

Effects of Different Nocturnal Lighting Stimuli on Melatonin, Sleep and Cognitive Performance of Workers in Confined Spaces

1
Shanghai Sunshine Rehabilitation Center, Shanghai Yangzhi Rehabilitation Hospital, School of Medicine, Tongji University, Shanghai 201619, China
2
School of Architecture and Urban Planning, Tongji University, Shanghai 200092, China
3
Key Laboratory of Ecology and Energy-Saving Study of Dense Habitat, Tongji University, Ministry of Education, Shanghai 200092, China
*
Author to whom correspondence should be addressed.
Buildings 2023, 13(8), 2112; https://0-doi-org.brum.beds.ac.uk/10.3390/buildings13082112
Submission received: 27 July 2023
/
Revised: 14 August 2023
/
Accepted: 18 August 2023
/
Published: 21 August 2023
(This article belongs to the Special Issue Lighting in Buildings)
Abstract
:Exposure to light during overtime work at night in confined spaces may disrupt the normal circadian clock, affect hormone secretion, sleep quality and performance, thereby posing great risks to the physical and mental health of night workers. Integrative lighting should be adopted to reduce the disturbance of normal physiological rhythm, while meeting the visual requirements of work. Through adjustable LED (CCT 6000 K/2700 K) and different vertical illuminance, five lighting patterns with different circadian stimuli (CS = 0.60, 0.30. 0.20, 0.10 and 0.05) were conducted, respectively, in a sleep lab using a within-subject design. Each lighting pattern lasted for 5 h every night. Eight healthy adults were recruited to complete the night work and their salivary melatonin, Karolinska sleepiness scale (KSS), Psychomotor Vigilance Task (PVT) and sleep quality were tested. The results showed that subjective sleepiness and melatonin concentration increased rapidly under low intervention (CS = 0.05) with the best sleep quality, while they decreased in high intervention (CS = 0.60) at night and led to significantly higher levels of sleepiness the next morning (p < 0.05). For the PVT, the middle intervention (CS = 0.30) showed the lowest response time and least errors (p < 0.05), suggesting that appropriate illuminance can improve visual performance. To reduce biorhythm disruptions, lower lighting stimulation is preferred during night work. For difficult visual tasks, high illuminances may not improve visual performance; just a slight increase in the existing lighting levels is adequate. Lighting interventions have a clear impact on sleep improvement and work capacity for those working overtime, and they may be translatable to other shift work scenarios.
1. Introduction
In modern society, there is an increasing demand for night work, with overtime or shift work becoming rather common. More and more office staff and workers have to work at night [1]. Particularly in confined spaces such as underground stations, underground shopping malls and underground control centres, people are often required to work until midnight. Due to the mismatch between working time and daily biological clock, the reduction and deprivation of sleeping time, and the suppression of light on the normal secretion of melatonin, improper light at night can aggravate problems of sleep rhythm, breast cancer [2], obesity and chronic diseases [3,4,5]. It is necessary to improve the lighting strategy and carry out integrative lighting [6,7] or Human-Centric Lighting (HCL) [8,9] to reduce the disturbance of normal physiological rhythms while meeting the visual requirements and performance of work [10,11,12].
With the discovery of the intrinsically photosensitive retinal ganglion cells (ipRGCs), the study of the biological effects of light has increased [13]. Night overtime work has a negative impact on circadian rhythm and mental health with the disturbance of internal rhythms also reducing performance and cognitive ability [14], leading to sleep problems, fatigue and decreased alertness [15]. Stimulation with bright light in the evening and at night (before the time of core body temperature minimum) could lead to the backward shift of the rhythm phase [16], while light rich in blue light in the morning was reported to induce the circadian rhythm phase to move forward and improve cognitive performance [17,18]. The alerting effect of light at dusk or night can also improve attention and memory ability [19,20], and bright light has been proven to have mood enhancing effects [6] on people with SAD and depression [21]. In an actual hospital project, ICU nurses working night shifts were exposed to 10 h of high illuminance (1500–2000 lx) white light, which reduced sleepiness but increased psychomotor errors on mental alertness tasks compared with a 300 lx standard lighting condition [22].
The Lighting Research Center (LRC) suggested a high circadian stimulus (CS ≥ 0.3) light during the day (at least for the first 2–3 h of the morning) and a low CS (<0.1) light during the evening to avoid the disruption of sleep and circadian rhythms thorough a series of field and laboratory research [23,24]. A dynamic light that changed the spectrum and illuminance throughout the waking period can promote better melatonin secretion and sleep initiation than static light [11,25,26]. CIE S 026:2018 “CIE System for Metrology of Optical Radiation for ipRGC-Influenced Responses to Light” [27] and position statements on non-visual effects of light [28] also suggest the use of high melanopic equivalent daylight illuminance (melanopic EDI) light during the day to improve alertness, circadian rhythm and nocturnal sleep, and the use of low melanopic EDI light at night to facilitate sleep; however, these recommendations lack specific numerical requirements. WELL Standard V2 recommends that the ocular vertical illuminance (melanopic EDI or equivalent melanopic lux (EML)), achieved on the vertical plane at eye level to simulate the light entering the eye, should be at least a certain level of illuminance between 9:00 and 13:00 and can be appropriately lowered after 20:00 [29]. “Recommendations for Healthy Daytime, Evening, and Night-Time Indoor Light Exposure” by the expert consensus from the fields of lighting, neurophysiological photometry, sleep and circadian rhythm research recommended that at least 250 lx melanopic EDI of vertical illuminance should be achieved at 1.2 m height during the day, and daylight should be preferred; at night, within 10 lx melanopic EDI at least 3 h before going to bed and it should not exceed 1 lx melanopic EDI during sleep [30]. Generally, existing studies have established light recommendations mainly for daytime work and nighttime rest but they are less suitable in the case of overtime work at night. In practical applications, a melanopic EDI illuminance at 10 lx is far from enough to meet the requirements of normal work.
Designing a reasonable lighting strategy for night work in confined spaces that reduces the negative influence on hormone secretion and circadian rhythm and ensures adequate visual and cognitive performance is a critical issue that needs to be explored. In order to test the comprehensive effects of different nocturnal lighting stimulations on sleep quality, rhythm phase and cognitive performance, lighting environments with high, medium and low circadian stimuli were used and were compared with the simulated current lighting conditions, with the aim to obtain the appropriate combination of light parameters for night work in confined spaces.
2. Materials and Methods
2.1. Experimental Conditions
To avoid daylight effects and simulate the confined spaces, two identical windowless basement rooms were used to create the “sleep lab” equipped with a central air-conditioning and ventilation system. Each room’s indoor furniture, soft furnishings and lighting scene were identical (Figure 1a). Each room can accommodate four people in two bunk beds. To simulate the layout of the real dormitories, the participants slept on the same bed each time they came to the laboratory. Dimming light panels were adopted and the correlated colour temperature (CCT) could vary from 2700 K to 6000 K. Four LED panel lights are installed 2.2 metres above the floor directly above the table in each room to provide different levels of lighting circadian stimuli. Five lighting scenes were pre-set with an intelligent lighting control system. The desktop horizontal illuminance and the eye-level vertical illuminance were calibrated using a tripod-mounted illuminance spectrophotometer (CL-500A, KONICA MINOL, Tokyo, Japan). Figure 1b shows the relative spectral power distribution (SPD) of different lighting scenes (6000 K and 2700 K CCT) which was measured in the middle of the table facing-up towards the light sources.
