
Association between Statin Use and Risk of Parkinson’s Disease: Evidence from 18 Observational Studies Comprising 3.7 Million Individuals


 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
2.1. Data Sources and Search Strategies
2.2. Eligibility Criteria
2.3. Data Extraction
2.4. Study Quality Assessment
2.5. Statistical Analysis
3. Results
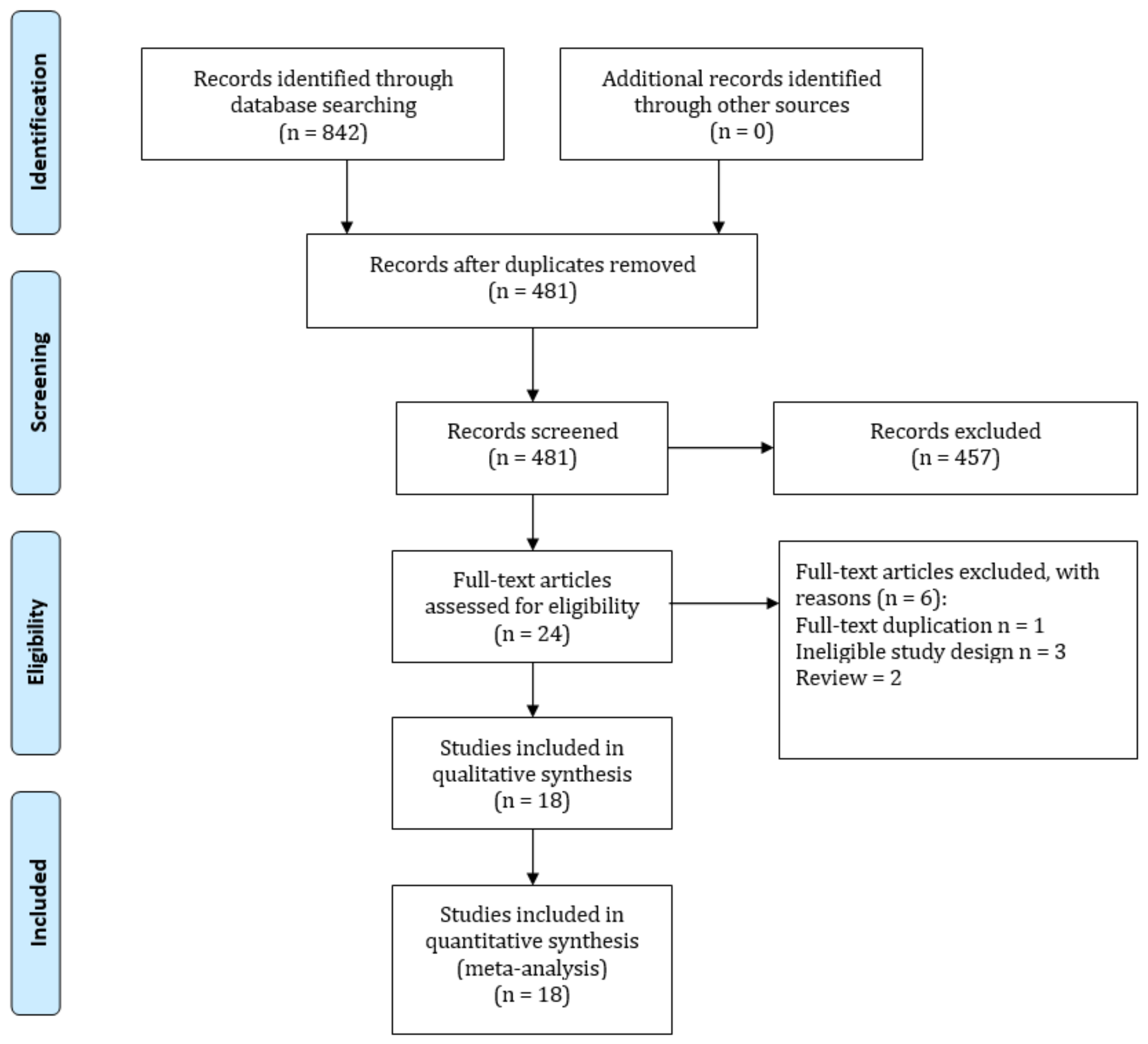
3.1. Study Identification
3.2. Study Characteristics and Quality Assessment
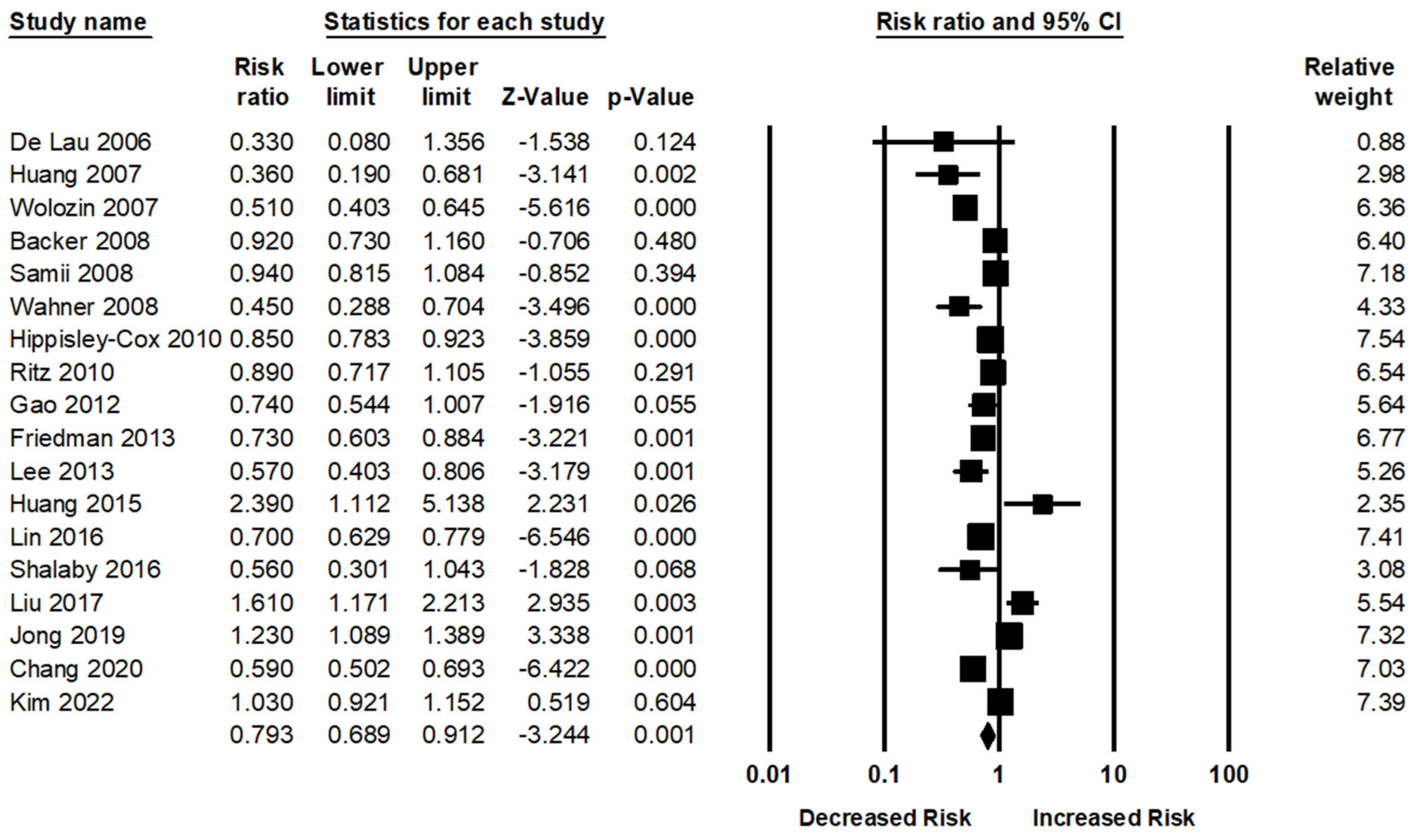
3.3. Statin Use and PD Risk
3.4. Subgroup Analysis
3.5. Sensitivity Analysis
3.6. Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Poly, T.N.; Islam, M.; Yang, H.-C.; Li, Y.-C.J. Non-steroidal anti-inflammatory drugs and risk of Parkinson’s disease in the elderly population: A meta-analysis. Eur. J. Clin. Pharmacol. 2019, 75, 99–108. [Google Scholar] [CrossRef] [PubMed]
- Dorsey, E.R.; Elbaz, A.; Nichols, E.; Abbasi, N.; Abd-Allah, F.; Abdelalim, A.; Adsuar, J.C.; Ansha, M.G.; Brayne, C.; Choi, J.-Y.J. Global, regional, and national burden of Parkinson’s disease, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018, 17, 939–953. [Google Scholar] [CrossRef] [Green Version]
- Feigin, V.L.; Abajobir, A.A.; Abate, K.H.; Abd-Allah, F.; Abdulle, A.M.; Abera, S.F.; Abyu, G.Y.; Ahmed, M.B.; Aichour, A.N.; Aichiour, I. Global, regional, and national burden of neurological disorders during 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Neurol. 2017, 16, 877–897. [Google Scholar] [CrossRef] [Green Version]
- Pezzoli, G.; Cereda, E. Exposure to pesticides or solvents and risk of Parkinson disease. Neurology 2013, 80, 2035–2041. [Google Scholar] [CrossRef]
- Gorell, J.M.; Peterson, E.L.; Rybicki, B.A.; Johnson, C.C. Multiple risk factors for Parkinson’s disease. J. Neurol. Sci. 2004, 217, 169–174. [Google Scholar] [CrossRef]
- Lai, B.; Marion, S.; Teschke, K.; Tsui, J.K.C. Occupational and environmental risk factors for Parkinson’s disease. Parkinsonism Relat. Disord. 2002, 8, 297–309. [Google Scholar] [CrossRef]
- Wechsler, L.S.; Checkoway, H.; Franklin, G.M.; Costa, L.G. A pilot study of occupational and environmental risk factors for Parkinson’s disease. Neurotoxicology 1991, 12, 387–392. [Google Scholar]
- Seidler, A.; Hellenbrand, W.; Robra, B.-P.; Vieregge, P.; Nischan, P.; Joerg, J.; Oertel, W.H.; Ulm, G.; Schneider, E. Possible environmental, occupational, and other etiologic factors for Parkinson’s disease: A case-control study in Germany. Neurology 1996, 46, 1275-1275. [Google Scholar] [CrossRef]
