Asymptomatic Strongyloidiasis among Latin American Migrants in Spain: A Community-Based Approach

 , , , , , , , , ,
, , , , , , , , ,  and
and
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Population
2.2. Questionnaires
2.3. Procedure: Serological Methods
2.4. Follow-Up of Participants with Positive Serology
2.5. Statistical Analysis
2.6. Ethical Considerations
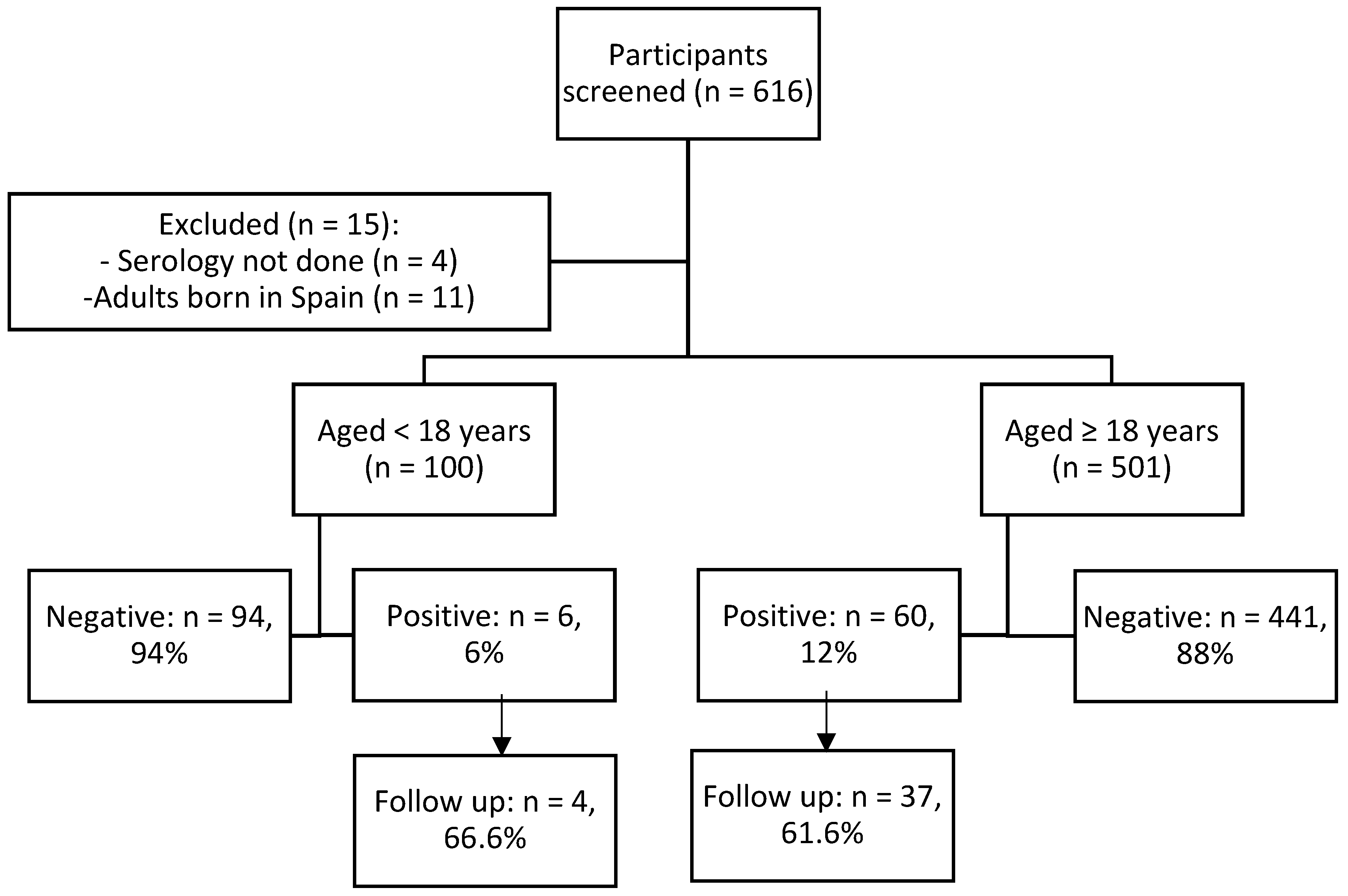
3. Results
3.1. S. stercoralis Infection in Children and Adolescents
3.2. S. stercoralis Infection in Adult Participants
3.3. Follow-Up of Participants with S. stercoralis Positive Serology
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Krolewiecki, A.; Nutman, T.B. Strongyloidiasis: A Neglected Tropical Disease. Infect. Dis. Clin. N. Am. 2019, 33, 135–151. [Google Scholar] [CrossRef] [PubMed]
- Schär, F.; Trostdorf, U.; Giardina, F.; Khieu, V.; Muth, S.; Marti, H.; Vounatsou, O.; Odermatt, P. Strongyloides stercoralis: Global Distribution and Risk Factors. PLoS Negl. Trop. Dis. 2013, 7, e2288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Requena-Méndez, A.; Salas-Coronas, J.; Salvador, F.; Gomez-Junyent, J.; Villar-Garcia, J.; Santin, M.; Muñoz, C.; González-Cordón, A.; Cabézas-Fernández, M.T.; Sulleiro, E.; et al. High Prevalence of Strongyloidiasis in Spain: A Hospital-Based Study. Pathogens 2020, 9, 107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keiser, P.B.; Nutman, T.B. Strongyloides stercoralis in the Immunocompromised Population. Clin. Microbiol. Rev. 2004, 17, 208–217. [Google Scholar] [CrossRef] [Green Version]