The experiment was carried out from 19:00 to 24:00 each night, and a fixed lighting scene was adopted. A total of 5 scenes of lighting modes with different circadian stimuli were designed, as shown in Table 1. Based on the lighting status of the offices investigated in the early stage, the simulation current lighting scene (CLS, CS = 0.1) was set using the working plane illuminance at 150 lx with a CCT of 6000 K. Since office lighting standards require 300 lx of desktop [31] illuminance, the designed lighting scene (DLS) was set at 300 lx and 6000 K (CS = 0.2). The circadian stimulus (CS) model, used to characterize the influence of nocturnal light stimulation on the suppression of human melatonin [32], suggested that CS ≤ 0.05 had little influence on the circadian stimulation. Therefore, the low light intervention scene (LIS, CS = 0.05) was set to a lower CCT of 2700 K to achieve a higher eye illuminance (about 43 lx). Considering that when CS value reaches 0.3, it will have a significant impact on circadian rhythm, a medium intervention scene (MIS, CS = 0.3) with 200 lx eye illuminance and 6000 K CCT was set. To achieve an obvious intervention effect, the high intervention scene (HIG, CS = 0.6) with about 1250 lx eye illuminance and 6000 K CCT was specially set to observe the changes in cognitive performance and hormone concentration.
The horizontal illuminance of the working surface was measured on the table using the grid method at 0.75 m above the floor, and the vertical illuminance of the eyes was 1.2 m above the floor where the participants were sitting. The CS value of each point was calculated using the circadian stimulus model proposed by Rea M [33] and the melanopic EDI was calculated as the average value using the toolbox of CIE S 026:2018.
2.2. Participant Selection
Referring to the methodology of small-sample studies of long-term confined experiments, such as the “Space 180” large science experiment (4 subjects) [34], the “Mars 500” simulated manned flight to Mars (6 subjects) [35] and the “ Moon Palace 365” experiment (4 subjects) [36], Lowden et al. conducted a dynamic lighting intervention with 7 shift workers in a windowless control room of a nuclear power plant [37], and Nie et al. used a light pattern that simulated daylight to allow 3 subjects to work shifts in an underground confined environment for 38 consecutive days [38]. This experiment served as a pre-experiment for the long-term confined experiment and a repeated measurement experiment design was also used. Eight participants, college students used to living in dormitories, were recruited, with four of them being males and the another four being females (age 26.25 ± 2.11 years old; range 23–30 years old). Each person was subjected to a repeated-measures experiment designed for within-subjects analyses, reducing the effect of individual differences. Participants had no long-term habit of smoking, drinking and coffee, no history of drug dependence, normal visual acuity or corrected visual acuity, and no eye diseases such as colour blindness or weakness. There were no significant differences in gender and age between groups (p > 0.05). This study was reviewed by the Medical and Life Sciences Ethics Committee of Tongji University (No. 2021tjdx069), and all participants had signed informed consent and received an experimental remuneration.
2.3. Experimental Protocol
Three days before the experiment day, the participants were required to wear a sleep bracelet to monitor sleep quality and to ensure regular work and rest. Each experiment lasted for one night, and the participants could carry out normal activities in the daytime. They arrived at the sleep laboratory at 18:30 and could read and write during the lighting stimulation from 19:00 to 24:00 to simulate the night work in a confined space. Electronic devices such as mobile phones and computers were not allowed, except at 21:30 for a five-minute Psychomotor Vigilance Task (PVT) test on iPads, with very low brightness and a dark grey background pattern to avoid the impact on sleep and melatonin secretion. They went to bed immediately after the test at midnight and woke up at 8:00 the next day and could not leave the lab until the test was complete. After resting for at least three days (washout period), the experiment was repeated with the next lighting scene (Figure 2).
2.4. Testing Methods
2.4.1. Collection and Processing of Saliva Melatonin Samples
The concentration of melatonin in saliva was detected through ELISA, and the cotton swabs were collected via chewing with saliva collection tubes at night (19:00, 20:00, 21:00, 22:00, 23:00 and 24:00). Food and water were forbidden within 10 min of the collection. The swabs were placed in the mouth and the saliva was stimulated with chewing for more than 45 s. Then, the drug swabs attached with saliva were returned to the saliva collection tubes and plugged. The saliva collection tubes were centrifuged at a speed of 2500 r/min for 5 min. The supernatant was taken and stored in centrifuge tubes and quickly placed in a low-temperature freezer at −40 °C. Saliva samples were measured using Saliva ELISA Kit from IBL International GmbH (tested by Wayen Biotechnologies (Shanghai), Inc., Shanghai, China). The detection range of salivary melatonin was 0–50 pg/mL, the intra-assay coefficient of variation (CV) was less than 10.8%, and the inter-assay CV was less than 13.0%.
2.4.2. Evaluation of Sleep Quality
The participants wore smart sleep wristbands (Huawei B4 Pro) [39] throughout the experiment to monitor sleep duration, time of falling asleep and waking up, and the ratio of deep sleep and light sleep. They woke up at 8:00, filled out the Pittsburgh Sleep Questionnaire and sleep diary immediately after waking, and reported subjectively whether they had symptoms of sleep disturbance. From the Pittsburgh Sleep Questionnaire used to evaluate subjective sleep quality [40], the Pittsburgh Sleep Quality Index (PSQI) was calculated based on the subjective ratings of seven aspects, such as subjective sleep quality, sleep efficiency (sleeping time and the ratio of time in bed), sleep latency period (from the bed to sleep the required length), the number of awakenings, sleep time, sleep disorder, daytime dysfunction and sleep medicine.
2.4.3. Cognitive Ability Test
The Psychomotor Vigilance Task (PVT) has been used as a method of attention evaluation in a lot of studies, which can quantitatively indicate alertness and speed of cognitive response [41,42]. A 5 min PVT test was performed at 21:30 after 2.5 h of light stimulation. The participants looked at the iPads with a dark grey background pattern whose luminance was very low (less than 0.2 cd/m2), clicked the screen once a number appeared, and recorded the reaction time (in milliseconds) from the appearance of the number to clicking on the screen. If the screen was clicked in advance, the number of errors would be recorded. The average response time and error numbers can be used to indicate the participants’ alertness and concentration levels.
2.4.4. Karolinska Sleepiness Scale (KSS)
The subjective scores of alertness were scored hourly using the KSS from 19:00 [43]. The level of alertness and sleepiness was ranked based on a 9-level Likert scale, with 1 indicating being most alert and awake and 9 indicating most sleepy and tired. The KSS sleepiness score was obtained by completing the KSS sleepiness questionnaire every hour.
2.5. Data Analysis
The experimental data were statistically analyzed using IBM SPSS Statistics 23.0 software, and the measurement data were expressed as Mean ± SD. Comparison between scenes was performed via paired sample T-test and the Wilcoxon signed-rank test was used if the indicators were not normally distributed; p < 0.05 means the difference was statistically significant.
3. Results
To understand the effects of different lighting patterns on the human body, four aspects were evaluated separately in terms of subjective sleepiness, melatonin concentration, sleep quality and PVT tests.