- Priyadarshi, A.; Khuder, S.A.; Schaub, E.A.; Shrivastava, S. A meta-analysis of Parkinson’s disease and exposure to pesticides. Neurotoxicology 2000, 21, 435–440. [Google Scholar]
- Weisskopf, M.G.; Weuve, J.; Nie, H.; Saint-Hilaire, M.-H.; Sudarsky, L.; Simon, D.K.; Hersh, B.; Schwartz, J.; Wright, R.O.; Hu, H. Association of cumulative lead exposure with Parkinson’s disease. Environ. Health Perspect. 2010, 118, 1609–1613. [Google Scholar] [CrossRef]
- Vlaar, T.; Kab, S.; Schwaab, Y.; Fréry, N.; Elbaz, A.; Moisan, F. Association of Parkinson’s disease with industry sectors: A French nationwide incidence study. Eur. J. Epidemiol. 2018, 33, 1101–1111. [Google Scholar] [CrossRef]
- Priyadarshi, A.; Khuder, S.A.; Schaub, E.A.; Priyadarshi, S.S. Environmental risk factors and Parkinson’s disease: A metaanalysis. Environ. Res. 2001, 86, 122–127. [Google Scholar] [CrossRef] [Green Version]
- Miller, P.E.; Martin, S.S. Approach to statin use in 2016: An update. Curr. Atheroscler. Rep. 2016, 18, 20. [Google Scholar] [CrossRef]
- Nanna, M.G.; Navar, A.M.; Zakroysky, P.; Xiang, Q.; Goldberg, A.C.; Robinson, J.; Roger, V.L.; Virani, S.S.; Wilson, P.W.F.; Elassal, J.; et al. Association of patient perceptions of cardiovascular risk and beliefs on statin drugs with racial differences in statin use: Insights from the patient and provider assessment of lipid management registry. JAMA Cardiol. 2018, 3, 739–748. [Google Scholar] [CrossRef] [Green Version]
- Hussain, M.A.; Saposnik, G.; Raju, S.; Salata, K.; Mamdani, M.; Tu, J.V.; Bhatt, D.L.; Verma, S.; Al-Omran, M. Association between statin use and cardiovascular events after carotid artery revascularization. J. Am. Heart Assoc. 2018, 7, e009745. [Google Scholar] [CrossRef]
- Islam, M.; Poly, T.N.; Walther, B.A.; Yang, H.-C.; Li, Y.-C.J. Statin use and the risk of hepatocellular carcinoma: A meta-analysis of observational studies. Cancers 2020, 12, 671. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Tang, W.; Wang, J.; Xie, L.; Li, T.; He, Y.; Deng, Y.; Peng, Q.; Li, S.; Qin, X. Association between statin use and colorectal cancer risk: A meta-analysis of 42 studies. Cancer Causes Control 2014, 25, 237–249. [Google Scholar] [CrossRef]
- Nielsen, S.F.; Nordestgaard, B.G.; Bojesen, S.E. Statin use and reduced cancer-related mortality. N. Engl. J. Med. 2012, 367, 1792–1802. [Google Scholar] [CrossRef] [Green Version]
- Manthravadi, S.; Shrestha, A.; Madhusudhana, S. Impact of statin use on cancer recurrence and mortality in breast cancer: A systematic review and meta-analysis. Int. J. Cancer 2016, 139, 1281–1288. [Google Scholar] [CrossRef]
