
Characterization of IgG Antibody Response against SARS-CoV-2 (COVID-19) in the Cypriot Population

 , , and
, , and
Abstract
:1. Introduction
2. Methodology
2.1. Ethical Approval and Subject Recruitment
2.2. Study Population and Sample Collection
2.3. Sample Processing and Analysis
2.4. Statistical Analysis
3. Results
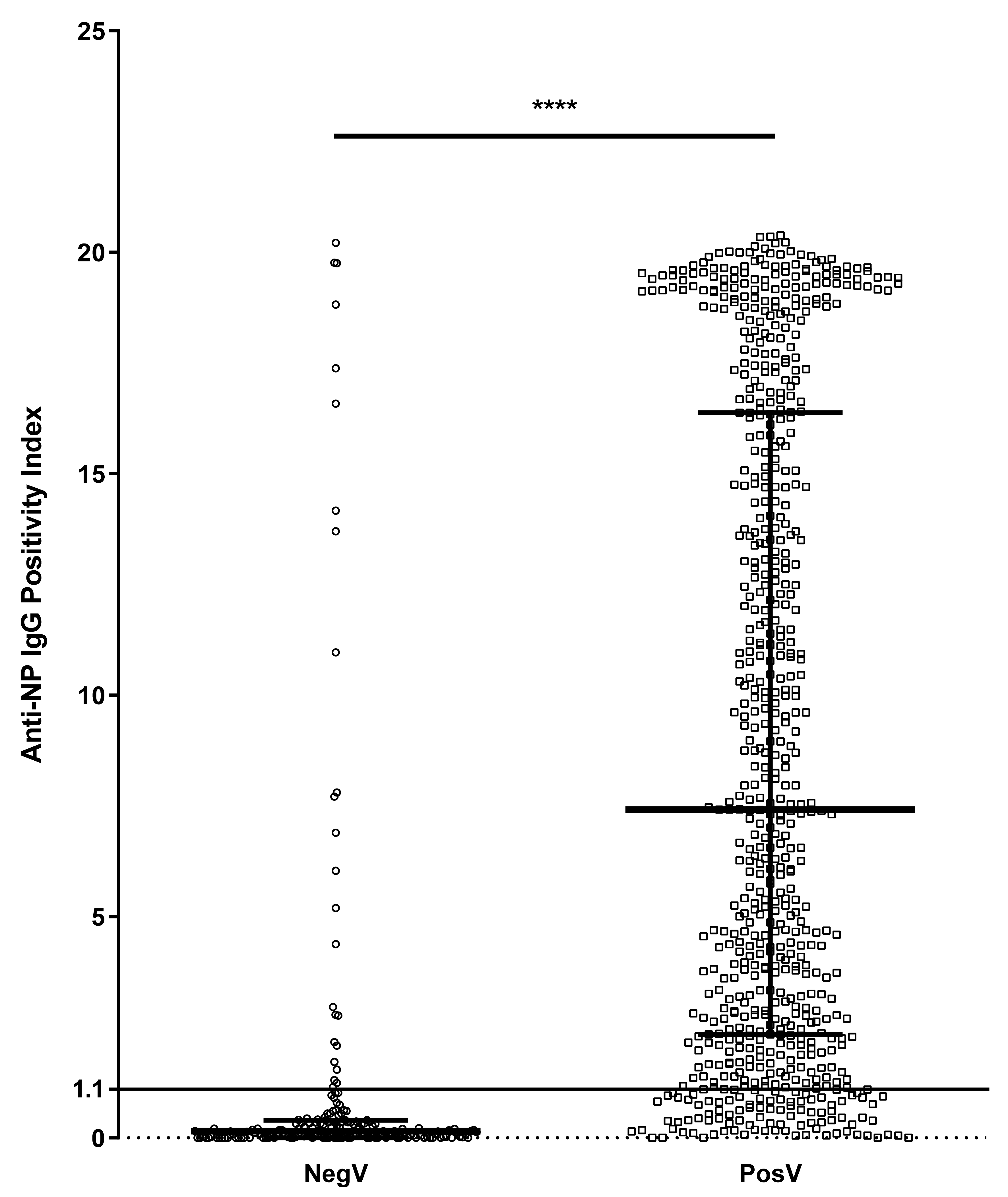
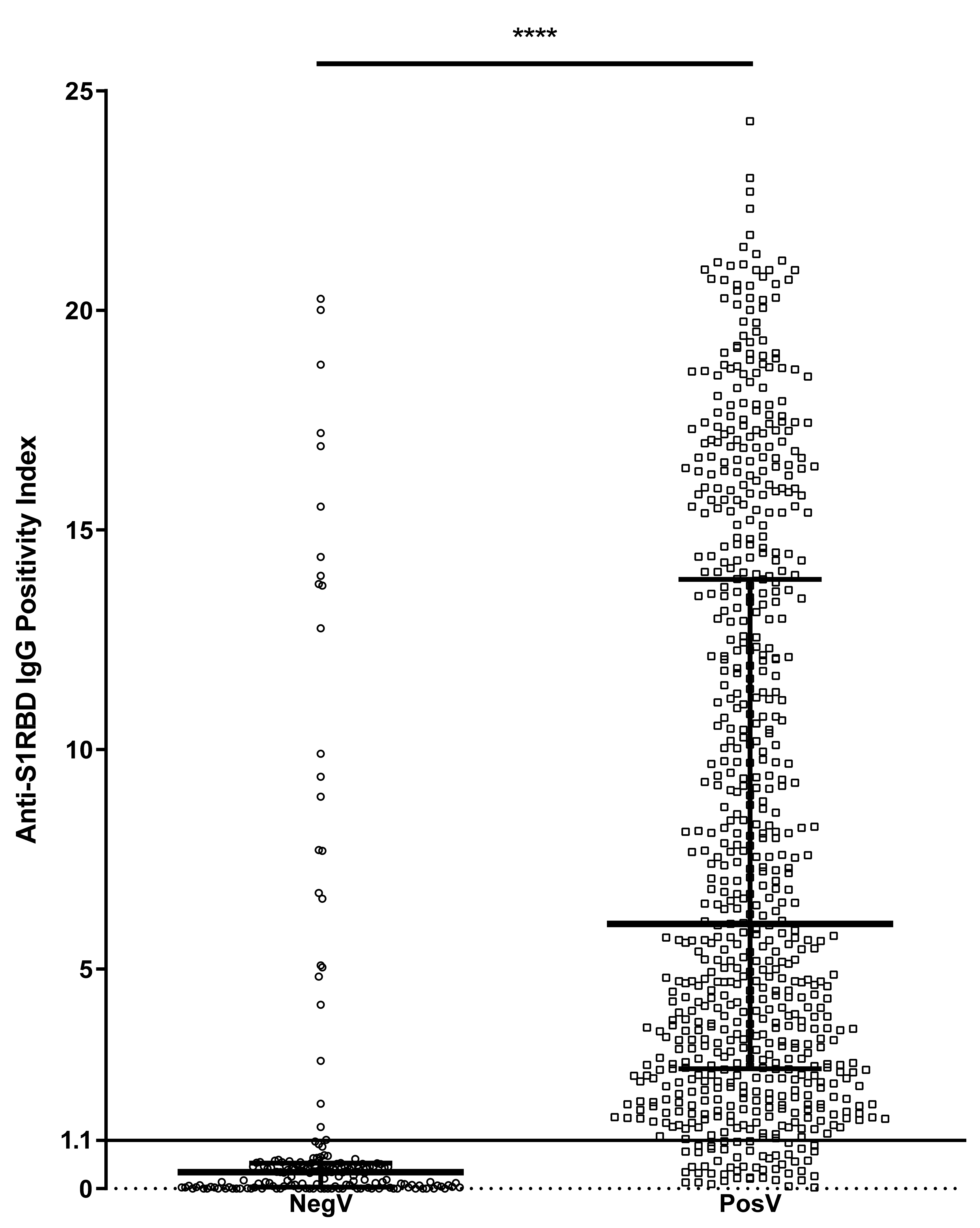
3.1. Seroprevalence of SARS-CoV-2 IgG in Previously Infected and Negative/Unknown Volunteers
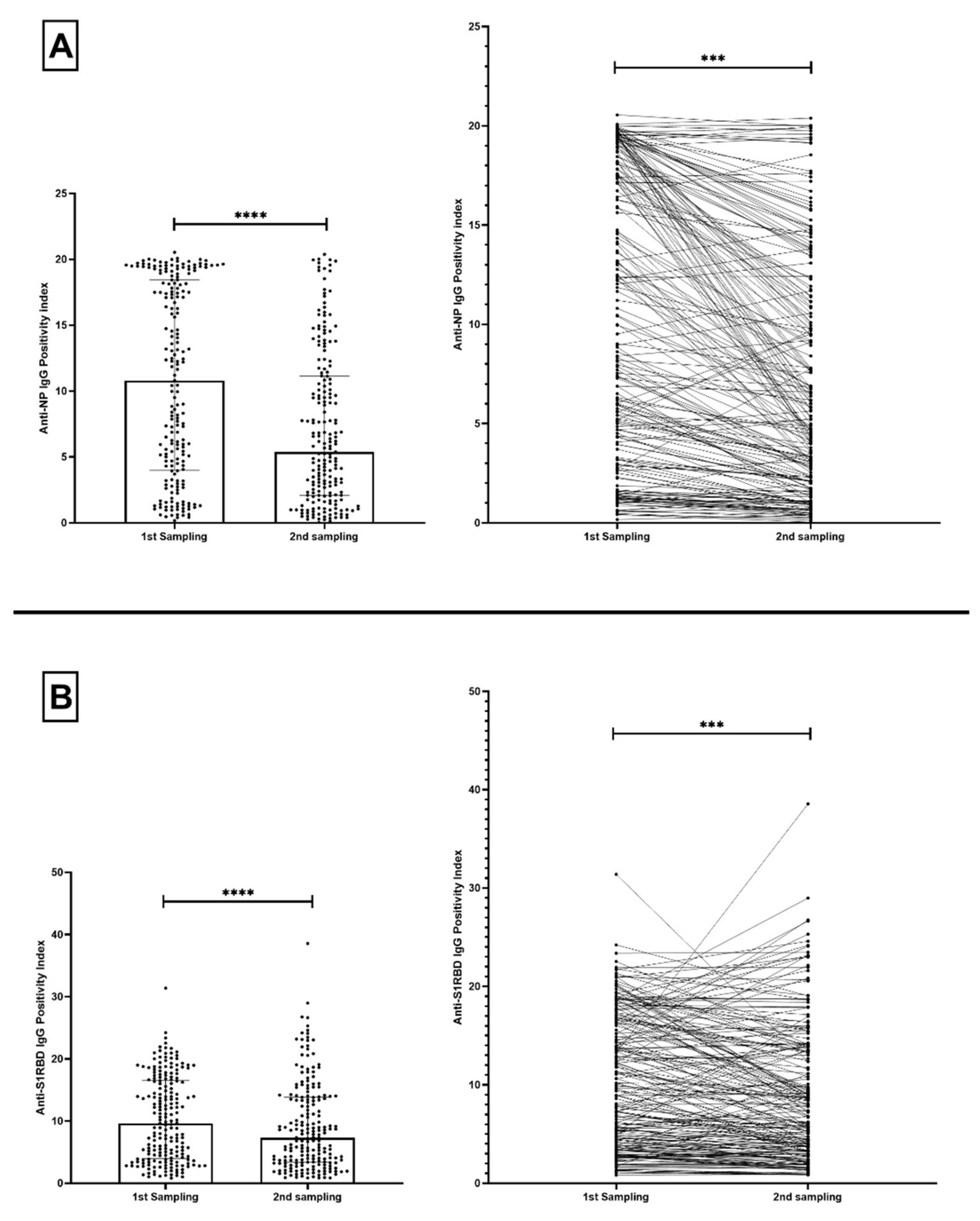
3.2. Change in SARS-CoV-2 IgG Levels of Previously Infected Volunteers across Time
