Pathological and Virological Studies of p16-Positive Oropharyngeal Carcinoma with a Good Response to Neoadjuvant Chemotherapy

 , ,
, ,  and
and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case and Methods
3. Results
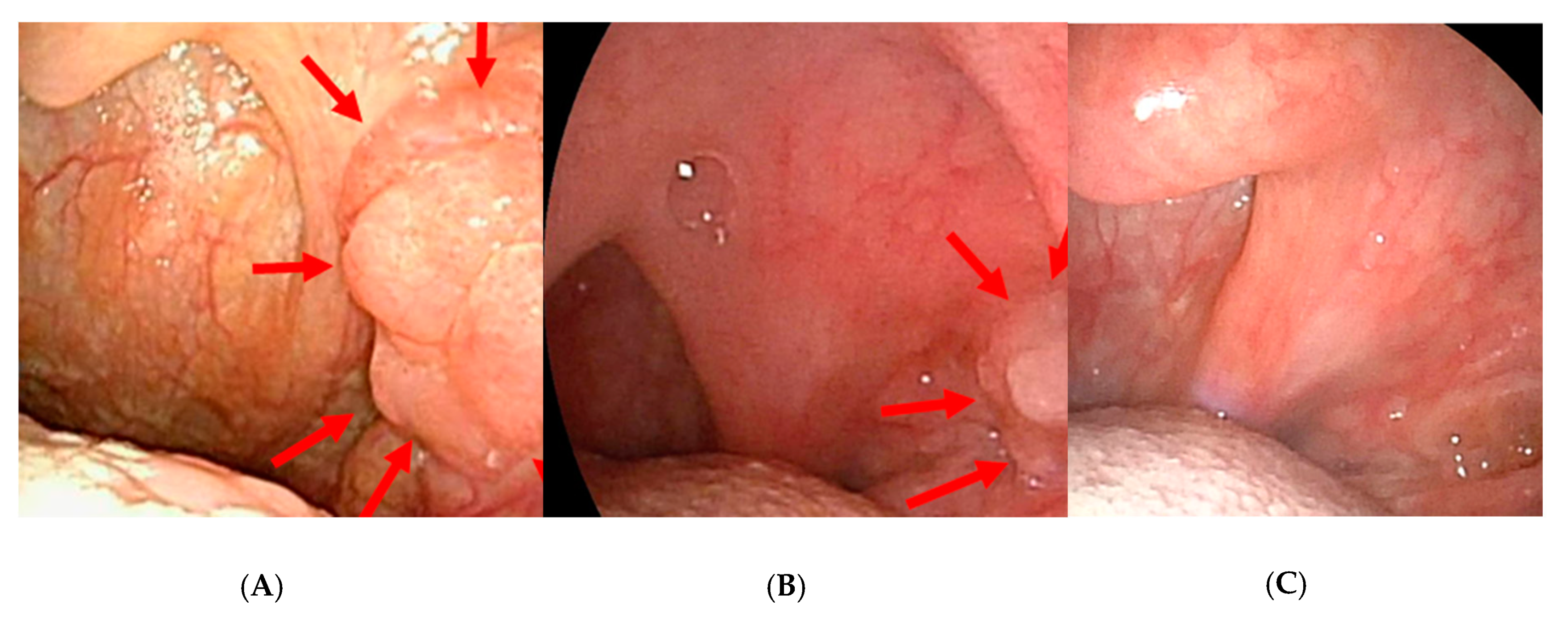
3.1. Macroscopic Findings of the Primary Lesion before and after Neoadjuvant Chemotherapy
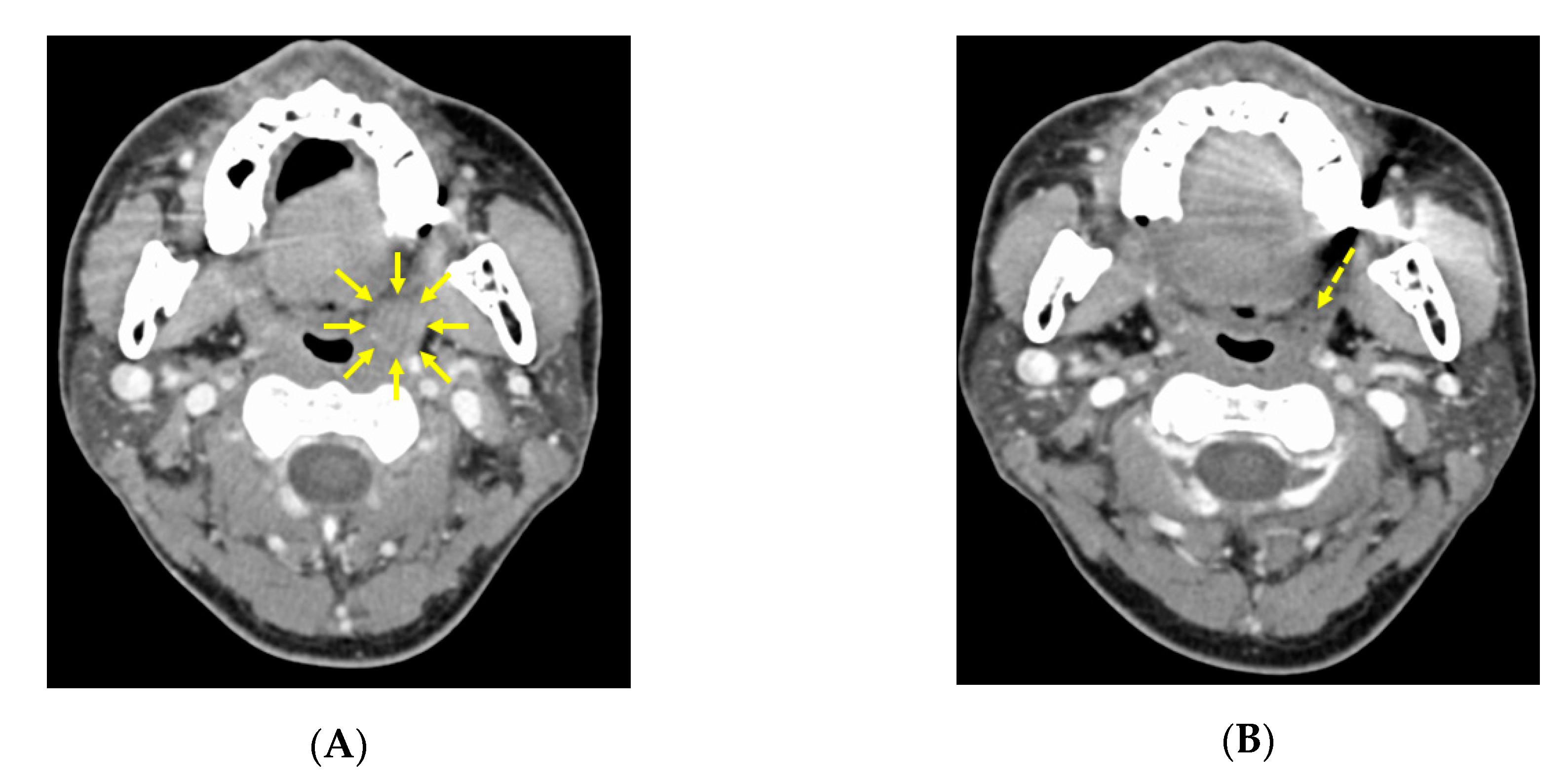
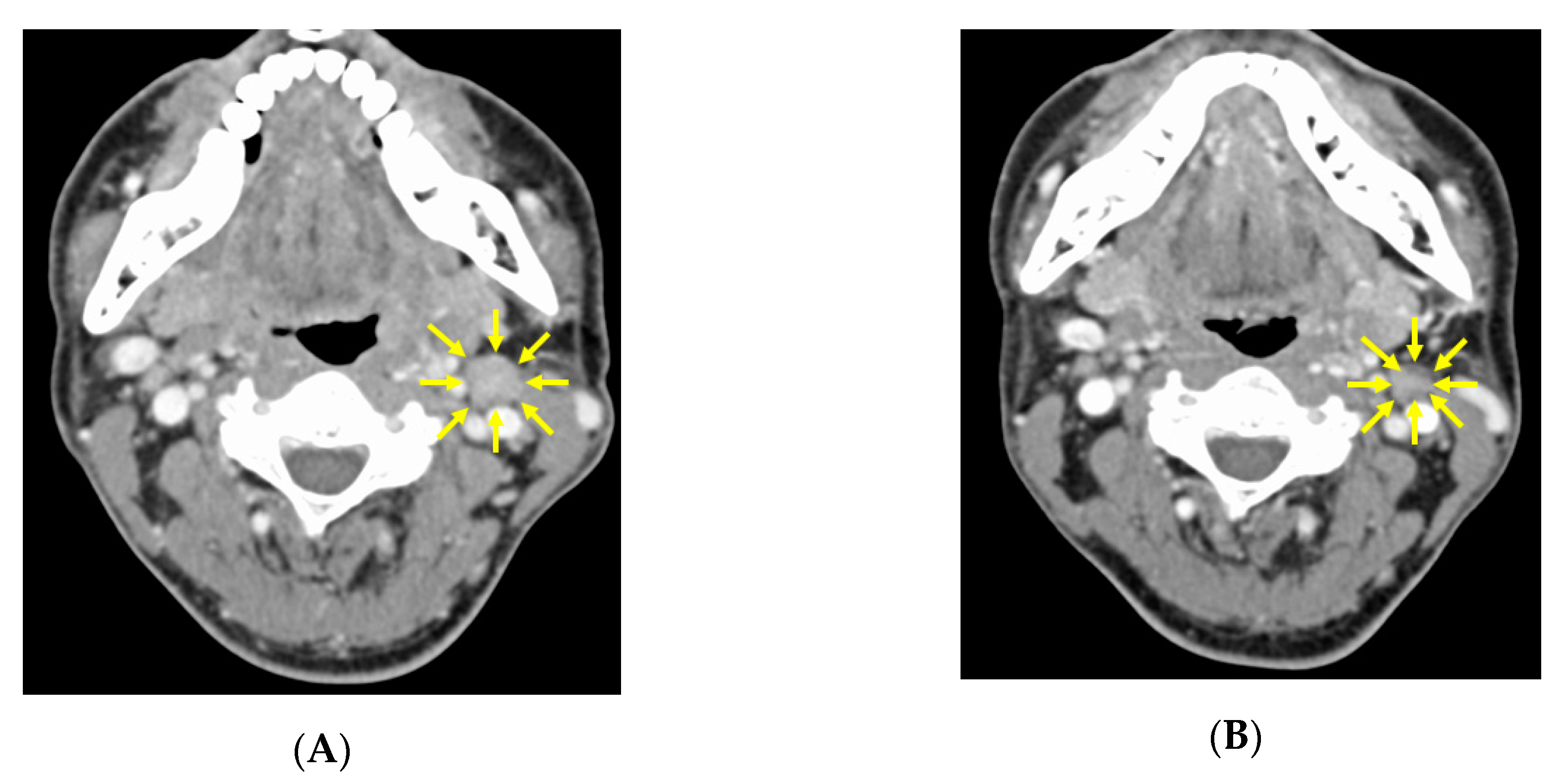
3.2. CT image Findings before and after Neoadjuvant Chemotherapy
3.3. Clinical Assessment after Neoadjuvant Chemotherapy and the Definitive Treatment Decision
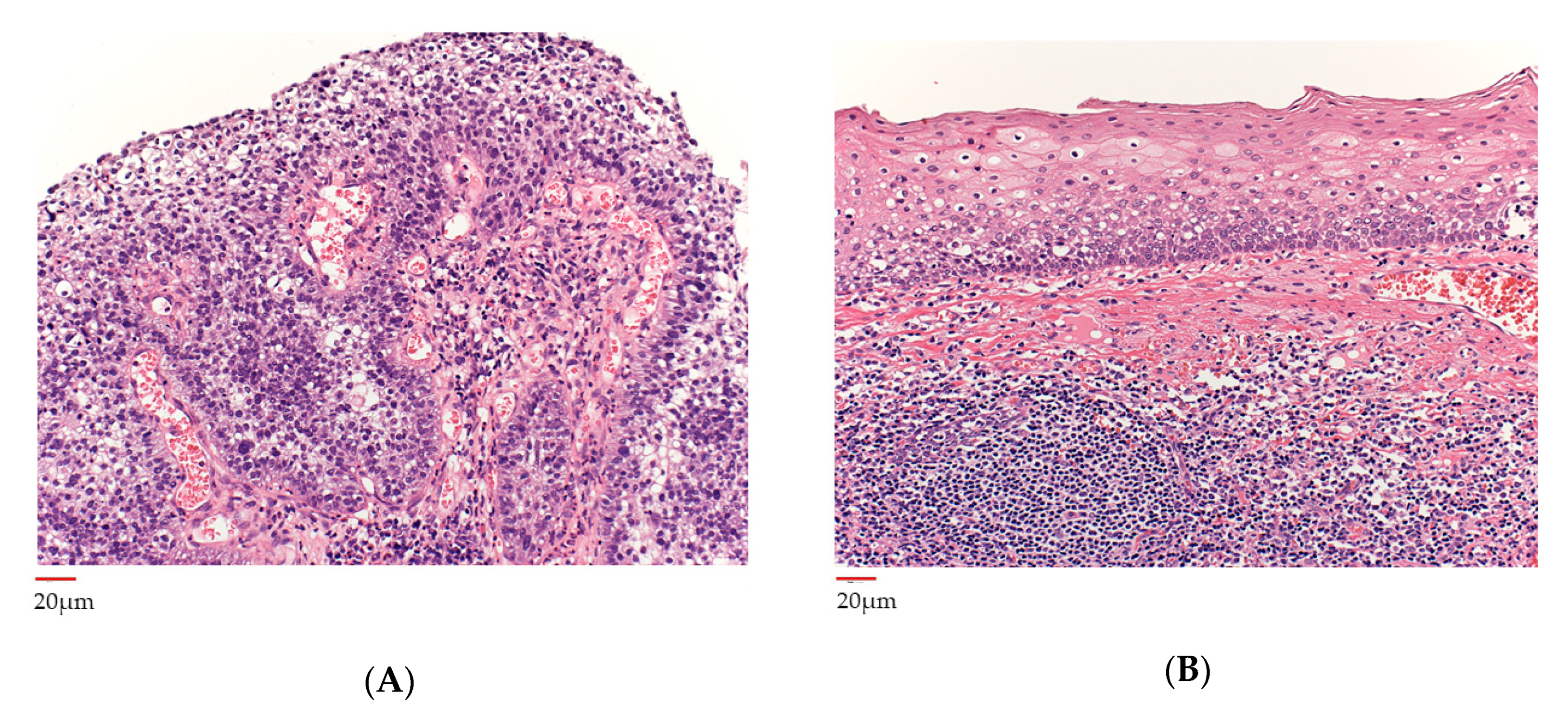
3.4. Histopathological Analysis before and after Neoadjuvant Chemotherapy
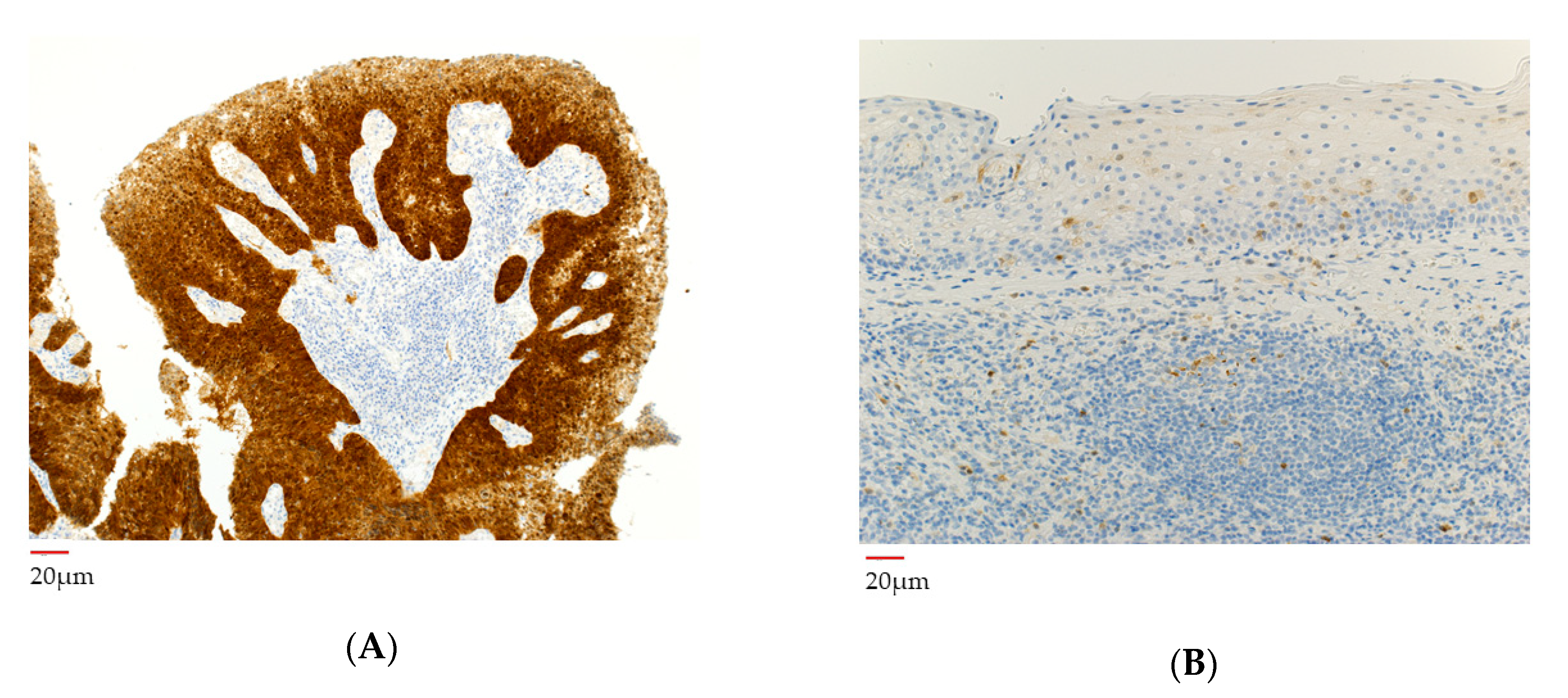
3.5. p16 Analysis before and after Neoadjuvant Chemotherapy
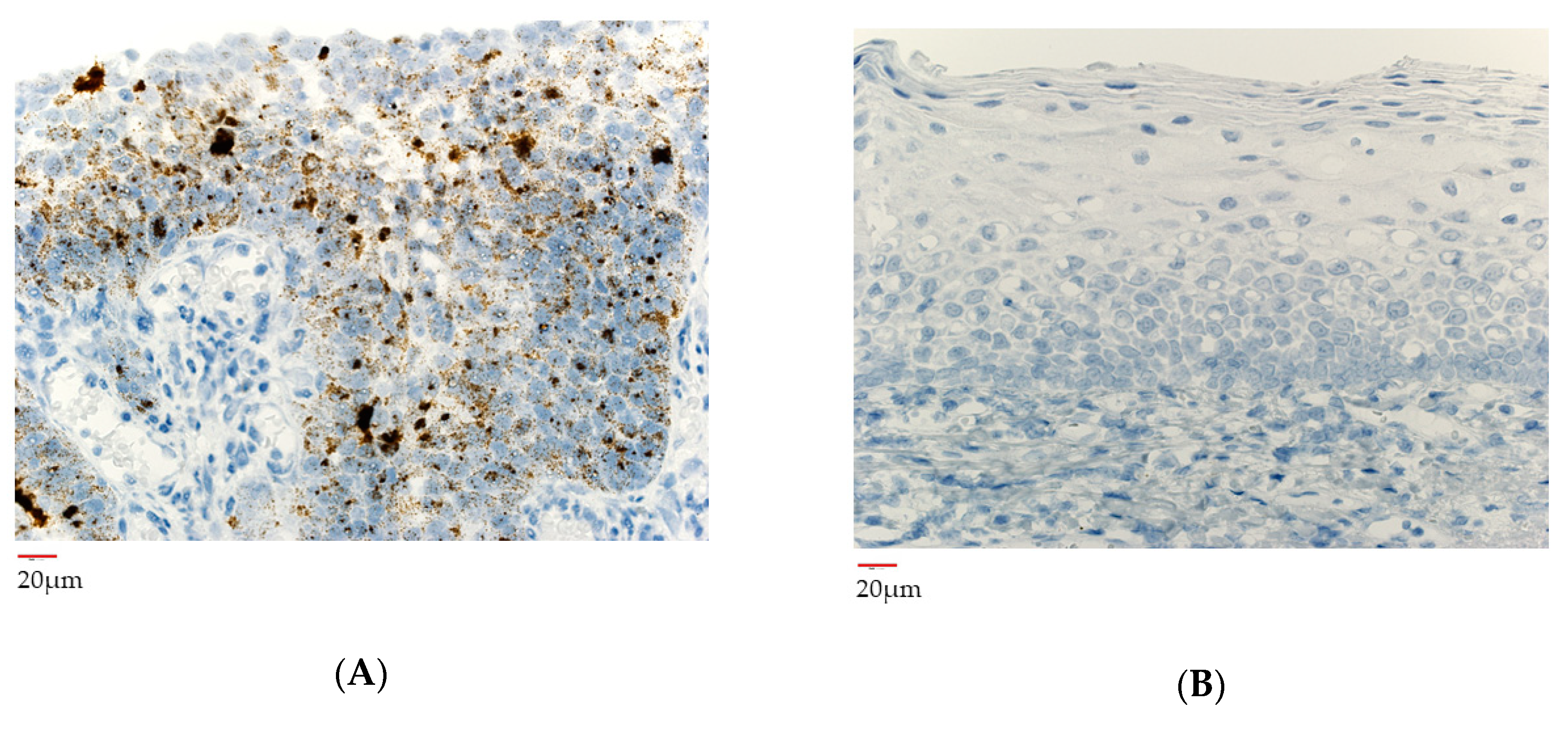
3.6. HPV Gene Integrated Cells before and after Neoadjuvant Chemotherapy
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Ang, K.K.; Harris, J.; Wheeler, R.; Weber, R.; Rosenthal, D.I.; Nguyen-Tân, P.F.; Westra, W.H.; Chung, C.H.; Jordan, R.C.; Luet, C.; et