Impact of Chronic Obstructive Pulmonary Disease on Incidence, Microbiology and Outcome of Ventilator-Associated Lower Respiratory Tract Infections

 ,
,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Study Design and Population
2.2. Data Collection
2.3. Definitions
2.3.1. Chronic Obstructive Pulmonary Disease
2.3.2. Ventilator-Associated Lower Respiratory Tract Infection
2.3.3. Antibiotic Treatment and Microbiological Data
2.4. Outcomes
2.5. Statistical Analysis
3. Results
3.1. Baseline Patient Characteristics
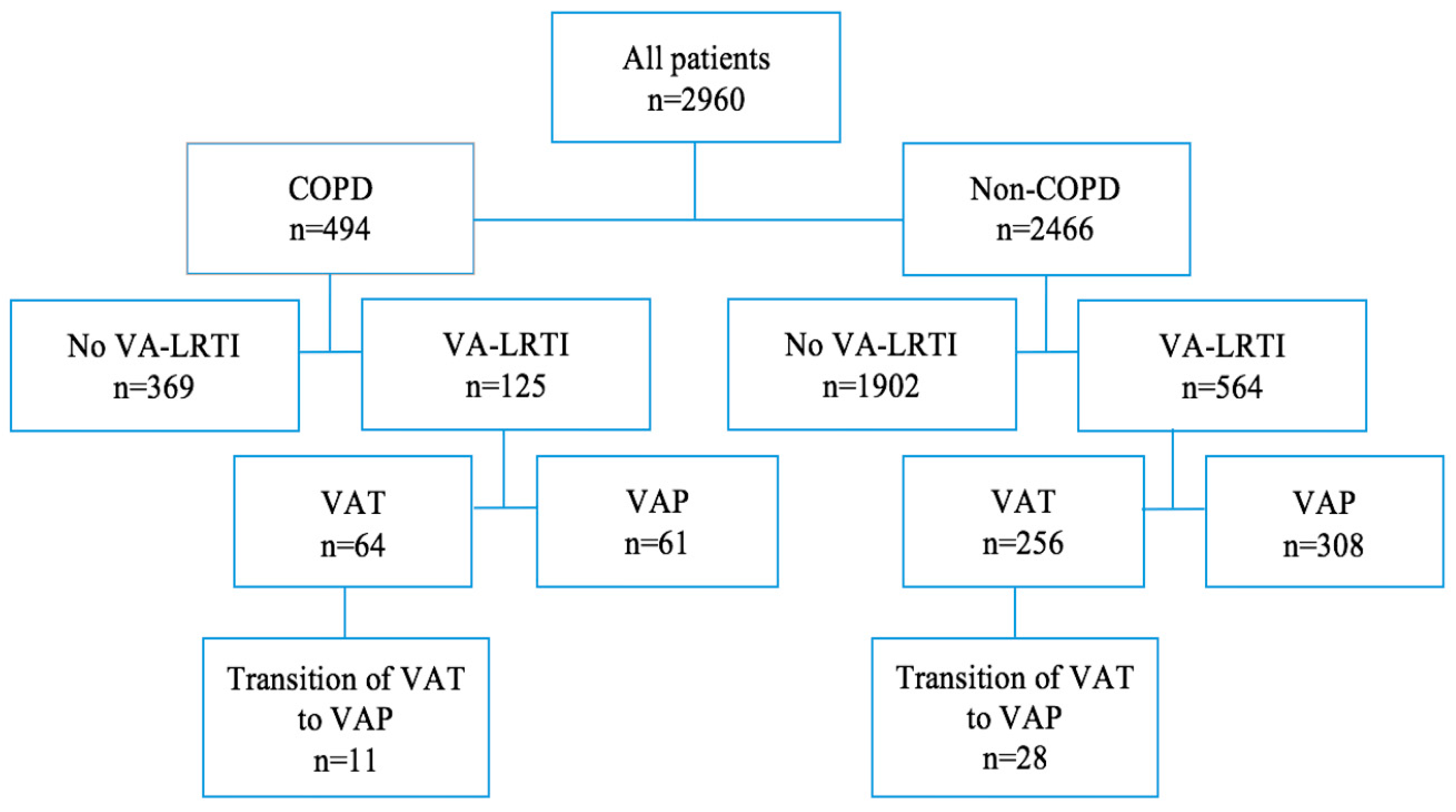
3.2. Incidence of Ventilator-Associated Lower Respiratory Tract Infections
3.3. Characteristics of Ventilator-Associated Lower Respiratory Tract Infections
3.3.1. Diagnostic Data
3.3.2. Microbiological Data
3.3.3. Impact of Antibiotic Treatment on Transition from VAT to VAP
3.4. Outcomes of Ventilator-Associated Lower Respiratory Tract Infections
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
The TAVeM Study Group Included the Following Contributors
Ethics Approval and Consent to Participate
Conflicts of Interest
Abbreviations
| COPD | chronic obstructive pulmonary disease |
| VA-LRTI | ventilator-associated lower respiratory tract infection |
| MV | mechanical ventilation |
| VAT | ventilator-associated tracheobronchitis |
| VAP | ventilator-associated pneumonia |
| ICU | intensive care unit |
| CFU | colony-forming units |
References
- Vestbo, J.; Hurd, S.S.; Agustí, A.G.; Jones, P.W.; Vogelmeier, C.; Anzueto, A.; Barnes, P.J.; Fabbri, L.M.; Martinez, F.J.; Nishimura, M.; et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease: GOLD Executive Summary. Am. J. Respir. Crit. Care Med. 2013, 187, 347–365. [Google Scholar] [CrossRef]
- World Health Organization Statistics 2008. Available online: https://www-who-int.gate2.inist.fr/gho/publications/world_health_statistics/EN_WHS08_Full.pdf?ua=1 (accessed on 13 August 2019).
- Funk, G.C.; Bauer, P.; Burghuber, O.C.; Fazekas, A.; Hartl, S.; Hochrieser, H.; Schmutz, R.; Metnitz, P. Prevalence and prognosis of COPD in critically ill patients between 1998 and 2008. Eur. Respir. J. 2013, 41, 792–799. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esteban, A.; Frutos-Vivar, F.; Muriel, A.; Ferguson, N.D.; Peñuelas, O.; Abraira, V.; Raymondos, K.; Rios, F.; Nin, N.; Apezteguía, C.; et al. Evolution of mortality over time in patients receiving mechanical ventilation. Am. J. Respir. Crit. Care Med. 2013, 188, 220–230. [Google Scholar] [CrossRef] [PubMed]