- Stewart, D.M.; Ramanathan, R.; Mahanty, S.; Fedorko, D.P.; Janik, J.E.; Morris, J.C. Disseminated Strongyloides stercoralis infection in HTLV-1-associated adult T-cell leukemia/lymphoma. Acta Haematol. 2011, 126, 63–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buonfrate, D.; Formenti, F.; Perandin, F.; Bisoffi, Z. Novel approaches to the diagnosis of Strongyloides stercoralis infection. Clin. Microbiol. Infect. 2015, 21, 543–552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belhassen-García, M.; Alonso-Sardón, M.; Martinez-Perez, A.; Soler, C.; Carranza-Rodriguez, C.; Pérez-Arellano, J.L.; Soil-Trasmitted Helminths Study group of the SEMTSI. Surveillance of strongyloidiasis in Spanish inpatients (1998–2014). PLoS ONE 2017, e0189449. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Perez, A.; Roure Díez, S.; Belhassen-Garcia, M.; Torrús-Tendero, D.; Perez-Arellano, J.L.; Cabezas, T.; Soler, C.; Díaz-Menéndez, M.; Navarro, M.; Trebiño, B.; et al. Management of severe strongyloidiasis attended at reference centers in Spain. PLoS Negl. Trop. Dis. 2018, 12. [Google Scholar] [CrossRef] [Green Version]
- Guevara, A.G.; Anselmi, M.; Bisoffi, Z.; Prandi, R.; Márquez, M.; Silva, R.; Vicuña, Y.; Calvaopiña, M.; Cevallos, W.; Pérez, J.; et al. Mapping the Prevalence of Strongyloides stercoralis Infection in Ecuador: A Serosurvey. Am. J. Trop. Med. Hyg. 2019. [Google Scholar] [CrossRef]
- Indice Nacional de Estadistica. España en cifras [Internet]. INE, Ed.; 2018. Available online: http://www.ine.es/prodyser/espa_cifras (accessed on 2 November 2019).