- Poly, T.N.; Islam, M.M.; Walther, B.A.; Yang, H.-C.; Wu, C.-C.; Lin, M.-C.; Li, Y.-C. Association between use of statin and risk of dementia: A meta-analysis of observational studies. Neuroepidemiology 2020, 54, 214–226. [Google Scholar] [CrossRef]
- Marques, N.F.; Castro, A.A.; Mancini, G.; Rocha, F.L.; Santos, A.R.S.; Prediger, R.D.; De Bem, A.F.; Tasca, C.I. Atorvastatin prevents early oxidative events and modulates inflammatory mediators in the striatum following intranasal 1-methyl-4-phenyl-1, 2, 3, 6-tetrahydropyridine (MPTP) administration in rats. Neurotox. Res. 2018, 33, 549–559. [Google Scholar] [CrossRef]
- Bai, S.; Song, Y.; Huang, X.; Peng, L.; Jia, J.; Liu, Y.; Lu, H. Statin use and the risk of Parkinson’s disease: An updated meta-analysis. PLoS ONE 2016, 11, e0152564. [Google Scholar] [CrossRef] [Green Version]
- Sheng, Z.; Jia, X.; Kang, M. Statin use and risk of Parkinson’s disease: A meta-analysis. Behav. Brain Res. 2016, 309, 29–34. [Google Scholar] [CrossRef]
- Undela, K.; Gudala, K.; Malla, S.; Bansal, D. Statin use and risk of Parkinson’s disease: A meta-analysis of observational studies. J. Neurol. 2013, 260, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Yan, J.; Qiao, L.; Tian, J.; Liu, A.; Wu, J.; Huang, J.; Shen, M.; Lai, X. Effect of statins on Parkinson’s disease: A systematic review and meta-analysis. Medicine 2019, 98, e14852. [Google Scholar] [CrossRef] [PubMed]
- Bykov, K.; Yoshida, K.; Weisskopf, M.G.; Gagne, J.J. Confounding of the association between statins and Parkinson disease: Systematic review and meta-analysis. Pharmacoepidemiol. Drug Saf. 2017, 26, 294–300. [Google Scholar] [CrossRef]
- Poly, T.N.; Islam, M.M.; Walther, B.A.; Yang, H.-C.; Nguyen, P.-A.; Huang, C.-W.; Shabbir, S.-A.; Li, Y.-C. Exploring the association between statin use and the risk of Parkinson’s disease: A meta-analysis of observational studies. Neuroepidemiology 2017, 49, 142–151. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Moher, D. Evaluations of the uptake and impact of the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) Statement and extensions: A scoping review. Syst. Rev. 2017, 6, 263. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Robertson, J.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; Oxford Publisher: Oxford, UK, 2000. [Google Scholar]
- Jackson, D.; White, I.R.; Thompson, S.G. Extending DerSimonian and Laird’s methodology to perform multivariate random effects meta-analyses. Stat. Med. 2010, 29, 1282–1297. [Google Scholar] [CrossRef]
- Brockwell, S.E.; Gordon, I.R. A comparison of statistical methods for meta-analysis. Stat. Med. 2001, 20, 825–840. [Google Scholar] [CrossRef] [PubMed]
