

The Impact of the COVID-19 Pandemic on Mental Health and Substance Use among People with and without HIV


Abstract
:1. Introduction
2. Materials and Method
2.1. Study Design and Participants
2.2. Ethics Approval
2.3. Statistical Analysis
3. Results
3.1. Cohort Characteristics
3.2. Depressive and Anxiety Symptoms
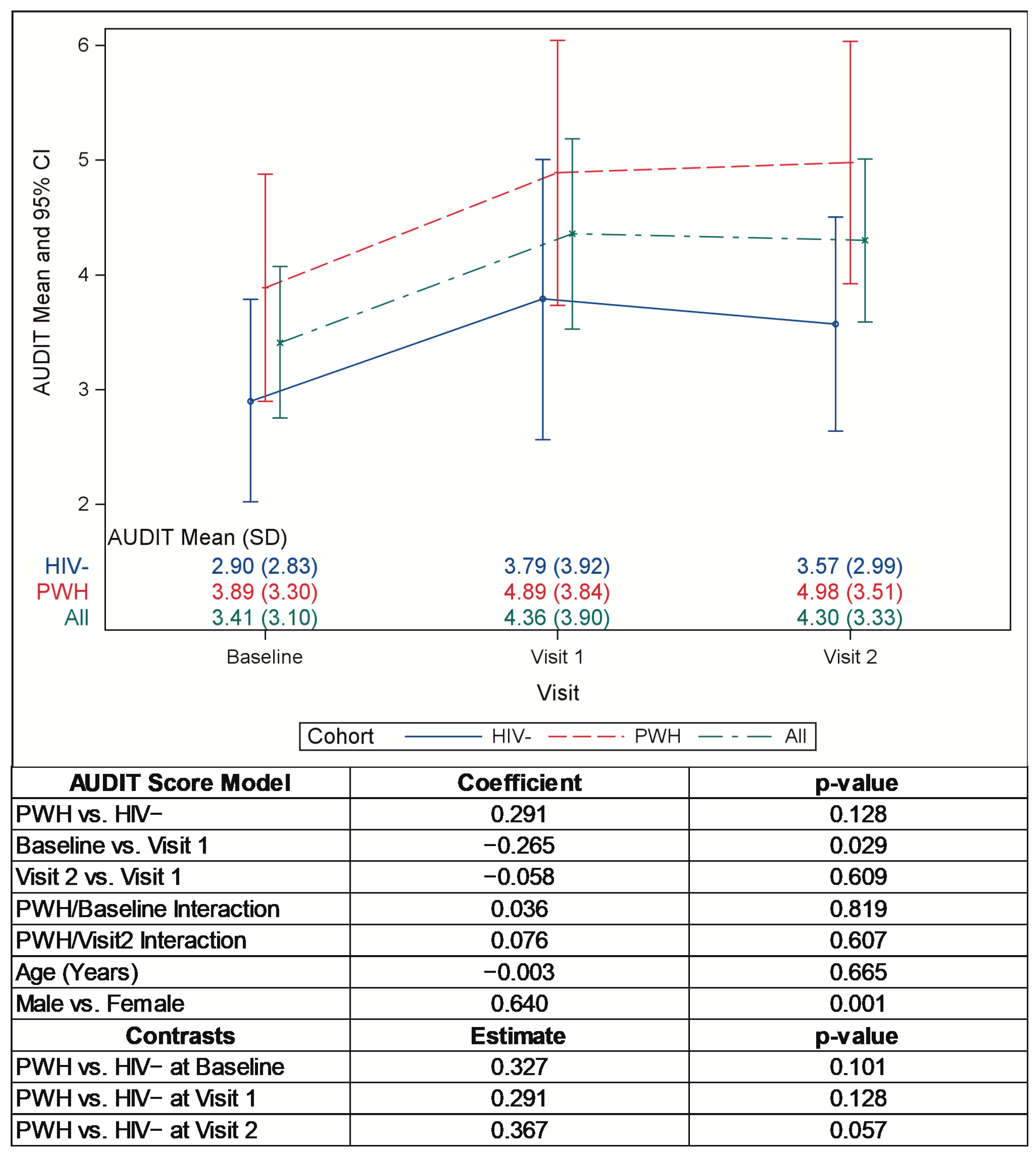
3.3. Alcohol Use
3.4. Other Substance Use
3.5. Sleep
3.6. Indirect Impacts of COVID-19 Questionnaire
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Czeisler, M.E.; Lane, R.I.; Petrosky, E.; Wiley, J.F.; Christensen, A.; Njai, R.; Weaver, W.D.; Robbins, R.; Facer-Childs, E.R.; Barger, L.K.; et al. Mental Health, Substance Use, and Suicidal Ideation During the COVID-19 Pandemic-United States, June 24-30, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1049–1057. [Google Scholar] [CrossRef]
- Nachega, J.B.; Morroni, C.; Zuniga, J.M.; Sherer, R.; Beyrer, C.; Solomon, S.; Schechter, M.; Rockstroh, J. HIV-related stigma, isolation, discrimination, and serostatus disclosure: A global survey of 2035 HIV-infected adults. J. Int. Assoc. Physicians AIDS Care 2012, 11, 172–178. [Google Scholar] [CrossRef] [Green Version]
- Gallant, J.; Hsue, P.Y.; Shreay, S.; Meyer, N. Comorbidities Among US Patients with Prevalent HIV Infection—A Trend Analysis. J. Infect. Dis. 2017, 216, 1525–1533. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.-Y.; Beymer, M.R.; Suen, S.-C. Chronic Disease Onset Among People Living with HIV and AIDS in a Large Private Insurance Claims Dataset. Sci. Rep. 2019, 9, 18514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amin, P.; Douaihy, A. Substance Use Disorders in People Living with Human Immunodeficiency Virus/AIDS. Nurs. Clin. North Am. 2018, 53, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Duko, B.; Ayalew, M.; Ayano, G. The prevalence of alcohol use disorders among people living with HIV/AIDS: A systematic review and meta-analysis. Subst. Abus. Treat. Prev. Policy 2019, 14, 52. [Google Scholar] [CrossRef] [Green Version]
- De Santis, J.P.; Florom-Smith, A.; Vermeesch, A.; Barroso, S.; DeLeon, D.A. Motivation, management, and mastery: A theory of resilience in the context of HIV infection. J. Am. Psychiatr. Nurses Assoc. 2013, 19, 36–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diehl, M.; Hay, E.L.; Chui, H. Chapter 13 Personal Risk and Resilience Factors in the Context of Daily Stress. Annu. Rev. Gerontol. Geriatr. 2012, 32, 251–274. [Google Scholar] [CrossRef] [Green Version]
- Baum, M.K.; Tamargo, J.A.; Diaz-Martinez, J.; Delgado-Enciso, I.; Meade, C.S.; Kirk, G.D.; Mehta, S.H.; Moore, R.; Kipke, M.D.; Shoptaw, S.J.; et al. HIV, psychological resilience, and substance misuse during the COVID-19 pandemic: A multi-cohort study. Drug Alcohol Depend. 2022, 231, 109230. [Google Scholar] [CrossRef]