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Coronavirus (COVID-19) Dashboard|WHO Coronavirus (COVID-19) Dashboard with Vaccination Data. Available online: https://covid19.who.int/ (accessed on 14 September 2021).
- Richter, J.; Fanis, P.; Tryfonos, C.; Koptides, D.; Krashias, G.; Bashiardes, S.; Hadjisavvas, A.; Loizidou, M.; Oulas, A.; Alexandrou, D.; et al. Molecular epidemiology of SARS-CoV-2 in Cyprus. PLoS ONE 2021, 16, e0248792. [Google Scholar] [CrossRef]
- Quattrocchi, A.; Mamais, I.; Tsioutis, C.; Christaki, E.; Constantinou, C.; Koliou, M.; Pana, Z.-D.; Silvestros, V.; Theophanous, F.; Haralambous, C.; et al. Extensive Testing and Public Health Interventions for the Control of COVID-19 in the Republic of Cyprus between March and May 2020. J. Clin. Med. 2020, 9, 3598. [Google Scholar] [CrossRef]
- Hasell, J.; Mathieu, E.; Beltekian, D.; Macdonald, B.; Giattino, C.; Ortiz-Ospina, E.; Roser, M.; Ritchie, H. A cross-country database of COVID-19 testing. Sci. Data 2020, 7, 1–7. [Google Scholar] [CrossRef]
- Li, R.; Pei, S.; Chen, B.; Song, Y.; Zhang, T.; Yang, W.; Shaman, J. Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-CoV-2). Science 2020, 368, 489–493. [Google Scholar] [CrossRef] [Green Version]
- Cumulative Confirmed COVID-19 Cases. Available online: https://ourworldindata.org/grapher/cumulative-covid-cases-region?tab=table (accessed on 13 September 2021).