3.1. Evaluation of Subjective Sleepiness (KSS Scores)
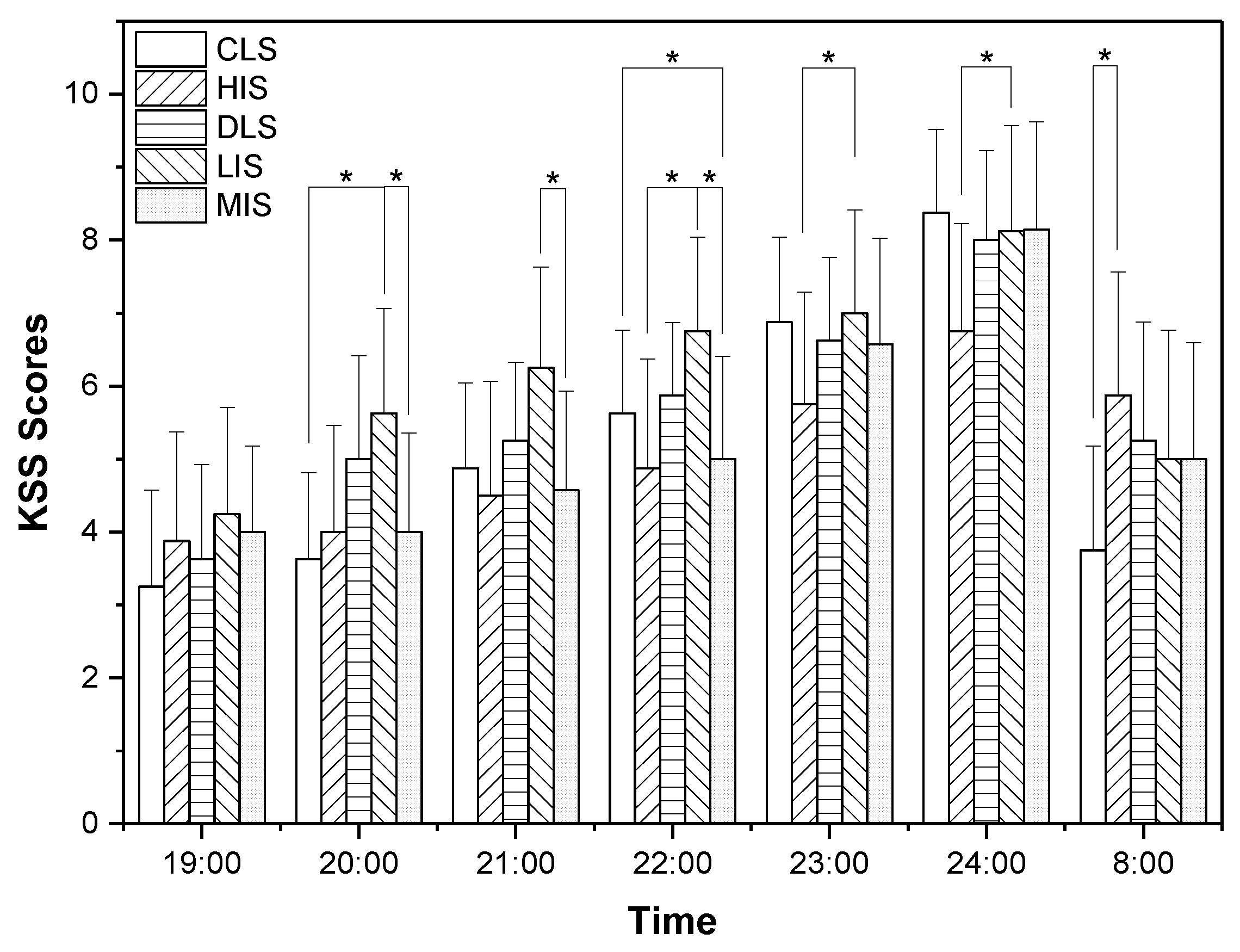
Figure 3 presents the variations in KSS scores during this experiment. Subjective sleepiness accessed with the KSS shows an increasing trend during the night and is maintained at a high level before sleep. It can be seen that at 19:00 there was nearly no significant difference in KSS scores across the different lighting conditions. Then, the LIS increased rapidly at 20:00, which was significantly higher than CLS (p = 0.022) and MIS (p = 0.044). At 21:00, the LIS still remained the highest, and was significantly higher than MIS (p = 0.030). At 22:00, the sleepiness degree of HIS was the lowest, while the LIS remained the highest, and the differences between HIS and LIS, CLS and MIS, LIS and MIS were significant (p < 0.05). The situation that occurred at 23:00 was similar to that at 22:00, with the lowest score in HIS and the highest in LIS, and the difference between them (HIS and LIS) was detected to be statistically significant (p = 0.038). At 24:00, the KSS score of HIS remained the lowest, and the sleepiness degree was significantly lower than LIS (p = 0.020). However, HIS showed the highest KSS score at 8:00 when the subjects woke up, and it was significantly higher than CLS (p = 0.024). Subjective sleepiness remained the lowest in the bright light scene during the night, but presented the highest level during the next morning. The changing trend in sleepiness degree in other scenes was similar, but the difference was not significant.
3.2. Analysis of Melatonin
Elevated levels of melatonin during the night will promote drowsiness and lead to more sleepiness [44,45]. Exposure to light at night may inhibit melatonin secretion, acutely affecting the melatonin onset and resetting the circadian rhythm of melatonin [46]. The area under the curve (AUC) of saliva melatonin [47] was calculated using the trapezoidal method for each patient (Figure 4). To detect the differences in the AUC of melatonin across nights affected by various lighting conditions, the paired T test was utilized. The AUC of melatonin during LIS was the highest, but there was no significant difference between LIS and other nights (p > 0.05). In LIS, the stimulation of light was the least, as was the suppression of melatonin. The AUC values of the other scenes were very close to each other, among which HIS showed the highest light level and the lowest average value of AUC, but without statistical significance. It was speculated that melatonin would be severely inhibited when the lighting stimulus at night reached a certain illuminance for a long time. Even moderate illuminance has a similar inhibitory effect on melatonin similar to high illuminance when stimulated for 5 h at night, which needs special attention during long hours of overtime work at night.
At the beginning (19:00), the melatonin concentration of the MIS was significantly higher than the CLS (p = 0.027), and there was no significant difference between the other paired comparison across scenes (Figure 5). After an hour, LIS showed the highest concentration, which was significantly higher than MIS (p = 0.021), while HIS showed the lowest concentration without significant difference. At 21:00, no significant difference was detected. At 22:00, the concentration of LIS remained the highest, significantly higher than DLS (p = 0.029) and MIS (p = 0.005). The concentration of CLS was also significantly higher than DLS (p = 0.028) and MIS (p = 0.018). At 23:00 and 24:00, the concentration level under the HIS condition was always the lowest, while LIS remained the highest, but no significant difference was detected.
