
Clinical, Laboratory, and Radiographic Features Can Help Predict Mycoplasma pneumoniae Lower Respiratory Tract Infection in Children

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
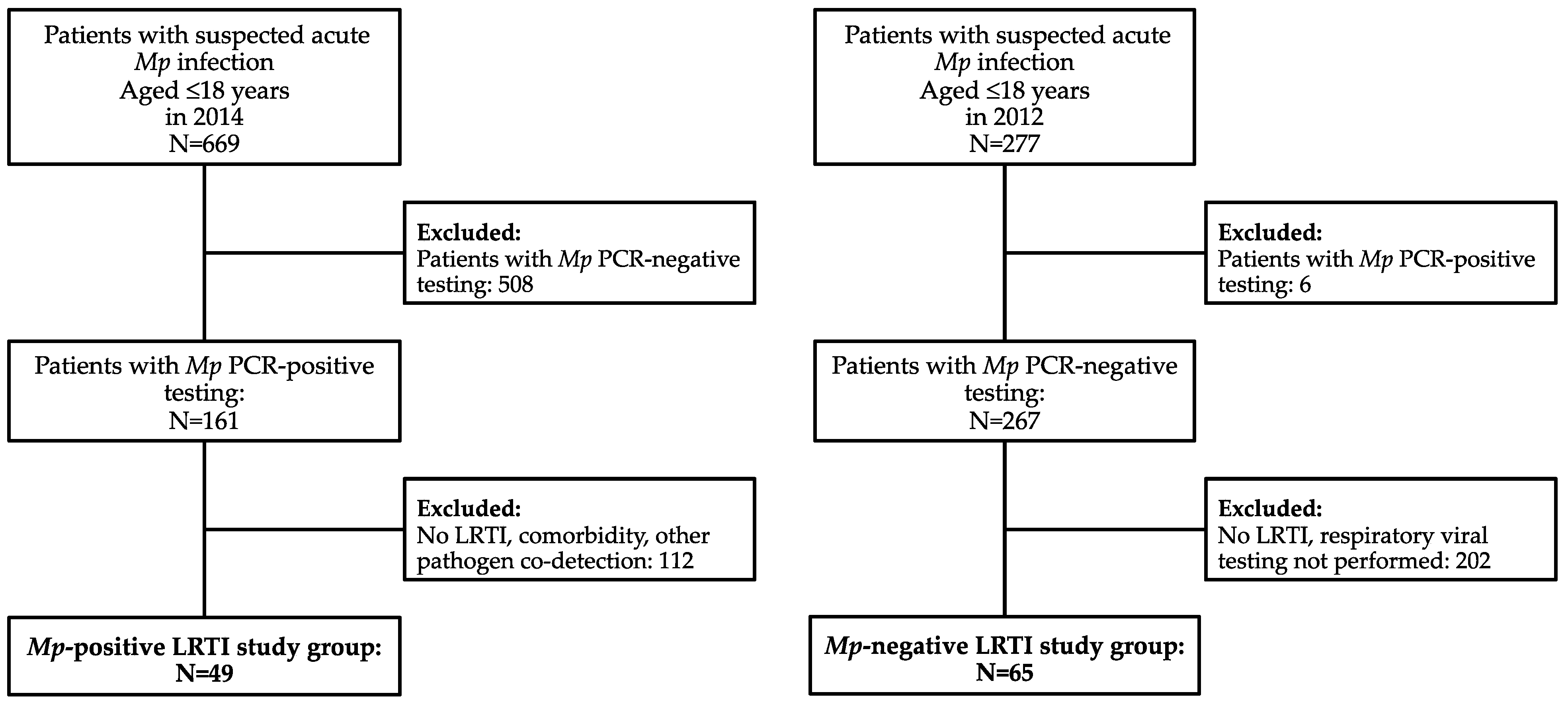
2.2. Study Subjects
2.2.1. Mp pneumoniae PCR-Positive LRTI Group
2.2.2. Mp pneumoniae PCR-Negative LRTI Group
2.3. Methods
2.4. Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Waites, K.B.; Xiao, L.; Liu, Y.; Balish, M.F.; Atkinson, T.P. Mycoplasma pneumoniae from the respiratory tract and beyond. Clin. Microbiol. Rev. 2017, 30, 747–809. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, T.P.; Waites, K.B. Mycoplasma pneumoniae infections in childhood. Pediatr. Infect. Dis. J. 2014, 33, 92–94. [Google Scholar] [CrossRef] [PubMed]
- Kutty, P.K.; Jain, S.; Taylor, T.H.; Bramley, A.M.; Diaz, M.H.; Ampofo, K.; Arnold, S.; Williams, D.; Edwards, K.; McCullers, J.; et al. Mycoplasma pneumoniae among children hospitalized with community-acquired pneumonia. Clin. Infect. Dis. 2019, 68, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Blasi, F. Atypical pathogens and respiratory tract infections. Eur. Respir. J. 2004, 24, 171–181. [Google Scholar] [CrossRef]
- Wang, K.; Gill, P.; Perera, R.; Thomson, A.; Mant, D.; Harnden, A. Clinical symptoms and signs for the diagnosis of Mycoplasma pneumoniae in children and adolescents with community-acquired pneumonia. Cochrane Database Syst. Rev. 2012, 10, CD009175. [Google Scholar]
- Spuesens, E.B.; Fraaij, P.L.; Visser, E.G.; Hoogenboezem, T.; Hop, W.C.; van Adrichem, L.N.; Weber, F.; Moll, H.A.; Broekman, B.; Berger, M.Y.; et al. Carriage of Mycoplasma pneumoniae in the upper respiratory tract of symptomatic and asymptomatic children: An observational study. PLoS Med. 2013, 10, e1001444. [Google Scholar] [CrossRef]
- Li, X.; Atkinson, T.P.; Hagood, J.; Makris, C.; Duffy, L.B.; Waites, K.B. Emerging macrolide resistance in Mycoplasma pneumoniae in children: Detection and characterization of resistant isolates. Pediatr. Infect. Dis. J. 2009, 28, 693–696. [Google Scholar] [CrossRef]
- Yamada, M.; Buller, R.; Bledsoe, S.; Storch, G.A. Rising rates of macrolide-resistant Mycoplasma pneumoniae in the central United States. Pediatr. Infect. Dis. J. 2012, 31, 409–411. [Google Scholar] [CrossRef]
- Principi, N.; Esposito, S. Macrolide-resistant Mycoplasma pneumoniae: Its role in respiratory infection. J. Antimicrob. Chemother. 2013, 68, 506–511. [Google Scholar] [CrossRef]
- Kogoj, R.; Praprotnik, M.; Mrvič, T.; Korva, M.; Keše, D. Genetic diversity and macrolide resistance of Mycoplasma pneumoniae isolates from two consecutive epidemics in Slovenia. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 99–107. [Google Scholar] [CrossRef]