al. Human papilloma virus and survival of patients with oropharyngeal cancer. N. Engl. J. Med. 2010, 363, 24–35. [Google Scholar] [CrossRef] [Green Version]
- Ragin, C.C.; Taioli, E. Survival of squamous cell carcinoma of the head and neck in relation to human papillomavirus infection: Review and meta-analysis. Int. J. Cancer 2007, 121, 1813–1820. [Google Scholar] [CrossRef]
- Posner, M.R.; Lorch, J.H.; Goloubeva, O.; Tan, M.; Schumaker, L.M.; Sarlis, N.J.; Haddad, R.I.; Cullen, K.J. Survival and human papillomavirus in oropharynx cancer in TAX 324: A subset analysis from an international phase III trial. Ann. Oncol. 2011, 22, 1071–1077. [Google Scholar] [CrossRef]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Rookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual:Continuing to Build a Bridge From a Population-Basedto a More “Personalized” Approach to Cancer Staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef]
- Adelstein, D.J.; Ismaila, N.; Ku, J.A.; Burtness, B.; Swiecicki, P.L.; Mell, L.; Beitler, J.J.; Gross, N.; Jones, C.U.; Kaufman, M.; et al. Role of Treatment Deintensification in the Management of p16+ Oropharyngeal Cancer: ASCO Provisional Clinical Opinion. J. Clin. Oncol. 2019, 37, 1578–1589. [Google Scholar] [CrossRef]
- Damien, U.; June, C.; Danny, R. What is the best treatment for patients with human papillomavirus-positive and -negative oropharyngeal cancer? Cancer 2014, 120, 1462–1470. [Google Scholar]
- Howard, J.; Dwivedi, R.C.; Masterson, L.; Kothari, P.; Quon, H.; Holsinger, F.C. De-intensified adjuvant (chemo)radiotherapy versus standard adjuvant chemoradiotherapy post transoral minimally invasive surgery for resectable HPV-positive oropharyngeal carcinoma. Cochrane Database Syst. Rev. 2018, 12, CD012939. [Google Scholar]
- Cohen, E.E.; LaMonte, S.J.; Erb, N.L.; Beckman, K.L.; Sadeghi, N.; Hutcheson, K.A.; Stubblefield, M.D.; Abbott, D.M.; Fisher, P.S.; Stein, K.D.; et al. American Cancer Society head and neck cancer survivorship care guideline. CA Cancer J. Clin. 2016, 66, 203–239. [Google Scholar] [CrossRef] [PubMed]