3.3. Evaluation of Sleep Quality
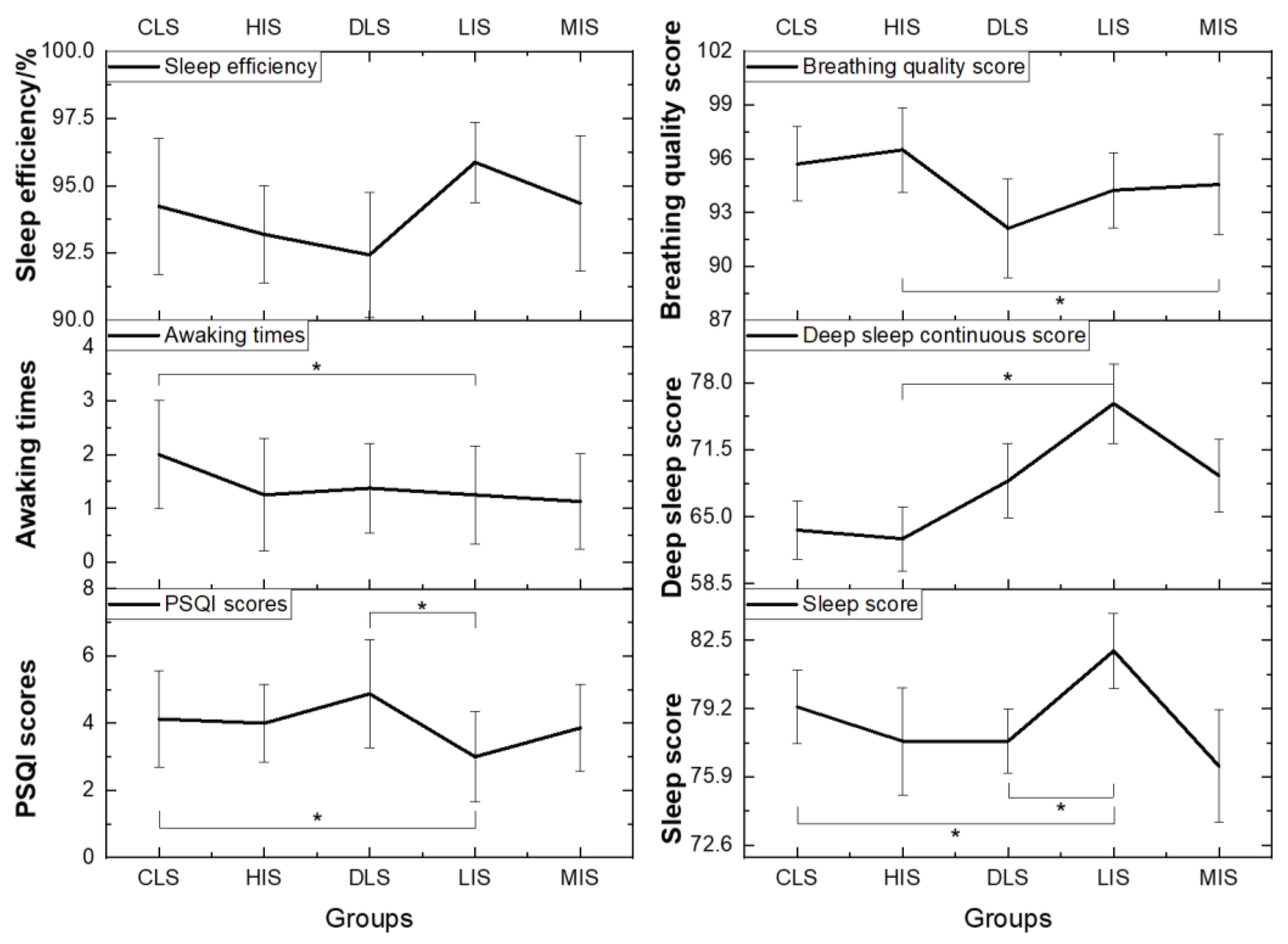
Figure 6 shows the indicators used to evaluate sleep quality: sleep efficiency, awaking times, PSQI scores, breathing quality score, deep sleep continuous score and sleep score. It can be seen that PSQI under the LIS condition was the lowest, indicating the best sleep quality, which was significantly lower than CLS (p = 0.026) and DLS (p = 0.014). The awakening times affected by CLS was the highest, while they were the lowest under HIS and LIS; the difference between CLS and LIS was significant (p = 0.020). Sleep efficiency of LIS was the highest, but there was no significant difference across the scenes. The overall score of sleep evaluation with sleep bracelet was the highest in LIS, which was significantly higher than CLS (p = 0.042) and DLS (p = 0.035), while the scores of HIS, DLS and MIS with strong light stimuli were lower and the sleep evaluation yielded the most negative results. Similarly, the continuity of deep sleep in LIS was significantly higher than HIS (p = 0.030), but the breathing quality of HIS was significantly better than MIS (p = 0.043). In general, sleep quality was the best in the LIS conditions where lighting stimulation was minimal, and gradually became worse as light stimulation increased.
Figure 7 shows that there was no significant difference detected in the time of sleep and before falling asleep, the proportion of deep sleep, light sleep and rapid eye movement (REM) (see Figure 7). LIS showed the longest sleep time and the shortest sleep latency, while DLS produced opposite results. HIS and MIS with strong light stimuli showed higher proportions of light sleep, while LIS and CLS had lower proportions of light sleep and higher proportions of deep sleep. There was little difference in the proportion of REM; both MIS and LIS were higher.
3.4. PVT Test
Based on the results of the PVT test, comparing the response time and error numbers of different scenes (Figure 8), it is found that the average response time affected by LIS was the longest, followed by CLS, and the average response time of MIS was the shortest. It indicates that cognitive performance requires appropriate illuminance, and too dark or bright light is not conducive to the cognitive response. Similarly, MIS showed the lowest error rate, significantly lower than CLS (p = 0.048). The errors under HIS and LIS increased slightly, which was more than that of MIS, indicating that too strong or dark light stimulation has the potential to increase error rates. Appropriate illuminance is thus beneficial to improve the response speed of visual operation and reduce error rates.
4. Discussion
The illuminance, spectral distribution, duration, timing, previous lighting [48,49,50], the direction of light [51,52], visual fields [53] and other factors will affect human cognitive performance [54,55], sleep rhythm [56], emotional state [48], and even social behaviour [57]. In this experiment, under the condition of a simulated night shift in a confined space, the basic lighting requirements were firstly met, after which five lighting environments with different intensities of the circadian stimuli were created with different illuminances and spectra, aiming to allow for a comprehensive comparison across the effects caused by each condition over the whole night period on sleep quality, melatonin suppression and cognitive performance.
Studies have shown that there is a positive correlation between the light dose at night and the suppression of melatonin concentration [58]. In light stimulations, high-light interventions for 0.5, 1 or 2 h have mostly been used [59,60,61]; there are a few studies on long-term continuous light intervention for more than 4 h. In this study, according to actual work requirements and shift work and rest system, different intensities of light were continuously used for stimulation during five hours of night work to explore the phased changes in melatonin concentration. The melatonin concentration of LIS was higher than other scenes, with an overall upward trend, because the light stimulation was the least. In the other scenes’ melatonin first decreased and then increased, indicating that there was a conflict between the inhibitory effects of light and the natural secretion of melatonin. The melatonin suppression can be predicted based on melanopic EDI and light exposure duration [62], and as long as the light duration is long enough, 50% melatonin suppression can be achieved under less than 10 lx melanopic EDI at night. In this study, melatonin was not measured in the dim light [63] (≤10 lx, refer to the measurement method of dim light melatonin onset (DLMO)), so the suppression rate of melatonin could not be calculated. However, since the melatonin of each scene was lower than usual at 24:00, it could be inferred that the melatonin of each scene was inhibited. The melatonin concentration of LIS was the highest due to the lowest melanopic EDI and melatonin suppression effects. After 1 h of light stimulation, the melatonin concentration of HIS was the lowest at 22:00 because of the strongest illuminance and melatonin suppression effects, followed by the MIS, because the illuminance of light in this scene was second only to HIS. The inhibitory effects of CLS and DLS were not obvious, basically consistent with the predicted circadian responses of the CS model and melanopic illuminance [64]. Subsequently, the concentrations of melatonin in HIS, MIS and DLS showed an apparent upward trend, and the fluctuation peak appeared around 21:00, while the concentration peak of CLS was delayed at 22:00. The concentrations of melatonin in the previous three scenes (HIS, MIS and DLS) were suppressed again, and MIS and DLS began to show an upward trend again after 22:00. The HIS with the strongest lighting exposure did not appear in the second round of melatonin fluctuation until about 23:00, which showed the most obvious suppression effect on melatonin and the slowest rise, and the rhythm fluctuation was significantly delayed. Maybe a longer duration is needed for further validation in the real environment, since the circadian offset under static lighting has been demonstrated in underground caves [65] or the Antarctic research stations during the polar night [66].