- Jevšnik Virant, M.; Uršič, T.; Kogoj, R.; Korva, M.; Petrovec, M.; Avšič-Županc, T. Evaluation of Two Broadly Used Commercial Methods for Detection of Respiratory Viruses with a Recently Added New Target for Detection of SARS-CoV-2. Viruses 2022, 14, 1530. [Google Scholar] [CrossRef]
- Jain, S.; Williams, D.J.; Arnold, S.R.; Ampofo, K.; Bramley, A.M.; Reed, C.; Stockmann, C.; Anderson, E.J.; Grijalva, C.G.; Self, W.H.; et al. CDC EPIC Study Team. Community-acquired pneumonia requiring hospitalization among U.S. children. N. Engl. J. Med. 2015, 372, 835–845. [Google Scholar] [CrossRef]
- Liu, B.; Chang, X.; Yan, N. Clinical analysis of the epidemiology and changes in inflammatory indexes of Mycoplasma pneumonia in acute and recovery stage pediatric patients. Transl. Pediatr. 2022, 11, 1645–1655. [Google Scholar] [CrossRef]
- Han, M.S.; Yun, K.W.; Lee, H.J.; Park, J.Y.; Rhie, K.; Lee, J.K.; Lee, H.; Kwak, Y.H.; Kim, D.K.; Suh, D.I.; et al. Contribution of Co-detected Respiratory Viruses and Patient Age to the Clinical Manifestations of Mycoplasma pneumoniae Pneumonia in Children. Pediatr. Infect. Dis. J. 2018, 37, 531–536. [Google Scholar] [CrossRef]
- Cilla, G.; Oñate, E.; Perez-Yarza, E.G.; Montes, M.; Vicente, D.; Perez-Trallero, E. Viruses in community-acquired pneumonia in children aged less than 3 years old: High rate of viral coinfection. J. Med. Virol. 2008, 80, 1843–1849. [Google Scholar] [CrossRef]
- Rhedin, S.; Lindstrand, A.; Hjelmgren, A.; Ryd-Rinder, M.; Öhrmalm, L.; Tolfvenstam, T.; Örtqvist, Å.; Rotzén-Östlund, M.; Zweygberg-Wirgart, B.; Henriques-Normark, B.; et al. Respiratory viruses associated with community-acquired pneumonia in children: Matched case-control study. Thorax 2015, 70, 847–853. [Google Scholar] [CrossRef] [PubMed]
- Meyer Sauteur, P.M.; Krautter, S.; Ambroggio, L.; Seiler, M.; Paioni, P.; Relly, C.; Capaul, R.; Kellenberger, C.; Haas, T.; Gysin, C.; et al. Improved Diagnostics Help to Identify Clinical Features and Biomarkers That Predict Mycoplasma pneumoniae Community-acquired Pneumonia in Children. Clin. Infect. Dis. 2020, 71, 1645–1654. [Google Scholar] [CrossRef]
- Mandell, L.A. Community-acquired pneumonia: An overview. Postgrad. Med. 2015, 127, 607–615. [Google Scholar] [CrossRef]
- Marino, S.; Pavone, P.; Marino, L.; Nunnari, G.; Ceccarelli, M.; Coppola, C.; Distefano, C.; Falsaperla, R. SARS-CoV-2: The Impact of Co-Infections with Particular Reference to Mycoplasma pneumonia—A Clinical Review. Microorganisms 2022, 10, 1936. [Google Scholar] [CrossRef]
- Wallihan, R.G.; Suárez, N.M.; Cohen, D.M.; Marcon, M.; Moore-Clingenpeel, M.; Mejias, A.; Ramilo, O. Molecular Distance to Health Transcriptional Score and Disease Severity in Children Hospitalized with Community-Acquired Pneumonia. Front. Cell. Infect. Microbiol. 2018, 8, 382. [Google Scholar] [CrossRef]