- Poly, T.; Islam, M.; Yang, H.-C.; Wu, C.; Li, Y.-C. Proton pump inhibitors and risk of hip fracture: A meta-analysis of observational studies. Osteoporos. Int. 2019, 30, 103–114. [Google Scholar] [CrossRef]
- Islam, M.; Yang, H.-C.; Nguyen, P.-A.; Poly, T.N.; Huang, C.-W.; Kekade, S.; Khalfan, A.M.; Debnath, T.; Li, Y.-C. Exploring association between statin use and breast cancer risk: An updated meta-analysis. Arch. Gynecol. Obstet. 2017, 296, 1043–1053. [Google Scholar] [CrossRef]
- De Lau, L.M.; Stricker, B.H.; Breteler, M.M. Serum cholesterol, use of lipid-lowering drugs, and risk of Parkinson disease. Mov. Disord. 2007, 22, 1985. [Google Scholar] [CrossRef]
- Wolozin, B.; Wang, S.W.; Li, N.-C.; Lee, A.; Lee, T.A.; Kazis, L.E. Simvastatin is associated with a reduced incidence of dementia and Parkinson’s disease. BMC Med. 2007, 5, 20. [Google Scholar] [CrossRef] [Green Version]
- Huang, X.; Chen, H.; Miller, W.C.; Mailman, R.B.; Woodard, J.L.; Chen, P.C.; Xiang, D.; Murrow, R.W.; Wang, Y.-Z.; Poole, C. Lower low-density lipoprotein cholesterol levels are associated with Parkinson’s disease. Mov. Disord Off. J. Mov. Disord. Soc. 2007, 22, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Samii, A.; Carleton, B.C.; Etminan, M. Statin use and the risk of Parkinson disease: A nested case control study. J. Clin. Neurosci. 2008, 15, 1272–1273. [Google Scholar] [CrossRef]
- Wahner, A.D.; Bronstein, J.M.; Bordelon, Y.M.; Ritz, B. Statin use and the risk of Parkinson disease. Neurology 2008, 70, 1418–1422. [Google Scholar] [CrossRef] [Green Version]
- Becker, C.; Jick, S.S.; Meier, C.R. Use of statins and the risk of Parkinson’s disease. Drug Saf. 2008, 31, 399–407. [Google Scholar] [CrossRef]
- Ritz, B.; Manthripragada, A.D.; Qian, L.; Schernhammer, E.; Wermuth, L.; Olsen, J.; Friis, S. Statin use and Parkinson’s disease in Denmark. Mov. Disord. 2010, 25, 1210–1216. [Google Scholar] [CrossRef] [Green Version]
- Hippisley-Cox, J.; Coupland, C. Unintended effects of statins in men and women in England and Wales: Population based cohort study using the QResearch database. BMJ 2010, 340, c2197. [Google Scholar] [CrossRef] [Green Version]
- Gao, X.; Simon, K.C.; Schwarzschild, M.A.; Ascherio, A. Prospective study of statin use and risk of Parkinson disease. Arch. Neurol. 2012, 69, 380–384. [Google Scholar] [CrossRef] [Green Version]
- Friedman, B.; Lahad, A.; Dresner, Y.; Vinker, S. Long-term statin use and the risk of Parkinson’s disease. Am. J. Manag. Care 2013, 19, 626–632. [Google Scholar]
