
Cardiopulmonary Effects and Pharmacokinetics of Dexmedetomidine Used as an Adjunctive Analgesic to Regional Anesthesia of the Oral Cavity with Levobupivacaine in Dogs


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
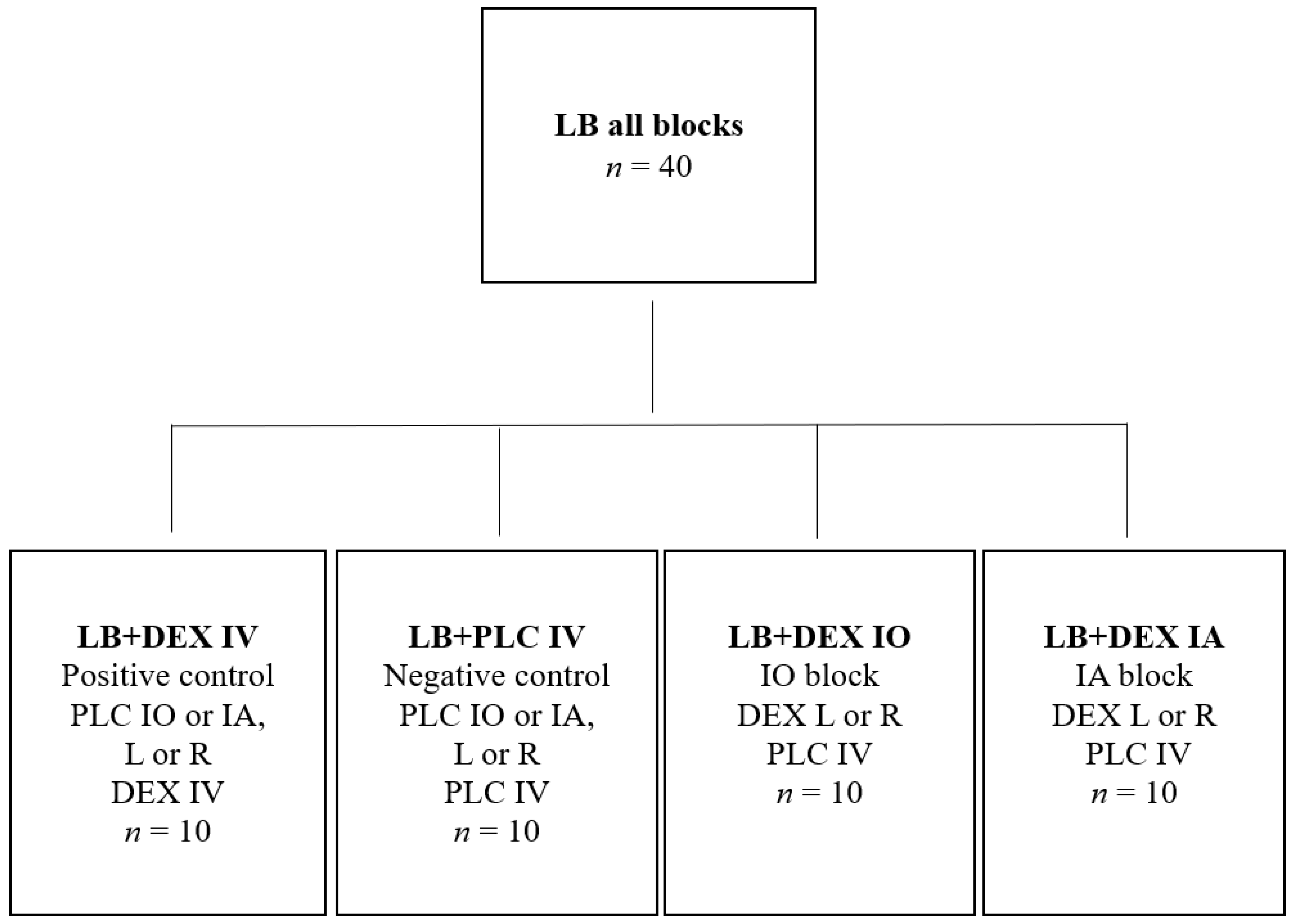
2.1. Pilot Study and Sample Size
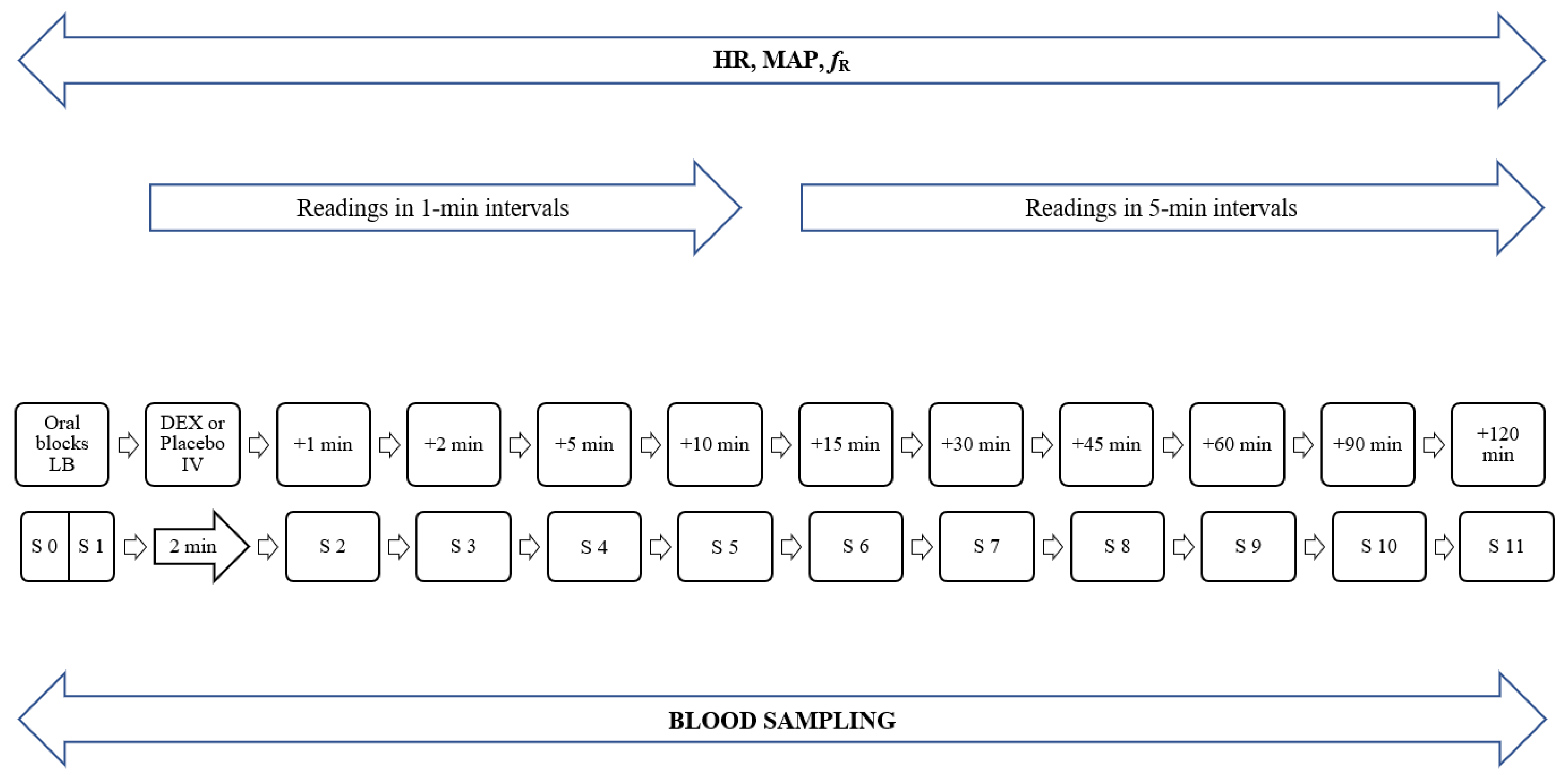
2.2. Main Study
2.3. Blood Sampling
2.4. Laboratory Analysis
2.5. Pharmacokinetic Analysis
2.6. Statistical Analysis
3. Results
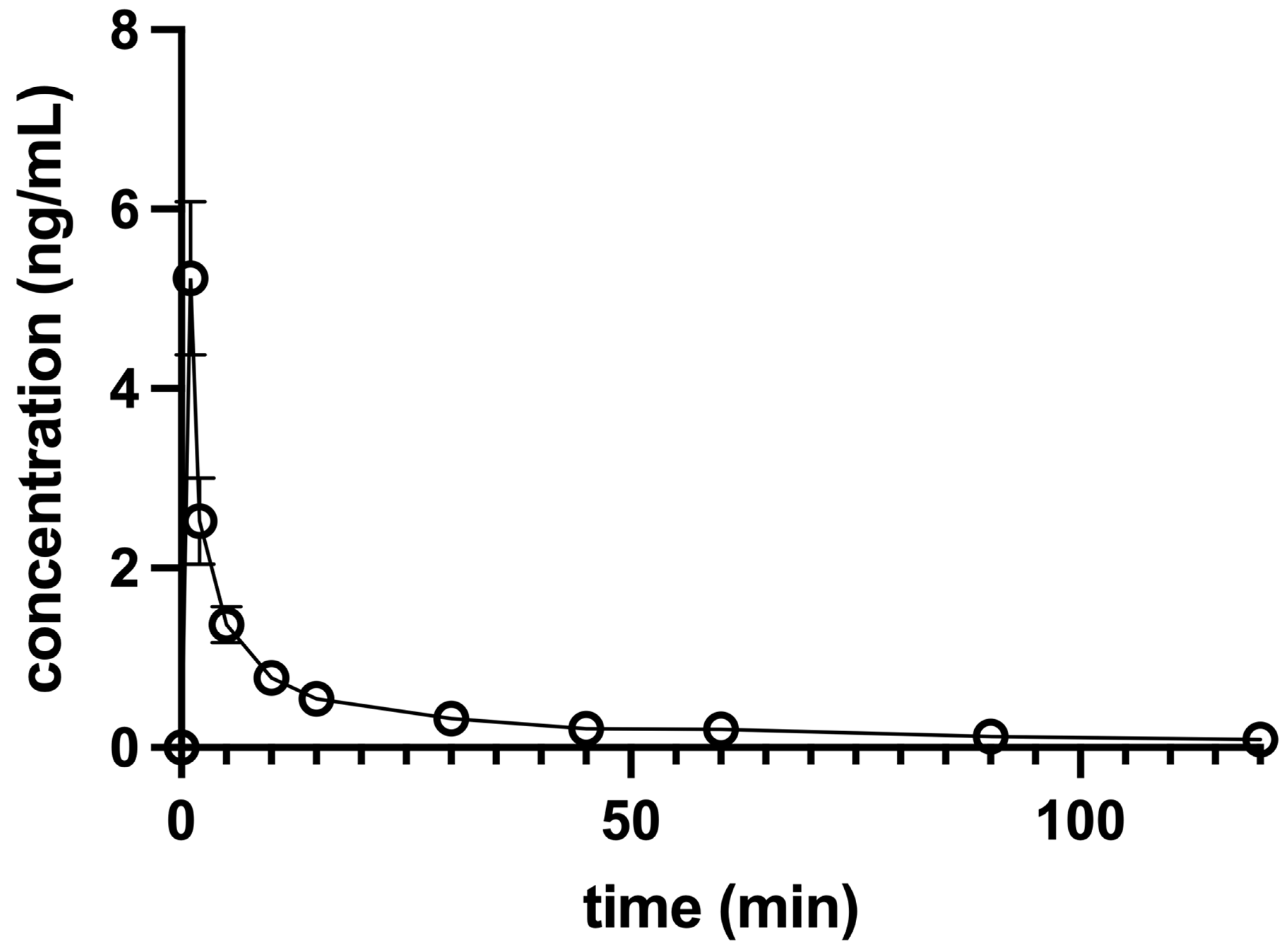
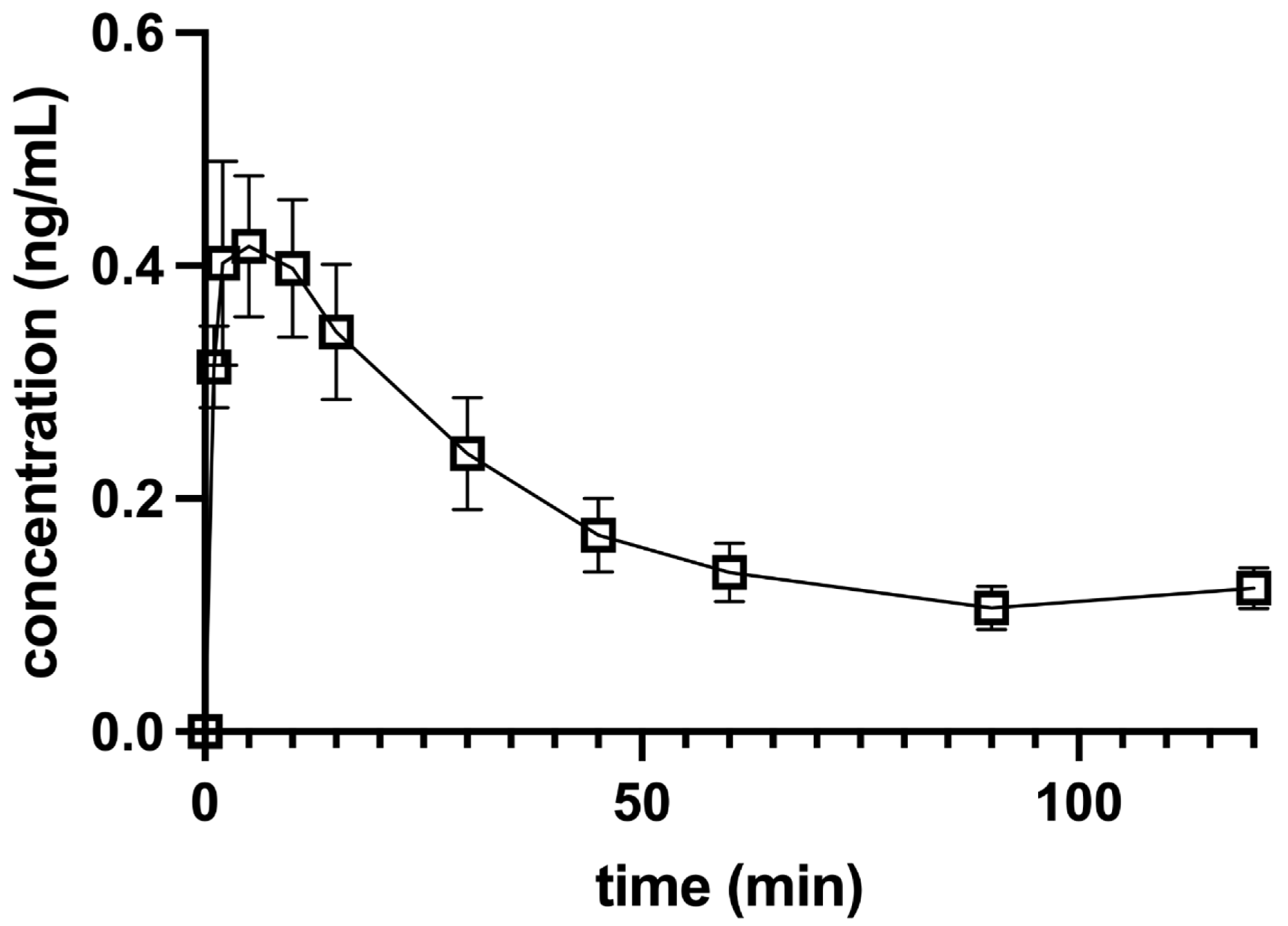
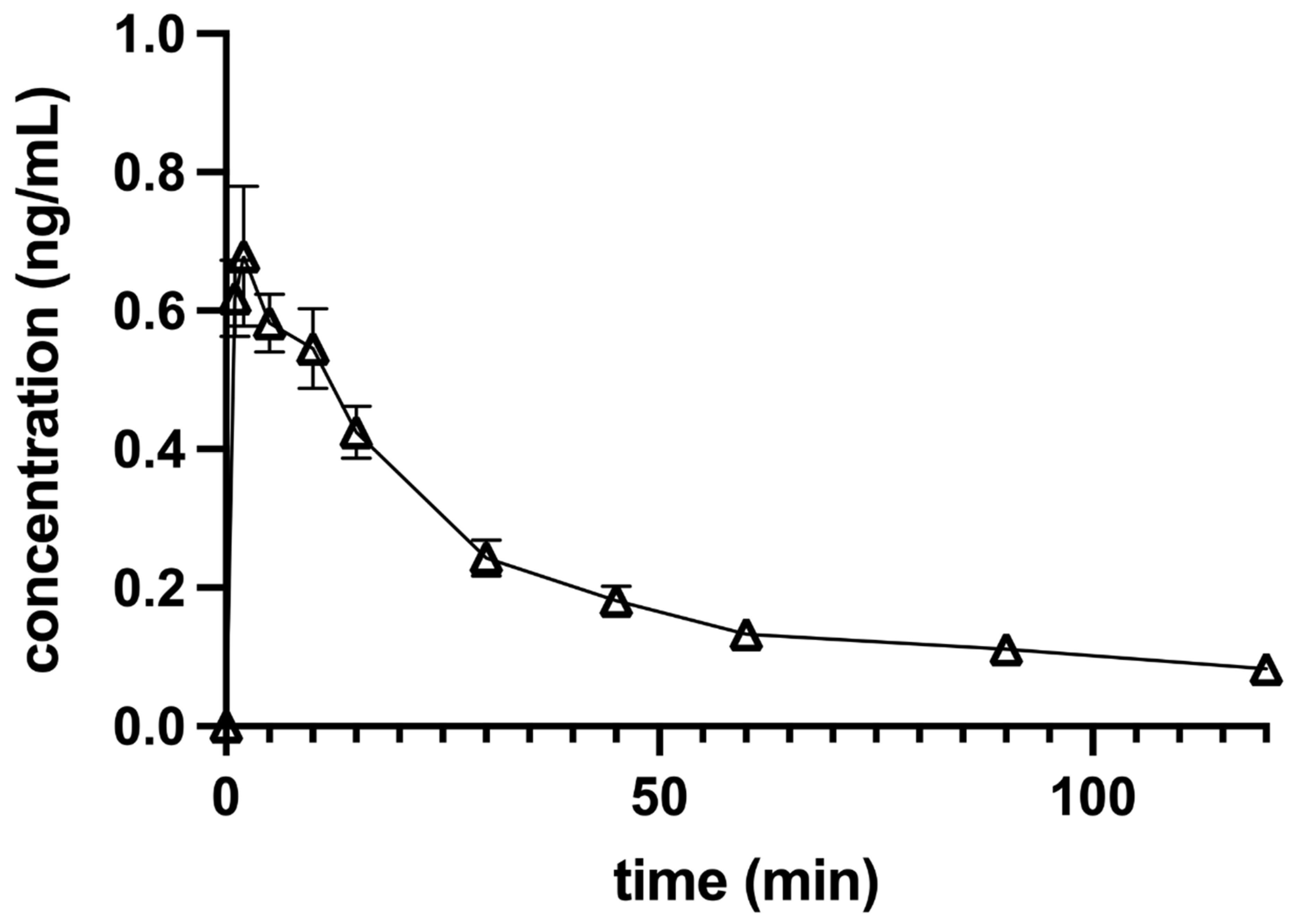
3.1. Pharmacokinetic Analysis
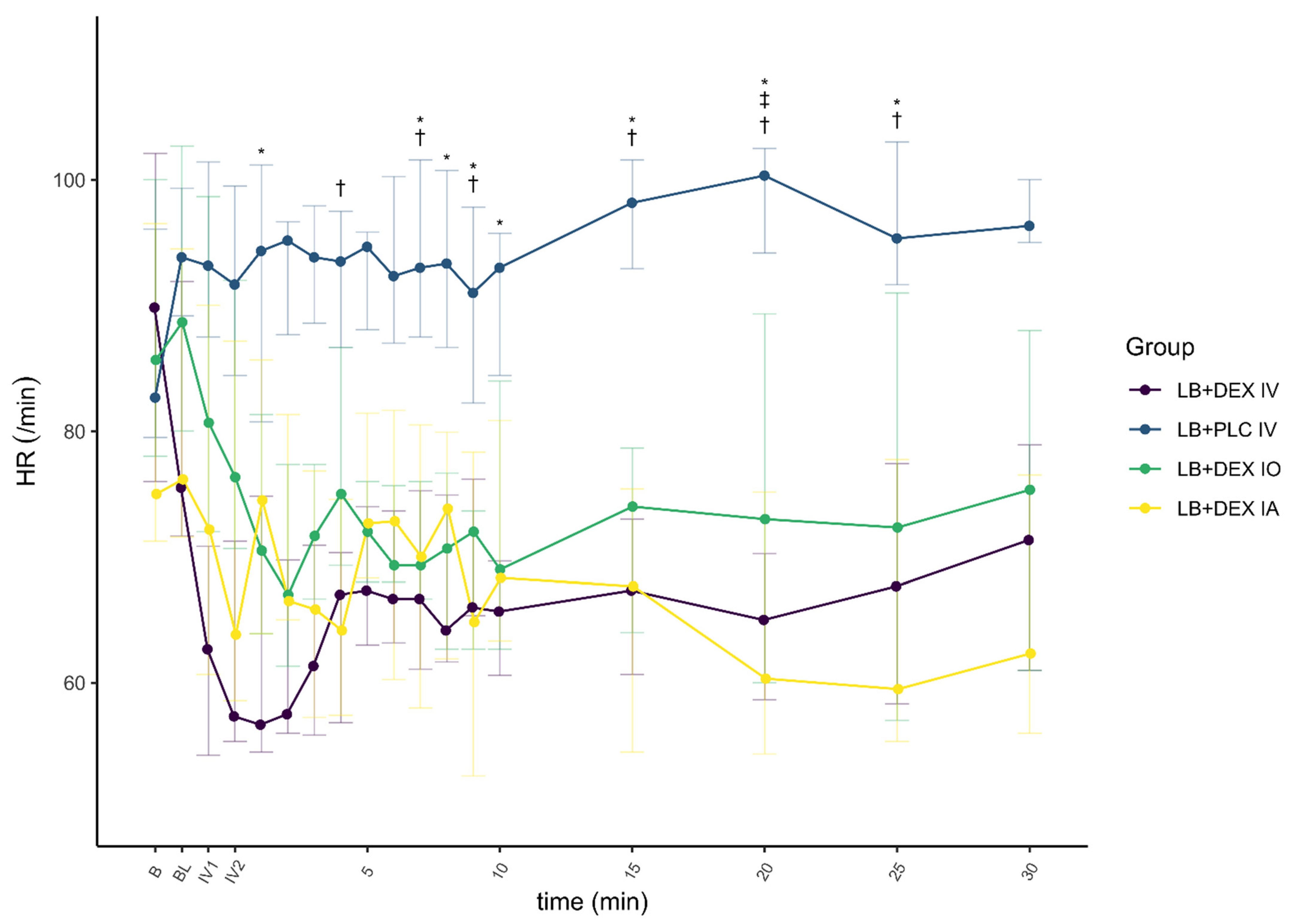
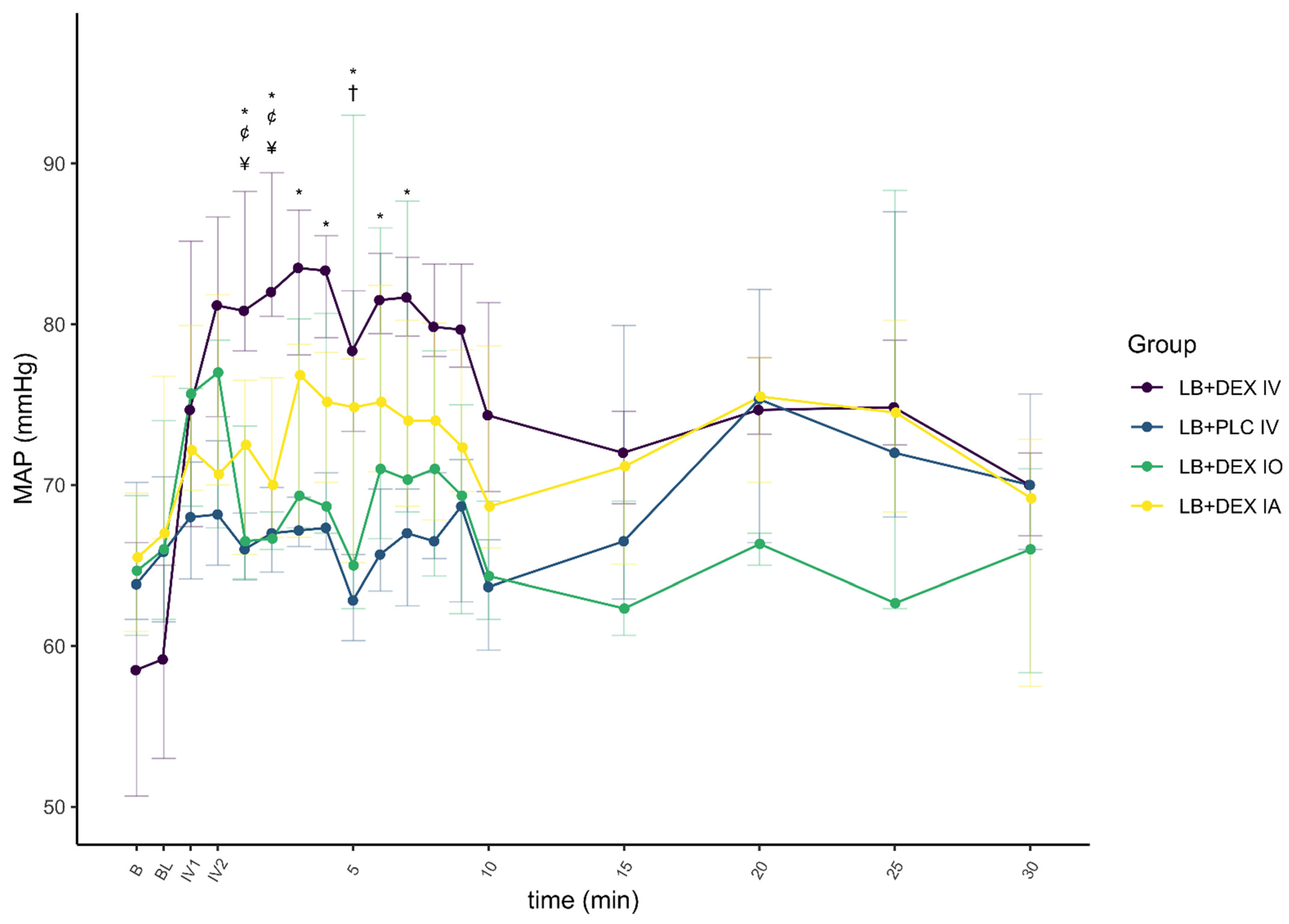
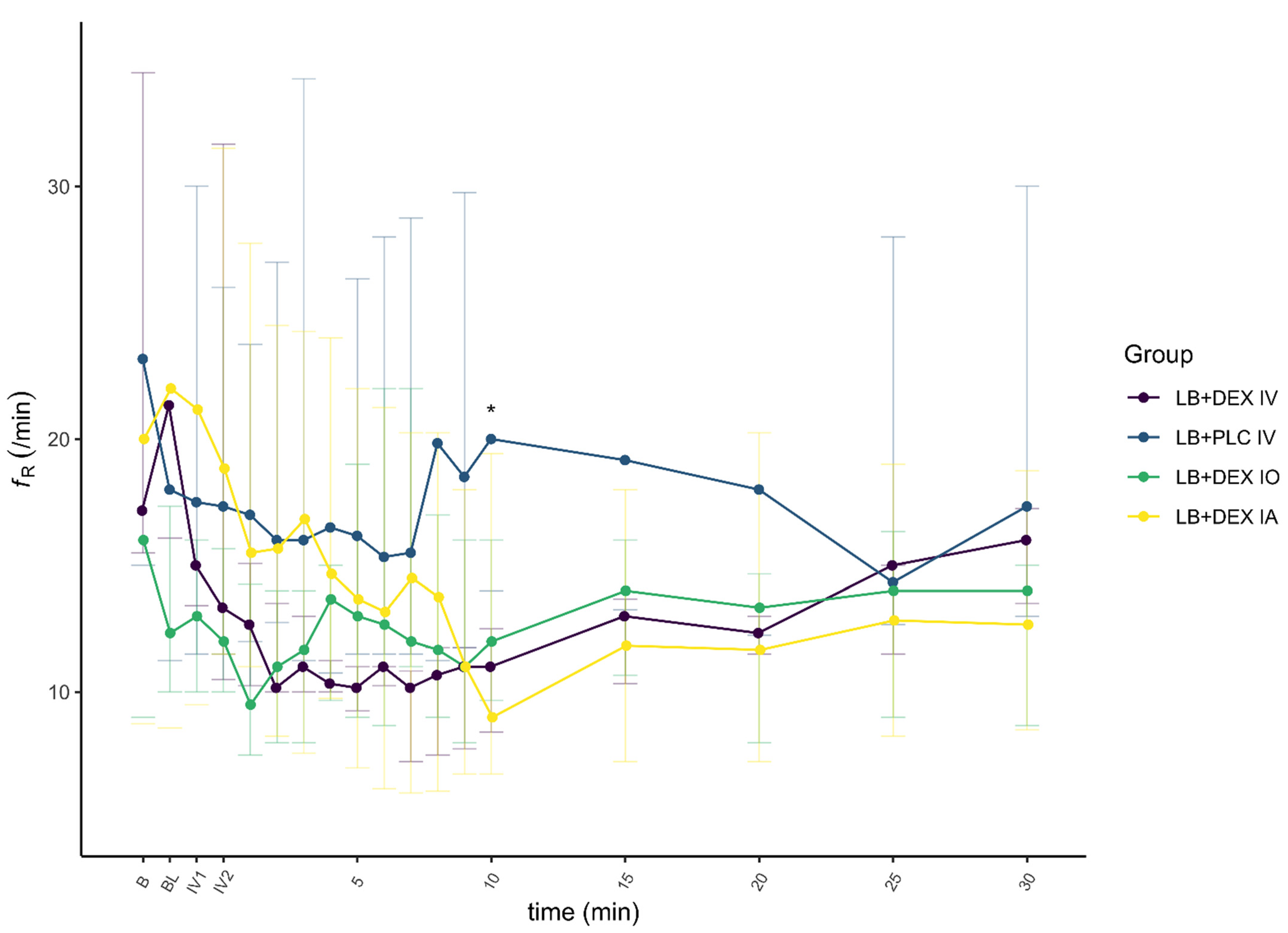
