Real Time In Vivo Confocal Microscopic Analysis of the Enamel Remineralization by Casein Phosphopeptide-Amorphous Calcium Phosphate (CPP-ACP): A Clinical Proof-of-Concept Study

 ,
,  , , , ,
, , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Featured Application
Abstract
1. Introduction
2. Patients, Materials and Methods
2.1. Patients
- Opacity, defined as a variation of the normal enamel translucence, clinically expressed by a white/creamy or yellow/brown discoloration, whose distribution may be linear, patchy or diffuse and with indistinct boundaries with the adjacent normal enamel.
- Hypoplasia, defined as a quantitative defect of the enamel, clinically expressed by areas of partial/total lack of enamel, rounded by smooth boundaries; the degree of enamel missing may correlate with the several clinical appearances: pits (tiny areas, single or multiple, shallow or deep, scattered or in rows); grooves/lines (single or multiple, narrow or wide until 2 mm in diameter/size); diffuse patch (wide areas, more than 2 mm in diameter/size, of partial/complete lack of enamel).
2.2. CPP-ACP Topical Application: Protocol
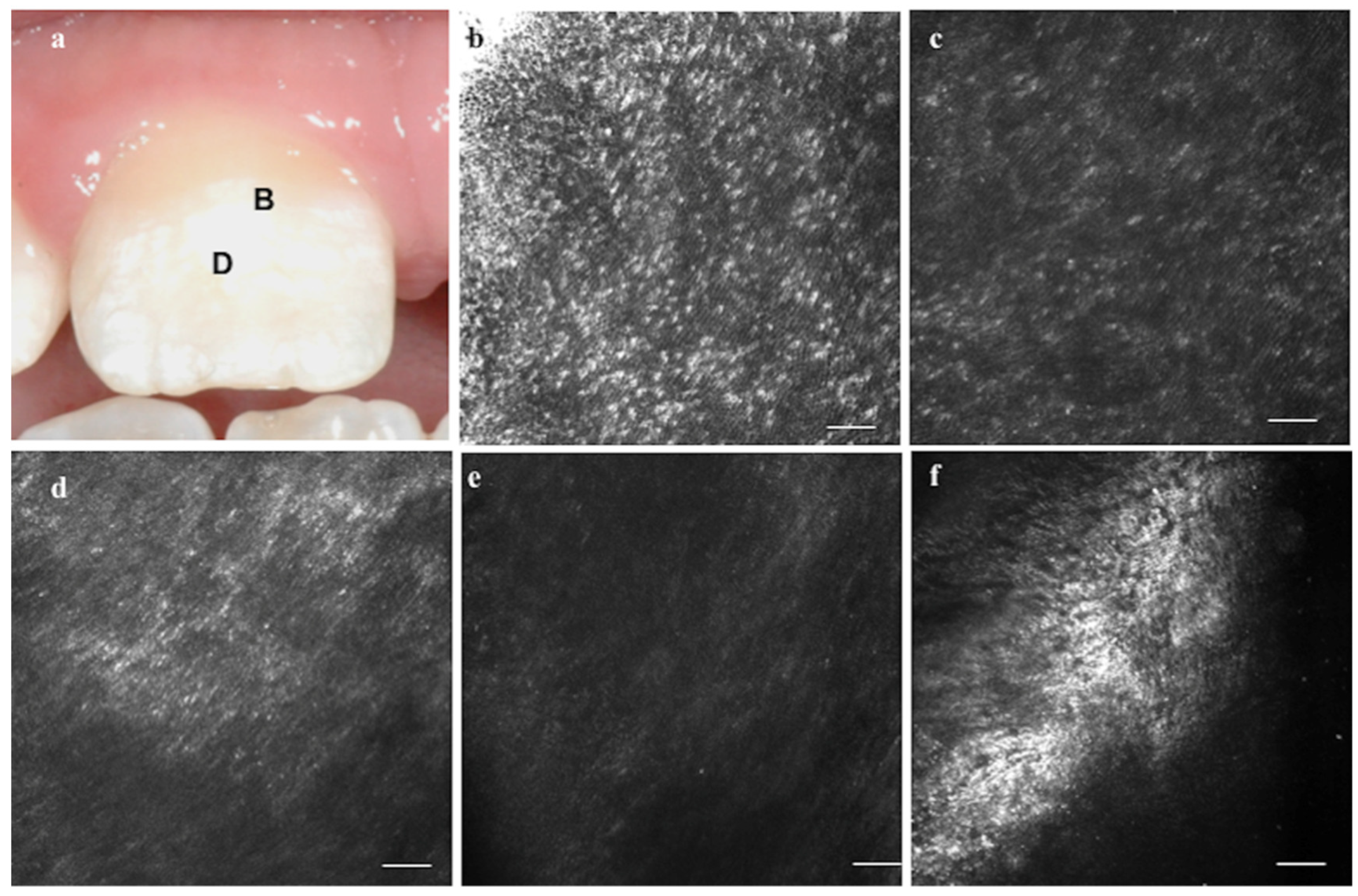
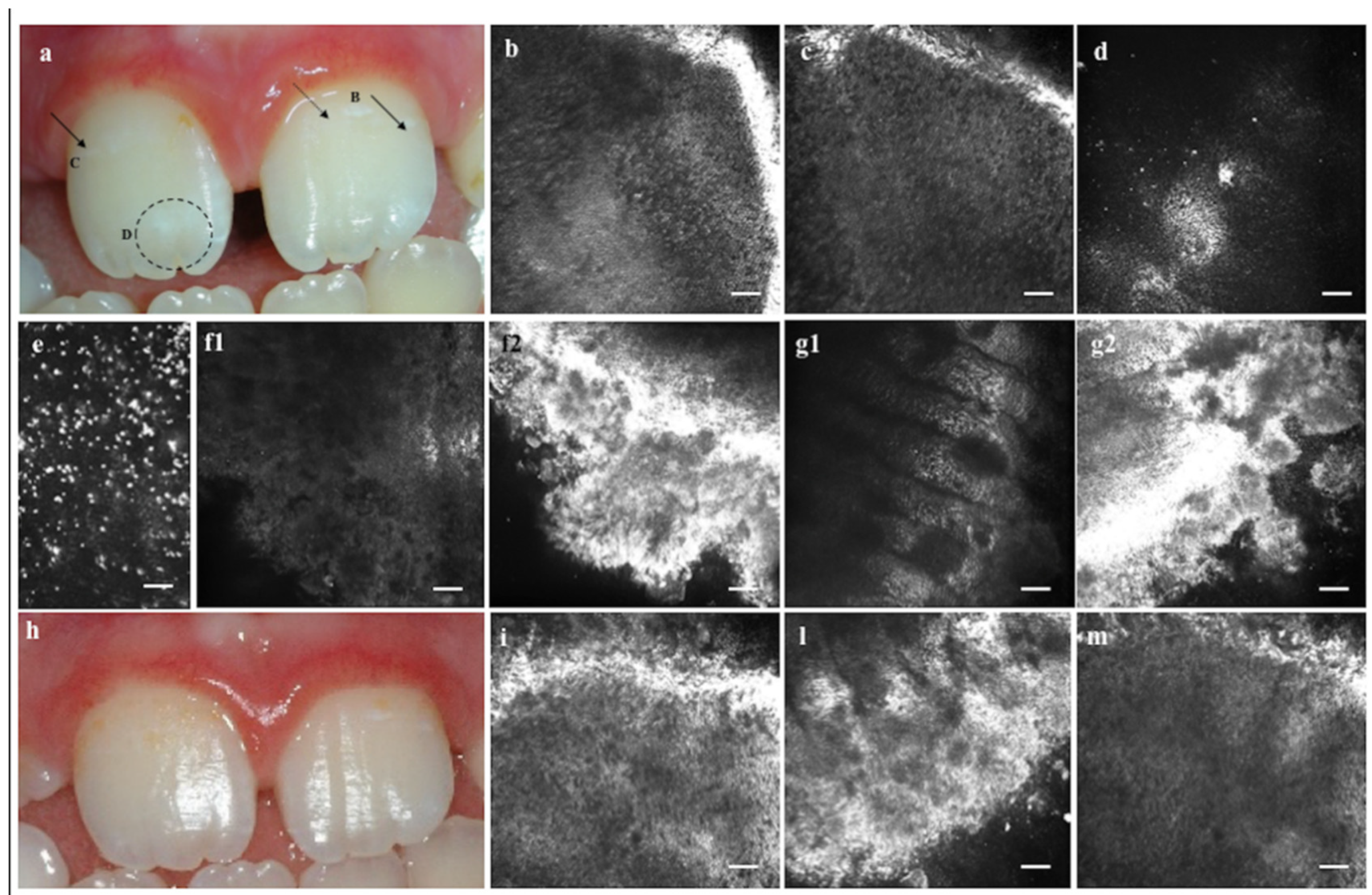
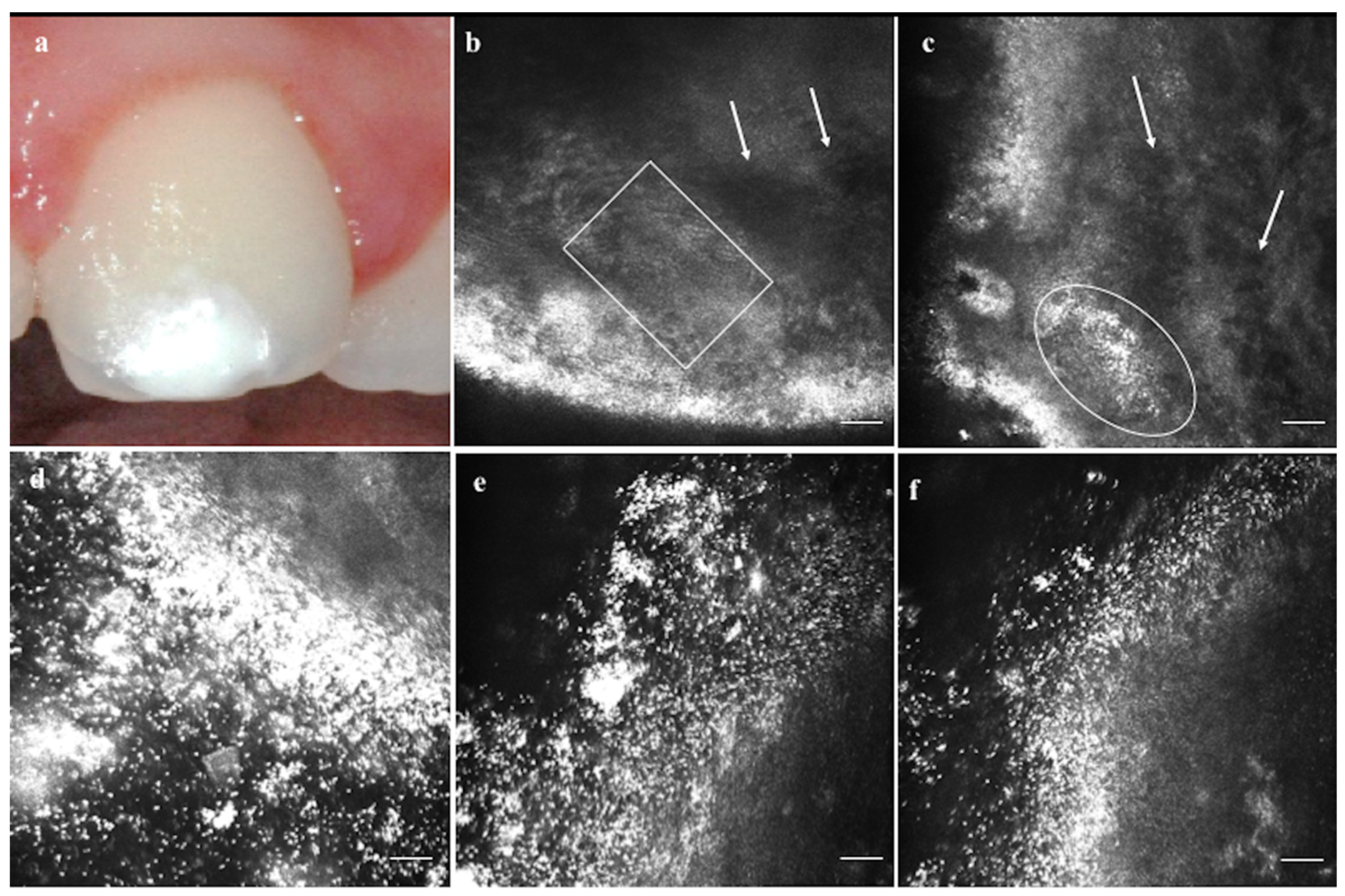
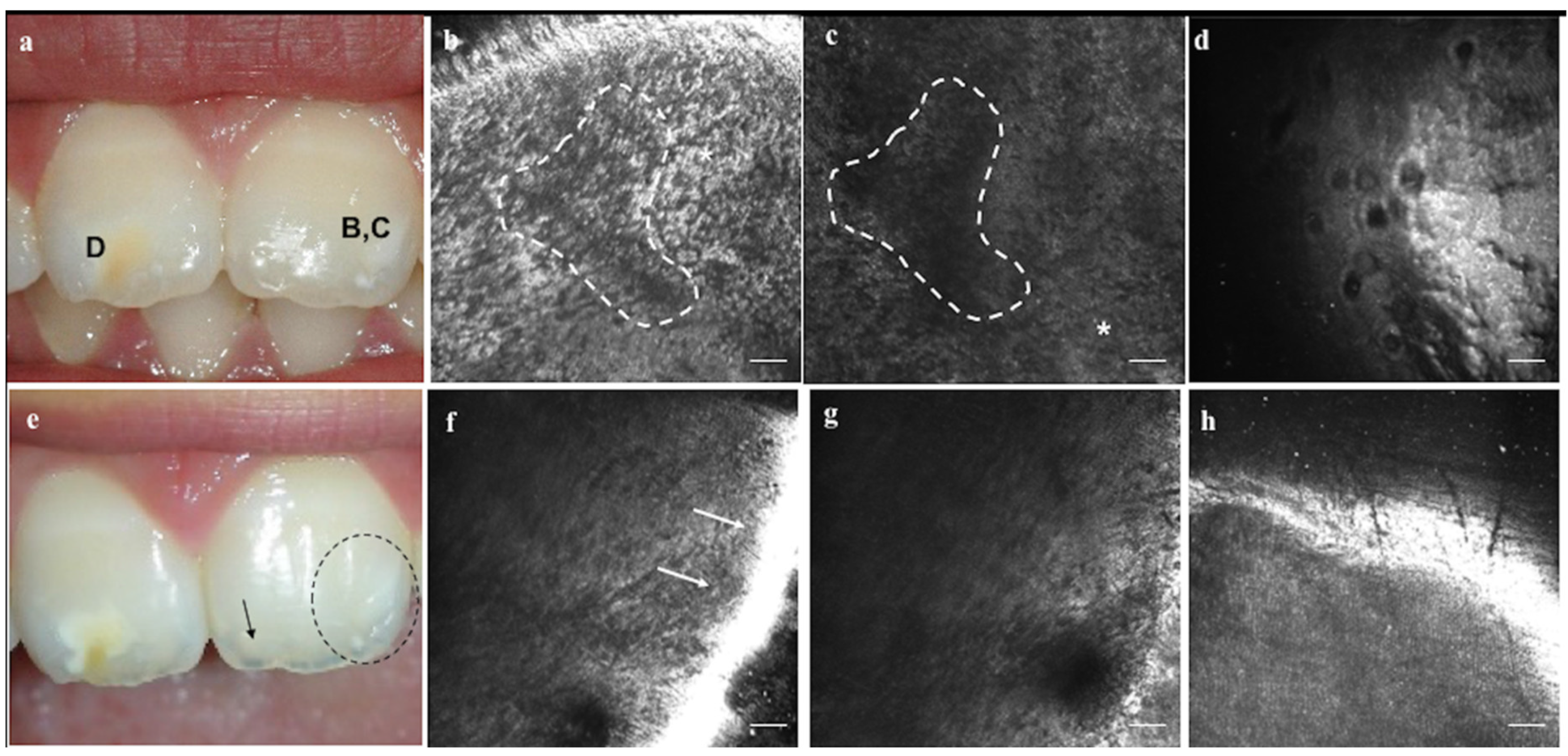
2.3. In Vivo Reflectance Confocal Laser Scanning Microscopy
3. Results
4. Discussion
Author Contributions
Funding
Conflicts of Interest
Ethics Approval
Consent to Participate
Consent for Publication
References
- Robles, M.J.; Ruiz, M.; Bravo-Perez, M.; González, E.; Peñalver, M.A. Prevalence of enamel defects in primary and permanent teeth in a group of schoolchildren from Granada (Spain). Med. Oral Patol. Oral Cir. Bucal. 2013, 18, e187–e193. [Google Scholar] [CrossRef]