- Jeong, J.E.; Soh, J.E.; Kwak, J.H.; Jung, H.L.; Shim, J.W.; Kim, D.S.; Park, M.S.; Shim, J.Y. Increased procalcitonin level is a risk factor for prolonged fever in children with Mycoplasma pneumonia. Korean J. Pediatr. 2018, 61, 258–263. [Google Scholar] [CrossRef] [PubMed]
- Alcoba, G.; Keitel, K.; Maspoli, V.; Lacroix, L.; Manzano, S.; Gehri, M.; Tabin, R.; Gervaix, A.; Galetto-Lacour, A. A three-step diagnosis of pediatric pneumonia at the emergency department using clinical predictors, C-reactive protein, and pneumococcal PCR. Eur. J. Pediatr. 2017, 176, 815–824. [Google Scholar] [CrossRef] [PubMed]
- Gordon, O.; Oster, Y.; Michael-Gayego, A.; Marans, R.S.; Averbuch, D.; Engelhard, D.; Moses, A.E.; Nir-Paz, R. The Clinical Presentation of Pediatric Mycoplasma pneumoniae Infections—A Single Center Cohort. Pediatr. Infect. Dis. J. 2019, 38, 698–705. [Google Scholar] [CrossRef]
- Narita, M. Classification of Extrapulmonary Manifestations Due to Mycoplasma pneumoniae Infection on the Basis of Possible Pathogenesis. Front. Microbiol. 2016, 7, 23. [Google Scholar] [CrossRef]
- Sánchez-Vargas, F.M.; Gómez-Duarte, O.G. Mycoplasma pneumoniae—An emerging extra-pulmonary pathogen. Clin. Microbiol. Infect. 2008, 14, 105–117. [Google Scholar] [CrossRef]
- Hu, J.; Ye, Y.; Chen, X.; Xiong, L.; Xie, W.; Liu, P. Insight into the Pathogenic Mechanism of Mycoplasma pneumoniae. Curr. Microbiol. 2022, 80, 14. [Google Scholar] [CrossRef]
- Rodman Berlot, J.; Krivec, U.; Praprotnik, M.; Mrvič, T.; Kogoj, R.; Keše, D. Clinical characteristics of infections caused by Mycoplasma pneumoniae P1 genotypes in children. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 1265–1272. [Google Scholar] [CrossRef]
- Terraneo, L.; Lava, S.A.; Camozzi, P.; Zgraggen, L.; Simonetti, G.D.; Bianchetti, M.G.; Milani, G.P. Unusual eruptions associated with Mycoplasma pneumoniae respiratory infections: Review of the literature. Dermatology 2015, 231, 152–157. [Google Scholar] [CrossRef]
- Canavan, T.N.; Mathes, E.F.; Frieden, I. Mycoplasma pneumoniae-induced rash and mucositis as a syndrome distinct from Stevens-Johnson syndrome and erythema multiforme: A systematic review. J. Am. Acad. Dermatol. 2015, 72, 239–245. [Google Scholar] [CrossRef]
- Rodman Berlot, J.; Mrvič, T.; Košnik, M.; Keše, D. The Association between Mycoplasma pneumoniae Genotype and Cutaneous Disease. Microorganisms 2023, 11, 205. [Google Scholar] [CrossRef]
- Cho, Y.J.; Han, M.S.; Kim, W.S.; Choi, E.H.; Choi, Y.H.; Yun, K.W.; Lee, S.; Cheon, J.E.; Kim, I.O.; Lee, H.J. Correlation between chest radiographic findings and clinical features in hospitalized children with Mycoplasma pneumoniae pneumonia. PLoS ONE 2019, 14, e0219463. [Google Scholar] [CrossRef] [PubMed]