- Buonfrate, D.; Mena, M.A.; Angheben, A.; Requena-Mendez, A.; Munõz, J.; Gobbi, F.; Albonico, M.; Gotuzzo, E.; Bisoffi, Z.; COHEMI Project Study Group. Prevalence of strongyloidiasis in Latin America: A systematic review of the literature. Epidemiol. Infect. 2015, 143, 452–460. [Google Scholar] [CrossRef] [Green Version]
- Morales, M.L.; Lopez, M.; Ly, P.; Anjum, S.; Fernandez-Baca, M.V.; Valdivia-Rodriguez, A.M.; Mamani-Licona, F.M.; Baca-Turpo, B.B.; Farfan-Gonzáles, N.; Chaman-Illanes, Y.; et al. Strongyloides stercoralis Infection at Different Altitudes of the Cusco Region in Peru. Am. J. Trop. Med. Hyg. 2019, 101, 422–427. [Google Scholar] [CrossRef] [PubMed]
- Ramos, J.M.; Leon, R.; Andreu, M.; de las Parras, E.R.; Rodriguez-Diaz, J.C.; Esteban, A.; Esteban, A.; Saugar, J.M.; Torrús, D. Serological study of Trypanosoma cruzi, Strongyloides stercoralis, HIV, human T cell lymphotropic virus (HTLV) and syphilis infections in asymptomatic Latin-American immigrants in Spain. Trans. R. Soc. Trop. Med. Hyg. 2015, 109, 447–453. [Google Scholar] [CrossRef] [PubMed]
- Asundi, A.; Beliavsky, A.; Liu, X.J.; Akaberi, A.; Schwarzer, G.; Bisoffi, Z.; Requena-Méndez, A.; Shrier, I.; Greenaway, C. Prevalence of strongyloidiasis and schistosomiasis among migrants: A systematic review and meta-analysis. Lancent Glob Health 2019, 7, e236–e248. [Google Scholar] [CrossRef] [Green Version]
- Navarro, M.; Berens-Riha, N.; Hohnerlein, S.; Seiringer, P.; Von Saldern, C.; Garcia, S.; Blasco-Hernández, T.; Navaza, B.; Shock, J.; Bretzel, G.; et al. Cross-sectional, descriptive study of Chagas disease among citizens of Bolivian origin living in Munich, Germany. BMJ Open 2017, 7, e013960. [Google Scholar] [CrossRef] [Green Version]
- Romay-Barja, M.; Boquete, T.; Martinez, O.; González, M.; Álvarez-Del Arco, D.; Benito, A.; Blasco-Hernández, T. Chagas screening and treatment among Bolivians living in Madrid, Spain: The need for an official protocol. PLoS ONE 2019, 14, e0213577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gómez I Prat, J.; Peremiquel-Trillas, P.; Claveria Guiu, I.; Choque, E.; Oliveira Souto, I.; Serre Delcor, N.; Blasco-Hernández, T. A Community-Based Intervention for the Detection of Chagas Disease in Barcelona, Spain. J. Community Health 2019, 44, 704–711. [Google Scholar] [CrossRef]
- Meymandi, S.K.; Hernandez, S.; Forsyth, C.J. A Community-Based Screening Program for Chagas Disease in the USA. Trends Parasitol. 2017, 33, 828–831. [Google Scholar] [CrossRef]
- Monge-Maillo, B.; Navarro, M.; Rodríguez, E.; Ramos Rincón, J.M.; Chamorro Tojeiro, S.; Jiménez Sánchez, S.; Casas del Corral, M.J.; López-Vélez, R. Community screening campaign for Strongyloides stercoralis among Latin American immigrants in Spain. Clin. Microbiol. Infect. 2018, 24, 1220–1221. [Google Scholar] [CrossRef] [Green Version]
- Instituto Nacional de Estadística de España. Población extranjera por Nacionalidad, provincias, Sexo y Año. 2019. Available online: https://www.ine.es/jaxi/Datos.htm?path=/t20/e245/p08/&file=03005.px#!tabs-tabla (accessed on 6 May 2020).