- Margalit, D.N.; Wong, S.J. Reirradiation for Head and Neck Cancer: The Who and the How. Int. J. Radiat. Oncol. Biol. Phys. 2018, 100, 618–620. [Google Scholar] [CrossRef] [PubMed]
- Budach, W.; Bölke, E.; Kammers, K.; Gerber, P.A.; Orth, K.; Gripp, S.; Matuschek, C. Induction chemotherapy followed by concurrent radio-chemotherapy versus concurrent radio-chemotherapy alone as treatment of locally advanced squamous cell carcinoma of the head and neck (HNSCC): A meta-analysis of randomized trials. Radiother. Oncol. 2016, 118, 238–243. [Google Scholar] [CrossRef] [Green Version]
- Huguet, F.; Schick, U.; Pointreau, Y. [Role of induction chemotherapy in head and neck cancer: Cons]. Cancer Radiother. 2017, 21, 510–514. [Google Scholar] [CrossRef]
- Hinni, M.L.; Nagel, T.; Howard, B. Oropharyngeal cancer treatment: The role of transoral surgery. Curr. Opin. Otolaryngol. Head Neck Surg. 2015, 23, 132–138. [Google Scholar] [CrossRef]
- Sadeghi, N.; Khalife, S.; Mascarella, M.A.; Ramanakumar, A.V.; Richardson, K.; Joshi, A.S.; Bouganim, N.; Taheri, R.; Fuson, A.; Siegel, R. Pathologic response to neoadjuvant chemotherapy in HPV-associated oropharynx cancer. Head Neck 2020, 42, 417–425. [Google Scholar] [CrossRef] [PubMed]