The changes in subjective sleepiness (KSS score) and melatonin concentration were a little different; the subjective sleepiness showed an overall increasing trend at night, but the increasing rate was different in each lighting scene. The subjective sleepiness of the darkest LIS increased rapidly from 20:00 and remained the highest all the time. However, KSS scores of HIS and MIS with strong lighting stimulation increased slowly. HIS showed the highest subjective wakefulness at 24:00, which corresponded with the lowest melatonin concentration. Intense light stimulation can improve alertness and reduce sleepiness at night, but the subjective sleepiness level of the bright light is higher in the morning of the following day, indicating that light not only affects sleepiness and circadian rhythm at night, but also has a further impact on alertness in the morning of the next day [67].
In terms of sleep quality, LIS with the least light stimulation showed the lowest PSQI, fewer awakenings, and the highest sleep evaluation score, denoting the best sleep quality. It was expected that HIS with the strongest light stimulation might seriously affect sleep quality, while results showed that the PSQI score, sleep efficiency, numbers of awakening and sleep evaluation score in the DLS reflected the poorest sleep quality. There was no significant difference in sleep time, time to fall asleep, the proportion of deep and light sleep, proportion of REM eye movement, etc. Thus, more sophisticated equipment (such as Polysomnography (PSG)) should be used to conduct experiments with a larger sample size in subsequent studies, since low proportional blue light exposure would prolong REM sleep and advance the DLMO phase while also increasing overall sleep time [68]. While lighting in the evening can suppress melatonin secretion and delay circadian phase, the patterning of light exposure across the day and evening can have moderating effects [69]. This is consistent with the field studies of Sahin [70], Taotao [26], Daniel [12], Schledermann [71] and Eowyn [72] in hospitals, offices, factories and so on, where it was found that a suitable combination of dynamic lighting parameters during the day and night can maintain the human circadian rhythm effectively and have positive non-visual effects on visual comfort, hormone secretion and sleep [73]. Therefore, not only the light dose at night but also the lighting pattern during the day need further control and research.
For cognitive tasks, MIS showed the best performance with the shortest response time and the lowest error rate, while HIS with the strongest light stimulation performed worse. DLS and CLS with weaker light stimulation also performed worse than the MIS. And LIS showed the longest average response time, but the error rate was not the highest. It indicates that visual work needs appropriate illuminance; too high or too low light stimulation is not conducive to good visual performance. Lin [74,75] also found that higher intensity blue light had a stronger alerting effect, but that the effect of intensity on alertness was not linear. In a recent field study, a small sample of subjects showed a significant relationship between subjective alertness and horizontal illuminance without the presence of any additional confounding variables [76]. In subsequent studies, more illuminance values between 300 and 3000 lx will be subdivided for more in-depth studies to determine the most appropriate threshold of illuminance.
Moreover, each lighting scene in this study was treated with light intervention for only one night at a time, and the more obvious circadian phase shift effects observed required more days of continuous light stimulation in subsequent experiments [11]. Due to individual differences in the response of light [77], future work could be improved by increasing the number of samples and carrying out strict screening of participants’ sleep types. It is necessary to consider the differences between ages and genders [78]. In addition, the amount of light exposure during the day needs to be strictly controlled to avoid any impact on sleep and cognitive status at night. Certainly, real-world occupational settings cannot be fully reproduced in the laboratory, and hence there is need for long-term interventions to simulate the effects of light in the realistic environment and post-occupancy evaluation are required as well.
5. Conclusions
In this study, five hours of continuous lighting stimulation were conducted at night to explore the effects of different lighting stimuli on sleepiness, melatonin, sleep quality and performance during night-time work in a confined space. The results showed that bright light stimulation significantly inhibited melatonin, leading to the lowest subjective sleepiness, and more sleepiness the next morning. Subjective sleepiness increased rapidly under “dark light” with the best sleep and melatonin suppression, provided that light exposure is of sufficient duration. The best visual performance occurred under moderate light conditions and the quality of sleep was relatively better. During shift work, light with low stimulations under the requirement of visual work would be preferred to reduce the impact on sleep rhythm. For difficult visual tasks, requiring higher light for visual work, moderate illuminance of light can achieve the best performance while avoiding serious disruptions to sleep. Although the subjective fatigue of high-light illuminance is low, it provides little help for improving cognitive tasks, but causes serious disturbance to circadian rhythm and sleep, which is not economical and energy saving. Therefore, the intensity of the lighting stimulus during night work should be chosen reasonably according to the type and requirements of the visual work.
Author Contributions
Conceptualization, T.W. and L.H.; methodology, T.W.; software, T.W.; validation, T.W., R.S. and L.H.; formal analysis, T.W.; investigation, R.S.; resources, R.S. and L.H.; data curation, T.W. and R.S.; writing—original draft preparation, T.W.; writing—review and editing, R.S. and L.H.; visualization, T.W.; supervision, R.S. and L.H.; project administration, L.H.; funding acquisition, L.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Scientific Research Project of Shanghai Municipal Science and Technology Commission, grant number 20dz1207200 and 22dz1202400.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
The authors would like to acknowledge Runqi Liang, Warren Julian, Zhidian Jiang, Yanfeng Huang, Yanni Wang, Juanjie Li, Shujian Dai, Li Wei and the Polar Research Institute of China for their technical and editorial assistance to this project.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Lu, Y.; Yin, P.; Wang, J.; Yang, Y.; Li, F.; Yuan, H.; Li, S.; Long, Z.; Zhou, M. Light at night and cause-specific mortality risk in Mainland China: A nationwide observational study. BMC Med. 2023, 21, 95. [Google Scholar] [CrossRef]
- Lai, K.Y.; Sarkar, C.; Ni, M.Y.; Cheung, L.W.T.; Gallacher, J.; Webster, C. Exposure to light at night (LAN) and risk of breast cancer: A systematic review and meta-analysis. Sci. Total Environ. 2021, 762, 143159. [Google Scholar] [CrossRef]
- Stevens, R.G.; Hansen, J.; Costa, G.; Haus, E.; Kauppinen, T.; Aronson, K.J.; Castaño-Vinyals, G.; Davis, S.; Frings-Dresen, M.H.; Fritschi, L. Considerations of circadian impact for defining ‘shift work’in cancer studies: IARC Working Group Report. Occup. Environ. Med. 2011, 68, 154–162. [Google Scholar] [CrossRef]
- Haus, E.L.; Smolensky, M.H. Shift work and cancer risk: Potential mechanistic roles of circadian disruption, light at night, and sleep deprivation. Sleep Med. Rev. 2013, 17, 273–284. [Google Scholar] [CrossRef]
- Sun, S.; Cao, W.; Ge, Y.; Ran, J.; Sun, F.; Zeng, Q.; Guo, M.; Huang, J.; Lee, R.S.-Y.; Tian, L. Outdoor light at night and risk of coronary heart disease among older adults: A prospective cohort study. Eur. Heart J. 2021, 42, 822–830. [Google Scholar] [CrossRef] [PubMed]
- Stefani, O.; Cajochen, C. Should we re-think regulations and standards for lighting at workplaces? A practice review on existing lighting recommendations. Front. Psychiatry 2021, 12, 652161. [Google Scholar] [CrossRef] [PubMed]
- CIE S 017/E:2020; ILV: International Lighting Vocabulary, 2nd ed. CIE Central Bureau: Vienna, Austria, 2020.