- Contaldo, M.; Luzzi, V.; Ierardo, G.; Raimondo, E.; Boccellino, M.; Ferati, K.; Bexheti-Ferati, A.; Inchingolo, F.; Di Domenico, M.; Serpico, R.; et al. Bisphosphonate-related osteonecrosis of the jaws and dental surgery procedures in children and young people with osteogenesis imperfecta: A systematic review. J. Stomatol. Oral Maxillofac. Surg. 2020. [Google Scholar] [CrossRef]
- Commission on Oral Health Research & Epidemiology. A review of the developmental defects of enamel index (DDE Index). Commission on Oral Health, Research & Epidemiology. Report of an FDI Working Group. Int. Dent. J. 1992, 42, 411–426. [Google Scholar]
- Farah, R.A.; Monk, B.C.; Swain, M.V.; Drummond, B.K. Protein content of molar-incisor hypomineralisation enamel. J. Dent. 2010, 38, 591–596. [Google Scholar] [CrossRef]
- Vargas-Ferreira, F.; Salas, M.M.; Nascimento, G.G.; Tarquinio, S.B.; Faggion, C.M., Jr.; Peres, M.A.; Thomson, W.M.; Demarco, F.F. Association between developmental defects of enamel and dental caries: A systematic review and meta-analysis. J. Dent. 2015, 43, 619–628. [Google Scholar] [CrossRef]
- Gupta, T.; Sadana, G.; Rai, H.K. Effect of Esthetic Defects in Anterior Teeth on the Emotional and Social Well-being of Children: A Survey. Int. J. Clin. Pediatr. Dent. 2019, 12, 229–232. [Google Scholar]
- Mony, S.; Rao, A.; Shenoy, R.; Suprabha, B.S. Comparative evaluation of the remineralizing efficacy of calcium sodium phosphosilicate agent and fluoride based on quantitative and qualitative analysis. J. Indian Soc. Pedod. Prev. Dent. 2015, 33, 291–295. [Google Scholar]