- Smeets, S.J.; Hesselink, A.T.; Speel, E.J.M.; Haesevoets, A.; Snijders, P.J.F.; Pawlita, M.; Meijer, C.J.L.M.; Braakhuis, B.J.M.; Leemans, C.R.; Brakenhoff, R.H. A novel algorithm for reliable detection of human papillomavirus in paraffin embedded head and neck cancer specimen. Int. J. Cancer. 2007, 121, 2465–2472. [Google Scholar] [CrossRef] [PubMed]
- Roner, M.R.; Carraher, C.E., Jr. Cisplatin Derivatives as Antiviral Agents. In Inorganic and Organometallic Macromolecules; Abd-El-Aziz, A.S., Carraher, C.E., Pittman, C.U., Zeldin, M., Eds.; Springer: New York, NY, USA, 2008; pp. 193–223. [Google Scholar]
- Mighty, K.K.; Laimins, L.A. The role of human papillomaviruses in oncogenesis. Recent Results Cancer Res. 2014, 19, 135–148. [Google Scholar]
- Wesierska-Gadek, J.; Schloffer, D.; Kotala, V.; Horky, M. Escape of p53 protein from E6-mediated degradation in HeLa cells after cisplatin therapy. Int. J. Cancer. 2002, 101, 128–136. [Google Scholar] [CrossRef]