- Huang, X.; Alonso, A.; Guo, X.; Umbach, D.M.; Lichtenstein, M.L.; Ballantyne, C.M.; Mailman, R.B.; Mosley, T.H.; Chen, H. Statins, plasma cholesterol, and risk of Parkinson’s disease: A prospective study. Mov. Disord. 2015, 30, 552–559. [Google Scholar] [CrossRef]
- Lee, Y.-C.; Lin, C.-H.; Wu, R.-M.; Lin, M.-S.; Lin, J.-W.; Chang, C.-H.; Lai, M.-S. Discontinuation of statin therapy associates with Parkinson disease: A population-based study. Neurology 2013, 81, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Shalaby, S.Y.; Louis, E.D. Statin use and its association with essential tremor and Parkinson’s disease. Neuroepidemiology 2016, 47, 11–17. [Google Scholar] [CrossRef] [Green Version]
- Liu, G.; Sterling, N.W.; Kong, L.; Lewis, M.M.; Mailman, R.B.; Chen, H.; Leslie, D.; Huang, X. Statins may facilitate Parkinson’s disease: Insight gained from a large, national claims database. Mov. Disord. 2017, 32, 913–917. [Google Scholar] [CrossRef]
- Jeong, S.M.; Jang, W.; Shin, D.W. Association of statin use with Parkinson’s disease: Dose–response relationship. Mov. Disord. 2019, 34, 1014–1021. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.-H.; Yen, S.-J.; Chang, Y.-H.; Wu, W.-J.; Lin, K.-D. Pioglitazone and statins lower incidence of Parkinson disease in patients with diabetes mellitus. Eur. J. Neurol. 2021, 28, 430–437. [Google Scholar] [CrossRef]
- Kim, J.H.; Chang, I.B.; Kim, Y.H.; Kwon, M.J.; Kim, J.-H.; Choi, H.G. Association between statin use and Parkinson’s disease in Korean patients with hyperlipidemia. Parkinsonism Relat. Disord. 2022, 97, 15–24. [Google Scholar] [CrossRef]
- Yan, J.; Xu, Y.; Zhu, C.; Zhang, L.; Wu, A.; Yang, Y.; Xiong, Z.; Deng, C.; Huang, X.-F.; Yenari, M.A.; et al. Simvastatin prevents dopaminergic neurodegeneration in experimental parkinsonian models: The association with anti-inflammatory responses. PLoS ONE 2011, 6, e20945. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.-Z.; Wu, S.-C.; Kwan, A.-L.; Lin, C.-L. Preconditioning with pitavastatin, an HMG-CoA reductase inhibitor, attenuates C-Jun N-terminal kinase activation in experimental subarachnoid hemorrhage-induced apoptosis. Acta Neurochir. 2015, 157, 1031–1041. [Google Scholar] [CrossRef]
- Banach, M. Lipid-lowering nutraceuticals in clinical practice: Position paper from an International Lipid Expert Panel. Nutr. Rev. 2017, 75, 731–767. [Google Scholar]
- Wang, Q.; Yan, J.; Chen, X.; Li, J.; Yang, Y.; Weng, J.; Deng, C.; Yenari, M.A. Statins: Multiple neuroprotective mechanisms in neurodegenerative diseases. Exp. Neurol. 2011, 230, 27–34. [Google Scholar] [CrossRef]
- Hu, G.; Antikainen, R.; Jousilahti, P.; Kivipelto, M.; Tuomilehto, J. Total cholesterol and the risk of Parkinson disease. Neurology 2008, 70, 1972–1979. [Google Scholar] [CrossRef]