- Esteves-Oliveira, M.; Witulski, N.; Hilgers, R.D.; Apel, C.; Meyer-Lueckel, H.; Eduardo Cde, P. Combined Tin-Containing Fluoride Solution and CO2 Laser Treatment Reduces Enamel Erosion in vitro. Caries Res. 2015, 49, 565–574. [Google Scholar] [CrossRef]
- Rirattanapong, P.; Vongsavan, K.; Saengsirinavin, C.; Phuekcharoen, P. Efficacy of fluoride mouthrinse containing tricalcium phosphate on primary enamel lesions: A polarized light microscopic study. Southeast Asian J. Trop. Med. Public Health 2015, 46, 168–174. [Google Scholar]
- Lv, X.; Yang, Y.; Han, S.; Li, D.; Tu, H.; Li, W.; Zhou, X.; Zhang, L. Potential of an amelogenin based peptide in promoting reminerlization of initial enamel caries. Arch. Oral Biol. 2015, 60, 1482–1487. [Google Scholar] [CrossRef]
- Iafisco, M.; Degli Esposti, L.; Ramírez-Rodríguez, G.B.; Carella, F.; Gómez-Morales, J.; Ionescu, A.C.; Brambilla, E.; Tampieri, A.; Delgado-López, J.M. Fluoride-doped amorphous calcium phosphate nanoparticles as a promising biomimetic material for dental remineralization. Sci. Rep. 2018, 8, 17016. [Google Scholar] [CrossRef] [PubMed]
- Kumar, K.; Sreedharan, S. Comparative Evaluation of the Remineralization Potential of Monofluorophosphate, Casein Phosphopeptide-Amorphous Calcium Phosphate and Calcium Sodium Phosphosilicate on Demineralized Enamel Lesions: An In Vitro Study. Cureus 2018, 10, e3059. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, L.; Geng, K.; Gao, Q. Early Caries Preventive Effects of Casein Phosphopeptide-Amorphous Calcium Phosphate (CPP-ACP) Compared with Conventional Fluorides: A Meta-analysis. Oral Health Prev. Dent. 2019, 17, 495–503. [Google Scholar] [PubMed]
