SARS-CoV-2 Virologic and Immunologic Correlates in Patients with Olfactory and Taste Disorders

 , and
, and
Abstract
:1. Introduction
2. Patients and Methods
2.1. Demographic and Clinical Characteristics of Enrolled Patients Reporting Olfactory and Taste Disorders
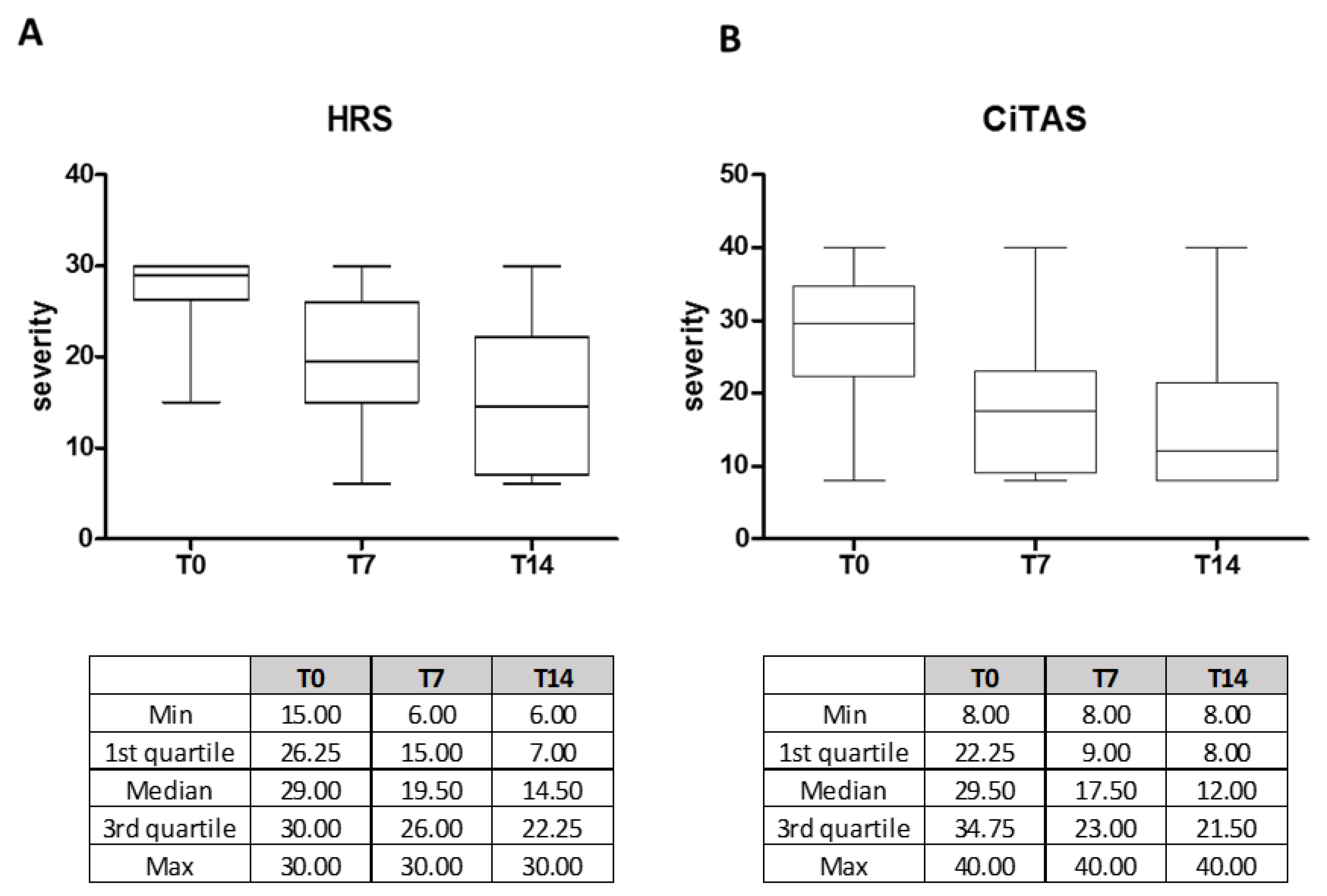
2.2. OTD Severity was Defined According to Hyposmia Rating Scale (HRS) and Chemotherapy Induced Taste Alteration Scale (CiTAS)
2.3. Sequential Samples’ Collection and Molecular Laboratory Testing
2.4. Serum Samples Collection and Serological Laboratory Testings
2.5. Statistical Analysis
3. Results
3.1. Analysis of Demographic and Clinical Characteristics of 69 OTDs Patients and SARS-CoV-2 Prevalence
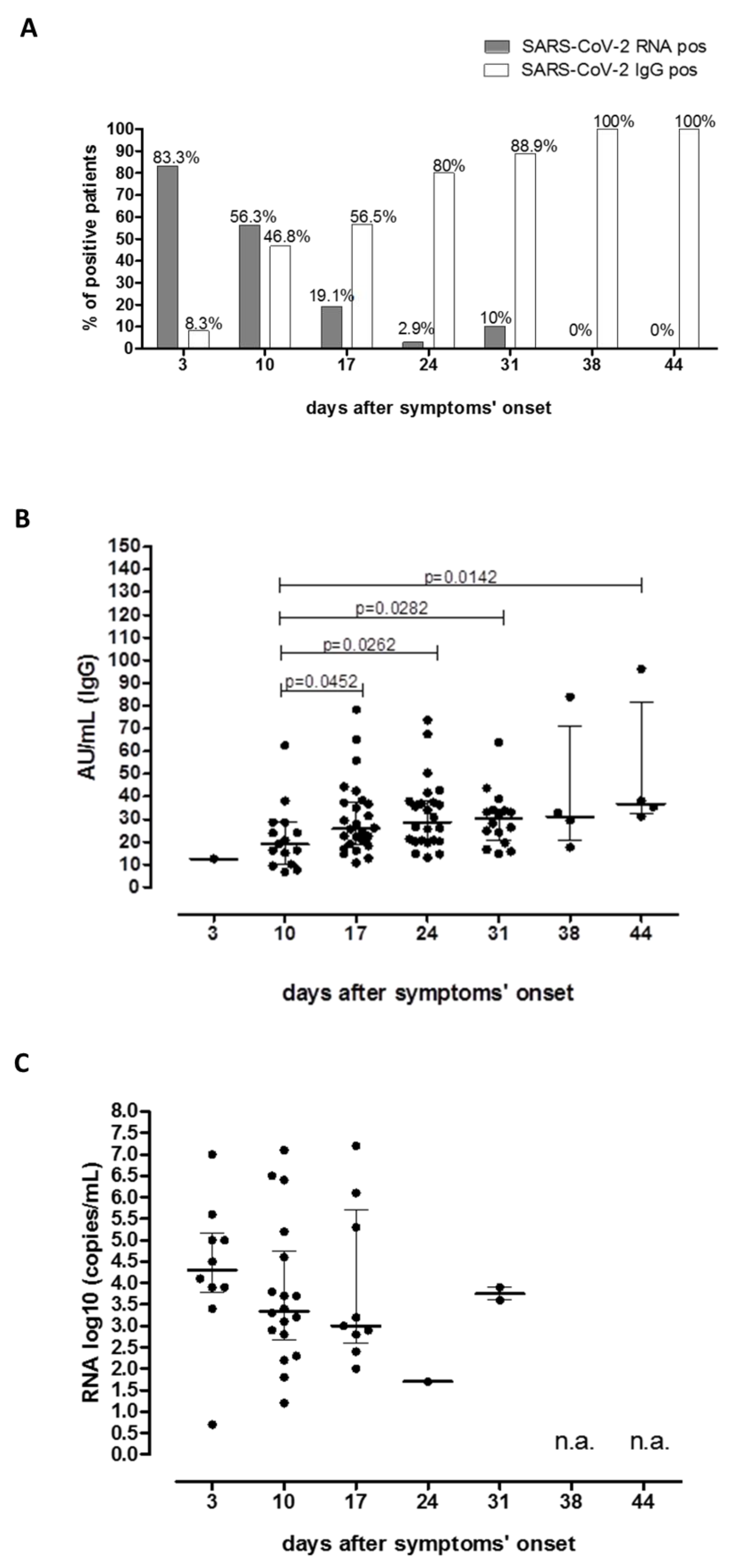
3.2. SARS-CoV-2 RNA and SARS-CoV-2 IgG Trend in 52 COVID-19 Patients Analyzed at Different Time Points
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Su, S.; Wong, G.; Shi, W.; Liu, J.; Lai, A.C.K.; Zhou, J.; Liu, W.; Bi, Y.; Gao, G.F. Epidemiology, Genetic Recombination, and Pathogenesis of Coronaviruses. Trends Microbiol. 