- Martin-Loeches, I.; Povoa, P.; Rodríguez, A.; Curcio, D.; Suarez, D.; Mira, J.P.; Cordero, M.L.; Lepecq, R.; Girault, C.; Candeias, C.; et al. Incidence and prognosis of ventilator-associated tracheobronchitis (TAVeM): A multicentre, prospective, observational study. Lancet Respir. Med. 2015, 3, 859–868. [Google Scholar] [CrossRef]
- Rouzé, A.; Cottereau, A.; Nseir, S. Chronic obstructive pulmonary disease and the risk for ventilator-associated pneumonia. Curr. Opin. Crit. Care 2014, 20, 525–531. [Google Scholar] [CrossRef] [PubMed]
- Torres, A.; Aznar, R.; Gatell, J.M.; Jiménez, P.; González, J.; Ferrer, A.; Celis, R.; Rodriguez-Roisin, R. Incidence, Risk, and Prognosis Factors of Nosocomial Pneumonia in Mechanically Ventilated Patients. Am. Rev. Respir. Dis. 1990, 142, 523–528. [Google Scholar] [CrossRef]
- Tejerina, E.; Frutos-Vivar, F.; Restrepo, M.I.; Anzueto, A.; Abroug, F.; Palizas, F.; González, M.; D’Empaire, G.; Apezteguía, C.; Esteban, A.; et al. Internacional Mechanical Ventilation Study Group. Incidence, risk factors, and outcome of ventilator-associated pneumonia. J. Crit. Care 2006, 21, 56–65. [Google Scholar] [CrossRef]
- Koulenti, D.; Blot, S.; Dulhunty, J.M.; Papazian, L.; Martin-Loeches, I.; Dimopoulos, G.; Brun-Buisson, C.; Nauwynck, M.; Putensen, C.; Sole-Violan, J.; et al. COPD patients with ventilator-associated pneumonia: Implications for management. Eur. J. Clin. Microbiol. Infect. Dis. 2015, 34, 2403–2411. [Google Scholar] [CrossRef]
- Melsen, W.G.; Rovers, M.M.; Groenwold, R.H.; Bergmans, D.C.; Camus, C.; Bauer, T.T.; Hanisch, E.W.; Klarin, B.; Koeman, M.; Krueger, W.A.; et al. Attributable mortality of ventilator-associated pneumonia: A meta-analysis of individual patient data from randomised prevention studies. Lancet Infect. Dis. 2013, 13, 665–671. [Google Scholar] [CrossRef]
- Nseir, S.; Di Pompeo, C.; Soubrier, S.; Cavestri, B.; Jozefowicz, E.; Saulnier, F.; Durocher, A. Impact of ventilator-associated pneumonia on outcome in patients with COPD. Chest 2005, 128, 1650–1656. [Google Scholar] [CrossRef] [Green Version]