- Bakry, A.S.; Abbassy, M.A. Increasing the efficiency of CPP-ACP to remineralize enamel white spot lesions. J. Dent. 2018, 76, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Huq, N.L.; Myroforidis, H.; Cross, K.J.; Stanton, D.P.; Veith, P.D.; Ward, B.R.; Reynolds, E.C. The Interactions of CPP-ACP with Saliva. Int. J. Mol. Sci. 2016, 17, E915. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lucchese, A.; Pilolli, G.P.; Petruzzi, M.; Crincoli, V.; Scivetti, M.; Favia, G. Analysis of collagen distribution in human crown dentin by confocal laser scanning microscopy. Ultrastruct. Pathol. 2008, 32, 107–111. [Google Scholar] [CrossRef]
- Scivetti, M.; Pilolli, G.P.; Corsalini, M.; Lucchese, A.; Favia, G. Confocal laser scanning microscopy of human cementocytes: Analysis of three-dimensional image reconstruction. Ann. Anat. 2007, 189, 169–174. [Google Scholar] [CrossRef]
- Llena, C.; Esteve, I.; Rodríguez-Lozano, F.J.; Forner, L. The application of casein phosphopeptide and amorphous calcium phosphate with fluoride (CPP-ACPF) for restoring mineral loss after dental bleaching with hydrogen or carbamide peroxide: An in vitro study. Ann. Anat. 2019, 225, 48–53. [Google Scholar] [CrossRef]
- Angelini Sfalcin, R.; da Silva, J.V.P.; Oliva Pessoa, V.; Santos, J.; Garcia Olivan, S.R.; Porta Santos Fernandes, K.; Melo Deana, A.; Makeeva, I.; Sauro, S.; Kalil Bussadori, S. Remineralization of early enamel caries lesions induced by bioactive particles: An in vitro speckle analysis. Photodiagnosis Photodyn. Ther. 2019, 28, 201–209. [Google Scholar] [CrossRef]