2016, 24, 490–502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhong, N.S.; Zheng, B.J.; Li Poe, Y.M.; Xie, Z.H.; Chan, K.H.; Li, P.H.; Tan, S.Y.; Chang, Q.; Xie, J.P.; Liu, X.Q.; et al. Epidemiology and cause of severe acute respiratory syndrome (SARS) in Guangdong, People’s Republic of China, in February, 2003. Lancet 2020, 362, 1353–1358. [Google Scholar] [CrossRef] [Green Version]
- Zaki, A.M.; van Boheemen, S.; Bestebroer, T.M.; Osterhaus, A.D.; Fouchier, R.A. Isolation of a novel coronavirus from a man with pneumonia in Saudi Arabia. N. Engl. J. Med. 2012, 367, 1814–1820. [Google Scholar] [CrossRef]
- Wu, D.; Wu, T.; Liu, Q.; Yang, Z. The SARS-CoV-2 Outbreak: What We Know. Int. J. Infect. Dis. 2020, 94, 44–48. [Google Scholar] [CrossRef]
- Cui, J.; Li, F.; Shi, Z.L. Origin and evolution of pathogenic coronaviruses. Nat. Rev. Microbiol. 2019, 17, 181–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. China Novel Coronavirus Investigating and Research Team. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Livingston, E.; Bucher, K. Coronavirus Disease 2019 (COVID-19) in Italy. JAMA 2020. [Google Scholar] [CrossRef] [Green Version]