3.2. Pharmacodynamic Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aguiar, J.; Chebroux, A.; Martinez-Taboada, F.; Leece, E.A. Analgesic effects of maxillary and inferior alveolar nerve blocks in cats undergoing dental extractions. J. Feline Med. Surg. 2014, 17, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Benito, J.; Monteiro, B.; Lavoie, A.-M.; Beauchamp, G.; Lascelles, B.D.X.; Steagall, P.V. Analgesic efficacy of intraperitoneal administration of bupivacaine in cats. J. Feline Med. Surg. 2016, 18, 906–912. [Google Scholar] [CrossRef] [PubMed]
- Verstraete, F.J.M.; Lommer, M.J.; Arzi, B. Anaesthesia and Pain Management. In Oral and Maxillofacial Surgery in Dogs and Cats, 2nd ed.; Verstraete, F.J.M., Lommer, M.J., Arzi, B., Eds.; Elsevier: Berkeley, CA, USA, 2020; pp. 22–43. ISBN 9780702076756. [Google Scholar]
- Cicirelli, V.; Lacalandra, G.M.; Aiudi, G.G. The effect of splash block on the need for analgesia in dogs subjected to video-assisted ovariectomy. Vet. Med. Sci. 2021, 8, 104–109. [Google Scholar] [CrossRef]
- Castejón-González, A.C.; Reiter, A.M. Locoregional Anesthesia of the Head. Vet. Clin. Small Anim. Pract. 2019, 49, 1041–1061. [Google Scholar] [CrossRef] [PubMed]
- Alaman, M.; González-Marrón, A.; Lorente, C.; Bonastre, C.; Laborda, A. Description of an Ultrasound-Guided Transverse Approach to the Transversus Thoracis Plane Block and Evaluation of Injectate Spread in Canine Cadavers. Animals 2021, 11, 2657. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Taboada, F.; Sun, T.C.; Redondo, J.I. Onset of Action of Bupivacaine Administered via Dural Puncture Epidural versus Spinal, Lumbosacral, and Sacrococcygeal Epidural Injections in Dogs: Randomised Clinical Trial. Animals 2021, 11, 2996. [Google Scholar] [CrossRef]