- Lowden, A.; Kecklund, G. Considerations on how to light the night-shift. Light. Res. Technol. 2021, 53, 437–452. [Google Scholar] [CrossRef]
- Hou, D.; He, S.; Dai, C.; Chen, S.; Chen, H.; Lin, Y. Lighting scheme recommendation for interior workplace to adjust the phase-advance jet lag. Build. Environ. 2021, 198, 107913. [Google Scholar] [CrossRef]
- Houser, K.; Boyce, P.; Zeitzer, J.; Herf, M. Human-centric lighting: Myth, magic or metaphor? Light. Res. Technol. 2021, 53, 97–118. [Google Scholar] [CrossRef]
- Wang, T.; Li, J.; Wang, Y.; Dai, S.; Shao, R.; Hao, L. Active interventions of dynamic lighting on human circadian rhythm and sleep quality in confined spaces. Build. Environ. 2022, 226, 109766. [Google Scholar] [CrossRef]
- Vethe, D.; Scott, J.; Engstrøm, M.; Salvesen, Ø.; Sand, T.; Olsen, A.; Morken, G.; Heglum, H.S.; Kjørstad, K.; Faaland, P.M.; et al. The evening light environment in hospitals can be designed to produce less disruptive effects on the circadian system and improve sleep. Sleep 2021, 44, 194. [Google Scholar] [CrossRef]
- Berson, D.M.; Dunn, F.A.; Takao, M. Phototransduction by retinal ganglion cells that set the circadian clock. Science 2002, 295, 1070–1073. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, M.; Din, N.S.B.M.; Tharumalay, R.D.; Che Din, N.; Ibrahim, N.; Amit, N.; Farah, N.M.; Osman, R.A.; Abdul Hamid, M.F.; Ibrahim, I.A. The effects of circadian rhythm disruption on mental health and physiological responses among shift workers and general population. Int. J. Environ. Res. Public Health 2020, 17, 7156. [Google Scholar] [CrossRef] [PubMed]
- Gou, Z.; Gou, B.; Liao, W.; Bao, Y.; Deng, Y. Integrated lighting ergonomics: A review on the association between non-visual effects of light and ergonomics in the enclosed cabins. Build. Environ. 2023, 243, 110616. [Google Scholar] [CrossRef]
- Khalsa, S.B.S.; Jewett, M.E.; Cajochen, C.; Czeisler, C.A. A phase response curve to single bright light pulses in human subjects. J. Physiol. 2003, 549, 945–952. [Google Scholar] [CrossRef] [PubMed]
- Minors, D.S.; Waterhouse, J.M.; Wirz-Justice, A. A human phase-response curve to light. Neurosci. Lett. 1991, 133, 36–40. [Google Scholar] [CrossRef]
- Gabel, V.; Maire, M.; Reichert, C.F.; Chellappa, S.L.; Schmidt, C.; Hommes, V.; Viola, A.U.; Cajochen, C. Effects of artificial dawn and morning blue light on daytime cognitive performance, well-being, cortisol and melatonin levels. Chronobiol. Int. 2013, 30, 988–997. [Google Scholar] [CrossRef]
- Souman, J.L.; Tinga, A.M.; Te Pas, S.F.; Van Ee, R.; Vlaskamp, B.N. Acute alerting effects of light: A systematic literature review. Behav. Brain Res. 2018, 337, 228–239. [Google Scholar] [CrossRef]
- Vandewalle, G.; Dijk, D.-J. Neuroimaging the Effects of Light on Non-Visual Brain Functions. 2012, pp. 171–178. Available online: https://orbi.uliege.be/bitstream/2268/149604/1/Vandewalle_Dijk_2013_book%20chapter.pdf (accessed on 7 November 2012).
- Mårtensson, B.; Pettersson, A.; Berglund, L.; Ekselius, L. Bright white light therapy in depression: A critical review of the evidence. J. Affect. Disord. 2015, 182, 1–7. [Google Scholar] [CrossRef]
- Griepentrog, J.E.; Labiner, H.E.; Gunn, S.R.; Rosengart, M.R. Bright environmental light improves the sleepiness of nightshift ICU nurses. Crit. Care 2018, 22, 295. [Google Scholar] [CrossRef]
- Figueiro, M.; Nagare, R.; Price, L. Non-visual effects of light: How to use light to promote circadian entrainment and elicit alertness. Light. Res. Technol. 2018, 50, 38–62. [Google Scholar] [CrossRef] [PubMed]
- Figueiro, M.; Steverson, B.; Heerwagen, J.; Yucel, R.; Roohan, C.; Sahin, L.; Kampschroer, K.; Rea, M. Light, entrainment and alertness: A case study in offices. Light. Res. Technol. 2020, 52, 736–750. [Google Scholar] [CrossRef]
- Stefani, O.; Freyburger, M.; Veitz, S.; Basishvili, T.; Meyer, M.; Weibel, J.; Kobayashi, K.; Shirakawa, Y.; Cajochen, C. Changing color and intensity of LED lighting across the day impacts on circadian melatonin rhythms and sleep in healthy men. J. Pineal Res. 2021, 70, e12714. [Google Scholar] [CrossRef]
- Ru, T.; Kompier, M.E.; Chen, Q.; Zhou, G.; Smolders, K.C. Temporal tuning of illuminance and spectrum: Effect of a full-day dynamic lighting pattern on well-being, performance and sleep in simulated office environment. Build. Environ. 2023, 228, 109842. [Google Scholar] [CrossRef]
- CIE S 026/E:2018; CIE System for Metrology of Optical Radiation for ipRGC-Influenced Responses to Light. CIE Central Bureau: Vienna, Austria, 2018.
- Schlangen, L.J. CIE Position Statement on Non-Visual Effects of Light: Recommending Proper Light at the Proper Time; CIE Central Bureau: Vienna, Austria, 2019. [Google Scholar]
- WELL-Building-Standard, v2 Pilot. Circadian Lighting Design. 2022. Available online: https://v2.wellcertified.com/en/wellv2/light/feature/3 (accessed on 15 June 2022).
- Brown, T.; Brainard, G.; Cajochen, C.; Czeisler, C.; Hanifin, J.; Lockley, S.; Lucas, R.; Munch, M.; O’Hagan, J.; Peirson, S. Recommendations for Healthy Daytime, Evening, and Night-Time Indoor Light Exposure. 2020. Available online: https://www.preprints.org/manuscript/202012.0037/v1 (accessed on 1 December 2020).
- GB 50034-2013; Ministry-of-Housing-and-Urban-Rural-Development, Standard for Lighting Design of Buildings. China Architecture and Building Press: Beijing, China, 2013.