- Guo, Y.R.; Cao, Q.D.; Hong, Z.S.; Tan, Y.Y.; Chen, S.D.; Jin, H.J.; Tan, K.S.; Wang, D.Y.; Yan, Y. The Origin, Transmission and Clinical Therapies on Coronavirus Disease 2019 (COVID-19) Outbreak—An Update on the Status. Mil. Med. Res. 2020, 7, 11. [Google Scholar] [CrossRef] [Green Version]
- Vaira, L.A.; Salzano, G.; Deiana, G.; De Riu, G. Anosmia and ageusia: Common findings in COVID-19 patients. Laryngoscope 2020, 130, 1787. [Google Scholar] [CrossRef] [Green Version]
- Giacomelli, A.; Pezzati, L.; Conti, F.; Bernacchia, D.; Siano, M.; Oreni, L.; Rusconi, S.; Gervasoni, C.; Ridolfo, A.L.; Rizzardini, G.; et al. Self-reported olfactory and taste disorders in SARS-CoV-2 patients: A cross-sectional study. Clin. Infect. Dis. 2020, ciaa330. [Google Scholar] [CrossRef] [Green Version]
- Spinato, G.; Fabbris, C.; Polesel, J.; Cazzador, D.; Borsetto, D.; Hopkins, C.; Boscolo-Rizzo, P. Alterations in smell or taste in mildly symptomatic outpatients with SARS-CoV-2 infection. JAMA 2020, 323, 2089–2090. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention. Coronavirus Disease 2019 (COVID-19)—Symptoms. 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/symptoms.html (accessed on 22 April 2020).