- Näsman, A.; Romanitan, M.; Nordfors, C.; Grün, N.; Johansson, H.; Hammarstedt, L.; Marklund, L.; Munck-Wikland, E.; Dalianis, T.; Ramqvist, T. Tumor Infiltrating CD8+ and Foxp3+ Lymphocytes Correlate to Clinical Outcome and Human Papillomavirus (HPV) Status in Tonsillar Cancer. PLoS ONE 2012, 7, e38711. [Google Scholar] [CrossRef]
- Leduc, C.; Adam, J.; Louvet, E.; Sourisseau, T.; Dorvault, N.; Bernard, M.; Maingot, E.; Faivre, L.; Cassin-Kuo, M.; Boissier, E. TPF induction chemotherapy increases PD-L1 expression in tumour cells and immune cells in head and neck squamous cell carcinoma. ESMO Open. 2018, 3, e000257. [Google Scholar] [CrossRef] [Green Version]
- Shuai, Z.; Jiao-Jiao, L.; Li-Jie, W.; Xiao-Min, S.; Jia-Qi, Z.; Li, X.; Luo, W.; Zhao, L. In Vitro and In Vivo Synergistic Therapeutic Effect of Cisplatin with Human Papillomavirus16 E6/E7 CRISPR/Cas9 on Cervical Cancer Cell Line. Transl. Oncol. 2016, 9, 498–504. [Google Scholar]
- Hancock, G.; Hellner, K.; Dorrell, L. Therapeutic HPV vaccine. Best Pract Res Clin. Obstet. Gvnecol. 2018, 47, 59–72. [Google Scholar] [CrossRef]
