
Treatment of Multidrug-Resistant and Extensively Drug-Resistant Tuberculosis in Children: The Role of Bedaquiline and Delamanid


Abstract
:1. Introduction
2. Management of MDR-TB in Pediatrics
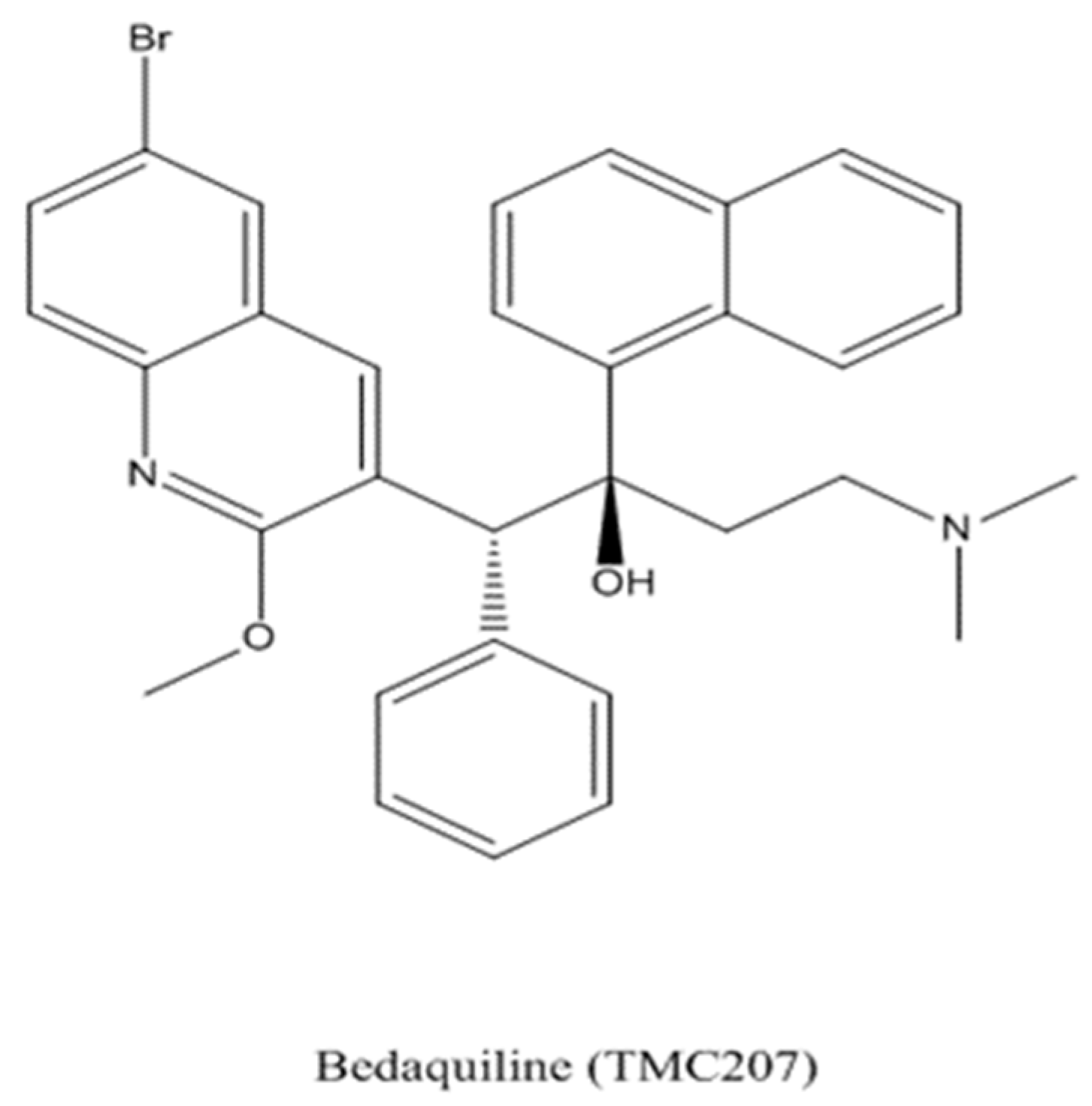
3. Bedaquiline
3.1. Mechanism of Action and Pharmacokinetics
3.2. Efficacy
3.3. Safety and Tolerability
3.4. Drug Interactions
3.5. Bedaquiline Treatment in the Pediatric Population
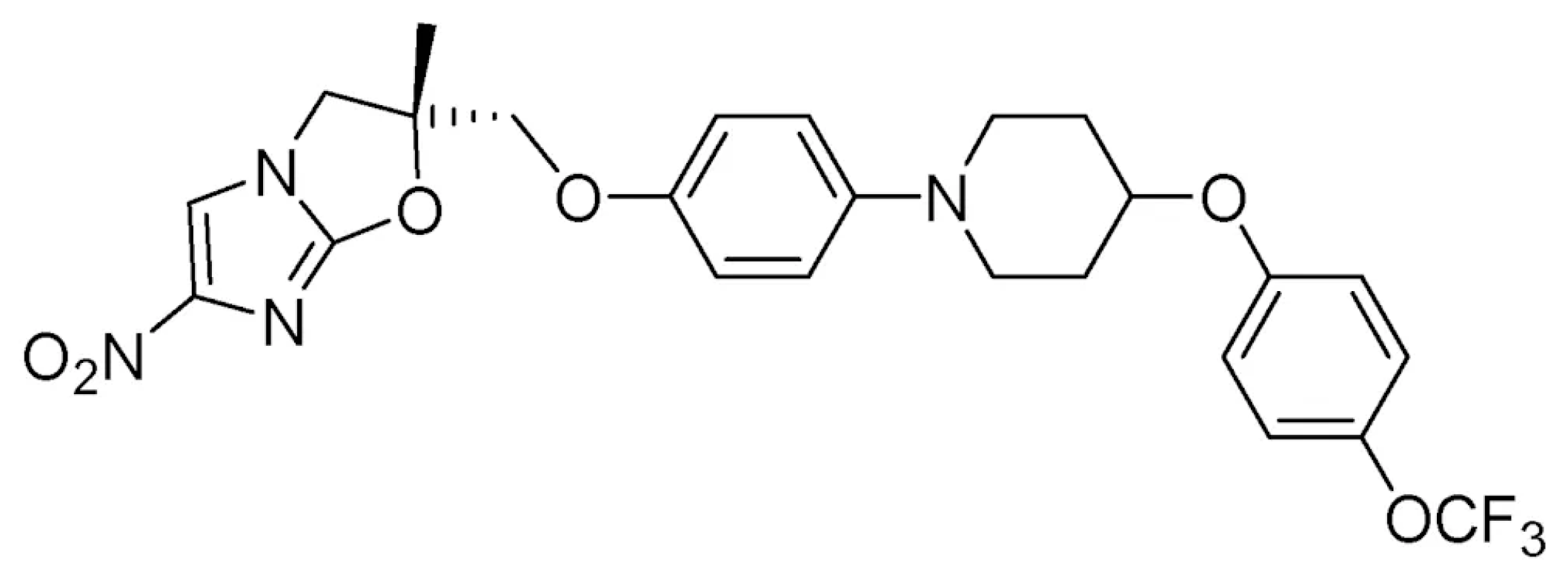
4. Delamanid
4.1. Mechanism of Action and Pharmacokinetics
4.2. Efficacy
4.3. Safety and Tolerability
4.4. Drug Interactions
4.5. Delamanid Treatment in the Pediatric Population
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Phillips, L. Infectious disease: TB’s revenge. Nature 2013, 493, 14–16. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Tuberculosis Report 2019. World Health Organization. 2019. Available online: https://apps.who.int/iris/handle/10665/329368 (accessed on 1 May 2021).