- Chi-Shin Hwang, C.S. Olfactory Neuropathy in Severe Acute Respiratory Syndrome: Report of A Case. Acta Neurol. Taiwan 2006, 15, 26–28. [Google Scholar]
- Suzuki, M.; Saito, K.; Min, W.P.; Vladau, C.; Toida, K.; Itoh, H.; Murakami, S. Identification of Viruses in Patients with Postviral Olfactory Dysfunction. Laryngoscope 2007, 117, 272–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamagishi, M.; Fujiwara, M.; Nakamura, H. Olfactory mucosal findings and clinical course in patients with olfactory disorders following upper respiratory viral infection. Rhinology 1994, 32, 113–118. [Google Scholar] [PubMed]
- Netland, J.; Meyerholz, D.K.; Moore, S.; Cassell, M.; Perlman, S. Severe acute respiratory syndrome coronavirus infection causes neuronal death in the absence of encephalitis in mice transgenic for human ACE2. J. Virol. 2008, 82, 7264–7275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, H.; Zhong, L.; Deng, J.; Peng, J.; Dan, H.; Zeng, X.; Li, T.; Chen, Q. High expression of ACE2 receptor of 2019-nCoV on the epithelial cells of oral mucosa. Int. J. Oral. Sci. 2020, 12, 8. [Google Scholar] [CrossRef] [PubMed]
- Millar Vernetti, P.; Perez Lloret, S.; Rossi, M.; Cerquetti, D.; Merello, M. Validation of a new scale to assess olfactory dysfunction in patients with Parkinson’s disease. Parkinsonism Relat. Disord. 2012, 18, 358–361. [Google Scholar] [CrossRef]
- Campagna, S.; Gonella, S.; Stuardi, M.; Sperlinga, R.; Cerponi, M.; Olivero, M.; Giuliano, P.L.; Marchese, R.; Carnovali, E.; Pedersini, R.; et al. Validazione italiana della Chemotherapy induced Taste Alteration Scale (CiTAS) [Italian validation of the Chemotherapy Induced Taste Alteration Scale]. Assist. Inferm. Ric. 2016, 35, 22–28. [Google Scholar] [CrossRef]
- WHO. Novel Coronavirus—China. Available online: http://wwwwhoint/csr/don/12-january-2020-novel-coronavirus-china/en/ (accessed on 19 January 2020).
- Corman, V.M.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.K.; Bleicker, T.; Brünink, S.; Schneider, J.; Schmidt, M.L.; et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. EuroSurveill 2020, 25, 2000045. [Google Scholar] [CrossRef] [Green Version]
- Conti, P.; Younes, a. Coronavirus COV-19/SARS-CoV-2 Affects Women Less Than Men: Clinical Response to Viral Infection. J. Biol. Regul. Homeost. Agents 2020, 34. [Google Scholar] [CrossRef]
- Falahi, S.; Azra Kenarkoohi, A. Sex and Gender Differences in the Outcome of Patients With COVID-19. J. Med. Virol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Ragab, D.; Salah Eldin, H.S.; Taeimah, M.; Khattab, R.; Salem, R. The COVID-19 Cytokine Storm; What We Know So Far. Front. Immunol. 2020, 11, 1446. [Google Scholar] [CrossRef] [PubMed]