- Figueiro, M. A working threshold for acute nocturnal melatonin suppression from “white” light sources used in architectural applications. J. Carcinog. Mutagen. 2013, 4, 150. [Google Scholar]
- Rea, M.S.; Figueiro, M.G.; Bierman, A.; Bullough, J.D. Circadian light. J. Circadian Rhythm. 2010, 8, 1–10. [Google Scholar] [CrossRef]
- Liu, H.; Yao, Z.; Fu, Y. Research status and development trend of bio-regenerative life support system for deep space exploration. J. Deep Space Explor. 2020, 7, 489. [Google Scholar]
- Tafforin, C. The Mars-500 crew in daily life activities: An ethological study. Acta Astronaut. 2013, 91, 69–76. [Google Scholar] [CrossRef]
- Meng, C.; Wang, W.; Hao, Z.; Liu, H. Investigation on the influence of isolated environment on human psychological and physiological health. Sci. Total Environ. 2020, 716, 136972. [Google Scholar] [CrossRef]
- Lowden, A.; Akerstedt, T. Assessment of a new dynamic light regimen in a nuclear power control room without windows on quickly rotating shiftworkers—Effects on health, wakefulness, and circadian alignment: A pilot study. Chronobiol. Int. 2012, 29, 641–649. [Google Scholar] [CrossRef]
- Nie, J.; Zhou, T.; Chen, Z.; Dang, W.; Jiao, F.; Zhan, J.; Chen, Y.; Chen, Y.; Pan, Z.; Kang, X.; et al. Investigation on entraining and enhancing human circadian rhythm in closed environments using daylight-like LED mixed lighting. Sci. Total Environ. 2020, 732, 139334. [Google Scholar] [CrossRef]
- Zhang, Z.; Henzmann, S.; Hugli, G.; Qi, M.; Chen, W.; Lu, C.; Khatami, R. Validation of wearable sleep monitoring device based on cardiopulmonary coupling and accelerometer with comparison to polysomnography in adults. In Proceedings of the 4th Congress of the European Academy of Neurology, Lisbon, Portugal, 16–19 June 2018; European Journal of Neurology: Lisbon, Portugal, 2018; p. 385. [Google Scholar]
- Carpenter, J.S.; Andrykowski, M.A. Psychometric evaluation of the Pittsburgh sleep quality index. J. Psychosom. Res. 1998, 45, 5–13. [Google Scholar] [CrossRef]
- Thomann, J.; Baumann, C.R.; Landolt, H.-P.; Werth, E. Psychomotor vigilance task demonstrates impaired vigilance in disorders with excessive daytime sleepiness. J. Clin. Sleep Med. 2014, 10, 1019–1024. [Google Scholar] [CrossRef] [PubMed]
- Basner, M.; Mollicone, D.; Dinges, D.F. Validity and sensitivity of a brief psychomotor vigilance test (PVT-B) to total and partial sleep deprivation. Acta Astronaut. 2011, 69, 949–959. [Google Scholar] [CrossRef]
- Kaida, K.; Takahashi, M.; Åkerstedt, T.; Nakata, A.; Otsuka, Y.; Haratani, T.; Fukasawa, K. Validation of the Karolinska sleepiness scale against performance and EEG variables. Clin. Neurophysiol. 2006, 117, 1574–1581. [Google Scholar] [CrossRef]
- Rajaratnam, S.M.; Middleton, B.; Stone, B.M.; Arendt, J.; Dijk, D.J. Melatonin advances the circadian timing of EEG sleep and directly facilitates sleep without altering its duration in extended sleep opportunities in humans. J. Physiol. 2004, 561, 339–351. [Google Scholar] [CrossRef] [PubMed]
- Sletten, T.L.; Magee, M.; Murray, J.M.; Gordon, C.J.; Lovato, N.; Kennaway, D.J.; Gwini, S.M.; Bartlett, D.J.; Lockley, S.W.; Lack, L.C. Efficacy of melatonin with behavioural sleep-wake scheduling for delayed sleep-wake phase disorder: A double-blind, randomised clinical trial. PLoS Med. 2018, 15, e1002587. [Google Scholar] [CrossRef]
- Falcón, J.; Torriglia, A.; Attia, D.; Viénot, F.; Gronfier, C.; Behar-Cohen, F.; Martinsons, C.; Hicks, D. Exposure to artificial light at night and the consequences for flora, fauna, and ecosystems. Front. Neurosci. 2020, 14, 1183. [Google Scholar] [CrossRef] [PubMed]
- Gooley, J.J.; Chamberlain, K.; Smith, K.A.; Khalsa, S.B.S.; Rajaratnam, S.M.; Van Reen, E.; Zeitzer, J.M.; Czeisler, C.A.; Lockley, S.W. Exposure to room light before bedtime suppresses melatonin onset and shortens melatonin duration in humans. J. Clin. Endocrinol. Metab. 2011, 96, E463–E472. [Google Scholar] [CrossRef]
- Dumont, M.; Beaulieu, C. Light exposure in the natural environment: Relevance to mood and sleep disorders. Sleep Med. 2007, 8, 557–565. [Google Scholar] [CrossRef]
- Xiao, H.; Cai, H.; Li, X. Non-visual effects of indoor light environment on humans: A review✰. Physiol. Behav. 2021, 228, 113195. [Google Scholar] [CrossRef] [PubMed]
- Khademagha, P.; Aries, M.; Rosemann, A.; Van Loenen, E. Implementing non-image-forming effects of light in the built environment: A review on what we need. Build. Environ. 2016, 108, 263–272. [Google Scholar] [CrossRef]
- Rea, M.S.; Nagare, R.; Figueiro, M.G. Relative light sensitivities of four retinal hemi-fields for suppressing the synthesis of melatonin at night. Neurobiol. Sleep Circadian Rhythm. 2021, 10, 100066. [Google Scholar] [CrossRef]
- Glickman, G.; Hanifin, J.P.; Rollag, M.D.; Wang, J.; Cooper, H.; Brainard, G.C. Inferior retinal light exposure is more effective than superior retinal exposure in suppressing melatonin in humans. J. Biol. Rhythm. 2003, 18, 71–79. [Google Scholar] [CrossRef]
- Lasko, T.A.; Kripke, D.F.; Elliot, J.A. Melatonin suppression by illumination of upper and lower visual fields. J. Biol. Rhythm. 1999, 14, 122–125. [Google Scholar] [CrossRef] [PubMed]
- Figueiro, M.; Kalsher, M.; Steverson, B.; Heerwagen, J.; Kampschroer, K.; Rea, M. Circadian-effective light and its impact on alertness in office workers. Light. Res. Technol. 2019, 51, 171–183. [Google Scholar] [CrossRef]
- Smolders, K.; De Kort, Y.; van den Berg, S.M. Daytime light exposure and feelings of vitality: Results of a field study during regular weekdays. J. Environ. Psychol. 2013, 36, 270–279. [Google Scholar] [CrossRef]
- Hubalek, S.; Brink, M.; Schierz, C. Office workers’ daily exposure to light and its influence on sleep quality and mood. Light. Res. Technol. 2010, 42, 33–50. [Google Scholar] [CrossRef]
- Hsu, Z.Y.; Moskowitz, D.; Young, S.N. The influence of light administration on interpersonal behavior and affect in people with mild to moderate seasonality. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2014, 48, 92–101. [Google Scholar] [CrossRef]
- Revell, V.L.; Skene, D.J. Light-induced melatonin suppression in humans with polychromatic and monochromatic light. Chronobiol. Int. 2007, 24, 1125–1137. [Google Scholar] [CrossRef]
- Chellappa, S.L.; Steiner, R.; Blattner, P.; Oelhafen, P.; Götz, T.; Cajochen, C. Non-visual effects of light on melatonin, alertness and cognitive performance: Can blue-enriched light keep us alert? PLoS ONE 2011, 6, e16429. [Google Scholar] [CrossRef] [PubMed]
- Chellappa, S.L.; Viola, A.U.; Schmidt, C.; Bachmann, V.; Gabel, V.; Maire, M.; Reichert, C.F.; Valomon, A.; Landolt, H.-P.; Cajochen, C. Light modulation of human sleep depends on a polymorphism in the clock gene Period3. Behav. Brain Res. 2014, 271, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Knaier, R.; Schäfer, J.; Rossmeissl, A.; Klenk, C.; Hanssen, H.; Höchsmann, C.; Cajochen, C.; Schmidt-Trucksäss, A. Prime time light exposures do not seem to improve maximal physical performance in male elite athletes, but enhance end-spurt performance. Front. Physiol. 2017, 8, 264. [Google Scholar] [CrossRef] [PubMed]
- Giménez, M.C.; Stefani, O.; Cajochen, C.; Lang, D.; Deuring, G.; Schlangen, L.J. Predicting melatonin suppression by light in humans: Unifying photoreceptor-based equivalent daylight illuminances, spectral composition, timing and duration of light exposure. J. Pineal Res. 2022, 72, e12786. [Google Scholar] [CrossRef]