- Hesseling, A.C.; Cotton, M.F.; Jennings, T.; Whitelaw, A.; Johnson, L.F.; Eley, B.; Roux, P.; Godfrey-Faussett, P.; Schaaf, H.S. High incidence of tuberculosis among HIV-infected infants: Evidence from a South African population-based study highlights the need for improved tuberculosis control strategies. Clin. Infect. Dis. 2009, 48, 108–114. [Google Scholar] [CrossRef]
- Schaaf, H.S.; Marais, B.J.; Whitelaw, A.; Hesseling, A.C.; Eley, B.; Hussey, G.D.; Donald, P.R. Culture-confirmed childhood tuberculosis in Cape Town, South Africa: A review of 596 cases. BMC Infect. Dis. 2007, 7, 140. [Google Scholar] [CrossRef]
- World Health Organization. Rapid Communication: Key Changes to Treatment of Drug-Resistant Tuberculosis; (WHO/CDS/TB/2019.26); World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Schaaf, H.S.; Marais, B.J.; Hesseling, A.C.; Brittle, W.; Donald, P.R. Surveillance of antituberculosis drug resistance among children from the Western Cape Province of South Africa—An upward trend. Am. J. Public Health 2009, 99, 1486–1490. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, H.E.; Yuen, C.M. The burden of multidrug-resistant tuberculosis in children. Int. J. Tuberc. Lung Dis. 2018, 22, 3–6. [Google Scholar] [CrossRef] [PubMed]
- Dodd, P.J.; Sismanidis, C.; Seddon, J.A. Global burden of drug-resistant tuberculosis in children: A mathematical modelling study. Lancet Infect. Dis. 2016, 16, 1193–1201. [Google Scholar] [CrossRef] [Green Version]
- Seddon, J.A.; Hesseling, A.C.; Godfrey-Faussett, P.; Schaaf, H.S. High treatment success in children treated for multidrug-resistant tuberculosis: An observational cohort study. Thorax 2014, 69, 458–464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nunn, A.J.; Phillips, P.P.J.; Meredith, S.K.; Chiang, C.Y.; Conradie, F.; Dalai, D.; van Deun, A.; Dat, P.T.; Lan, N.; Master, I.; et al. A Trial of a Shorter Regimen for Rifampin-Resistant Tuberculosis. N. Engl. J. Med. 2019, 380, 1201–1213. [Google Scholar] [CrossRef]
- Seddon, J.A.; Thee, S.; Jacobs, K.; Ebrahim, A.; Hesseling, A.C.; Schaaf, H.S. Hearing loss in children treated for multidrug-resistant tuberculosis. J. Infect. 2013, 66, 320–329. [Google Scholar] [CrossRef]
- Gandhi, N.R.; Moll, A.; Sturm, A.W.; Pawinski, R.; Govender, T.; Lalloo, U.; Zeller, K.; Andrews, J.; Friedland, G. Extensively drug-resistant tuberculosis as a cause of death in patients co-infected with tuberculosis and HIV in a rural area of South Africa. Lancet 2006, 368, 1575–1580. [Google Scholar] [CrossRef]
- Jenkins, H.E.; Tolman, A.W.; Yuen, C.M.; Parr, J.B.; Keshavjee, S.; Pérez-Vélez, C.M.; Pagano, M.; Becerra, M.C.; Cohen, T. Incidence of multidrug-resistant tuberculosis disease in children: Systematic review and global estimates. Lancet 2014, 383, 1572–1579. [Google Scholar] [CrossRef] [Green Version]
- Zignol, M.; Sismanidis, C.; Falzon, D.; Glaziou, P.; Dara, M.; Floyd, K. Multidrug-resistant tuberculosis in children: Evidence from global surveillance. Eur. Respir. J. 2013, 42, 701–707. [Google Scholar] [CrossRef] [Green Version]
- Marks, S.M.; Mase, S.R.; Morris, S.B. Systematic Review, Meta-analysis, and Cost-effectiveness of Treatment of Latent Tuberculosis to Reduce Progression to Multidrug-Resistant Tuberculosis. Clin. Infect. Dis. 2017, 64, 1670–1677. [Google Scholar] [CrossRef]
- World Health Organization. WHO Consolidated Guidelines on Tuberculosis: Tuberculosis Preventive Treatment; World Health Organization: Geneva, Switzerland, 2020. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK554956/pdf/Bookshelf_NBK554956.pdf (accessed on 23 November 2020).
- Schaaf, H.S. Diagnosis and Management of Multidrug-Resistant Tuberculosis in Children: A Practical Approach. Indian J. Pediatr. 2019, 86, 717–724. [Google Scholar] [CrossRef]
- Seddon, J.A.; Johnson, S.; Palmer, M.; van der Zalm, M.M.; Lopez-Varela, E.; Hughes, J.; Schaaf, H.S. Multidrug-resistant tuberculosis in children and adolescents: Current strategies for prevention and treatment. Expert Rev. Respir. Med. 2020, 15, 221–237. [Google Scholar] [CrossRef]
- World Health Organization. WHO Consolidated Guidelines on Tuberculosis. Module 4: Treatment. Drug-Resistant Tuberculosis Treatment; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Nahid, P.; Mase, S.R.; Migliori, G.B.; Sotgiu, G.; Bothamley, G.H.; Brozek, J.; Cattamanchi, A.; Cegielski, J.P.; Chen, L.; Daley, C.L.; et al. Treatment of Drug-Resistant Tuberculosis. An Official ATS/CDC/ERS/IDSA Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2019, 200, e93–e142. [Google Scholar] [CrossRef]
- The Sentinel Project for Pediatric Drug-Resistant Tuberculosis. Management of Drug-Resistant Tuberculosis in Children: A Field Guide, 4th ed.; The Sentinel Project for Pediatric Drug-Resistant Tuberculosis: Boston, MA, USA, 2018; Available online: http://sentinel-project.org/wp-content/uploads/2019/02/Updated_DRTB-Field-Guide-2019-V3.pdf (accessed on 24 November 2020).