- Conti, P.; Gallenga, C.E.; Tetè, G.; Caraffa, A.; Ronconi, G.; Younes, A.; Toniato, E.; Ross, R.; Kritas, S.K. How to reduce the likelihood of coronavirus-19 (CoV-19 or SARS-CoV-2) infection and lung inflammation mediated by IL-1. J. Biol. Regul. Homeost. Agents 2020, 34. [Google Scholar] [CrossRef]
- Conti, P.; Ronconi, G.; Caraffa, A.; Gallenga, C.; Ross, R.; Frydas, I.; Kritas, S. Induction of Pro-Inflammatory Cytokines (IL-1 and IL-6) and Lung Inflammation by Coronavirus-19 (COVI-19 or SARS-CoV-2): Anti-Inflammatory Strategies. J. Biol. Regul. Homeost. Agents 2020, 34, 1. [Google Scholar] [CrossRef]
- Rovida, F.; Cereda, D.; Novati, S.; Licari, A.; Triarico, A.; Marseglia, G.L.; Bruno, R.; Baldanti, F. San Matteo Pavia COVID-19 Task Force Low Risk for SARS-CoV2 Symptomatic Infection and Early Complications in Paediatric Patients During the Ongoing CoVID19 Epidemics in Lombardy. Clin. Microbiol. Infect. 2020. [Google Scholar] [CrossRef] [PubMed]
- Ong, J.S.M.; Tosoni, A.; Kim, Y.; Kissoon, N.; Murthy, S. Coronavirus Disease 2019 in Critically Ill Children: A Narrative Review of the Literature. Pediatr. Crit. Care Med. 2020, 21, 662–666. [Google Scholar] [CrossRef]
- Verdoni, L.; Mazza, A.; Gervasoni, A.; Martelli, L.; Ruggeri, M.; Ciuffreda, M.; Bonanomi, E.; D’Antiga, L. An Outbreak of Severe Kawasaki-like Disease at the Italian Epicentre of the SARS-CoV-2 Epidemic: An Observational Cohort Study. Lancet 2020, 395, 1771–1778. [Google Scholar] [CrossRef]
- Riphagen, S.; Gomez, X.; Gonzalez-Martinez, C.; Wilkinson, N.; Theocharis, P. Hyperinflammatory shock in children during COVID-19 pandemic. Lancet 2020, 23. [Google Scholar] [CrossRef]
- Viner, R.M.; Whittaker, E. Kawasaki-like disease: Emerging complication during the COVID-19 pandemic. Lancet 2020, 395, 1741–1743. [Google Scholar] [CrossRef]
- Ronconi, G.; Teté, G.; Kritas, S.K.; Gallenga, C.E.; Caraffa, A.; Ross, R.; Conti, P. SARS-CoV-2, which induces COVID-19, causes kawasaki-like disease in children: Role of pro-inflammatory and anti-inflammatory cytokines. J. Biol. Regul. Homeost. Agents 2020, 34, Online. [Google Scholar] [CrossRef]
- Rowley, A.H. Is Kawasaki Disease an Infectious Disorder? Int. J. Rheum. Dis. 2018, 21, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Magro, G. COVID-19: Review on Latest Available Drugs and Therapies Against SARS-CoV-2. Coagulation and Inflammation Cross-Talking. Virus Res. 2020, 286, 198070. [Google Scholar] [CrossRef] [PubMed]
- Theoharides, T.C.; Conti, P. Dexamethasone for COVID-19? Not so fast. J. Biol. Regul. Homeost. Agents. 2020, 34. [Google Scholar] [CrossRef]
- Russell, C.D.; Millar, J.E.; Baillie, J.K. Clinical evidence does not support corticosteroid treatment for 2019-nCoV lung injury. Lancet 2020, 395, 473–475. [Google Scholar] [CrossRef] [Green Version]
- RECOVERY Trial. 2020. Available online: https://www.recoverytrial.net/results (accessed on 19 January 2020).