- Doria, M.; Maugest, L.; Moreau, T.; Lizard, G.; Vejux, A. Contribution of cholesterol and oxysterols to the pathophysiology of Parkinson’s disease. Free. Radic. Biol. Med. 2016, 101, 393–400. [Google Scholar] [CrossRef]
- Xu, X.; Gao, W.; Dou, S.; Cheng, B. Simvastatin inhibited the apoptosis of PC12 cells induced by 1-methyl-4-phenylpyridinium ion via inhibiting reactive oxygen species production. Cell. Mol. Neurobiol. 2013, 33, 69–73. [Google Scholar] [CrossRef]
- Tan, W.; Xue-bin, C.; Tian, Z.; Xiao-Wu, C.; Pei-Pei, H.; Zhi-Bin, C.; Bei-Sha, T. Effects of simvastatin on the expression of inducible nitric oxide synthase and brain-derived neurotrophic factor in a lipopolysaccharide-induced rat model of Parkinson disease. Int. J. Neurosci. 2016, 126, 278–286. [Google Scholar] [CrossRef]
- Yood, M.U.; McCarthy, B.D.; Kempf, J.; Kucera, G.P.; Wells, K.; Oliveria, S.; Stang, P. Racial differences in reaching target low-density lipoprotein goal among individuals treated with prescription statin therapy. Am. Heart J. 2006, 152, 777–784. [Google Scholar] [CrossRef]
- Clark, L.T.; Maki, K.C.; Galant, R.; Maron, D.J.; Pearson, T.A.; Davidson, M.H. Ethnic Differences in Achievement of Cholesterol Treatment Goals: Results from the National Cholesterol Education Program Evaluation Project Utilizing Novel E-Technology II. J. Gen. Intern. Med. 2006, 21, 320–326. [Google Scholar] [CrossRef] [Green Version]
- Gans, K.M.; Burkholder, G.J.; Risica, P.M.; Laster, T.M. Baseline Fat-Related Dietary Behaviors of White, Hispanic, and Black Participants in a Cholesterol Screening and Education Project in New England; Elsevier: Amsterdam, The Netherlands, 2003. [Google Scholar]
- Patterson, R.E.; Kristal, A.; Rodabough, R.; Caan, B.; Lillington, L.; Mossavar-Rahmani, Y.; Simon, M.S.; Snetselaar, L.; Horn, L.V. Changes in food sources of dietary fat in response to an intensive low-fat dietary intervention: Early results from the Women’s Health Initiative. J. Am. Diet. Assoc. 2003, 103, 454–460. [Google Scholar]
- Crespo, C.J.; Smit, E.; Andersen, R.E.; Carter-Pokras, O.; Ainsworth, B.E. Race/ethnicity, social class and their relation to physical inactivity during leisure time: Results from the Third National Health and Nutrition Examination Survey, 1988–1994. Am. J. Prev. Med. 2000, 18, 46–53. [Google Scholar] [CrossRef]
- Schachter, M. Chemical, pharmacokinetic and pharmacodynamic properties of statins: An update. Fundam. Clin. Pharmacol. 2005, 19, 117–125. [Google Scholar] [CrossRef]