- Bogogiannidou, Z.; Vontas, A.; Dadouli, K.; Kyritsi, M.A.; Soteriades, S.; Nikoulis, D.J.; Mouchtouri, V.; Koureas, M.; Kazakos, E.I.; Spanos, E.G.; et al. Repeated leftover serosurvey of SARS-CoV-2 IgG antibodies, Greece, March and April 2020. Eurosurveillance 2020, 25, 1–6. [Google Scholar] [CrossRef]
- Goldblatt, D.; Johnson, M.; Falup-Pecurariu, O.; Ivaskeviciene, I.; Spoulou, V.; Tamm, E.; Wagner, M.; Zar, H.J.; Bleotu, L.; Ivaskevicius, R.; et al. Cross-sectional prevalence of SARS-CoV-2 antibodies in healthcare workers in paediatric facilities in eight countries. J. Hosp. Infect. 2021, 110, 60–66. [Google Scholar] [CrossRef]
- Psichogiou, M.; Karabinis, A.; Pavlopoulou, I.D.; Basoulis, D.; Petsios, K.; Roussos, S.; Pratikaki, M.; Jahaj, E.; Protopapas, K.; Leontis, K.; et al. Antibodies against SARS-CoV-2 among health care workers in a country with low burden of COVID-19. PLoS ONE 2020, 15, e0243025. [Google Scholar] [CrossRef]
- Vlachoyiannopoulos, P.; Alexopoulos, H.; Apostolidi, I.; Bitzogli, K.; Barba, C.; Athanasopoulou, E.; Dalakas, M.; Tzioufas, A. Anti-SARS-CoV-2 antibody detection in healthcare workers of two tertiary hospitals in Athens, Greece. Clin. Immunol. 2020, 221, 108619. [Google Scholar] [CrossRef]
- Arora, R.K.; Joseph, A.; Van Wyk, J.; Rocco, S.; Atmaja, A.; May, E.; Yan, T.; Bobrovitz, N.; Chevrier, J.; Cheng, M.P.; et al. SeroTracker: A global SARS-CoV-2 seroprevalence dashboard. Lancet Infect. Dis. 2021, 21, e75–e76. [Google Scholar] [CrossRef]
- Aziz, N.A.; Corman, V.M.; Echterhoff, A.K.C.; Müller, M.A.; Richter, A.; Schmandke, A.; Schmidt, M.L.; Schmidt, T.H.; de Vries, F.M.; Drosten, C.; et al. Seroprevalence and correlates of SARS-CoV-2 neutralizing antibodies from a population-based study in Bonn, Germany. Nat. Commun. 2021, 12, 1–10. [Google Scholar] [CrossRef]
- Demographic Statistics 2019; Ministry of Finance, Republic of Cyprus: Nicosia, Cyprus, 2019; pp. 1–12.