- Pandi-Perumal, S.R.; Smits, M.; Spence, W.; Srinivasan, V.; Cardinali, D.P.; Lowe, A.D.; Kayumov, L. Dim light melatonin onset (DLMO): A tool for the analysis of circadian phase in human sleep and chronobiological disorders. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2007, 31, 1–11. [Google Scholar] [CrossRef]
- Brown, T.M. Melanopic illuminance defines the magnitude of human circadian light responses under a wide range of conditions. J. Pineal Res. 2020, 69, e12655. [Google Scholar] [CrossRef]
- Mills, J. Circadian rhythms during and after three months in solitude underground. J. Physiol. 1964, 174, 217–231. [Google Scholar] [CrossRef]
- Broadway, J.; Arendt, J.; Folkard, S. Bright light phase shifts the human melatonin rhythm during the Antarctic winter. Neurosci. Lett. 1987, 79, 185–189. [Google Scholar] [CrossRef]
- Höhn, C.; Schmid, S.R.; Plamberger, C.P.; Bothe, K.; Angerer, M.; Gruber, G.; Pletzer, B.; Hoedlmoser, K. Preliminary results: The impact of smartphone use and short-wavelength light during the evening on circadian rhythm, sleep and alertness. Clocks Sleep 2021, 3, 66–86. [Google Scholar] [CrossRef]
- Vethe, D.; Drews, H.J.; Scott, J.; Engstrøm, M.; Heglum, H.S.A.; Grønli, J.; Wisor, J.; Sand, T.; Lydersen, S.; Kjørstad, K. Evening light environments can be designed to consolidate and increase the duration of REM-sleep. Sci. Rep. 2022, 12, 8719. [Google Scholar] [CrossRef]
- Ricketts, E.J.; Joyce, D.S.; Rissman, A.J.; Burgess, H.J.; Colwell, C.S.; Lack, L.C.; Gradisar, M. Electric lighting, adolescent sleep and circadian outcomes, and recommendations for improving light health. Sleep Med. Rev. 2022, 64, 101667. [Google Scholar] [CrossRef]
- Sahin, L.; Figueiro, M. A 24-h lighting scheme to promote alertness and circadian entrainment in railroad dispatchers on rotating shifts: A field study. Light. Res. Technol. 2022, 54, 441–457. [Google Scholar] [CrossRef]
- Schledermann, K.; Bjørner, T.; West, A.; Hansen, T. Evaluation of staff’s perception of a circadian lighting system implemented in a hospital. Build. Environ. 2023, 242, 110488. [Google Scholar] [CrossRef]
- Van de Putte, E.; Kindt, S.; Bracke, P.; Stevens, M.; Vansteenkiste, M.; Vandevivere, L.; Ryckaert, W.R. The influence of integrative lighting on sleep and cognitive functioning of shift workers during the morning shift in an assembly plant. Appl. Ergon. 2022, 99, 103618. [Google Scholar] [CrossRef]
- Schlangen, L.J.; Price, L.L. The lighting environment, its metrology, and non-visual responses. Front. Neurol. 2021, 12, 624861. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Westland, S. Effect of long-wavelength light on electroencephalogram and subjective alertness. Light. Res. Technol. 2020, 52, 763–774. [Google Scholar] [CrossRef]
- Lin, J.; Westland, S.; Cheung, V. Effect of intensity of short-wavelength light on electroencephalogram and subjective alertness. Light. Res. Technol. 2020, 52, 413–422. [Google Scholar] [CrossRef]
- van Duijnhoven, J.; Aarts, M.; Rosemann, A.; Kort, H. Ambiguities regarding the relationship between office lighting and subjective alertness: An exploratory field study in a Dutch office landscape. Build. Environ. 2018, 142, 130–138. [Google Scholar] [CrossRef]
- Phillips, A.J.; Vidafar, P.; Burns, A.C.; McGlashan, E.M.; Anderson, C.; Rajaratnam, S.M.; Lockley, S.W.; Cain, S.W. High sensitivity and interindividual variability in the response of the human circadian system to evening light. Proc. Natl. Acad. Sci. USA 2019, 116, 12019–12024. [Google Scholar] [CrossRef]
- Daneault, V.; Dumont, M.; Massé, É.; Vandewalle, G.; Carrier, J. Light-sensitive brain pathways and aging. J. Physiol. Anthropol. 2016, 35, 9. [Google Scholar] [CrossRef]
Figure 1.
The layout of the experimental rooms and relative SPD of different lighting scenes. (a) Each room can accommodate four people in two bunk beds. The room height is 2.45 metres. (b) Relative spectral power distribution (SPD) of different lighting scenes (6000 K and 2700 K CCT) was measured by the illuminance spectrophotometer in the middle of the table facing up towards the light sources.
Figure 1.
The layout of the experimental rooms and relative SPD of different lighting scenes. (a) Each room can accommodate four people in two bunk beds. The room height is 2.45 metres. (b) Relative spectral power distribution (SPD) of different lighting scenes (6000 K and 2700 K CCT) was measured by the illuminance spectrophotometer in the middle of the table facing up towards the light sources.

Figure 2.
Experimental protocol and data collection schedule.

Figure 3.
Variation trend in KSS scores with time in different lighting scenes hourly (* represents p < 0.05).
Figure 3.
Variation trend in KSS scores with time in different lighting scenes hourly (* represents p < 0.05).

Figure 4.
Comparison of melatonin AUC (area under the curve 5 h prior to bedtime) during the treatment nights.
Figure 4.
Comparison of melatonin AUC (area under the curve 5 h prior to bedtime) during the treatment nights.

Figure 5.
Changes in melatonin concentration with time in different lighting scenes (* represents p < 0.05, ** represents p < 0.01).
Figure 5.
Changes in melatonin concentration with time in different lighting scenes (* represents p < 0.05, ** represents p < 0.01).

Figure 6.
Comparison of PSQI scores and sleep quality indexes in different lighting scenes (* represents p < 0.05).
Figure 6.
Comparison of PSQI scores and sleep quality indexes in different lighting scenes (* represents p < 0.05).

Figure 7.
Comparison of sleep bracelet data in different lighting scenes.

Figure 8.
Comparison of PVT results in different lighting scenes (* represents p < 0.05).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Lighting parameters of different intervention scenes.
| Light Scenes | CCT/K | Illuminance of Working Plane/lx | Vertical Illuminance at the Eyes/lx | Melanopic EDI/lx | Circadian Stimulus, CS |
|---|---|---|---|---|---|
| current lighting scene (CLS) | 6000 | 151.53 | 63.31 | 56.50 | 0.10 |
| high intervention scene (HIS) | 6000 | 3415.96 | 1255.80 | 1171.25 | 0.60 |
| design lighting scene (DLS) | 6000 | 333.34 | 129.85 | 124.10 | 0.20 |
| low intervention scene (LIS) | 2700 | 103.97 | 43.68 | 19.65 | 0.05 |
| medium intervention scene (MIS) | 6000 | 531.77 | 215.25 | 202.28 | 0.30 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Wang, T.; Shao, R.; Hao, L. Effects of Different Nocturnal Lighting Stimuli on Melatonin, Sleep and Cognitive Performance of Workers in Confined Spaces. Buildings 2023, 13, 2112. https://0-doi-org.brum.beds.ac.uk/10.3390/buildings13082112
AMA Style
Wang T, Shao R, Hao L. Effects of Different Nocturnal Lighting Stimuli on Melatonin, Sleep and Cognitive Performance of Workers in Confined Spaces. Buildings. 2023; 13(8):2112. https://0-doi-org.brum.beds.ac.uk/10.3390/buildings13082112
Chicago/Turabian StyleWang, Tongyue, Rongdi Shao, and Luoxi Hao. 2023. "Effects of Different Nocturnal Lighting Stimuli on Melatonin, Sleep and Cognitive Performance of Workers in Confined Spaces" Buildings 13, no. 8: 2112. https://0-doi-org.brum.beds.ac.uk/10.3390/buildings13082112
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.