- Buonfrate, D.; Perandin, F.; Formenti, F.; Bisoffi, Z. A retrospective study comparing agar plate culture, indirect immunofluorescence and real-time PCR for the diagnosis of Strongyloides stercoralis infection. Parasitology 2017, 144, 812–816. [Google Scholar] [CrossRef]
- Requena-Méndez, A.; Chiodini, P.; Bisoffi, Z.; Buonfrate, D.; Gotuzzo, E.; Muñoz, J. The laboratory diagnosis and follow up of strongyloidiasis: A systematic review. PLoS Negl. Trop. Dis. 2013, 7, e2002. [Google Scholar] [CrossRef]
- Saugar, J.M.; Merino, F.J.; Martín-Rabadán, P.; Fernández-Soto, P.; Ortega, S.; Gárate, T.; Rodrígez, E. Application of real-time PCR for the detection of Strongyloides spp. in clinical samples in a reference center in Spain. Acta Trop. 2015, 142, 20–25. [Google Scholar] [CrossRef]
- Buonfrate, D.; Salas-Coronas, J.; Muñoz, J.; Maruri, B.T.; Rodari, P.; Castelli, F.; Zammarchi, L.; Bianchi, L.; Gobbi, F.; Cabezas-Fernández, T.; et al. Multiple-dose versus single-dose ivermectin for Strongyloides stercoralis infection (Strong Treat 1 to 4): A multicentre, open-label, phase 3, randomised controlled superiority trial. Lancet Infect. Dis. 2019, 19, 1181–1190. [Google Scholar] [CrossRef]
- Buonfrate, D.; Sequi, M.; Mejia, R.; Cimino, R.O.; Krolewiecki, A.J.; Albonico, M.; Degani, M.; Tais, S.; Angheben, A.; Requena-Mendez, A.; et al. Accuracy of Five Serologic Tests for the Follow up of Strongyloides stercoralis Infection. PLoS Negl. Trop. Dis. 2015, 9. [Google Scholar] [CrossRef] [Green Version]
- Salvador, F.; Treviño, B.; Chamorro-Tojeiro, S.; Sánchez-Montalvá, A.; Herrero-Martínez, J.M.; Rodríguez-Guardado, A.; Serre-Delcor, N.; Torrús, D.; Goikoetxea, J.; Zubero, Z.; et al. Imported strongyloidiasis: Data from 1245 cases registered in the +REDIVI Spanish collaborative network (2009-2017). PLoS Negl. Trop. Dis. 2019, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navarro, M.; Monge-Maíllo, B.; Flores-Chavez, M.D.; López-Vélez, R. Hunting hidden parasites: Trypanosoma cruzi. Lancet 2017, 390, 724–726. [Google Scholar] [CrossRef]
- Abanyie, F.A.; Valice, E.; Delli Carpini, K.W.; Gray, E.B.; McAuliffe, I.; Chin-Hong, P.V.; Handali, S.; Montgomery, S.P.; Huprikar, S. Organ donor screening practices for Strongyloides stercoralis infection among US organ procurement organizations. Transpl. Infect. Dis. 2018, 20. [Google Scholar] [CrossRef] [PubMed]
- Casado, L.; Rodriguez-Guardado, A.; Boga, J.A.; Fernández-Suarez, J.; Martínez-Camblor, P.; Rodríguez-Perez, M.; García-Pérez, A.; Vazquez, F.; Gascon, J. Use of serology in a systematic screening programme for strongyloidiasis in an immigrant population. Int. J. Infect. Dis. 2019, 88, 60–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salvador, F.; Treviño, B.; Bosch-Nicolau, P.; Serre-Delcor, N.; Sánchez-Montalvá, A.; Oliveira, I.; Sulleiro, E.; Aznar, M.L.; Pou, D.; Sao-Avilés, A.; et al. Strongyloidiasis screening in migrants living in Spain: Systematic review and meta-analysis. Trop. Med. Int. Health 2020, 25, 281–290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van De, N.; Minh, P.N.; Van Duyet, L.; Mas-Coma, S. Strongyloidiasis in northern Vietnam: Epidemiology, clinical characteristics and molecular diagnosis of the causal agent. Parasit. Vectors 2019, 12, 515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dopico, E.; Rando-Matos, Y.; Solsona, L.; Almeda, J.; Santos, F.L.N.; Vinuesa, T. Infection by Strongyloides stercoralis in immigrants with Chagas disease: Evaluation of eosinophilia as screening method in primary care. Trop. Med. Int. Health 2019. [Google Scholar] [CrossRef] [PubMed]