- Schwendicke, F.; Al-Abdi, A.; Pascual Moscardó, A.; Ferrando Cascales, A.; Sauro, S. Remineralization effects of conventional and experimental ion-releasing materials in chemically or bacterially-induced dentin caries lesions. Dent. Mater. 2019, 35, 772–779. [Google Scholar] [CrossRef]
- Ferrazzano, G.F.; Amato, I.; Cantile, T.; Sangianantoni, G.; Ingenito, A. In vivo remineralising effect of GC tooth mousse on early dental enamel lesions: SEM analysis. Int. Dent. J. 2011, 61, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Moscarella, E.; González, S.; Agozzino, M.; Sánchez-Mateos, J.L.; Panetta, C.; Contaldo, M.; Ardigò, M. Pilot study on reflectance confocal microscopy imaging of lichen planus: A real-time, non-invasive aid for clinical diagnosis. J. Eur. Acad. Dermatol. Venereol. 2012, 26, 1258–1265. [Google Scholar] [CrossRef] [PubMed]
- Gareau, D.S.; Patel, Y.G.; Rajadhyaksha, M. Introduction to Reflectance Confocal Microscopy. In Reflectance Confocal Microscopy of Cutaneous Tumors: An Atlas with Clinical, Dermoscopic and Histological Correlations; Gonzales, S., Gill, M., Halpern, A.C., Eds.; Informa Healthcare: London, UK, 2008; pp. 1–3. [Google Scholar]
- Rajadhyaksha, M.; Grossman, M.; Esterowitz, D.; Webb, R.H.; Anderson, R.R. In vivo confocal scanning laser microscopy of human skin: Melanin provides strong contrast. J. Investig. Dermatol. 1995, 104, 946–952. [Google Scholar] [CrossRef] [Green Version]
- Ulrich, M.; Roewert-Huber, J.; González, S.; Rius-Diaz, F.; Stockfleth, E.; Kanitakis, J. Peritumoral clefting in basal cell carcinoma: Correlation of in vivo reflectance confocal microscopy and routine histology. J. Cutan. Pathol. 2011, 38, 190–195. [Google Scholar] [CrossRef]