- Parisi, C.E.; Varma, D.S.; Wang, Y.; Vaddiparti, K.; Ibañez, G.E.; Cruz, L.; Cook, R.L. Changes in Mental Health Among People with HIV During the COVID-19 Pandemic: Qualitative and Quantitative Perspectives. AIDS Behav. 2022, 26, 1980–1991. [Google Scholar] [CrossRef]
- Ballivian, J.; Alcaide, M.L.; Cecchini, D.; Jones, D.L.; Abbamonte, J.M.; Cassetti, I. Impact of COVID–19-Related Stress and Lockdown on Mental Health Among People Living with HIV in Argentina. Am. J. Ther. 2020, 85, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Sun, S.; Hou, J.; Chen, Y.; Lu, Y.; Brown, L.; Operario, D. Challenges to HIV Care and Psychological Health During the COVID-19 Pandemic Among People Living with HIV in China. AIDS Behav. 2020, 24, 2764–2765. [Google Scholar] [CrossRef] [PubMed]
- Kuman, T.O.; Pullukcu, H.; Erdem, H.A.; Kurtaran, B.; Tasbakan, S.E.; Tasbakan, M. COVID-19-related anxiety in people living with HIV: An online cross-sectional study. Turk. J. Med. Sci. 2020, 50, 1792–1800. [Google Scholar] [CrossRef] [PubMed]
- Marbaniang, I.; Sangle, S.; Nimkar, S.; Zarekar, K.; Salvi, S.; Chavan, A.; Gupta, A.; Suryavanshi, N.; Mave, V. The burden of anxiety among people living with HIV during the COVID-19 pandemic in Pune, India. BMC Public Health 2020, 20, 1598. [Google Scholar] [CrossRef]
- Landis, D.; Courtney, W.; Dieringer, C.; Kelly, R.; King, M.; Miller, B.; Wang, R.; Wood, D.; Turner, J.A.; Calhoun, V.D. COINS Data Exchange: An open platform for compiling, curating, and disseminating neuroimaging data. Neuroimage 2016, 124, 1084–1088. [Google Scholar] [CrossRef] [Green Version]
- Scott, A.; Courtney, W.; Wood, D.; de la Garza, R.; Lane, S.; King, M.; Wang, R.; Roberts, J.; Turner, J.A.; Calhoun, V.D. COINS: An Innovative Informatics and Neuroimaging Tool Suite Built for Large Heterogeneous Datasets. Front. Neuroinform. 2011, 5, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Manual for the Beck Depression Inventory-II.; Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Beck, A.T.; Steer, R.A. Beck Anxiety Inventory Manual; Psychological Corporation: San Antonio, TX, USA, 1993. [Google Scholar]
- Babor, T.F.; Higgins-Biddle, J.C.; Saunders, J.B.; Monteiro, M.G. The Alcohol Use Disorder Identification Test: Guidelines for Use in Primary Care, 2nd ed.; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- NIDA. Resource Guide: Screening for Drug Use in General Medical Settings. Available online: https://archives.drugabuse.gov/publications/resource-guide-screening-drug-use-in-general-medical-settings (accessed on 10 February 2022).