- Salvador, F.; Sulleiro, E.; Piron, M.; Sánchez-Montalvá, A.; Sauleda, S.; Molina-Morant, D.; Mourez, Z.; Molina, I. Strongyloides stercoralis infection increases the likelihood to detect Trypanosoma cruzi DNA in peripheral blood in Chagas disease patients. Trop. Med. Int. Health 2017, 22, 1436–1441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salvador, F.; Sulleiro, E.; Sánchez-Montalvá, A.; Martínez-Gallo, M.; Carrillo, E.; Molina, I. Impact of Helminth Infection on the Clinical and Microbiological Presentation of Chagas Diseases in Chronically Infected Patients. PLoS Negl. Trop. Dis. 2016, 10. [Google Scholar] [CrossRef] [PubMed]
- Echazú, A.; Juarez, M.; Vargas, P.A.; Cajal, S.P.; Cimino, R.O.; Heredia, V.; Caropresi, S.; Paredes, G.; Arias, L.M.; Abril, M.; et al. Albendazole and ivermectin for the control of soil-transmitted helminths in an area with high prevalence of Strongyloides stercoralis and hookworm in northwestern Argentina: A community-based pragmatic study. PLoS Negl. Trop. Dis. 2017, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bisoffi, Z.; Buonfrate, D.; Sequi, M.; Mejia, R.; Cimino, R.O.; Krolewiecki, A.J.; Albonico, M.; Gobbo, M.; Bonafini, S.; Angheben, A.; et al. Diagnostic Accuracy of Five Serologic Tests for Strongyloides stercoralis Infection. PLoS Negl. Trop. Dis. 2014, 8, 38. [Google Scholar] [CrossRef] [Green Version]
- Navarro, M.; Navaza, B.; Guionnet, A.; López-Vélez, R. A multidisciplinary approach to engage VFR migrants in Madrid, Spain. Travel. Med. Infect. Dis. 2012, 10, 152–156. [Google Scholar] [CrossRef]
- Roger, D.; González-Escalada, A.; Navarro, M. Evaluación del conocimiento sobre Enfermedades Tropicales Desatendidas en estudiantes de sexto curso del grado en Medicina de la Comunidad Autónoma de Madrid; IV Congreso de Estudiantes de Medicina de la Universidad Rey Juan Carlos: Alcorcón, Madrid, Spain, 2017. Available online: https://eciencia.urjc.es/bitstream/handle/10115/13140/ISSN-2444-5479%28IV%29.pdf?sequence=16&isAllowed=y (accessed on 14 June 2020).
- Salvador, F.; Sulleiro, E.; Sánchez-Montalvá, A.; Saugar, J.M.; Rodríguez, E.; Pahissa, A.; Molina, I. Usefulness of Strongyloides stercoralis serology in the management of patients with eosinophilia. Am. J. Trop. Med. Hyg. 2014, 90, 830–834. [Google Scholar] [CrossRef]
- Buonfrate, D.; Requena-Mendez, A.; Angheben, A.; Cinquini, M.; Cruciani, M.; Fittipaldo, A.; Giorli, G.; Gobbi, F.; Piubelli, C.; Bisoffi, Z. Accuracy of molecular biology techniques for the diagnosis of Strongyloides stercoralis infection—A systematic review and meta-analysis. PLoS Negl. Trop. Dis. 2018, 12. [Google Scholar] [CrossRef] [Green Version]
- Repetto, E.C.; Zachariah, R.; Kumar, A.; Angheben, A.; Gobbi, F.; Anselmi, M.; Al Rousan, A.; Torrico, C.; Ruiz, R.; Ledezma, G.; et al. Neglect of a Neglected Disease in Italy: The Challenge of Access-to-Care for Chagas Disease in Bergamo Area. PLoS Negl. Trop. Dis. 2015, 9. [Google Scholar] [CrossRef]
- Fundación, M.S.; Madrid, S.; Salud, E.C. Evaluación de la Eficiencia de las Campañas de Cribado Comunitario de la Enfermedad de Chagas en Madrid; Informe de Evaluación de las Campañas 2014–2017: Madrid, España, 2018; Available online: https://www.saludentreculturas.es/wp-content/uploads/2019/05/Cascada-diagnostico-a-tratamiento-EChagas-Final.pdf (accessed on 14 June 2020).