- Bekaert, M.; Timsit, J.F.; Vansteelandt, S.; Depuydt, P.; Vésin, A.; Garrouste-Orgeas, M.; Decruyenaere, J.; Clec’h, C.; Azoulay, E.; Benoit, D. Attributable mortality of ventilator-associated pneumonia: A reappraisal using causal analysis. Am. J. Respir. Crit. Care Med. 2011, 184, 1133–1139. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez, A.; Póvoa, P.; Nseir, S.; Salluh, J.; Curcio, D.; Martín-Loeches, I. Incidence and diagnosis of ventilator-associated tracheobronchitis in the intensive care unit: An international online survey. Crit. Care 2014, 18, R32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nseir, S.; Povoa, P.; Salluh, J.; Rodriguez, A.; Martin-Loeches, I. Is there a continuum between ventilator-associated tracheobronchitis and ventilator-associated pneumonia? Intensive Care Med. 2016, 42, 1190–1192. [Google Scholar] [CrossRef] [PubMed]
- Dallas, J.; Skrupky, L.; Abebe, N.; Boyle, W.A., III; Kollef, M.H. Ventilator-associated tracheobronchitis in a mixed surgical and medical ICU population. Chest 2011, 139, 513–518. [Google Scholar] [CrossRef] [PubMed]
- Craven, D.E.; Lei, Y.; Ruthazer, R.; Sarwar, A.; Hudcova, J. Incidence and outcomes of ventilator-associated tracheobronchitis and pneumonia. Am. J. Med. 2013, 126, 542–549. [Google Scholar] [CrossRef] [PubMed]
- Nseir, S.; Di Pompeo, C.; Pronnier, P.; Beague, S.; Onimus, T.; Saulnier, F.; Grandbastien, B.; Mathieu, D.; Delvallez-Roussel, M.; Durocher, A. Nosocomial tracheobronchitis in mechanically ventilated patients: Incidence, aetiology and outcome. Eur. Respir. J. 2002, 20, 1483–1489. [Google Scholar] [CrossRef] [Green Version]
- Karvouniaris, M.; Makris, D.; Manoulakas, E.; Zygoulis, P.; Mantzarlis, K.; Triantaris, A.; Chatzi, M.; Zakynthinos, E. Ventilator-associated tracheobronchitis increases the length of intensive care unit stay. Infect. Control Hosp. Epidemiol. 2013, 34, 800–808. [Google Scholar] [CrossRef]
- Paul, M.; Shani, V.; Muchtar, E.; Kariv, G.; Robenshtok, E.; Leibovici, L. Systematic Review and Meta-Analysis of the Efficacy of Appropriate Empiric Antibiotic Therapy for Sepsis. Antimicrob. Agents Chemother. 2010, 54, 4851–4863. [Google Scholar] [CrossRef] [Green Version]
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [Green Version]
- Bouza, E.; Granda, M.J.P.; Hortal, J.; Barrio, J.M.; Cercenado, E.; Muñoz, P. Pre-emptive broad-spectrum treatment for ventilator-associated pneumonia in high-risk patients. Intensive Care Med. 2013, 39, 1547–1555. [Google Scholar] [CrossRef]
- Nair, G.B.; Niederman, M.S. Ventilator-associated pneumonia: Present understanding and ongoing debates. Intensive Care Med. 2014, 41, 34–48. [Google Scholar] [CrossRef] [PubMed]