- Lechien, J.R.; Chiesa-Estomba, C.M.; De Siati, D.R.; Horoi, M.; Le Bon, S.D.; Rodriguez, A.; Dequanter, D.; Blecic, S.; El Afia, F.; Distinguin, L.; et al. Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): A multicenter European study. Eur. Arch. Otorhinolaryngol. 2020, 277, 2251–2261. [Google Scholar] [CrossRef]
- Soler, Z.M.; Patel, Z.M.; Turner, J.H.; Holbrook, E.H. A primer on viral-associated olfactory loss in the era of COVID-19. Int. Forum Allergy Rhinol. 2020, 10, 814–820. [Google Scholar] [CrossRef]
- Vaira, L.A.; Hopkins, C.; Salzano, G.; Petrocelli, M.; Melis, A.; Cucurullo, M.; Ferrari, M.; Gagliardini, L.; Pipolo, C.; Deiana, G. Olfactory and gustatory function impairment in COVID-19 patients: Italian objective multicenter-study. Head Neck 2020. [Google Scholar] [CrossRef]
- Tong, J.Y.; Wong, A.; Zhu, D.; Fastenberg, J.H.; Tham, T. The Prevalence of Olfactory and Gustatory Dysfunction in COVID-19 Patients: A Systematic Review and Meta-analysis. Otolaryngol. Head Neck Surg. 2020, 163, 3–11. [Google Scholar] [CrossRef]
- Beltrán-Corbellini, Á.; Chico-García, J.L.; Martínez-Poles, J.; Rodríguez-Jorge, F.; Alonso-Cánovas, A. Acute-onset smell and taste disorders in the context of Covid-19: A pilot multicenter PCR-based case-control study. Eur. J. Neurol. 2020. [Google Scholar] [CrossRef]
- Xydakis, M.S.; Dehgani-Mobaraki, P.; Holbrook, E.H.; Geisthoff, U.W.; Bauer, C.; Hautefort, C.; Herman, P.; Manley, G.T.; Lyon, D.M.; Hopkins, C. Smell and taste dysfunction in patients with COVID-19. Lancet Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Wee, L.E.; Chan, Y.F.Z.; Teo, N.W.Y.; Cherng, B.P.Z.; Thien, S.T.; Won, H.M.; Wijaya, L.; Toh, S.T.; Tan, T.T. The role of self-reported olfactory and gustatory dysfunction as a screening criterion for suspected COVID-19. Eur. Arch. Otorhinolaryngol. 2020, 277, 2389–2390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lechien, J.R.; Hopkins, C.; Saussez, S. Sniffing out the evidence; It’s now time for public health bodies recognize the link between COVID-19 and smell and taste disturbance. Rhinology 2020. [Google Scholar] [CrossRef]
- Zhao, J.; Yuan, Q.; Wang, H.; Liu, W.; Liao, X.; Su, Y.; Wang, X.; Yuan, J.; Li, T.; Li, J.; et al. Antibody responses to SARS-CoV-2 in patients of novel coronavirus disease 2019. Clin. Infect. Dis. 2020, ciaa344. [Google Scholar] [CrossRef]
- Percivalle, E.; Cambiè, G.; Cassaniti, I.; Vecchio Nepita, E.; Maserati, R.; Ferrari, A.; Di Martino, R.; Isernia, P.; Mojoli, F.; Bruno, R. Prevalence of SARS-CoV-2 specific neutralising antibodies in blood donors from the Lodi Red Zone in Lombardy, Italy, as at 06 April 2020. EuroSurveill 2020, 25, 2001031. [Google Scholar] [CrossRef] [PubMed]
- de Haro-Licer, J.; Roura-Moreno, J.; Vizitiu, A.; González-Fernández, A.; González-Ares, J.A. Long term serious olfactory loss in colds and/or flu. Acta Otorrinolaringol. Esp. 2013, 64, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Hummel, T.; Landis, B.N.; Hüttenbrink, K.B. Smell and taste disorders. GMS Curr. Top. Otorhinolaryngol. Head Neck Surg. 2011, 10, Doc04. [Google Scholar] [CrossRef] [PubMed]
- van Riel, D.; Verdijk, R.; Kuiken, T. The olfactory nerve: A shortcut for influenza and other viral diseases into the central nervous system. J. Pathol. 2015, 235, 277–287. [Google Scholar] [CrossRef]