- Lucchese, A.; Gentile, E.; Romano, A.; Maio, C.; Laino, L.; Serpico, R. The potential role of in vivo reflectance confocal microscopy for evaluating oral cavity lesions: A systematic review. J. Oral Pathol. Med. 2016, 45, 723–729. [Google Scholar] [CrossRef]
- Contaldo, M.; Poh, C.F.; Guillaud, M.; Lucchese, A.; Rullo, R.; Lam, S.; Serpico, R.; MacAulay, C.E.; Lane, P.M. Oral mucosa optical biopsy by a novel handheld fluorescent confocal microscope specifically developed: Technologic improvements and future prospects. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 116, 752–758. [Google Scholar] [CrossRef]
- Contaldo, M.; Agozzino, M.; Moscarella, E.; Esposito, S.; Serpico, R.; Ardigò, M. In vivo characterization of healthy oral mucosa by reflectance confocal microscopy: A translational research for optical biopsy. Ultrastruct. Pathol. 2013, 37, 151–158. [Google Scholar] [CrossRef]
- Contaldo, M.; Agozzino, M.; Ardigò, M. In vivo reflectance confocal microscopy for oral mucosa assessment. In Non Invasive Diagnostic Techniques in Clinical Dermatology; Berardesca, E., Maibach, H., Wilhelm, K., Eds.; Springer: Berlin/Heidelberg, Germany, 2014; pp. 81–87. [Google Scholar]
- Alessi, S.S.; Nico, M.M.; Fernandes, J.D.; Lourenço, S.V. Reflectance confocal microscopy as a new tool in the in vivo evaluation of desquamative gingivitis: Patterns in mucous membrane pemphigoid, pemphigus vulgaris and oral lichen planus. Br. J. Dermatol. 2013, 168, 257–264. [Google Scholar] [CrossRef]
- Contaldo, M.; Di Stasio, D.; Petruzzi, M.; Serpico, R.; Lucchese, A. In vivo reflectance confocal microscopy of oral lichen planus. Int. J. Dermatol. 2019, 58, 940–945. [Google Scholar] [CrossRef]