- Patrick, L.; Uzick, M. Cardiovascular disease: C-reactive protein and the inflammatory disease paradigm: HMG-CoA reductase inhibitors, alpha-tocopherol, red yeast rice, and olive oil polyphenols. A review of the literature. Altern. Med. Rev. 2001, 6, 248–271. [Google Scholar]
- Sierra, S.; Ramos, M.C.; Molina, P.; Esteo, C.; Vázquez, J.A.; Burgos, J.S. Statins as neuroprotectants: A comparative in vitro study of lipophilicity, blood-brain-barrier penetration, lowering of brain cholesterol, and decrease of neuron cell death. J. Alzheimers Dis. 2011, 23, 307–318. [Google Scholar] [CrossRef]
- Van der Most, P.J.; Dolga, A.M.; Nijholt, I.M.; Luiten, P.G.; Eisel, U.L. Statins: Mechanisms of neuroprotection. Prog. Neurobiol. 2009, 88, 64–75. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study | Publication Year | Study Duration | Study Type | Population | PD Cases | Definition of Statin Use | Identification of Statin Users | Country | Quality Score |
|---|---|---|---|---|---|---|---|---|---|
| De Lau | 2006 | 1990–2004 | Co | 6465 | 87 | Medical record | ATC | Netherland | 8 |
| Huang | 2007 | 2002–2004 | C-C | 236 | 124 | Medical record | ATC | USA | 7 |
| Wolozin | 2007 | 2003–2005 | Co | 1,226,198 | 5107 | Database | ATC | USA | 6 |
| Becker | 2008 | 1994–2005 | C-C | 7274 | 3637 | Medical records | ATC | UK | 9 |
| Samii | 2008 | 1997–2003 | C-C | 23,780 | 4756 | Medical records | ATC | Canada | 6 |
| Wahner | 2008 | 2001–2007 | C-C | 654 | 312 | Self-report | ATC | USA | 7 |
| HippisleyCox | 2010 | 2002–2008 | Co | 2,004,692 | 3553 | Database | ATC | UK | 6 |
| Ritz | 2010 | 2001–2006 | C-C | 11,582 | 1931 | Medical report | ATC | Denmark | 7 |
| Gao | 2012 | 1994–2006 | Co | 129,006 | 644 | Self-report | ATC | USA | 7 |
| Friedman | 2013 | 2000–2007 | Co | 87,971 | 824 | Database | ATC | Israel | 8 |
| Lee | 2013 | 2001–2008 | Co | 43,810 | 1886 | Database | ATC | China | 9 |
| Huang | 2015 | 1987–2008 | Co | 15,291 | 56 | Medical records | ATC | USA | 6 |
| Lin | 2016 | 1996–2008 | Co | 50,432 | 651 | Database | ATC | China | 8 |
| Shalaby | 2016 | 2009–2014 | C-C | 230 | 108 | Self-report | ATC | USA | 7 |
| Liu | 2017 | 2008–2012 | C-C | 4644 | 2322 | Database | ATC | USA | 7 |
| Jong | 2019 | 2002–2015 | Co | 76,043 | 1427 | Database | ATC | USA | 8 |
| Chang | 2020 | 1996–2013 | Co | 48828 | 692 | Database | ATC | Taiwan | 8 |
| Kim | 2022 | 2002–2015 | C-C | 15,130 | 3036 | Database | ATC | South Korea | 8 |
| Study | No of Studies | Pooled Estimates | Test of Heterogeneity | |||
|---|---|---|---|---|---|---|
| RR (95% CI) | p-Value | Q Value | p Value | I2 (%) | ||
| All studies | 18 | 0.79 (0.68–0.91) | 0.001 | 149.02 | <0.001 | 82.05 |