- Osborne, R. First novel anti-tuberculosis drug in 40 years. Nat. Biotechnol. 2013, 31, 89–91. [Google Scholar] [CrossRef]
- Caminero, J.A.; Piubello, A.; Scardigli, A.; Migliori, G.B. Bedaquiline: How better to use it. Eur. Respir. J. 2017, 50, 1701670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andries, K.; Verhasselt, P.; Guillemont, J.; Göhlmann, H.W.; Neefs, J.M.; Winkler, H.; Van Gestel, J.; Timmerman, P.; Zhu, M.; Lee, E.; et al. A diarylquinoline drug active on the ATP synthase of Mycobacterium tuberculosis. Science 2005, 307, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Haagsma, A.C.; Abdillahi-Ibrahim, R.; Wagner, M.J.; Krab, K.; Vergauwen, K.; Guillemont, J.; Andries, K.; Lill, H.; Koul, A.; Bald, D. Selectivity of TMC207 towards mycobacterial ATP synthase compared with that towards the eukaryotic homologue. Antimicrob. Agents Chemother. 2009, 53, 1290–1292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koul, A.; Vranckx, L.; Dhar, N.; Göhlmann, H.W.; Özdemir, E.; Neefs, J.M.; Schulz, M.; Lu, P.; Mørtz, E.; McKinney, J.D.; et al. Delayed bactericidal response of Mycobacterium tuberculosis to bedaquiline involves remodelling of bacterial metabolism. Nat. Commun. 2014, 5, 3369. [Google Scholar] [CrossRef]
- D’Ambrosio, L.; Centis, R.; Tiberi, S.; Tadolini, M.; Dalcolmo, M.; Rendon, A.; Esposito, S.; Migliori, G.B. Delamanid and bedaquiline to treat multidrug-resistant and extensively drug-resistant tuberculosis in children: A systematic review. J Thorac Dis. 2017, 9, 2093–2101. [Google Scholar] [CrossRef] [Green Version]
- Diacon, A.H.; Dawson, R.; Von Groote-Bidlingmaier, F.; Symons, G.; Venter, A.; Donald, P.R.; Conradie, A.; Erondu, N.; Ginsberg, A.M.; Egizi, E.; et al. Randomized dose-ranging study of the 14-day early bactericidal activity of bedaquiline (TMC207) in patients with sputum microscopy smear-positive pulmonary tuberculosis. Antimicrob. Agents Chemother. 2013, 57, 2199–2203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esposito, S.; Bianchini, S.; Blasi, F. Bedaquiline and delamanid in tuberculosis. Expert Opin. Pharmacother. 2015, 16, 2319–2330. [Google Scholar] [CrossRef] [PubMed]
- Guglielmetti, L.; Le Dû, D.; Jachym, M.; Henry, B.; Martin, D.; Caumes, E.; Veziris, N.; Métivier, N.; Robert, J.; MDR-TB Management Group of the French National Reference Center for Mycobacteria and the Physicians of the French MDR-TB Cohort. Compassionate use of bedaquiline for the treatment of multidrug-resistant and extensively drug-resistant tuberculosis: Interim analysis of a French cohort. Clin. Infect. Dis. 2015, 60, 188–194. [Google Scholar] [CrossRef] [PubMed]
- Guglielmetti, L.; Jaspard, M.; Le Dû, D.; Lachâtre, M.; Marigot-Outtandy, D.; Bernard, C.; Veziris, N.; Robert, J.; Yazdanpanah, Y.; Caumes, E.; et al. Long-term outcome and safety of prolonged bedaquiline treatment for multidrug-resistant tuberculosis. Eur. Respir. J. 2017, 49, 1601799. [Google Scholar] [CrossRef]
- Olaru, I.D.; Heyckendorf, J.; Andres, S.; Kalsdorf, B.; Lange, C. Bedaquiline-based treatment regimen for multidrug-resistant tuberculosis. Eur. Respir. J. 2017, 49, 1700742. [Google Scholar] [CrossRef] [PubMed]
- Skrahina, A.; Hurevich, H.; Falzon, D.; Zhilevich, L.; Rusovich, V.; Dara, M.; Setkina, S. Bedaquiline in the multidrug-resistant tuberculosis treatment: Belarus experience. Int. J. Mycobacteriol. 2016, 5 (Suppl. 1), S62–S63. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. The Use of Bedaquiline in the Treatment of Multidrug-Resistant Tuberculosis Interim Policy Guidance; WHO/HTM/TB/2013.6; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- Hewison, C.; Bastard, M.; Khachatryan, N.; Kotrikadze, T.; Hayrapetyan, A.; Avaliani, Z.; Kiria, N.; Yegiazaryan, L.; Chumburidze, N.; Kirakosyan, O.; et al. Is 6 months of bedaquiline enough? Results from the compassionate use of bedaquiline in Armenia and Georgia. Int. J. Tuberc. Lung Dis. 2018, 22, 766–772. [Google Scholar] [CrossRef]
- Borisov, S.E.; Dheda, K.; Enwerem, M.; Romero Leyet, R.; D’Ambrosio, L.; Centis, R.; Sotgiu, G.; Tiberi, S.; Alffenaar, J.W.; Maryandyshev, A.; et al. Effectiveness and safety of bedaquiline-containing regimens in the treatment of MDR- and XDR-TB: A multicentre study. Eur. Respir. J. 2017, 49, 1700387. [Google Scholar] [CrossRef] [Green Version]
- Diacon, A.H.; Pym, A.; Grobusch, M.; Patientia, R.; Rustomjee, R.; Page-Shipp, L.; Pistorius, C.; Krause, R.; Bogoshi, M.; Churchyard, G.; et al. The diarylquinoline TMC207 for multidrug-resistant tuberculosis. N. Engl. J. Med. 2009, 360, 2397–2405. [Google Scholar] [CrossRef] [Green Version]
- Diacon, A.H.; Donald, P.R.; Pym, A.; Grobusch, M.; Patientia, R.F.; Mahanyele, R.; Bantubani, N.; Narasimooloo, R.; De Marez, T.; van Heeswijk, R.; et al. Randomized pilot trial of eight weeks of bedaquiline (TMC207) treatment for multidrug-resistant tuberculosis: Long-term outcome, tolerability, and effect on emergence of drug resistance. Antimicrob. Agents Chemother. 2012, 56, 3271–3276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diacon, A.H.; Pym, A.; Grobusch, M.P.; de los Rios, J.M.; Gotuzzo, E.; Vasilyeva, I.; Leimane, V.; Andries, K.; Bakare, N.; De Marez, T.; et al. Multidrug-resistant tuberculosis and culture conversion with bedaquiline. N. Engl. J. Med. 2014, 371, 723–732. [Google Scholar] [CrossRef] [Green Version]
- Pym, A.S.; Diacon, A.H.; Tang, S.J.; Conradie, F.; Danilovits, M.; Chuchottaworn, C.; Vasilyeva, I.; Andries, K.; Bakare, N.; De Marez, T.; et al. Bedaquiline in the treatment of multidrug- and extensively drug-resistant tuberculosis. Eur. Respir. J. 2016, 47, 564–574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amankwa, K.; Krishnan, S.C.; Tisdale, J.E. Torsades de pointes associated with fluoroquinolones: Importance of concomitant risk factors. Clin. Pharmacol. Ther. 2004, 75, 242–247. [Google Scholar] [CrossRef] [PubMed]
- Choudhri, S.H.; Harris, L.; Butany, J.W.; Keystone, J.S. Clofazimine induced cardiotoxicity—A case report. Lepr. Rev. 1995, 66, 63–68. [Google Scholar] [CrossRef]
- European Medicines Agency. Sirturo (Bedaquiline). Available online: www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/human/medicines/002614human_med_001730.jsp&mid=WC0b01ac058001d124 (accessed on 1 May 2021).