- Contaldo, M.; Lajolo, C.; Di Petrillo, M.; Ballini, A.; Inchingolo, F.; Serpico, R.; Romano, A. Analysis of lip pigmentations by reflectance confocal microscopy: Report of two cases. J. Biol. Regul. Homeost. Agents 2019, 33, 19–25. [Google Scholar]
- Romano, A.; Santarelli, A.; Lajolo, C.; Della Vella, F.; Mascitti, M.; Serpico, R.; Contaldo, M. Analysis of oral mucosa erosive-ulcerative lesions by reflectance confocal microscopy. J. Biol. Regul. Homeost. Agents 2019, 33, 11–17. [Google Scholar] [PubMed]
- Contaldo, M.; Lauritano, D.; Carinci, F.; Romano, A.; Di Stasio, D.; Lajolo, C.; Della Vella, F.; Serpico, R.; Lucchese, A. Intraoral confocal microscopy of suspicious oral lesions: A prospective case series. Int. J. Dermatol. 2020, 59, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Contaldo, M.; Serpico, R.; Lucchese, A. In vivo imaging of enamel by reflectance confocal microscopy (RCM): Non-invasive analysis of dental surface. Odontology 2014, 102, 325–329. [Google Scholar] [CrossRef] [PubMed]
- Gentile, E.; Di Stasio, D.; Santoro, R.; Contaldo, M.; Salerno, C.; Serpico, R.; Lucchese, A. In vivo microstructural analysis of enamel in permanent and deciduous teeth. Ultrastruct. Pathol. 2015, 39, 131–134. [Google Scholar] [CrossRef] [Green Version]
- Contaldo, M.; Di Stasio, D.; Santoro, R.; Laino, L.; Perillo, L.; Petruzzi, M.; Lauritano, D.; Serpico, R.; Lucchese, A. Non-invasive in vivo visualization of enamel defects by reflectance confocal microscopy (RCM). Odontology 2015, 103, 177–184. [Google Scholar] [CrossRef]
- Ghanim, A.; Elfrink, M.; Weerheijm, K.; Mariño, R.; Manton, D. A practical method for use in epidemiological studies on enamel hypomineralisation. Eur. Arch. Paediatr. Dent. 2015, 16, 235–246. [Google Scholar] [CrossRef] [Green Version]