| Study design | ||||||
| Cohort | 10 | 0.75 (0.62–0.91) | 0.004 | 98.14 | <0.001 | 90.83 |
| Case–control | 8 | 0.85 (0.70–1.04) | 0.09 | 35.35 | <0.001 | 80.19 |
| Region | ||||||
| North America | 9 | 0.81 (0.60–1.09) | 0.17 | 85.20 | <0.001 | 90.61 |
| Europe | 4 | 0.85 (0.79–0.92) | <0.001 | 2.26 | <0.001 | 0 |
| Asia | 5 | 0.71 (0.57–0.90) | 0.005 | 42.86 | <0.001 | 90.66 |
| Adjusted for age | ||||||
| Yes | 14 | 0.80 (0.66–0.97) | 0.02 | 125.79 | <0.001 | 89.66 |
| No | 4 | 0.75 (0.61–0.92) | 0.006 | 21.36 | <0.001 | 85.96 |
| Adjusted for gender | ||||||
| Yes | 13 | 0.84 (0.69–1.03) | 0.06 | 102.57 | <0.001 | 88.30 |
| No | 5 | 0.69 (0.58–0.82) | <0.001 | 21.91 | <0.001 | 81.74 |
| Adjusted for smoking status | ||||||
| Yes | 10 | 0.78 (0.62–0.97) | 0.02 | 86.14 | <0.001 | 89.14 |
| No | 8 | 0.79 (0.65–0.96) | 0.02 | 56.60 | <0.001 | 87.63 |
| Quality of Studies | ||||||
| Medium | 10 | 0.79 (0.64–0.97) | 0.02 | 59.85 | <0.001 | 84.96 |
| High | 8 | 0.79 (0.63–0.98) | 0.03 | 88.93 | <0.001 | 92.12 |
| Statin type | ||||||
| Simvastatin | 6 | 0.67 (0.53–0.84) | 0.001 | 111.29 | <0.001 | 93.71 |
| Atorvastatin | 5 | 0.73 (0.59–0.90) | 0.003 | 32.80 | <0.001 | 81.71 |
| Lovastatin | 3 | 0.89 (0.65–1.21) | 0.46 | 6.26 | 0.005 | 81.02 |
| Pravastatin | 3 | 1.09 (0.65–1.84) | 0.72 | 6.56 | 0.08 | 54.30 |
| Study year | ||||||
| ≤5 | 3 | 0.68 (0.28–1.65) | 0.39 | 37.41 | <0.001 | 94.65 |
| ≤10 | 7 | 0.76 (0.66–0.88) | <0.001 | 18.61 | 0.005 | 67.77 |
| >10 | 8 | 0.88 (0.69–1.11) | 0.29 | 87.86 | <0.001 | 92.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, C.-C.; Islam, M.M.; Lee, A.-J.; Su, C.-H.; Weng, Y.-C.; Yeh, C.-Y.; Lee, H.-H.; Lin, M.-C. Association between Statin Use and Risk of Parkinson’s Disease: Evidence from 18 Observational Studies Comprising 3.7 Million Individuals. J. Pers. Med. 2022, 12, 825. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12050825
Wu C-C, Islam MM, Lee A-J, Su C-H, Weng Y-C, Yeh C-Y, Lee H-H, Lin M-C. Association between Statin Use and Risk of Parkinson’s Disease: Evidence from 18 Observational Studies Comprising 3.7 Million Individuals. Journal of Personalized Medicine. 2022; 12(5):825. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12050825
Chicago/Turabian StyleWu, Chieh-Chen, Md. Mohaimenul Islam, An-Jen Lee, Chun-Hsien Su, Yung-Ching Weng, Chih-Yang Yeh, Hsun-Hua Lee, and Ming-Chin Lin. 2022. "Association between Statin Use and Risk of Parkinson’s Disease: Evidence from 18 Observational Studies Comprising 3.7 Million Individuals" Journal of Personalized Medicine 12, no. 5: 825. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12050825