- Schnippel, K.; Ndjeka, N.; Maartens, G.; Meintjes, G.; Master, I.; Ismail, N.; Hughes, J.; Ferreira, H.; Padanilam, X.; Romero, R.; et al. Effect of bedaquiline on mortality in South African patients with drug-resistant tuberculosis: A retrospective cohort study. Lancet Respir. Med. 2018, 6, 699–706. [Google Scholar] [CrossRef]
- Collaborative Group for the Meta-Analysis of Individual Patient Data in MDR-TB Treatment–2017; Ahmad, N.; Ahuja, S.D.; Akkerman, O.W.; Alffenaar, J.C.; Anderson, L.F.; Baghaei, P.; Bang, D.; Barry, P.M.; Bastos, M.L.; et al. Treatment correlates of successful outcomes in pulmonary multidrug-resistant tuberculosis: An individual patient data meta-analysis. Lancet 2018, 392, 821–834. [Google Scholar]
- Mbuagbaw, L.; Guglielmetti, L.; Hewison, C.; Bakare, N.; Bastard, M.; Caumes, E.; Fréchet-Jachym, M.; Robert, J.; Veziris, N.; Khachatryan, N.; et al. Outcomes of Bedaquiline Treatment in Patients with Multidrug-Resistant Tuberculosis. Emerg. Infect. Dis. 2019, 25, 936–943. [Google Scholar] [CrossRef] [Green Version]
- Olayanju, O.; Limberis, J.; Esmail, A.; Oelofse, S.; Gina, P.; Pietersen, E.; Fadul, M.; Warren, R.; Dheda, K. Long-term bedaquiline-related treatment outcomes in patients with extensively drug-resistant tuberculosis from South Africa. Eur. Respir. J. 2018, 51, 1800544. [Google Scholar] [CrossRef]
- Rouan, M.C.; Lounis, N.; Gevers, T.; Dillen, L.; Gilissen, R.; Raoof, A.; Andries, K. Pharmacokinetics and pharmacodynamics of TMC207 and its N-desmethyl metabolite in a murine model of tuberculosis. Antimicrob. Agents Chemother. 2012, 56, 1444–1451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Svensson, E.M.; Aweeka, F.; Park, J.G.; Marzan, F.; Dooley, K.E.; Karlsson, M.O. Model-based estimates of the effects of efavirenz on bedaquiline pharmacokinetics and suggested dose adjustments for patients coinfected with HIV and tuberculosis. Antimicrob. Agents Chemother. 2013, 57, 2780–2787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Interim Guidance on the Use of Bedaquiline to Treat MDR-TB. Available online: https://apps.who.int/iris/bitstream/handle/10665/84879/9789241505482_eng.pdf?sequence=1 (accessed on 1 May 2021).
- Dooley, K.E.; Park, J.G.; Swindells, S.; Allen, R.; Haas, D.W.; Cramer, Y.; Aweeka, F.; Wiggins, I.; Gupta, A.; Lizak, P.; et al. Safety, tolerability, and pharmacokinetic interactions of the antituberculous agent TMC207 (bedaquiline) with efavirenz in healthy volunteers: AIDS Clinical Trials Group Study A5267. J. Acquir. Immune Defic. Syndr. 2012, 59, 455–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koirala, S.; Borisov, S.; Danila, E.; Mariandyshev, A.; Shrestha, B.; Lukhele, N.; Dalcolmo, M.; Shakya, S.R.; Miliauskas, S.; Kuksa, L.; et al. Outcome of treatment of MDR-TB or drug-resistant patients treated with bedaquiline and delamanid: Results from a large global cohort. Pulmonology 2021. [Google Scholar] [CrossRef] [PubMed]
- Svensson, E.M.; Dooley, K.E.; Karlsson, M.O. Impact of lopinavir-ritonavir or nevirapine on bedaquiline exposures and potential implications for patients with tuberculosis-HIV coinfection. Antimicrob. Agents Chemother. 2014, 58, 6406–6412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brill, M.J.; Svensson, E.M.; Pandie, M.; Maartens, G.; Karlsson, M.O. Confirming model-predicted pharmacokinetic interactions between bedaquiline and lopinavir/ritonavir or nevirapine in patients with HIV and drug-resistant tuberculosis. Int. J. Antimicrob. Agents 2017, 49, 212–217. [Google Scholar] [CrossRef]
- Achar, J.; Hewison, C.; Cavalheiro, A.P.; Skrahina, A.; Cajazeiro, J.; Nargiza, P.; Herboczek, K.; Rajabov, A.S.; Hughes, J.; Ferlazzo, G.; et al. Off-Label Use of Bedaquiline in Children and Adolescents with Multidrug-Resistant Tuberculosis. Emerg. Infect. Dis. 2017, 23, 1711–1713. [Google Scholar] [CrossRef] [Green Version]
- Conradie, F.; Diacon, A.H.; Ngubane, N.; Howell, P.; Everitt, D.; Crook, A.M.; Mendel, C.M.; Egizi, E.; Moreira, J.; Timm, J.; et al. Treatment of Highly Drug-Resistant Pulmonary Tuberculosis. N. Engl. J. Med. 2020, 382, 893–902. [Google Scholar] [CrossRef]
- Pharmacokinetic Study to Evaluate Anti-Mycobacterial Activity of TMC207 in Combination with Background Regimen (BR) of Multidrug Resistant Tuberculosis (MDR-TB) Medications for Treatment of Children/Adolescents Pulmonary MDR-TB—Full Text View—ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT02354014 (accessed on 1 May 2021).