- Cicirelli, V.; Debidda, P.; Maggio, N.; Caira, M.; Lacalandra, G.; Aiudi, G. Ultrasound-Guided Funicular Block: Ropivacaine Injection into the Tissue around the Spermatic Cord to Improve Analgesia during Orchiectomy in Dogs. Animals 2021, 11, 1275. [Google Scholar] [CrossRef]
- McLeod, G.A.; Burke, D. Levobupivacaine. Anaesthesia 2001, 56, 331–341. [Google Scholar] [CrossRef]
- Campoy, L.; Read, M.R. (Eds.) The thoracic limb. In Small Animal Regional Anesthesia and Analgesia; Willey-Blackwell: Malden, MA, USA, 2013; pp. 141–165. ISBN 9780813819945. [Google Scholar]
- Brummett, M.C.M.; Hong, B.E.K.; Janda, A.; Amodeo, B.F.S.; Lydic, R. Perineural Dexmedetomidine Added to Ropivacaine for Sciatic Nerve Block in Rats Prolongs the Duration of Analgesia by Blocking the Hyperpolarization-activated Cation Current. Anesthesiology 2011, 115, 836–843. [Google Scholar] [CrossRef] [Green Version]
- Brummett, M.C.M.; Padda, B.A.K.; Amodeo, B.F.S.; Welch, M.K.B.; Lydic, R. Perineural Dexmedetomidine Added to Ropivacaine Causes a Dose-dependent Increase in the Duration of Thermal Antinociception in Sciatic Nerve Block in Rat. Anesthesiology 2009, 111, 1111–1119. [Google Scholar] [CrossRef] [Green Version]
- Esmaoglu, A.; Yegenoglu, F.; Akin, A.; Turk, C.Y. Dexmedetomidine Added to Levobupivacaine Prolongs Axillary Brachial Plexus Block. Anesth. Analg. 2010, 111, 1548–1551. [Google Scholar] [CrossRef] [PubMed]
- Sarotti, D.; Rabozzi, R.; Franci, P. Effects of intravenous dexmedetomidine infusion on local anaesthetic block: A spinal anaesthesia clinical model in dogs undergoing hind limb surgery. Res. Vet. Sci. 