- Bradley, J.S.; Byington, C.L.; Shah, S.S.; Alverson, B.; Carter, E.R.; Harrison, C.; Kaplan, S.L.; Mace, S.E.; McCracken, G.H., Jr.; Moore, M.R.; et al. The management of community-acquired pneumonia in infants and children older than 3 months of age: Clinical practice guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America. Clin. Infect. Dis. 2011, 53, e25–e76. [Google Scholar] [CrossRef]
- Bandell, R.A.M.; Dekkers, T.; Semmekrot, B.A.; de Wildt, S.N.; Fleuren, H.W.H.A.; Warlé-van Herwaarden, M.F.; Füssenich, P.; Gerrits, G.P.; Kramers, C. Macrolide prescription in Dutch children: Compliance with guidelines. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 675–681. [Google Scholar] [CrossRef]
- Oishi, T.; Ouchi, K. Recent Trends in the Epidemiology, Diagnosis, and Treatment of Macrolide-Resistant Mycoplasma pneumoniae. J. Clin. Med. 2022, 11, 1782. [Google Scholar] [CrossRef]
- Loconsole, D.; De Robertis, A.L.; Sallustio, A.; Centrone, F.; Morcavallo, C.; Campanella, S.; Accogli, M.; Chironna, M. Update on the Epidemiology of Macrolide-Resistant Mycoplasma pneumoniae in Europe: A Systematic Review. Infect. Dis. Rep. 2021, 13, 811–820. [Google Scholar] [CrossRef]
- Leng, M.; Yang, J.; Zhou, J. The molecular characteristics, diagnosis, and treatment of macrolide-resistant Mycoplasma pneumoniaein children. Front. Pediatr. 2023, 11, 1115009. [Google Scholar] [CrossRef]
- Vázquez-Laslop, N.; Mankin, A.S. How Macrolide Antibiotics Work. Trends. Biochem. Sci. 2018, 43, 668–684. [Google Scholar] [CrossRef]
- Kogoj, R.; Mrvič, T.; Praprotnik, M.; Keše, D. Prevalence, genotyping and macrolide resistance of Mycoplasma pneumoniae among isolates of patients with respiratory tract infections, Central Slovenia, 2006 to 2014. Eurosurveillance 2015, 20, 30018. [Google Scholar] [CrossRef]
- Dumke, R.; Stolz, S.; Jacobs, E.; Juretzek, T. Molecular characterization of macrolide resistance of a Mycoplasma pneumoniae strain that developed during therapy of a patient with pneumonia. Int. J. Infect. Dis. 2014, 29, 197–199. [Google Scholar] [CrossRef]
- Zhou, Y.; Zhang, Y.; Sheng, Y.; Zhang, L.; Shen, Z.; Chen, Z. More complications occur in macrolide-resistant than in macrolide-sensitive Mycoplasma pneumoniae pneumonia. Antimicrob. Agents Chemother. 2014, 58, 1034–1038. [Google Scholar] [CrossRef]
- Dumke, R. Molecular Tools for Typing Mycoplasma pneumoniae and Mycoplasma genitalium. Front. Microbiol. 2022, 13, 904494. [Google Scholar] [CrossRef] [PubMed]
- Simon, A.K.; Hollander, G.A.; McMichael, A. Evolution of the immune system in humans from infancy to old age. Proc. Biol. Sci. 2015, 282, 20143085. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Mp PCR-Positive LRTI | Mp PCR-Negative LRTI | Test Statistic | p Value | |
|---|---|---|---|---|
| Subjects N | 49 | 65 | ||
| Boys/girls (%) | 59.2/40.8 | 66.2/33.8 | χ2 = 0.583 | 0.445 |
| Age (years) | 5.8 (IQR 3.4–8.6) | 2.2 (IQR 1.3–4.5) | U = 729.00 | <0.001 |