- Upchurch, C.P.; Grijalva, C.G.; Wunderink, R.G.; Williams, D.J.; Waterer, G.W.; Anderson, E.J.; Zhu, Y.; Hart, E.M.; Carroll, F.; Bramley, A.M.; et al. Community-acquired Pneumonia Visualized on Computed Tomography but Not Chest X-Ray: Pathogens, Severity, and Clinical Outcomes. Chest 2018, 153, 601–610. [Google Scholar] [CrossRef] [PubMed]
- Bouhemad, B.; Dransart-Rayé, O.; Mojoli, F.; Mongodi, S. Lung ultrasound for diagnosis and monitoring of ventilator-associated pneumonia. Ann. Transl. Med. 2018, 6, 418. [Google Scholar] [CrossRef] [PubMed]
- Parmentier-Decrucq, E.; Poissy, J.; Favory, R.; Nseir, S.; Onimus, T.; Guerry, M.J.; Durocher, A.; Mathieu, D. Adverse events during intrahospital transport of critically ill patients: Incidence and risk factors. Ann. Intensive Care 2013, 3, 10. [Google Scholar] [CrossRef] [Green Version]
- Makris, D.; Desrousseaux, B.; Zakynthinos, E.; Durocher, A.; Nseir, S. The impact of COPD on ICU mortality in patients with ventilator-associated pneumonia. Respir Med. 2011, 105, 1022–1029. [Google Scholar] [CrossRef] [Green Version]
- Nseir, S.; Di Pompeo, C.; Cavestri, B.; Jozefowicz, E.; Nyunga, M.; Soubrier, S.; Roussel-Delvallez, M.; Saulnier, F.; Mathieu, D.; Durocher, A. Multiple-drug-resistant bacteria in patients with severe acute exacerbation of chronic obstructive pulmonary disease: Prevalence, risk factors, and outcome. Crit. Care Med. 2006, 34, 2959–2966. [Google Scholar] [CrossRef]
- Nseir, S.; Di Pompeo, C.; Brisson, H.; Dewavrin, F.; Tissier, S.; Diarra, M.; Boulo, M.; Durocher, A. Intensive care unit-acquired Stenotrophomonas maltophilia: Incidence, risk factors, and outcome. Crit. Care 2006, 10, R143. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez, A.; Lisboa, T.; Solé-Violán, J.; Gómez, F.; Roca, O.; Trefler, S.; Gea, J.; Masclans, J.R.; Rello, J. Impact of nonexacerbated COPD on mortality in critically ill patients. Chest 2011, 139, 1354–1360. [Google Scholar] [CrossRef]


{kind=link}
| COPD n = 494 | No COPD n = 2466 | p | |
|---|---|---|---|
| Age, years | 68 (60–76) | 63 (49–74) | <0.001 |
| Male gender | 355 (72) | 1494 (61) | <0.001 |
| Severity scores | |||
| SAPS II | 50 (39–62) | 50 (37–63) | 0.27 |
| SOFA score | 8 (5–10) | 8 (5–11) | 0.29 |
| Comorbidities | |||
| Diabetes mellitus | 126 (26) | 442 (18) | <0.001 |
| Chronic respiratory failure | 187 (38) | 99 (4) | <0.001 |
| Chronic heart failure | 36 (7) | 176 (7) | 0.91 |
| Chronic kidney disease | 76 (15) | 217 (9) | <0.001 |
| Cirrhosis | 25 (5) | 152 (6) | 0.35 |