- Sempos, C.T.; Tian, L. Adjusting Coronavirus Prevalence Estimates for Laboratory Test Kit Error. Am. J. Epidemiol. 2021, 190, 109–115. [Google Scholar] [CrossRef]
- Radulescu, A.; Istrate, A.; Flonta, M.; Lupse, M. Antibody and viral RNA kinetics in SARS-CoV2 infected patients admitted in a Romanian University Hospital of Infectious Diseases. Int. J. Infect. Dis. 2021, 107, 205–211. [Google Scholar] [CrossRef] [PubMed]
- González, F.; Zepeda, O.; Toval-Ruiz, C.; Matute, A.; Vanegas, H.; Munguia, N.; Centeno, E.; Reyes, Y.; Svensson, L.; Nordgren, J.; et al. Antibody response to SARS-CoV-2 infection over six months among Nicaraguan outpatients. medRxiv 2021. [Google Scholar] [CrossRef]
- Vusirikala, A.; Whitaker, H.; Jones, S.; Tessier, E.; Borrow, R.; Linley, E.; Hoschler, K.; Baawuah, F.; Ahmad, S.; Andrews, N.; et al. Seroprevalence of SARS-CoV-2 Antibodies in University Students: Cross-sectional study, December 2020, England. J. Infect. 2021. [Google Scholar] [CrossRef]
- Napolitano, F.; Di Giuseppe, G.; Montemurro, M.V.; Molinari, A.M.; Donnarumma, G.; Arnese, A.; Pavia, M.; Angelillo, I.F. Seroprevalence of SARS-CoV-2 Antibodies in Adults and Healthcare Workers in Southern Italy. Int. J. Environ. Res. Public Health 2021, 18, 4761. [Google Scholar] [CrossRef]
- Stefanelli, P.; Bella, A.; Fedele, G.; Pancheri, S.; Leone, P.; Vacca, P.; Neri, A.; Carannante, A.; Fazio, C.; Benedetti, E.; et al. Prevalence of SARS-CoV-2 IgG antibodies in an area of northeastern Italy with a high incidence of COVID-19 cases: A population-based study. Clin. Microbiol. Infect. 2021, 27, 633.e1–633.e7. [Google Scholar] [CrossRef]
- Havers, F.P.; Reed, C.; Lim, T.; Montgomery, J.M.; Klena, J.D.; Hall, A.J.; Fry, A.M.; Cannon, D.L.; Chiang, C.F.; Gibbons, A.; et al. Seroprevalence of Antibodies to SARS-CoV-2 in 10 Sites in the United States, 23 March–12 May 2020. JAMA Intern. Med. 2020, 180, 1776–1786. [Google Scholar] [CrossRef]
- Gudbjartsson, D.F.; Norddahl, G.L.; Melsted, P.; Gunnarsdottir, K.; Holm, H.; Eythorsson, E.; Arnthorsson, A.O.; Helgason, D.; Bjarnadottir, K.; Ingvarsson, R.F.; et al. Humoral Immune Response to SARS-CoV-2 in Iceland. N. Engl. J. Med. 2020, 383, 1724–1734. [Google Scholar] [CrossRef]
- Wajnberg, A.; Amanat, F.; Firpo, A.; Altman, D.R.; Bailey, M.J.; Mansour, M.; McMahon, M.; Meade, P.; Mendu, D.R.; Muellers, K.; et al. Robust neutralizing antibodies to SARS-CoV-2 infection persist for months. Science 2020, 370, 1227–1230. [Google Scholar] [CrossRef]
- Wu, S.L.; Mertens, A.N.; Crider, Y.S.; Nguyen, A.; Pokpongkiat, N.N.; Djajadi, S.; Seth, A.; Hsiang, M.S.; Colford, J.M.; Reingold, A.; et al. Substantial underestimation of SARS-CoV-2 infection in the United States. Nat. Commun. 2020, 11, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Bobrovitz, N.; Arora, R.K.; Cao, C.; Boucher, E.; Liu, M.; Donnici, C.; Yanes-Lane, M.; Whelan, M.; Perlman-Arrow, S.; Chen, J.; et al. Global seroprevalence of SARS-CoV-2 antibodies: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0252617. [Google Scholar] [CrossRef]
- Siggins, M.K.; Thwaites, R.S.; Openshaw, P.J.M. Durability of Immunity to SARS-CoV-2 and Other Respiratory Viruses. Trends Microbiol. 2021, 29, 648. [Google Scholar] [CrossRef] [PubMed]
- Levi, R.; Ubaldi, L.; Pozzi, C.; Angelotti, G.; Sandri, M.T.; Azzolini, E.; Salvatici, M.; Savevski, V.; Mantovani, A.; Rescigno, M. The antibody response to SARS-CoV-2 infection persists over at least 8 months in symptomatic patients. Commun. Med. 2021, 1, 1–9. [Google Scholar] [CrossRef]