- Huang, S.H.; Perez-Ordonez, B.; Weinreb, I.; Hope, A.; Massey, C.; Waldron, J.N.; Kim, J.; Bayley, A.J.; Cummings, B.; Cho, B.C.J.; et al. Natural course of distant metastases following radiotherapy or chemoradiotherapy in HPV-related oropharyngeal cancer. Oral Oncol. 2013, 49, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Marur, S.; D’Souza, G.; Westra, W.H.; Forastiere, A.A. HPV-associated head and neck cancer: A virus-related cancer epidemic. Lancet Oncol. 2010, 11, 781–789. [Google Scholar] [CrossRef] [Green Version]
- Chera, B.S.; Amdur, R.J.; Green, R.; Shen, C.; Gupta, G.; Tan, X.; Knowles, M.; Fried, D.; Hayes, N.; Weiss, J.; et al. Phase II Trial of De-Intensified Chemoradiotherapy for Human Papillomavirus-Associated Oropharyngeal Squamous Cell Carcinoma. J. Clin. Oncol. 2019, 37, 2661–2669. [Google Scholar] [CrossRef]
- Zanoni, D.K.; Patel, S.G.; Shah, J.P. Changes in the 8th Edition of the American Joint Committee on Cancer (AJCC) Staging of Head and Neck Cancer: Rationale and implications. Curr. Oncol. Rep. 2019, 21, 52. [Google Scholar] [CrossRef]






© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inukai, D.; Kan, T.; Yamanaka, S.; Okamoto, H.; Fujimoto, Y.; Ito, T.; Taniguchi, N.; Yamamoto, Y.; Tsuzuki, T.; Takami, A.; et al. Pathological and Virological Studies of p16-Positive Oropharyngeal Carcinoma with a Good Response to Neoadjuvant Chemotherapy. Microorganisms 2020, 8, 1497. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms8101497
Inukai D, Kan T, Yamanaka S, Okamoto H, Fujimoto Y, Ito T, Taniguchi N, Yamamoto Y, Tsuzuki T, Takami A, et al. Pathological and Virological Studies of p16-Positive Oropharyngeal Carcinoma with a Good Response to Neoadjuvant Chemotherapy. Microorganisms. 2020; 8(10):1497. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms8101497
Chicago/Turabian StyleInukai, Daisuke, Taichi Kan, Shunpei Yamanaka, Hiroki Okamoto, Yasushi Fujimoto, Takanori Ito, Natsuki Taniguchi, Yuuki Yamamoto, Toyonori Tsuzuki, Akiyoshi Takami, and et al. 2020. "Pathological and Virological Studies of p16-Positive Oropharyngeal Carcinoma with a Good Response to Neoadjuvant Chemotherapy" Microorganisms 8, no. 10: 1497. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms8101497