- Evaluating the Pharmacokinetics, Safety, and Tolerability of Bedaquiline in HIV-Infected and HIV-Uninfected Infants, Children, and Adolescents with Multidrug-Resistant Tuberculosis—Full Text View—ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT02906007 (accessed on 1 May 2021).
- Esposito, S.; Bianchini, S.; Argentiero, A.; Neglia, C.; Principi, N. How does one choose the appropriate pharmacotherapy for children with lower respiratory tract infections? Expert Opin. Pharmacother. 2020, 21, 1739–1747. [Google Scholar] [CrossRef]
- Matsumoto, M.; Hashizume, H.; Tomishige, T.; Kawasaki, M.; Tsubouchi, H.; Sasaki, H.; Shimokawa, Y.; Komatsu, M. OPC-67683, a nitro-dihydro-imidazooxazole derivative with promising action against tuberculosis in vitro and in mice. PLoS Med. 2006, 3, e466. [Google Scholar] [CrossRef]
- Liu, Y.; Matsumoto, M.; Ishida, H.; Ohguro, K.; Yoshitake, M.; Gupta, R.; Geiter, L.; Hafkin, J. Delamanid: From discovery to its use for pulmonary multidrug-resistant tuberculosis (MDR-TB). Tuberculosis 2018, 111, 20–30. [Google Scholar] [CrossRef]
- Lewis, J.M.; Sloan, D.J. The role of delamanid in the treatment of drug-resistant tuberculosis. Ther. Clin. Risk Manag. 2015, 11, 779–791. [Google Scholar]
- Szumowski, J.D.; Lynch, J.B. Profile of delamanid for the treatment of multidrug-resistant tuberculosis. Drug Des. Dev. Ther. 2015, 9, 677–682. [Google Scholar]
- Deltyba, INN-Delamanid—European Medicines Agency—Europa. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/deltyba (accessed on 14 May 2021).
- Sasahara, K.; Shimokawa, Y.; Hirao, Y.; Koyama, N.; Kitano, K.; Shibata, M.; Umehara, K. Pharmacokinetics and metabolism of delamanid, a novel anti-tuberculosis drug, in animals and humans: Importance of albumin metabolism in vivo. Drug Metab. Dispos. 2015, 43, 1267–1276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shibata, M.; Shimokawa, Y.; Sasahara, K.; Yoda, N.; Sasabe, H.; Suzuki, M.; Umehara, K. Absorption, distribution and excretion of the anti-tuberculosis drug delamanid in rats: Extensive tissue distribution suggests potential therapeutic value for extrapulmonary tuberculosis. Biopharm. Drug Dispos. 2017, 38, 301–312. [Google Scholar] [CrossRef]
- Diacon, A.H.; Dawson, R.; Hanekom, M.; Narunsky, K.; Venter, A.; Hittel, N.; Geiter, L.J.; Wells, C.D.; Paccaly, A.J.; Donald, P.R. Early bactericidal activity of delamanid (OPC-67683) in smear-positive pulmonary tuberculosis patients. Int. J. Tuberc. Lung Dis. 2011, 15, 949–954. [Google Scholar] [CrossRef] [PubMed]
- Stinson, K.; Kurepina, N.; Venter, A.; Fujiwara, M.; Kawasaki, M.; Timm, J.; Shashkina, E.; Kreiswirth, B.N.; Liu, Y.; Matsumoto, M.; et al. MIC of Delamanid (OPC-67683) against Mycobacterium tuberculosis Clinical Isolates and a Proposed Critical Concentration. Antimicrob. Agents Chemother. 2016, 60, 3316–3322. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Hashizume, H.; Tomishige, T.; Nakamura, I.; Matsuba, M.; Fujiwara, M.; Kitamoto, R.; Hanaki, E.; Ohba, Y.; Matsumoto, M. Delamanid kills dormant mycobacteria in vitro and in a Guinea pig model of tuberculosis. Antimicrob. Agents Chemother. 2017, 61, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gler, M.T.; Skripconoka, V.; Sanchez-Garavito, E.; Xiao, H.; Cabrera-Rivero, J.L.; Vargas-Vasquez, D.E.; Gao, M.; Awad, M.; Park, S.K.; Shim, T.S.; et al. Delamanid for multidrug-resistant pulmonary tuberculosis. N. Engl. J. Med. 2012, 366, 2151–2160. [Google Scholar] [CrossRef] [Green Version]
- Skripconoka, V.; Danilovits, M.; Pehme, L.; Tomson, T.; Skenders, G.; Kummik, T.; Cirule, A.; Leimane, V.; Kurve, A.; Levina, K.; et al. Delamanid improves outcomes and reduces mortality in multidrug-resistant tuberculosis. Eur. Respir. J. 2013, 41, 1393–1400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wells, C.D.; Gupta, R.; Hittel, N.; Geiter, L.J. Long-term mortality assessment of multidrug- resistant tuberculosis patients treated with delamanid. Eur. Respir. J. 2015, 45, 1498–1501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Von Groote-Bidlingmaier, F.; Patientia, R.; Sanchez, E.; Balanag VJr Ticona, E.; Segura, P.; Cadena, E.; Yu, C.; Cirule, A.; Lizarbe, V.; Davidaviciene, E.; et al. Efficacy and safety of delamanid in combination with an optimised background regimen for treatment of multidrug-resistant tuberculosis: A multicentre, randomised, double-blind, placebo-controlled, parallel group phase 3 trial. Lancet Respir. Med. 2019, 7, 249–259. [Google Scholar] [CrossRef]