- Gaebler, C.; Wang, Z.; Lorenzi, J.C.C.; Muecksch, F.; Finkin, S.; Tokuyama, M.; Cho, A.; Jankovic, M.; Schaefer-Babajew, D.; Oliveira, T.Y.; et al. Evolution of antibody immunity to SARS-CoV-2. Nature 2021, 591, 639–644. [Google Scholar] [CrossRef] [PubMed]
- Steenhuis, M.; Mierlo, G.; van Derksen, N.I.; Heer, P.O.; Kruithof, S.; Loeff, F.L.; Berkhout, L.C.; Linty, F.; Reusken, C.; Reimerink, J.; et al. Dynamics of antibodies to SARS-CoV-2 in convalescent plasma donors. Clin. Transl. Immunol. 2021, 10, e1285. [Google Scholar] [CrossRef]
- Bavaro, D.F.; Laghetti, P.; Milano, E.; Brindicci, G.; Volpe, A.; Lagioia, A.; Saracino, A.; Monno, L. Anti-spike S1 receptor-binding domain antibodies against SARS-CoV-2 persist several months after infection regardless of disease severity. J. Med. Virol. 2021, 93, 3158–3164. [Google Scholar] [CrossRef]
- Bai, Z.; Cao, Y.; Liu, W.; Li, J. The SARS-CoV-2 Nucleocapsid Protein and Its Role in Viral Structure, Biological Functions, and a Potential Target for Drug or Vaccine Mitigation. Viruses 2021, 13, 1115. [Google Scholar] [CrossRef]
- Burbelo, P.D.; Riedo, F.X.; Morishima, C.; Rawlings, S.; Smith, D.; Das, S.; Strich, J.R.; Chertow, D.S.; Davey, R.T., Jr.; Cohen, J.I. Detection of Nucleocapsid Antibody to SARS-CoV-2 is More Sensitive than Antibody to Spike Protein in COVID-19 Patients. medRxiv 2020. [Google Scholar] [CrossRef]
- Krammer, F.; Srivastava, K.; Alshammary, H.; Amoako, A.A.; Awawda, M.H.; Beach, K.F.; Bermúdez-González, M.C.; Bielak, D.A.; Carreño, J.M.; Chernet, R.L.; et al. Antibody Responses in Seropositive Persons after a Single Dose of SARS-CoV-2 mRNA Vaccine. N. Engl. J. Med. 2021, 384, 1372–1374. [Google Scholar] [CrossRef]
- Levi, R.; Azzolini, E.; Pozzi, C.; Ubaldi, L.; Lagioia, M.; Mantovani, A.; Rescigno, M. One dose of SARS-CoV-2 vaccine exponentially increases antibodies in individuals who have recovered from symptomatic COVID-19. J. Clin. Investig. 2021, 131. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Features | SARS-CoV-2-Positive Volunteers (PosV) | SARS-CoV-2-Negative/-Unknown SARS-CoV-2 History (NegV) | p-Value |
|---|---|---|---|
| Number of volunteers | 695 | 194 | |
| Age (mean (SD)) | 47.95 ± 13.92 | 45.92 ± 14.57 | 0.051 |
| Sex (male/female) | 283/412 | 85/109 | 0.459 |
| Volunteers | n | Positive for Anti-NP IgG | Crude Prevalence | Adjusted Prevalence | Positive for Anti-S1RBD IgG | Crude Prevalence | Adjusted Prevalence |
|---|---|---|---|---|---|---|---|
| PosV | 695 | 598 | 86.04% | 88.59% | 645 | 92.81% | 100% |
| NegV | 194 | 25 | 12.89% | 12.38% | 24 | 12.37% | 6.61% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krashias, G.; Deeba, E.; Constantinou, A.; Hadjiagapiou, M.; Koptides, D.; Richter, J.; Tryfonos, C.; Bashiardes, S.; Lambrianides, A.; Loizidou, M.A.; et al. Characterization of IgG Antibody Response against SARS-CoV-2 (COVID-19) in the Cypriot Population. Microorganisms 2022, 10, 85. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms10010085
Krashias G, Deeba E, Constantinou A, Hadjiagapiou M, Koptides D, Richter J, Tryfonos C, Bashiardes S, Lambrianides A, Loizidou MA, et al. Characterization of IgG Antibody Response against SARS-CoV-2 (COVID-19) in the Cypriot Population. Microorganisms. 2022; 10(1):85. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms10010085
Chicago/Turabian StyleKrashias, George, Elie Deeba, Astero Constantinou, Maria Hadjiagapiou, Dana Koptides, Jan Richter, Christina Tryfonos, Stavros Bashiardes, Anastasia Lambrianides, Maria A. Loizidou, and et al. 2022. "Characterization of IgG Antibody Response against SARS-CoV-2 (COVID-19) in the Cypriot Population" Microorganisms 10, no. 1: 85. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms10010085