2019, 124, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Tisotti, T.; Valverde, A.; Hopkins, A.; O’Sullivan, M.L.; Hanna, B.; Arroyo, L. Use of intravenous lidocaine to treat dexmedetomidine-induced bradycardia in sedated and anesthetized dogs. Vet. Anaesth. Analg. 2020, 48, 174–186. [Google Scholar] [CrossRef]
- Weerink, M.; Struys, M.M.R.F.; Hannivoort, L.N.; Barends, C.R.M.; Absalom, A.R.; Colin, P. Clinical Pharmacokinetics and Pharmacodynamics of Dexmedetomidine. Clin. Pharmacokinet. 2017, 56, 893–913. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuusela, E.; Raekallio, M.; Anttila, M.; Falck, I.; Mölsä, S.; Vainio, O.M. Clinical effects and pharmacokinetics of medetomidine and its enantiomers in dogs. J. Vet. Pharmacol. Ther. 2000, 23, 15–20. [Google Scholar] [CrossRef]
- Dent, B.T.; Aarnes, T.K.; Wavreille, V.; Lakritz, J.; Lerche, P.; KuKanich, B.; Pereira, C.H.R.; Bednarski, R.M. Pharmacokinetics and pharmacodynamic effects of oral transmucosal and intravenous administration of dexmedetomidine in dogs. Am. J. Vet. Res. 2019, 80, 969–975. [Google Scholar] [CrossRef]
- Viscasillas, J.; Seymour, C.J.; Brodbelt, D.C. A cadaver study comparing two approaches for performing maxillary nerve block in dogs. Vet. Anaesth. Analg. 2013, 40, 212–219. [Google Scholar] [CrossRef]
- Toutain, P.-L.; Bousquet-Melou, A. Plasma terminal half-life. J. Vet. Pharmacol. Ther. 2004, 27, 427–439. [Google Scholar] [CrossRef]
- European Medicines Agency. European Public Assessment Report. Available online: https://www.ema.europa.eu/en/documents/product-information/dexdomitor-epar-product-information_en.pdf (accessed on 30 January 2022).