- Moura-Netto, C.; Mello-Moura, A.C.; Palo, R.M.; Prokopowitsch, I.; Pameijer, C.H.; Marques, M.M. Adaptation and penetration of resin-based root canal sealers in root canals irradiated with high-intensity lasers. J. Biomed. Opt. 2015, 20, 038002. [Google Scholar] [CrossRef] [Green Version]
- Marzuki, A.F.; Masudi, S.M. Confocal laser scanning microscopy study of dentinal tubules in dental caries stained with alizarin red. Arch. Orofac. Sci. 2008, 3, 2–6. [Google Scholar]




© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Contaldo, M.; Di Stasio, D.; della Vella, F.; Lauritano, D.; Serpico, R.; Santoro, R.; Lucchese, A. Real Time In Vivo Confocal Microscopic Analysis of the Enamel Remineralization by Casein Phosphopeptide-Amorphous Calcium Phosphate (CPP-ACP): A Clinical Proof-of-Concept Study. Appl. Sci. 2020, 10, 4155. https://0-doi-org.brum.beds.ac.uk/10.3390/app10124155
Contaldo M, Di Stasio D, della Vella F, Lauritano D, Serpico R, Santoro R, Lucchese A. Real Time In Vivo Confocal Microscopic Analysis of the Enamel Remineralization by Casein Phosphopeptide-Amorphous Calcium Phosphate (CPP-ACP): A Clinical Proof-of-Concept Study. Applied Sciences. 2020; 10(12):4155. https://0-doi-org.brum.beds.ac.uk/10.3390/app10124155
Chicago/Turabian StyleContaldo, Maria, Dario Di Stasio, Fedora della Vella, Dorina Lauritano, Rosario Serpico, Rossella Santoro, and Alberta Lucchese. 2020. "Real Time In Vivo Confocal Microscopic Analysis of the Enamel Remineralization by Casein Phosphopeptide-Amorphous Calcium Phosphate (CPP-ACP): A Clinical Proof-of-Concept Study" Applied Sciences 10, no. 12: 4155. https://0-doi-org.brum.beds.ac.uk/10.3390/app10124155