- Tadolini, M.; Garcia-Prats, A.J.; D’Ambrosio, L.; Hewison, C.; Centis, R.; Schaaf, H.S.; Marais, B.J.; Ferreira, H.; Caminero, J.A.; Jonckheere, S.; et al. Compassionate use of new drugs in children and adolescents with multidrug-resistant and extensively drug-resistant tuberculosis: Early experiences and challenges. Eur. Respir. J. 2016, 48, 938–943. [Google Scholar] [CrossRef] [PubMed]
- Hafkin, J.; Gler, M.; Frias, M.; Leon, A.; Hittel, N.; Geiter, L.; Wells, C.M.S. Long-term safety, tolerability, and pharmacokinetics of delamanid in children ages 12–17. In Proceedings of the 46th Union World Conference on Lung Health, Cape Town, South Africa, 28–30 November 2015. [Google Scholar]
- Shah, I.; Gandhi, S.; Shetty, N.S. Bedaquiline and Delamanid in Children with XDR Tuberculosis: What is prolonged QTc? Pediatr. Infect. Dis. J. 2020, 39, 512–513. [Google Scholar] [CrossRef] [PubMed]
- Mallikaarjun, S.; Wells, C.; Petersen, C.; Paccaly, A.; Shoaf, S.E.; Patil, S.; Geiter, L. Delamanid Coadministered with Antiretroviral Drugs or Antituberculosis Drugs Shows No Clinically Relevant Drug-Drug Interactions in Healthy Subjects. Antimicrob. Agents Chemother. 2016, 60, 5976–5985. [Google Scholar] [CrossRef] [Green Version]
- Dooley, K.E.; Rosenkranz, S.L.; Conradie, F.; Moran, L.E.; Hafner, R.; von Groote-Bidlingmaier, F.; Lama, J.R.; Shenje, J.; Comins, K.; Morganroth, J.; et al. QT effects of bedaquiline, delamanid or both in MDR-TB patients: The DELIBERATE trial (DELamanId BEdaquiline for ResistAnt TubErculosis). In Proceedings of the Conference on Retroviruses and Opportunistic Infections (CROI), Seattle, WA, USA, 4–7 March 2019. [Google Scholar]
- Esposito, S.; Bosis, S.; Tadolini, M.; Bianchini, S.; Migliori, G.B.; Principi, N. Efficacy, safety, and tolerability of a 24-month treatment regimen including delamanid in a child with extensively drug-resistant tuberculosis: A case report and review of the literature. Medicine 2016, 95, e5347. [Google Scholar] [CrossRef]
- Esposito, S.; D’Ambrosio, L.; Tadolini, M.; Schaaf, H.S.; Luna, J.C.; Marais, B.; Centis, R.; Dara, M.; Matteelli, A.; Blasi, F.; et al. ERS/WHO Tuberculosis Consilium assistance with extensively drug-resistant tuberculosis management in a child: Case study of compassionate delamanid use. Eur. Respir. J. 2014, 44, 811–815. [Google Scholar] [CrossRef] [Green Version]
- Kuksa, L.; Barkane, L.; Hittel, N.; Gupta, R. Final treatment outcomes of multidrug- and extensively drug-resistant tuberculosis patients in Latvia receiving delamanid-containing regimens. Eur. Respir. J. 2017, 50, 1701105. [Google Scholar] [CrossRef] [Green Version]
- Mohr, E.; Hughes, J.; Reuter, A.; Trivino Duran, L.; Ferlazzo, G.; Daniels, J.; De Azevedo, V.; Kock, Y.; Steele, S.J.; Shroufi, A.; et al. Delamanid for rifampicin-resistant tuberculosis: A retrospective study from South Africa. Eur. Respir. J. 2018, 51, 1800017. [Google Scholar] [CrossRef]
- Hewison, C.; Ferlazzo, G.; Avaliani, Z.; Hayrapetyan, A.; Jonckheere, S.; Khaidarkhanova, Z.; Mohr, E.; Sinha, A.; Skrahina, A.; Vambe, D.; et al. Six-Month Response to Delamanid Treatment in MDR TB Patients. Emerg. Infect. Dis. 2017, 23, 1746–1748. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. The Use of Delamanid in the Treatment of Multidrug-Resistant Tuberculosis in Children and Adolescents: Interim Policy Guidance. 2016. Available online: https://apps.who.int/iris/bitstream/handle/10665/250614/9789241549899-eng.pdf?sequence=1 (accessed on 1 May 2021).
- ClinicalTrials.gov. A 6-Month Safety, Efficacy, and PK Trial of Delamanid in Pediatric Patients with Multidrug Resistant Tuberculosis. Available online: https://clinicaltrials.gov/ct2/show/NCT01859923 (accessed on 1 May 2021).
- ClinicalTrials.gov. Pharmacokinetic and Safety Trial to Determine the Appropriate Dose for Pediatric Patients with Multidrug Resistant Tuberculosis. Available online: https://clinicaltrials.gov/ct2/show/NCT01856634 (accessed on 1 May 2021).
- ClinicalTrials.gov. Evaluating the Pharmacokinetics, Safety, and Tolerability of Delamanid in Combination with Optimized Multidrug Background Regimen (OBR) for Multidrug-Resistant Tuberculosis (MDR-TB) in HIV-Infected and HIV-Uninfected Children with MDR-TB. Available online: https://www.clinicaltrials.gov/ct2/show/NCT03141060 (accessed on 1 May 2021).