- Wikman-Jorgensen, P.; Llenas-García, J.; Shedrawy, J.; Gascon, J.; Muñoz, J.; Bisoffi, Z.R.-M.A. Cost-effectiveness of different strategies for Strongyloides stercoralis screening and treatment among migrants from endemic countries to the European Union. BMJ Glob. Health 2020, 5, e002321. [Google Scholar] [CrossRef]
- Forsyth, C.; Meymandi, S.; Moss, I.; Cone, J.; Cohen, R.; Batista, C. Proposed multidimensional framework for understanding Chagas disease healthcare barriers in the United States. PLoS Negl. Trop. Dis. 2019. [Google Scholar] [CrossRef] [Green Version]
- Navarro, M.; Navaza, B.; Guionnet, A.; López-Vélez, R. Chagas Disease in Spain: Need for Further Public Health Measures. PLoS Negl. Trop. Dis. 2012, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agbata, E.N.; Morton, R.L.; Bisoffi, Z.; Bottieau, E.; Greenaway, C.; Biggs, B.A.; Montero, N.; Tran, A.; Rowutham, N.; Arévalo-Rodríguez, I.; et al. Effectiveness of screening and treatment approaches for schistosomiasis and strongyloidiasis in newly-arrived migrants from endemic countries in the EU/EEA: A systematic review. Int. J. Environ. Res. Public Health 2019, 16, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Der Werf, J.; Derrough, T.; Duffell, E.; Pharris, A.; Suk, J.; De, H.; Mardh, O.; Velasco Muñoz, C.; Causevic, S.; Thoft Nielsen, R.; et al. Public Health Guidance on Screening and Vaccination for Infectious Diseases in Newly Arrived Migrants within the EU/EEA, 1st ed.; European Centre for Disease Prevention and Control: Stockholm, Sweden, 2018; pp. 1–77. [Google Scholar] [CrossRef]
- Clemente, W.T.; Pierrotti, L.C.; Abdala, E.; Morris, M.I.; Azevedo, L.S.; López-Vélez, R.; Cuenc-Estrella, M.; Torre-Cisneros, j.; Petersen, E.; A Camargo, L.F.; et al. Recommendations for Management of Endemic Diseases and Travel Medicine in Solid-Organ Transplant Recipients and Donors: Latin America. Transplantation 2018, 102, 193–208. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total (n = 100) | S. stercoralis Infection (n = 6) | No Infection (n = 94) | OR (95% CI) | p Value | |
|---|---|---|---|---|---|
| Demographics | |||||
| Boys, n (%) | 43 (43) | 4 (66.7) | 2 (2.1) | 2.82 (0.49–16.17) | 0.23 |
| Median age, years (IQR) (n = 69) | 11 (9–14) | 5 (4–6) | 12 (10–14) | 0.58 (0.39–0.85) | 0.001 |
| Country of birth, n (%) | |||||
| Spain * | 74 (74) | 6 (100) | 68 (72.3) | NA | 0.13 |
| Bolivia | 13 (13) | 0 | 13 (13.8) | NA | 0.99 |
| Ecuador | 9 (9) | 0 | 9 (9.6) | NA | 0.99 |
| Argentina | 2 (0) | 0 | 2 (0.1) | NA | 0.99 |
| Uruguay | 2 (2) | 0 (0.0) | 2 (0.1) | NA | 0.99 |
| Total (n = 501) | S. stercoralis Infection (n = 60) | No Infection (n = 441) | OR (95% CI) | p Value | ORa (95% CI) | p Value | |
|---|---|---|---|---|---|---|---|
| Demographics | |||||||
| Men, n (%) | 198 (39.5) | 34 (56.7) | 164 (37.2) | 2.20 (1.28–3.81) | 0.004 | 2.28 (1.29–4.03) | 0.004 |
| Median age, years (IQR) (n = 493) | 41 (34–49) | 44 (37–51) | 41 (34–49) | 1.02 (1.00–1.04) | 0.046 | 1.02 (0.99–1.05) | 0.064 |
| Education, n (%) (n = 478) | |||||||
| Primary school | 128 (26.9) | 21 (35.6) | 107 (25.5) | 1.61 (0.90–2.86) | 0.10 | - | |
| Secondary school | 226 (55.6) | 34 (57.6) | 232 (55.4) | 1.09 (0.63–1.90) | 0.71 | - | |
| University studies | 84 (17.6) | 4 (6.8) | 80 (19.1) | 0.30 (0.10–0.87) | 0.02 | 0.29 (0.31–0.88) | 0.029 |