- Deems, D.A.; Doty, R.L.; Settle, R.G.; Moore-Gillon, V.; Shaman, P.; Mester, A.F.; Kimmelman, C.P.; Brightman, V.J.; Snow, J.B., Jr. Smell and Taste Disorders, a Study of 750 Patients From the University of Pennsylvania Smell and Taste Center. Arch. Otolaryngol. Head Neck Surg. 1991, 117, 519–528. [Google Scholar] [CrossRef] [PubMed]
- Pellegrino, R.; Walliczek-Dworschak, U.; Winter, G.; Hull, D.; Hummel, T. Investigation of chemosensitivity during and after an acute cold. Int. Forum Allergy Rhinol. 2017, 7, 185–191. [Google Scholar] [CrossRef]
- Lou, B.; Li, T.D.; Zheng, S.F.; Su, Y.Y.; Li, Z.Y.; Liu, W.; Yu, F.; Ge, S.X.; Zou, Q.D.; Yuan, Q.; et al. Serology characteristics of SARS-CoV-2 infection since exposure and post symptom onset. Eur. Respir. J. 2020, 2000763. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Patients | N = 52 | |
|---|---|---|
| Age (median range) | 41 (19–58) | |
| Female | 29 | 55.8% |
| Smoking | ||
| Never | 36 | 69.2% |
| Previous smoker | 7 | 13.5% |
| Active smoker | 9 | 17.3% |
| Comorbidities | ||
| None | 38 | 73.1% |
| Hypertension | 4 | 7.7% |
| Cardiovascular | 1 | 1.9% |
| Neoplastic | 1 (parotid adenoma) | 1.9% |
| Hormonal | 1 (Hashimoto’s disease) | 1.9% |
| Other (diverticulosis, psoriasis, etc.) | 7 | 13.5% |
| Allergy | 10 | 19.2% |
| Sleep-related breathing disorders | ||
| Snoring | 5 | 9.6% |
| None | 47 | 90.4% |
| Seasonal influenza vaccination | 7 | 13.5% |
| Travel in risky areas for COVID-19 | 0 | 0 |
| Contact with COVID-19 patients | 18 | 34.6% |
| Sinonasal sign and symptoms | ||
| Nasal obstruction | 12 | 23.1% |
| Rhinorrhea | 12 | 23.1% |
| Epistaxis | 0 | 0 |
| Cacosmia | 3 | 5.8% |
| Olfactory disorder only | ||
| Anosmia | 4 | 7.7% |
| Hyposmia | 0 | 0 |
| Taste disorder only | 0 | 0 |
| Combined perceptive disorder | ||
| Anosmia and ageusia | 38 | 73.1% |
| Anosmia and hypogeusia | 5 | 9.6% |
| Hyposmia and ageusia | 0 | 0 |
| Hyposmia and hypogeusia | 5 | 9.6% |
| COVID-19 symptoms | ||
| OTDs only | 11 | 21.2% |
| Contemporary onset of OTDs and flu-like symptoms (fever, cough, asthenia, diarrhea) | 11 | 21.2% |
| OTDs before flu-like symptoms | 3 | 5.8% |
| OTDs after flu-like symptoms | 27 | 51.8% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Benazzo, M.; Cassaniti, I.; Maiorano, E.; Calastri, A.; Novazzi, F.; Bonetti, A.; Sarasini, A.; Bruno, R.; Baldanti, F. SARS-CoV-2 Virologic and Immunologic Correlates in Patients with Olfactory and Taste Disorders. Microorganisms 2020, 8, 1052. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms8071052
Benazzo M, Cassaniti I, Maiorano E, Calastri A, Novazzi F, Bonetti A, Sarasini A, Bruno R, Baldanti F. SARS-CoV-2 Virologic and Immunologic Correlates in Patients with Olfactory and Taste Disorders. Microorganisms. 2020; 8(7):1052. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms8071052
Chicago/Turabian StyleBenazzo, Marco, Irene Cassaniti, Eugenia Maiorano, Anna Calastri, Federica Novazzi, Alice Bonetti, Antonella Sarasini, Raffaele Bruno, and Fausto Baldanti. 2020. "SARS-CoV-2 Virologic and Immunologic Correlates in Patients with Olfactory and Taste Disorders" Microorganisms 8, no. 7: 1052. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms8071052