- Khoshnood, S.; Goudarzi, M.; Taki, E.; Darbandi, A.; Kouhsari, E.; Heidary, M.; Motahar, M.; Moradi, M.; Bazyar, H. Bedaquiline: Current status and future perspectives. J. Glob. Antimicrob. Resist. 2021, 25, 48–59. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, M.; Kawasaki, M.; Hariguchi, N.; Liu, Y.; Matsumoto, M. Mechanisms of resistance to delamanid, a drug for Mycobacterium tuberculosis. Tuberculosis 2018, 108, 186–194. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Groups and Steps | Medicine | Abbreviation |
|---|---|---|
| Group A: Include all three medicines | Levofloxacin or moxifloxacin | Lfx Mfx |
| Bedaquiline | Bdq | |
| Linezolid | Lzd | |
| Group B: Add one or both medicines | Clofazimine | Cfz |
| Cycloserine or terizidone | Cs Trd | |
| Group C: Add to complete the regimen, and when medicines from Groups A and B cannot be used | Ethambutol | E |
| Delamanid | Dlm | |
| Pyrazinamide | Z | |
| Imipenem-cilastatin or meropenem | Ipm-Cln Mpm | |
| Amikacin (or streptomycin) | Am (S) | |
| Ethionamide or prothionamide | Eto Pto | |
| P-aminosalicylic acidi | PAS |
| Authors [Reference] (Year) | Type of Study | Study Population (Age of Patients) | Therapy | Results |
|---|---|---|---|---|
| Diacon et al. [37] (2009) | phase 2, randomized, double-blind, controlled trial | 47 patients with MDR pulmonary tuberculosis (18–65 years) | Bedaquiline (400 mg once daily for 2 weeks, followed by 200 mg three times a week for 6 weeks), or placebo, plus background regimen (8 weeks) | Reduction of time to induce sputum conversion, as compared with placebo (p = 0.003) Increased proportion of patients with conversion of sputum culture (48% vs. 9%) |
| Diacon et al. [39] (2014) | phase 2, randomized, double-blind, controlled trial | 160 patients with MDR pulmonary tuberculosis (18–65 years) | Bedaquiline (400 mg once daily for 2 weeks, followed by 200 mg three times a week for 6 weeks), or placebo, plus background regimen (24 weeks) | Reduction of the median time to culture conversion, as compared with placebo, from 125 days to 83 days (p < 0.001) Increased rate of culture conversion at 24 weeks (p = 0.008) and at 120 weeks (p = 0.04). |
| Guglielmetti et al. [30] (2015) | retrospective cohort study | 35 patients with MDR-TB (18–70 years) | Bedaquiline (400 mg once daily for 2 weeks, followed by 200 mg three times a week), plus background regimen | Culture conversion achieved in 28 of 29 (97%) cases with culture-positive pulmonary tuberculosis at bedaquiline initiation |
| Pym et al. [40] (2016) | phase 2, multicenter, open-label, single-arm trial | 205 patients with MDR-TB (18–68 years) | Bedaquiline (400 mg once daily for 2 weeks, followed by 200 mg three times a week for a further 22 weeks), plus background regimen | Culture conversion was 72.2% at 120 weeks: MDR-TB (73.1%), pre-XDR-TB (70.5%) XDR-TB (62.2%) |
| Guglielmetti et al. [31] (2017) | multicentre observational study | 45 patients with MDR-TB (30–42 years) | Bedaquiline (400 mg once daily for 2 weeks, followed by 200 mg three times a week) -12 patients: standard bedaquiline treatment (≤ 190 days) -33 patients: prolonged bedaquiline treatment (>190 days) | 36 patients (80%) had favourable outcome 5 were lost to follow-up 3 died 1 failed and acquired bedaquiline resistance |
| Olaru et al. [32] (2017) | retrospective cohort study | 30 patients with MDR/XDR-TB (23–39 years) | 6 months of a bedaquiline-containing regimen | Culture conversion achieved within 8 weeks of initiating MDR-TB treatment in 12 (60%) patients and within 6 months in 20 (100%) patients |
| Borisov et al. [36] (2017) | large, retrospective, multicenter observational study | 428 patients with MDR/XDR-TB (27–44 years) | Bedaquiline (400 mg once daily for 2 weeks, followed by 200 mg three times a week), plus background regimen | Culture conversion rates: 30.1% at 30 days 56.7%, at 60 days 80.5%, at 90 days 91.2% at the end of treatment |
| Hewison et al. [35] (2018) | retrospective cohort study | 82 patients with MDR-TB/pre-XDR-TB/XDR-TB (31–51 years) | Bedaquiline (400 mg once daily for 2 weeks, followed by 200 mg three times a week) | Culture conversion achieved in 54/64 (84.4%) patients with a positive culture at treatment initiation |
| Authors (Year) | Type of Study | Study Population | Median Age of Patients (Range) | Therapy | Results |
|---|---|---|---|---|---|
| Aschar et al. [55] (2017) | retrospective cohort study | 27 patients with confirmed or presumed MDR/XDR-TB | 16 years (10–17 years) | Bedaquiline (400 mg once daily for 2 weeks, followed by 200 mg three times a week for 24 weeks), plus background regimen One 10-years-old girl (weighing 35 kg) received 300 mg daily during her loading phase | Sputum culture negative: 23/23 (100%) and No clinical signs suggestive of treatment failure 5 patients (19%) reported adverse effects caused by bedaquiline (prolongation of QTc), without correlated symptoms |
| Conradie et al. [56] (2020) | Open-label, single-group study | 109 patients with MDR/XDR-TB | 35 years (17–60 years) | Bedaquiline (400 mg once daily for 2 weeks, followed by 200 mg three times a week for 24 weeks) + Pretomanid (200 mg daily for 26 weeks) + Linezolid (1200 mg daily for 26 weeks) | Unfavourable outcome: 11 patients (10%) vs. Favourable outcome: 98 patients (90%) Serious adverse events: 19 patients (17%) No patient had a QT interval increase > 480 msec. |
| Title | Study Design | Target Population | Intervention | Outcome Measures |
|---|---|---|---|---|
| Janssen C221 (NCT02354014) | A phase II, open-label, multicenter, single-arm study | Children and adolescents who have confirmed or probable pulmonary MDR-TB enrolled in 4 age-based cohorts: (1) ≥12–<18 years (2) ≥5–<12 years (3) ≥2–<5 years (4) 0 months–<2 years | Cohort 1: bedaquiline 400 mg qd, for first 2 weeks, followed by 200 mg tiw for 22 weeks Cohort 2: bedaquiline 200 mg qd for first 2 weeks, followed by 100 mg tiw for 22 weeks. Cohort 3: bedaquiline 8 mg/kg qd for the first 2 weeks, followed by 4 mg/kg tiw for 22 weeks. Cohort 4: bedaquiline dose will be selected based on the results from the previous cohorts 1, 2 and 3. + BR MDR-TB Medications. | Pharmacokinetic, safety, tolerability, and antimycobacterial activity of bedaquiline |
| IMPAACT P1108 (NCT02906007) | Phase I/II, open-label, single-arm study to evaluate | HIV-infected and HIV-uninfected infants, children, and adolescents with MDR-TB disease. Age at enrollment: Cohort 1: ≥6–<18 years Cohort 1: ≥2–<6 years Cohort 1: 0–<2 years Weight at enrollment: Cohort 1: ≥15 Cohort 1: ≥7 Cohort 1: ≥3 | Bedaquiline doses will vary based on the participant’s age and weight. + optimized individualized MDR-TB therapy | Pharmacokinetic, safety, and tolerability of bedaquiline |