| Immunosuppression | 113 (23) | 549 (22) | 0.77 |
| Alcohol abuse | 84 (17) | 274 (11) | <0.001 |
| Intravenous drug abuse | 10 (2) | 43 (2) | 0.67 |
| Category of admission | <0.001 | ||
| Medical | 392 (79) | 1496 (61) | |
| Surgical | 68 (14) | 476 (19) | |
| Trauma | 34 (7) | 494 (20) | |
| Main causes for ICU admission | |||
| Shock | 33 (7) | 238 (10) | 0.037 |
| Sepsis | 54 (11) | 284 (12) | 0.71 |
| Acute respiratory distress syndrome | 23 (5) | 124 (5) | 0.73 |
| Pneumonia | 110 (22) | 308 (12) | <0.001 |
| Aspiration | 5 (1) | 44 (2) | 0.22 |
| Congestive heart failure | 20 (4) | 76 (3) | 0.27 |
| Myocardial infarction | 12 (2) | 57 (2) | 0.87 |
| Arrhythmia | 6 (1) | 28 (1) | 0.88 |
| Coma | 26 (5) | 248 (10) | <0.001 |
| Stroke | 6 (1) | 115 (5) | <0.001 |
| Seizure | 5 (1) | 66 (3) | 0.027 |
| Brain aneurysm | 5 (1) | 37 (2) | 0.40 |
| Traumatic brain injury | 6 (1) | 153 (6) | <0.001 |
| Acute renal failure | 9 (2) | 36 (1) | 0.55 |
| COPD n = 125 | No COPD N = 564 | |||||
|---|---|---|---|---|---|---|
| VAT n = 64 | VAP n = 61 | p | VAT n = 256 | VAP n = 308 | p | |
| CRP | 69 (9–201) | 129 (17–230) | 0.374 | 126 (51–211) | 120 (30–239) | 0.78 |
| PCT | 0.1 (0.0–1.7) | 0.8 (0.0–3.8) | 0.219 | 0.1 (0.0–1.0) | 0.4 (0.0–5.0) | <0.001 |
| CPIS | 5 (3–6) | 6 (5–8) | <0.001 | 4 (3–6) | 7 (5–8) | <0.001 |
| Endotracheal aspirate | 52 (81) | 41 (67) | 0.072 | 226 (88) | 212 (69) | <0.001 |
| Bronchoscopy | 7 (11) * | 15 (25) * | 0.045 | 10 (4) | 41 (13) | <0.001 |
| Bronchoalveolar lavage | 6 (9) ** | 15 (25) ** | 0.023 | 6 (2) | 44 (14) | <0.001 |
| Mini bronchoalveolar lavage | 5 (8) | 4 (7) | 0.786 | 11 (4) | 41 (13) | <0.001 |
| Blind protected specimen brush | 8 (13) | 12 (20) | 0.274 | 24 (9) | 39 (13) | 0.22 |
| COPD n = 125 | No COPD n = 564 | p | |
|---|---|---|---|
| Polymicrobial | 33 (26) | 132 (23) | 0.48 |
| Multidrug-resistant isolates | 75 (60) | 346 (62) | 0.71 |
| Gram-negative bacilli | |||
| Pseudomonas aeruginosa | 32 (26) | 136 (24) | 0.73 |
| Escherichia coli | 23 (18) | 54 (10) | 0.005 |
| Klebsiella pneumoniae | 15 (12) | 86 (15) | 0.35 |
| Enterobacter spp. | 15 (12) | 66 (12) | 0.93 |
| Stenotrophomonas maltophilia | 11 (9) | 20 (4) | 0.010 |
| Haemophilus influenzae | 7 (6) | 50 (9) | 0.23 |
| Proteus mirabilis | 7 (6) | 22 (4) | 0.39 |
| Serratia marcescens | 5 (4) | 23 (4) | 0.97 |
| Acinetobacter baumannii | 4 (3) | 37 (7) | 0.15 |
| Citrobacter freundii | 3 (2) | 10 (2) | 0.71 |