- Di Cesare, F.; Gioeni, D.; Ravasio, G.; Pellegrini, A.; Lucatello, L.; Bisutti, V.; Villa, R.; Cagnardi, P. Clinical pharmacokinetics of a dexmedetomidine–methadone combination in dogs undergoing routine anaesthesia after buccal or intramuscular administration. J. Vet. Pharmacol. Ther. 2019, 42, 392–400. [Google Scholar] [CrossRef]
- Dutta, S.; Lal, R.; Karol, M.D.; Cohen, T.; Ebert, T. Influence of Cardiac Output on Dexmedetomidine Pharmacokinetics. J. Pharm. Sci. 2000, 89, 519–527. [Google Scholar] [CrossRef]
- Avram, M.J.; Krejcie, T.C.; Niemann, C.U.; Enders-Klein, C.; Shanks, C.A.; Henthorn, T.K. Isoflurane Alters the Recirculatory Pharmacokinetics of Physiologic Markers. Anesthesiology 2000, 92, 1757–1768. [Google Scholar] [CrossRef] [PubMed]
- Di Bella, C.; Skouropoulou, D.; Stabile, M.; Muresan, C.; Grasso, S.; Lacitignola, L.; Valentini, L.; Crovace, A.; Staffieri, F. Respiratory and hemodynamic effects of 2 protocols of low-dose infusion of dexmedetomidine in dogs under isoflurane anesthesia. Can. J. Vet. Res. 2020, 84, 96–107. [Google Scholar] [PubMed]
- Kersten, J.; Pagel, P.S.; Tessmer, J.P.; Roerig, D.L.; Schmeling, W.T.; Waritier, D.L. Dexmedetomidine Alters the Hemodynamic Effects of Desflurane and Isoflurane in Chronically Instrumented Dogs. Anesthesiology 1993, 79, 1022–1032. [Google Scholar] [CrossRef] [PubMed]
- Grasso, S.C.; Ko, J.C.; Weil, A.B.; Paranjape, V.; Constable, P.D. Hemodynamic influence of acepromazine or dexmedetomidine premedication in isoflurane-anesthetized dogs. J. Am. Vet. Med. Assoc. 2015, 246, 754–764. [Google Scholar] [CrossRef] [PubMed]
- Akashi, N.; Murahata, Y.; Hosokawa, M.; Hikasa, Y.; Okamoto, Y.; Imagawa, T. Cardiovascular and renal effects of constant rate infusions of remifentanil, dexmedetomidine and their combination in dogs anesthetized with sevoflurane. J. Vet. Med. Sci. 2021, 83, 285–296. [Google Scholar] [CrossRef]
- Kuusela, E.; Raekallio, M.; Hietanen, H.; Huttula, J.; Vainio, O. 24-hour Holter-Monitoring in the Perianaesthetic Period in Dogs Premedicated with Dexmedetomidine. Vet. J. 2002, 164, 235–239. [Google Scholar] [CrossRef]
- Congdon, J.M.; Marquez, M.; Niyom, S.; Boscan, P. Evaluation of the sedative and cardiovascular effects of intramuscular administration of dexmedetomidine with and without concurrent atropine administration in dogs. J. Am. Vet. Med. Assoc. 2011, 239, 81–89. [Google Scholar] [CrossRef]
- Murrell, J.C.; Hellebrekers, L.J. Medetomidine and dexmedetomidine: A review of cardiovascular effects and antinociceptive properties in the dog. Vet. Anaesth. Analg. 2005, 32, 117–127. [Google Scholar] [CrossRef]
- Pypendop, B.H.; Verstegen, J.P. Hemodynamic effects of medetomidine in the dog: A dose titration study. Vet. Surg. 1998, 27, 612–622. [Google Scholar] [CrossRef]
- Heppolette, C.A.A.; Brunnen, D.; Bampoe, S.; Odor, P.M. Clinical Pharmacokinetics and Pharmacodynamics of Levobupivacaine. Clin. Pharmacokinet. 2020, 59, 715–745. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Procedure |
|---|---|
| LB + DEX IV | EX of up to four teeth on R MAX, multi EX |
| LB + DEX IO | EX of up to four teeth on L MAN, EX of up to four teeth on L MAX |
| LB + DEX IA | 2 × multi EX |
| Group | Procedure |
|---|---|
| LB + DEX IV | 2 × EX of up to four teeth on R MAX, 2 × EX of up to four teeth on L MAX, 3 × EX of up to four teeth on L MAN, multi EX, GG on L + R MAN, PCP of C on R MAN |
| LB + PLC IV | 2 × EX of up to four teeth on L MAX, EX of up to four teeth on L MAN, 3 × multi EX, multi EX with full-mouth GG, PCP of C on L MAN, PCP of C on L + R MAN, ENDO of C on L MAX |
| LB + DEX IO | EX of up to four teeth on R MAX, 2 × EX of up to four teeth on L MAX, EX of up to four teeth on L + R MAX, EX of up to four teeth on L MAN, EX of up to four teeth on R MAN with IPP on L + R MAX, 2 × multi EX, PCP of C on L + R MAN, ENDO of C on L MAN |
| LB + DEX IA | EX of up to four teeth on R MAX, 2 × EX of up to four teeth on L + R MAX, EX of up to four teeth on L MAN, 2 x EX of up to four teeth on R MAN, 3 × multi EX, ENDO of C on L MAN |
| AUC(0→120) (ng/mL min) | VD (L/kg) | Cl (mL/min/kg) | |
|---|---|---|---|
| IV | 42.11 ± 5.01 | 0.12 ± 0.02 | 14.17 ± 1.58 |
| IO | 20.08 ± 3.82 * | NA | NA |
| IA | 23.78 ± 3.78 * | NA | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pavlica, M.; Kržan, M.; Nemec, A.; Kosjek, T.; Baš, A.; Seliškar, A. Cardiopulmonary Effects and Pharmacokinetics of Dexmedetomidine Used as an Adjunctive Analgesic to Regional Anesthesia of the Oral Cavity with Levobupivacaine in Dogs. Animals 2022, 12, 1217. https://0-doi-org.brum.beds.ac.uk/10.3390/ani12091217
Pavlica M, Kržan M, Nemec A, Kosjek T, Baš A, Seliškar A. Cardiopulmonary Effects and Pharmacokinetics of Dexmedetomidine Used as an Adjunctive Analgesic to Regional Anesthesia of the Oral Cavity with Levobupivacaine in Dogs. Animals. 2022; 12(9):1217. https://0-doi-org.brum.beds.ac.uk/10.3390/ani12091217
Chicago/Turabian StylePavlica, Matic, Mojca Kržan, Ana Nemec, Tina Kosjek, Anže Baš, and Alenka Seliškar. 2022. "Cardiopulmonary Effects and Pharmacokinetics of Dexmedetomidine Used as an Adjunctive Analgesic to Regional Anesthesia of the Oral Cavity with Levobupivacaine in Dogs" Animals 12, no. 9: 1217. https://0-doi-org.brum.beds.ac.uk/10.3390/ani12091217