- Buysse, D.J.; Reynolds, C.F., 3rd; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Diaz-Martinez, J.; Tamargo, J.A.; Delgado-Enciso, I.; Liu, Q.; Acuña, L.; Laverde, E.; Barbieri, M.A.; Trepka, M.J.; Campa, A.; Siminski, S.; et al. Resilience, Anxiety, Stress, and Substance Use Patterns During COVID-19 Pandemic in the Miami Adult Studies on HIV (MASH) Cohort. AIDS Behav. 2021, 25, 3658–3668. [Google Scholar] [CrossRef]
- Roberts, A.; Rogers, J.; Mason, R.; Siriwardena, A.N.; Hogue, T.; Whitley, G.A.; Law, G.R. Alcohol and other substance use during the COVID-19 pandemic: A systematic review. Drug Alcohol Depend. 2021, 229, 109150. [Google Scholar] [CrossRef]
- Pellowski, J.A.; Kalichman, S.C.; Matthews, K.A.; Adler, N. A pandemic of the poor: Social disadvantage and the U.S. HIV epidemic. Am. Psychol. 2013, 68, 197–209. [Google Scholar] [CrossRef] [Green Version]
- Okonkwo, N.E.; Aguwa, U.T.; Jang, M.; Barré, I.A.; Page, K.R.; Sullivan, P.S.; Beyrer, C.; Baral, S. COVID-19 and the US response: Accelerating health inequities. BMJ Evidence-Based Med. 2020, 26, 176–179. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| HIV− (N = 42) | PWH (N = 45) | p-Value | |
|---|---|---|---|
| Age at Baseline (years), mean (sd) | 47.1 (13.4) | 45.2 (13.0) | 0.492 |
| Age at Baseline, n (%) | 0.584 | ||
| 21–30 | 6 (14) | 10 (22) | |
| 31–40 | 8 (19) | 5 (11) | |
| 41–50 | 8 (19) | 11 (24) | |
| 51–68 | 20 (48) | 19 (42) | |
| Sex, n (%) | 0.82 | ||
| Male | 27 (64) | 31 (69) | |
| Female | 15 (36) | 14 (31) | |
| Race and Ethnicity, n (%) | 0.689 | ||
| Non-Hispanic White | 33 (79) | 32 (71) | |
| Non-Hispanic Black | 4 (10) | 8 (18) | |
| Hispanic | 1 (2) | 2 (4) | |
| Other | 4 (10) | 3 (7) | |
| Highest Level of Education, n (%) | 0.001 | ||
| Some grade/high school | 0 (0) | 5 (11) | |
| High school graduate | 0 (0) | 7 (16) | |
| Some college | 7 (17) | 16 (36) | |
| Associate degree | 5 (12) | 4 (9) | |
| Bachelor’s degree or greater | 30 (71) | 13 (29) | |
| Income, n (%) | 0.251 | ||
| Less than $25,000 | 4 (10) | 11 (25) | |
| $25,000–50,000 | 7 (17) | 6 (14) | |
| Over $50,000, under $100,000 | 8 (19) | 7 (16) | |
| $100,000 plus | 14 (33) | 8 (18) | |
| Prefer not to answer | 9 (21) | 12 (27) | |
| Federal Poverty Level 2019, mean (sd) | 470 (314) | 344 (266) | 0.086 |
| Federal Poverty Level 2021, mean (sd) | 494 (334) | 319 (226) | 0.008 |
| Essential Worker, n (%) | 0.286 | ||
| Yes | 19 (45) | 26 (58) | |
| No | 23 (55) | 19 (42) | |
| Number residing in house, n (%) | 0.319 | ||
| 1 | 11 (26) | 15 (33) | |
| 2 | 15 (36) | 21 (47) | |
| 3 | 9 (21) | 5 (11) | |
| ≥4 | 7 (17) | 4 (9) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zabel, M.; Wilson, T.W.; Sayles, H.; May, P.E.; Furl, R.; Bares, S.H. The Impact of the COVID-19 Pandemic on Mental Health and Substance Use among People with and without HIV. Pathogens 2023, 12, 461. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens12030461
Zabel M, Wilson TW, Sayles H, May PE, Furl R, Bares SH. The Impact of the COVID-19 Pandemic on Mental Health and Substance Use among People with and without HIV. Pathogens. 2023; 12(3):461. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens12030461
Chicago/Turabian StyleZabel, Morgan, Tony W. Wilson, Harlan Sayles, Pamela E. May, Renae Furl, and Sara H. Bares. 2023. "The Impact of the COVID-19 Pandemic on Mental Health and Substance Use among People with and without HIV" Pathogens 12, no. 3: 461. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens12030461