| Bedaquiline | ≥15 Years | < 15 Years | |
|---|---|---|---|
| 16–30 kg | >30 kg | ||
| 100 mg tab | 4 tabs qd for first 2 weeks; then 2 tabs qd M/W/F for 22 weeks | 2 tabs qd for 2 weeks; then 1 tab qd M/W/F for 22 weeks | 4 tabs qd for 2 weeks; then 2 tabs qd M/W/F for 22 weeks |
| 20 mg dt | 10 dts qd for 2 weeks; then 5 dts od M/W/F for 22 weeks | 20 dts qd for 2 weeks; then 10 dts od M/W/F for 22 weeks | |
| Authors [Reference] (Year) | Type of Study | Study Population (Age of Patients) | Therapy | Results |
|---|---|---|---|---|
| Diacon et al. [67] (2011) | phase IIa, open-label, randomised, controlled trial | 48 patients with newly diagnosed smear-positive pulmonary TB (18–64 years) | four groups of 12 patients receiving (1) delamanid 100 mg qd (2) delamanid 200 mg qd (3) delamanid 300 mg qd (4) delamanid 400 mg qd + one control group of 6 patients receiving standard four-drug anti-tuberculosis treatment (HRZE) | Delamanid at all dosages demonstrated significant exposure dependent EBA over 14 days |
| Gler et al. [70] (2012) | Double-blind, multicenter, randomized, placebo-controlled trial | 481 patients with pulmonary MDR-TB (18–64 years) | Group 1: Delamanid 100 mg td + BR Group 2: Delamanid 200 mg td + BR Group 3: Placebo + BR | Statistically significant difference in sputum-culture conversion between delamanid groups and placebo group |
| Skripconoka et al. [71] (2013) | Multicenter observational study | 421 patients with pulmonary MDR-TB (18–63 years) | Group 1: Delamanid (100 mg td or 200 mg td) for ≥ 6 months + BR Group 2: Delamanid (100 mg td or 200 mg td) for < 6 months + BR | Favourable outcomes observed in patients who received delamanid for ≥6 months, compared to patients who received delamanid for ≤2 months. Reduction of mortality of 1.0% among those receiving long-term delamanid vs. short-term/no delamanid (p < 0.001) |
| Von Groote-Bidlingmaier et al. [73] (2019) | Phase III, randomised, double-blind, placebo-controlled trial | 511 patients with a diagnosis of pulmonary MDR tuberculosis (18–69 years) | Group 1: Delamanid (100 mg td for 2 months followed by 200 mg qd for 4 months) + BR Group 2: Placebo + BR | No significant advantage in the delamanid arm in reducing the median time to sputum culture conversion |
| Authors (Year) | Type of Study | Study Population | Median Age of Patients (Range) | Therapy | Results |
|---|---|---|---|---|---|
| Esposito S et al. [79] (2016) | Case report | 1 patient with confirmed pulmonary XDR-TB | 12 years | Delamanid 100 mg td for 24 months + BR | Gastric aspirate culture negative after 1 week, the patient was considered cured at the end of the treatment. No adverse events were reported, normal corrected QT interval. |
| Tadolini M et al. [74] (2016) | Case series | 16 patients with confirmed pulmonary MDR/XDR-TB (2 also had extrapulmonary TB) | 15 years (8–14 years) | Delamanid 100 mg td for 24 weeks + BR (except one who received 50 mg td) | 81.2% culture-negative; no or mild adverse events except one patient who experienced severe vomiting, renal impairment, hypokalaemia, hypomagnesaemia and QT interval prolongation |
| Kuksa L et al. [81] (2017) | Case series | 2 patients with PreXDR/XDR-TB | 12 years (11–13 years) | Delamanid for 24 weeks (dosage not reported) + BR | Both patients were considered cured at the end of the treatment. No adverse events were reported, normal corrected QT interval. |
| Title | Study Design | Target Population | Intervention | Outcome Measures |
|---|---|---|---|---|
| A 6-Month Safety, Efficacy, and pharmacokinetic Trial of Delamanid in Pediatric Patients With MDR-TB (NCT01859923) | Phase 2, Open-label, Multiple-dose Trial | Children and adolescents who have confirmed or probable pulmonary MDR-TB enrolled in 4 age-based cohorts: (1) 12 to 17 years (2) 6 to 11 years (3) 3 to 5 years (4) 0 to 2 years | Group 1: Delamanid 100 mg td for 182 days + BR for 365 days Group 2: Delamanid 50 mg td for 182 days + BR for 365 days Group 3: Delamanid 25 mg (pediatric formulation) td for 182 days + BR for 365 days Cohort 4: Delamanid from 5 mg qd to 10 mg td (pediatric formulation) based on weight measurements for 182 days + BR for 365 days | Pharmacokinetic, safety, tolerability, and efficacy of delamanid |
| Pharmacokinetic and Safety Trial to Determine the Appropriate Dose for Pediatric Patients with MDR-TB (NCT01856634) | Phase 1, Open-label, Multiple-dose, and Age De-escalation Trial | Children and adolescents who have confirmed or probable pulmonary MDR-TB enrolled in 4 age-based cohorts: (1) 12 to 17 years (2) 6 to 11 years (3) 3 to 5 years (4) 0 to 2 years | Group 1: Delamanid 100 mg td + BR for 10 days Group 2: Delamanid 50 mg td + BR for 10 days Group 3: Delamanid 25 mg (pediatric formulation) td + BR for 10 days Cohort 4: Delamanid from 5 mg to 10 mg td (pediatric formulation) based on weight measurements + BR for 10 days | Pharmacokinetics, Safety and Tolerability of Delamanid |
| Evaluating the Pharmacokinetics, Safety, and Tolerability of Delamanid in Combination With Optimized Multidrug Background Regimen for MDR-TB in HIV-Infected and HIV-Uninfected Children With MDR-TB (NCT03141060) | Phase I/II Open-Label, Single-Arm Study | Children and adolescents who have MDR-TB with and without HIV-infection, enrolled in 4 age-based cohorts: (1) 12 to 17 years (2) 6 to 11 years (3) 3 to 5 years (4) 0 to 2 years | Delamanid for 24 weeks + BR, dose based on age group and weight | Pharmacokinetics, Safety, and Tolerability of Delamanid |
| Delamanid | ||
|---|---|---|
| Age (Weight Band) | Dose | 50 mg Tablet |
| 3–5 yrs (<24 kg) | 25 mg twice daily | - a |
| 6–11 yrs (24–34 kg) | 50 mg twice daily | 1 tablet twice daily |
| 12–17 yrs (>35 kg) | 100 mg twice daily | 2 tablets twice daily |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pecora, F.; Dal Canto, G.; Veronese, P.; Esposito, S. Treatment of Multidrug-Resistant and Extensively Drug-Resistant Tuberculosis in Children: The Role of Bedaquiline and Delamanid. Microorganisms 2021, 9, 1074. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9051074
Pecora F, Dal Canto G, Veronese P, Esposito S. Treatment of Multidrug-Resistant and Extensively Drug-Resistant Tuberculosis in Children: The Role of Bedaquiline and Delamanid. Microorganisms. 2021; 9(5):1074. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9051074
Chicago/Turabian StylePecora, Francesco, Giulia Dal Canto, Piero Veronese, and Susanna Esposito. 2021. "Treatment of Multidrug-Resistant and Extensively Drug-Resistant Tuberculosis in Children: The Role of Bedaquiline and Delamanid" Microorganisms 9, no. 5: 1074. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9051074