| <5 years (%) 5–18 years (%) | 44.9 (22/49)55.1 (27/49) | 76.9 (50/65)23.1 (15/65) | χ2 = 4.89 | 0.027 |
| Duration of symptoms (days) | 7 (IQR 5–10) | 4 (IQR 2–7) | U = 866.00 | <0.001 |
| CRP (mg/L) | 13 (IQR 7–28) | 17 (IQR 7–48) | U = 1423.50 | 0.539 |
| WBC (×109/L) | 9.9 (IQR 7.0–11.6) | 12.7 (IQR 9.3–15.6) | U = 935.00 | <0.001 |
| Radiographic findings | ||||
| Effusion (%) | 22.0 (9/41) | 21.8 (12/55) | χ2 = 0.00 | 0.988 |
| Unilateral/Bilateral infiltrates (%) | 57.5/32.5 | 24.1/75.9 | χ2 = 10.87 | 0.001 |
| Extrapulmonary manifestations | ||||
| All (%) | 16.3 (8/49) | 21.5 (14/65) | χ2 = 4.87 | 0.485 |
| Dermatological (%) | 12.2 (6/49) | 4.6 (3/65) | χ2 = 2.24 | 0.135 |
| Gastrointestinal (%) | 0 (0/49) | 10.8 (7/65) | χ2 = 5.62 | 0.018 |
| Cardiovascular (%) | 2.0 (1/49) | 0 (0/65) | χ2 = 1.34 | 0.247 |
| Neurological (%) | 2.0 (1/49) | 1.5 (1/65) | χ2 = 0.04 | 0.840 |
| Ophtalmological (%) | 0 (0/49) | 3.1 (2/65) | χ2 = 1.54 | 0.215 |
| Hospitalization (%) | 75.5 (37/49) | 90.7 (59/65) | χ2 = 4.89 | 0.027 |
| Mp PCR-Positive LRTI | Mp PCR-Negative LRTI | Test Statistic | p Value | |
|---|---|---|---|---|
| Subjects N | 37 | 59 | ||
| Age (years) | 4.9 (IQR 3.2–8.1) | 2.2 (IQR 1.3–4.6) | U = 542.00 | <0.001 |
| <5 years (%) 5–18 years (%) | 51.4 (19/37) 48.6 (18/37) | 76.3 (45/59) 23.7 (14/59) | χ2 = 6.36 | 0.012 |
| Hospital stay (days) | 3 (IQR 2–5) | 5 (IQR 4–8) | U = 532.50 | <0.001 |
| Oxygen therapy (%) | 54.1 (20/37) | 86.4 (51/59) | χ2 = 12.38 | <0.001 |
| Odds Ratio (OR) | 95% CI for OR | p Value | |
|---|---|---|---|
| Age | 1.28 | 1.08–1.52 | 0.005 |
| Duration of symptoms | 1.15 | 1.01–1.31 | 0.038 |
| CRP | 0.97 | 0.95–0.99 | 0.012 |
| X-ray infiltrates * | 3.15 | 1.02–9.72 | 0.046 |
| Extrapulmonary manifestations | 0.88 | 0.21–3.69 | 0.856 |
| Hospitalization | 0.29 | 0.04–2.21 | 0.233 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodman Berlot, J.; Dolenc, Š.; Krivec, U.; Keše, D. Clinical, Laboratory, and Radiographic Features Can Help Predict Mycoplasma pneumoniae Lower Respiratory Tract Infection in Children. Microorganisms 2023, 11, 1358. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms11051358
Rodman Berlot J, Dolenc Š, Krivec U, Keše D. Clinical, Laboratory, and Radiographic Features Can Help Predict Mycoplasma pneumoniae Lower Respiratory Tract Infection in Children. Microorganisms. 2023; 11(5):1358. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms11051358
Chicago/Turabian StyleRodman Berlot, Jasna, Špela Dolenc, Uroš Krivec, and Darja Keše. 2023. "Clinical, Laboratory, and Radiographic Features Can Help Predict Mycoplasma pneumoniae Lower Respiratory Tract Infection in Children" Microorganisms 11, no. 5: 1358. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms11051358