitive-behavioural and behavioural treatment of anorexia nervosa. Behav. Res. Ther. 1989, 27, 529–535. [Google Scholar] [CrossRef]
- Ball, J.; Mitchell, P. A randomized controlled study of cognitive behavior therapy and behavioral family therapy for anorexia nervosa patients. Eat. Disord. 2004, 12, 303–314. [Google Scholar] [CrossRef]
- Murray, S.B.; Griffiths, S.; Mond, J.M. Evolving eating disorder psychopathology: Conceptualising muscularity-oriented disordered eating. Br. J. Psychiatry 2016, 208, 414–415. [Google Scholar] [CrossRef] [Green Version]
- Murray, S.B.; Nagata, J.M.; Griffiths, S.; Calzo, J.P.; Brown, T.A.; Mitchison, D.; Blashill, A.J.; Mond, J.M. The enigma of male eating disorders: A critical review and synthesis. Clin. Psychol. Rev. 2017, 57, 1–11. [Google Scholar] [CrossRef]
- Addis, M.E.; Mahalik, J.R. Men, masculinity, and the contexts of help seeking. Am. Psychol. 2003, 58, 5. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez, J.M.; Alegría, M.; Prihoda, T.J.; Copeland, L.A.; Zeber, J.E. How the relationship of attitudes toward mental health treatment and service use differs by age, gender, ethnicity/race and education. Soc. Psychiatry Psychiatr. Epidemiol. 2011, 46, 45–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monell, E.; Clinton, D.; Birgegård, A. Emotion dysregulation and eating disorders—Associations with diagnostic presentation and key symptoms. Int. J. Eat. Disord. 2018, 51, 921–930. [Google Scholar] [CrossRef] [PubMed]
- Fassbinder, E.; Schweiger, U.; Martius, D.; Brand-de Wilde, O.; Arntz, A. Emotion Regulation in Schema Therapy and Dialectical Behavior Therapy. Front. Psychol. 2016, 1373. [Google Scholar] [CrossRef] [Green Version]
- May, J.M.; Richardi, T.M.; Barth, K.S. Dialectical behavior therapy as treatment for borderline personality disorder. Ment. Health Clin. 2016, 6, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Stanley, K. Design of Randomized Controlled Trials. Circulation 2007, 115, 1164–1169. [Google Scholar] [CrossRef]
- Nair, B. Clinical Trial Designs. Indian Dermatol. Online J. 2019, 10, 201. [Google Scholar] [CrossRef]
- Williamson, P.R.; Altman, D.G.; Blazeby, J.M.; Clarke, M.; Devane, D.; Gargon, E.; Tugwell, P. Developing core outcome sets for clinical trials: Issues to consider. Trials 2012, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bjureberg, J.; Ljótsson, B.; Tull, M.T.; Hedman, E.; Sahlin, H.; Lundh, L.G.; Bjärehed, J.; DiLillo, D.; Messman-Moore, T.; Gumpert, C.H.; et al. Development and Validation of a Brief Version of the Difficulties in Emotion Regulation Scale: The DERS-16. J. Psychopathol. Behav. Assess. 2016, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gross, J.J.; John, O.P. Individual Differences in Two Emotion Regulation Processes: Implications for Affect, Relationships, and Well-Being. J. Personal. Soc. Psychol. 2003, 85. [Google Scholar] [CrossRef] [PubMed]
- Charles, S.T.; Pasupathi, M. Age-related patterns of variability in self-descriptions: Implications for everyday affective experience. Psychol. Aging 2003, 18. [Google Scholar] [CrossRef] [PubMed]
- Röcke, C.; Li, S.C.; Smith, J. Intraindividual Variability in Positive and Negative Affect Over 45 Days: Do Older Adults Fluctuate Less Than Young Adults? Psychol. Aging 2009, 24. [Google Scholar] [CrossRef]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rozakou-Soumalia, N.; Dârvariu, Ş.; Sjögren, J.M. Dialectical Behaviour Therapy Improves Emotion Dysregulation Mainly in Binge Eating Disorder and Bulimia Nervosa: A Systematic Review and Meta-Analysis. J. Pers. Med. 2021, 11, 931. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11090931
Rozakou-Soumalia N, Dârvariu Ş, Sjögren JM. Dialectical Behaviour Therapy Improves Emotion Dysregulation Mainly in Binge Eating Disorder and Bulimia Nervosa: A Systematic Review and Meta-Analysis. Journal of Personalized Medicine. 2021; 11(9):931. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11090931
Chicago/Turabian StyleRozakou-Soumalia, Natalia, Ştefana Dârvariu, and Jan Magnus Sjögren. 2021. "Dialectical Behaviour Therapy Improves Emotion Dysregulation Mainly in Binge Eating Disorder and Bulimia Nervosa: A Systematic Review and Meta-Analysis" Journal of Personalized Medicine 11, no. 9: 931. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11090931