| Gram-positive cocci | |||
| MSSA | 21 (17) | 125 (22) | 0.18 |
| MRSA | 4 (3) | 12 (2) | 0.51 |
| Streptococcus pneumoniae | 8 (6) | 32 (6) | 0.75 |
| COPD n = 64 | No COPD n = 256 | |||||
|---|---|---|---|---|---|---|
| VAT to VAP Progression n = 11 | No VAT to VAP Progression n = 53 | p | VAT to VAP Progression n = 28 | No VAT to VAP Progression n = 228 | p | |
| Antibiotic treatment | 10 (91) | 50 (94) | 0.539 | 21 (75) | 213 (93) | 0.005 |
| Appropriate antibiotic treatment | 6 (55) | 42 (79) | 0.124 | 13 (46) | 189 (83) | <0.001 |
| Length of antibiotic treatment, days | 7 (3–8) | 7 (4–10) | 0.591 | 6 (4–10) | 7 (4–10) | 0.99 |
| COPD n = 494 | No COPD n = 2466 | |||||||
|---|---|---|---|---|---|---|---|---|
| VAT n = 64 | VAP n = 61 | No VA-LRTI n = 369 | p | VAT n = 256 | VAP n = 308 | No VA-LRTI n = 1902 | p | |
| MV duration, days | 17(9–30) | 15(8–27) | 7(4–12) | <0.001 | 13(8–21) | 15(8–26) | 7(4–13) | <0.001 |
| ICU length of stay, days | 24(17–39) | 21(14–40) | 12(8–19) | <0.001 | 20(14–31) | 21(13–33) | 12(8–19) | <0.001 |
| Hospital length of stay, days | 42(22–59) | 30(18–56) | 23(14–38) | <0.001 | 36(21–54) | 31(20–54) | 23(14–41) | <0.001 |
| ICU mortality | 24 (38) $ | 27 (44) | 95 (26) * | 0.006 | 68 (27) £ | 116 (38) | 565 (30) | <0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rouzé, A.; Boddaert, P.; Martin-Loeches, I.; Povoa, P.; Rodriguez, A.; Ramdane, N.; Salluh, J.; Houard, M.; Nseir, S. Impact of Chronic Obstructive Pulmonary Disease on Incidence, Microbiology and Outcome of Ventilator-Associated Lower Respiratory Tract Infections. Microorganisms 2020, 8, 165. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms8020165
Rouzé A, Boddaert P, Martin-Loeches I, Povoa P, Rodriguez A, Ramdane N, Salluh J, Houard M, Nseir S. Impact of Chronic Obstructive Pulmonary Disease on Incidence, Microbiology and Outcome of Ventilator-Associated Lower Respiratory Tract Infections. Microorganisms. 2020; 8(2):165. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms8020165
Chicago/Turabian StyleRouzé, Anahita, Pauline Boddaert, Ignacio Martin-Loeches, Pedro Povoa, Alejandro Rodriguez, Nassima Ramdane, Jorge Salluh, Marion Houard, and Saad Nseir. 2020. "Impact of Chronic Obstructive Pulmonary Disease on Incidence, Microbiology and Outcome of Ventilator-Associated Lower Respiratory Tract Infections" Microorganisms 8, no. 2: 165. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms8020165