| Country of birth, n (%) | |||||||
| Bolivia | 202 (40.3) | 33 (55) | 169 (38.3) | 1.96 (1.14–3.38) | 0.013 | 2.03 (1.15–3.59) | 0.014 |
| Ecuador | 188 (37.5) | 19 (31.7) | 169 (38.3) | 0.74 (0.41–1.32) | 0.32 | - | |
| Colombia | 65 (13.0) | 6 (10.0) | 59 (13.4) | 0.71 (0.29–1.74) | 0.46 | - | |
| Argentina | 13 (2.6) | 1 (1.7) | 12 (2.7) | 0.60 (0.07–4.75) | 0.63 | - | |
| Brazil | 7 (1.4) | 0 (0.0) | 7 (1.6) | NA | 0.99 | - | |
| Paraguay | 6 (1.2) | 0 (0.0) | 6 (1.4) | NA | 0.99 | - | |
| Dominican Republic | 4 (0.8) | 0 (0.0) | 4 (0.9) | NA | 0.99 | - | |
| Peru | 4 (0.8) | 0 (0.0) | 4 (0.9) | NA | 0.99 | - | |
| Venezuela | 4 (0.8) | 0 (0.0) | 4 (0.9) | NA | 0.99 | - | |
| Other * | 8 (1.6) | 1 (1.7) | 7 (1.6) | 1.01 (0.12–8.69) | 0.99 | - | |
| Knowledge about disease, n affirmative response (%) | |||||||
| Have you ever heard of Strongyloides parasite or strongyloidiasis? | 39 (7.9) | 1 (1.7) | 38 (8.7) | 0.18 (0.02–1.35) | 0.07 | - | |
| Variable | Total n/N (%) | Children n/N (%) | Adults n/N (%) |
|---|---|---|---|
| S. stercoralis infection | 66/601 (11) | 6/100 (6) | 60/501 (11) |
| Follow-up of patients | |||
| Available | 41/66 (62.1) | 4/6 (66.6) | 37/60 (61.6) |
| Unavailable | 25/66 (37.9) | 2/6 (33.3) | 23/60 (38.3) |
| Reason for not following up | |||
| No phone contact | 17/25 (68) | 1/2 (50) | 16/23 (69.5) |
| Current phone not available | 7/25 (28) | 1/2 (50) | 6/23 (26.1) |
| Picked up the phone, but did not go to the appointment | 1/25 (4) | 0 | 1/23 (4.3) |
| Follow-up for confirmation | |||
| Stool examination | |||
| Negative | 27/41(65.9) | 2/4 (50) | 23/37 (62.2) |
| Positive * | 8/41 (19.5) | 0 | 8/37 (21.6) |
| Not recovered | 6/41 (14.6) | ||
| Eosinophilia (>5% leukocyte or >500 eosinophils) | 16/27 (59.2) | 1/1 (100) | 15/26 (57.7) |
| IgE > 100 | 9/10 (90) | 1/1 (100) | 8/9 (88.8) |
| Outcome | |||
| Treatment | 28/41 (68.3) | 2/4 (50) | 26/37 (70.2) |
| Results of treatment † | |||
| Cure | 12/28 (42.9) | 0 | 12/26 (46.2) |
| Ongoing | 12/28 (42.9) | 0 | 10/26 (38.4) |
| Lost to follow-up after treatment | 4/28 (14.2) | 2/4 (50) | 4/26 (15.4) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramos-Sesma, V.; Navarro, M.; Llenas-García, J.; Gil-Anguita, C.; Torrús-Tendero, D.; Wikman-Jorgensen, P.; Amador-Prous, C.; Ventero-Martín, M.-P.; Garijo-Sainz, A.-M.; García-López, M.; et al. Asymptomatic Strongyloidiasis among Latin American Migrants in Spain: A Community-Based Approach. Pathogens 2020, 9, 511. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens9060511
Ramos-Sesma V, Navarro M, Llenas-García J, Gil-Anguita C, Torrús-Tendero D, Wikman-Jorgensen P, Amador-Prous C, Ventero-Martín M-P, Garijo-Sainz A-M, García-López M, et al. Asymptomatic Strongyloidiasis among Latin American Migrants in Spain: A Community-Based Approach. Pathogens. 2020; 9(6):511. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens9060511
Chicago/Turabian StyleRamos-Sesma, Violeta, Miriam Navarro, Jara Llenas-García, Concepción Gil-Anguita, Diego Torrús-Tendero, Philip Wikman-Jorgensen, Concepción Amador-Prous, María-Paz Ventero-Martín, Ana-María Garijo-Sainz, María García-López, and et al. 2020. "Asymptomatic Strongyloidiasis among Latin American Migrants in Spain: A Community-Based Approach" Pathogens 9, no. 6: 511. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens9060511