A New Approach to Set the Absolute Midsagittal Plane of the Mandible Using a Similarity Index in Skeletal Class III Patients with Facial Asymmetry




Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Surgical and Orthodontic Treatment
2.3. Data Acquisition, 3D Landmark Determination, and Image Reorientation
2.4. Morphological Operation of Mandible
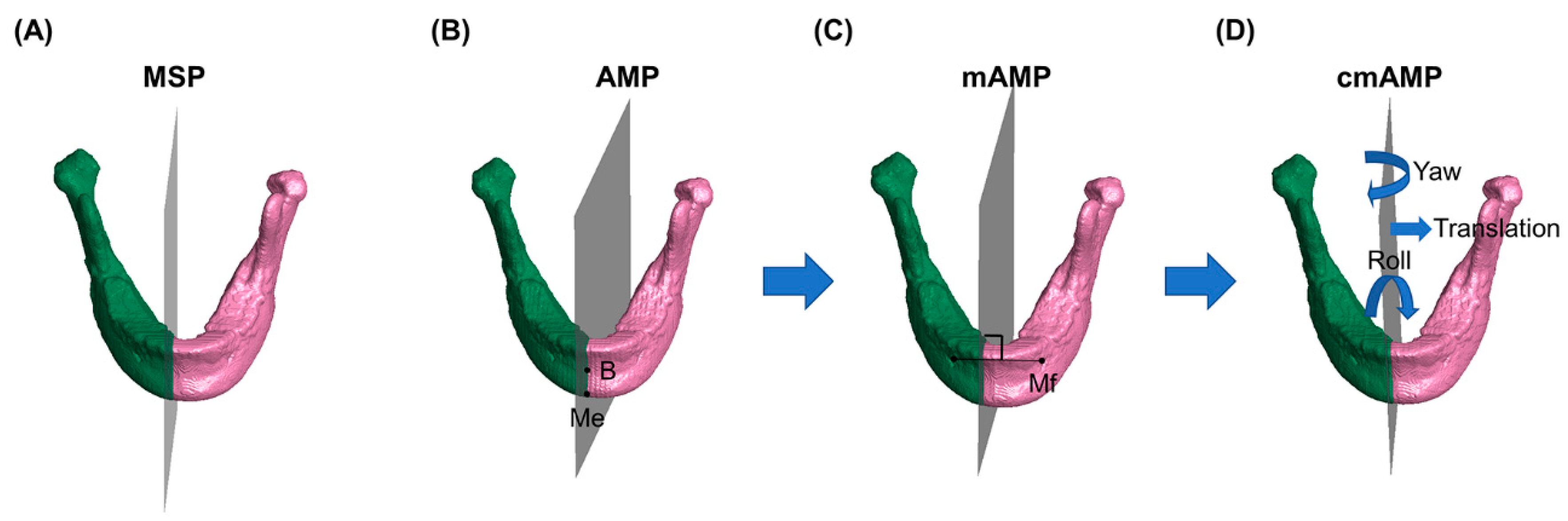
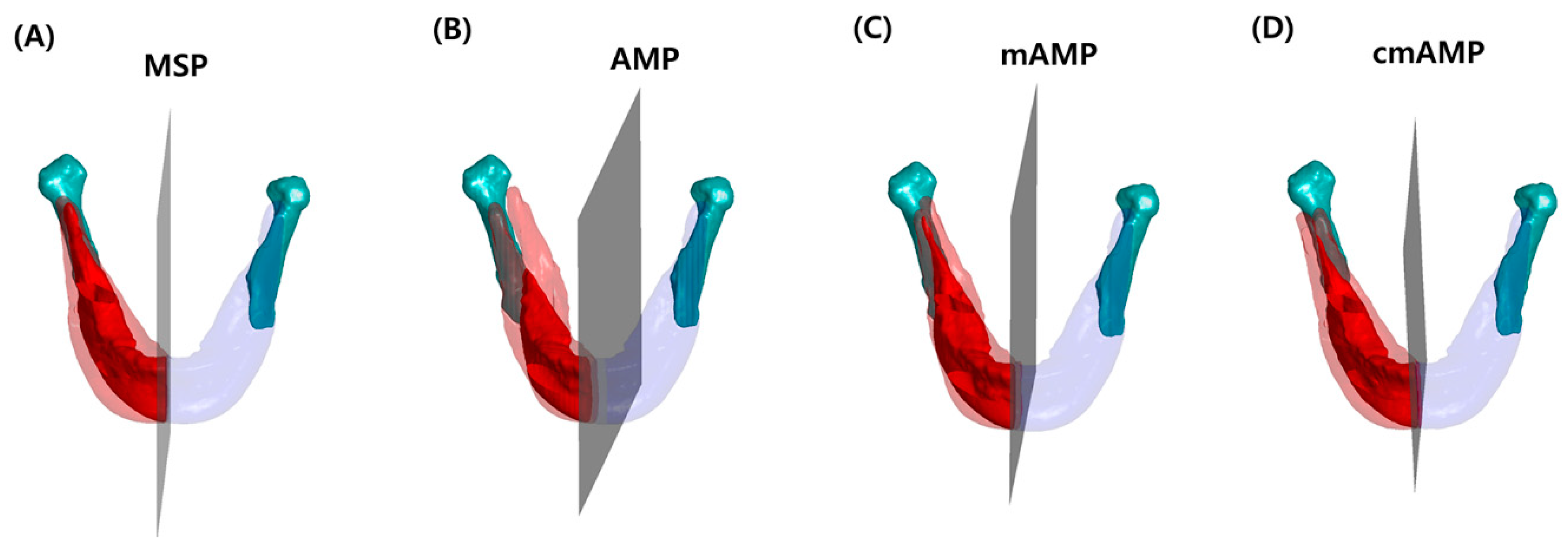
2.5. AMP, mAMP, cmAMP Assessments
2.6. Non-Overlapping Surface, Volume, and SI with Each Mandibular Midsagittal Plane
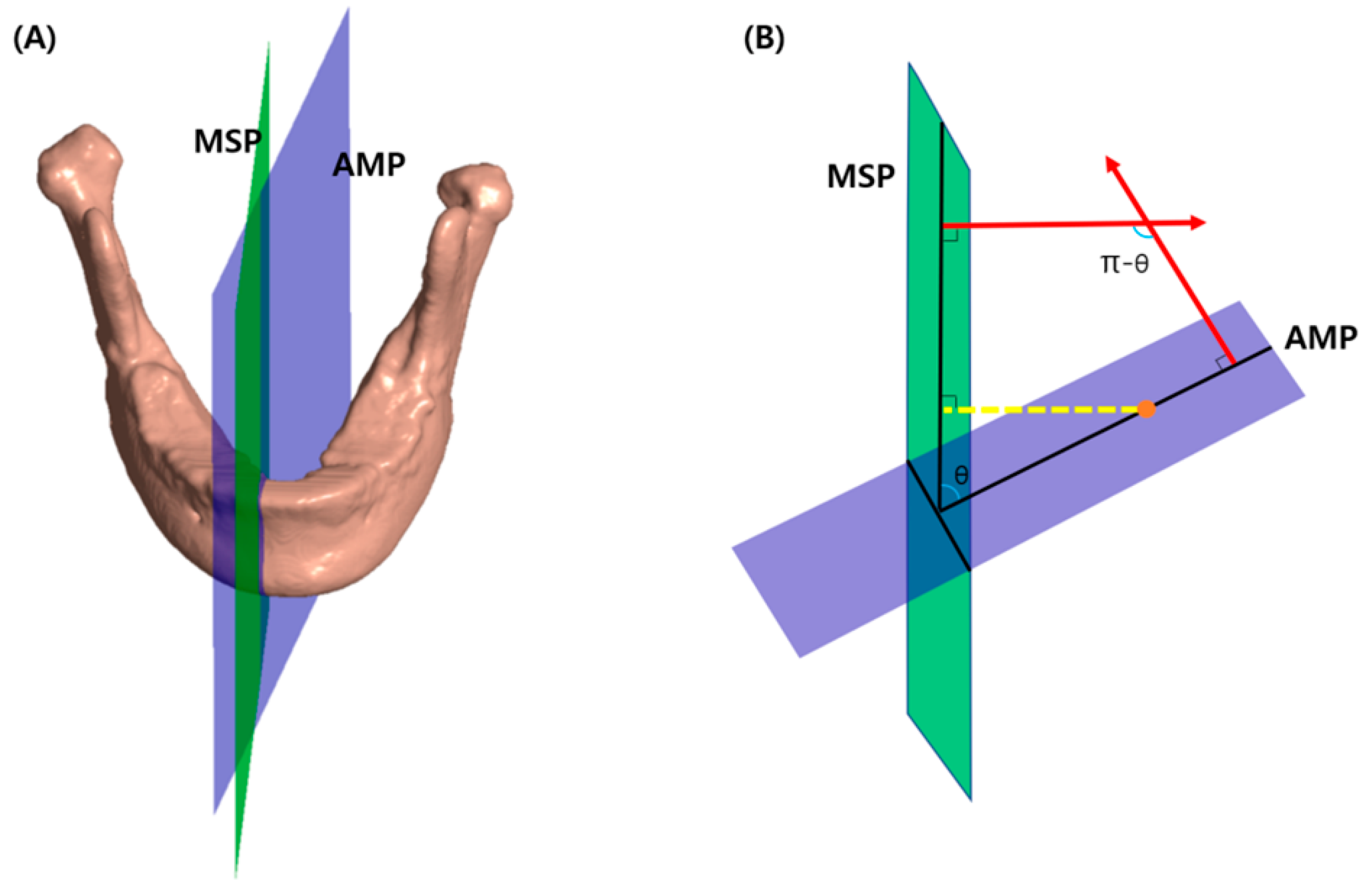
2.7. Angle and Distance between MSP and Each Midsagittal Plane of the Mandible
2.8. Reliability
2.9. Statistical Analysis
3. Results
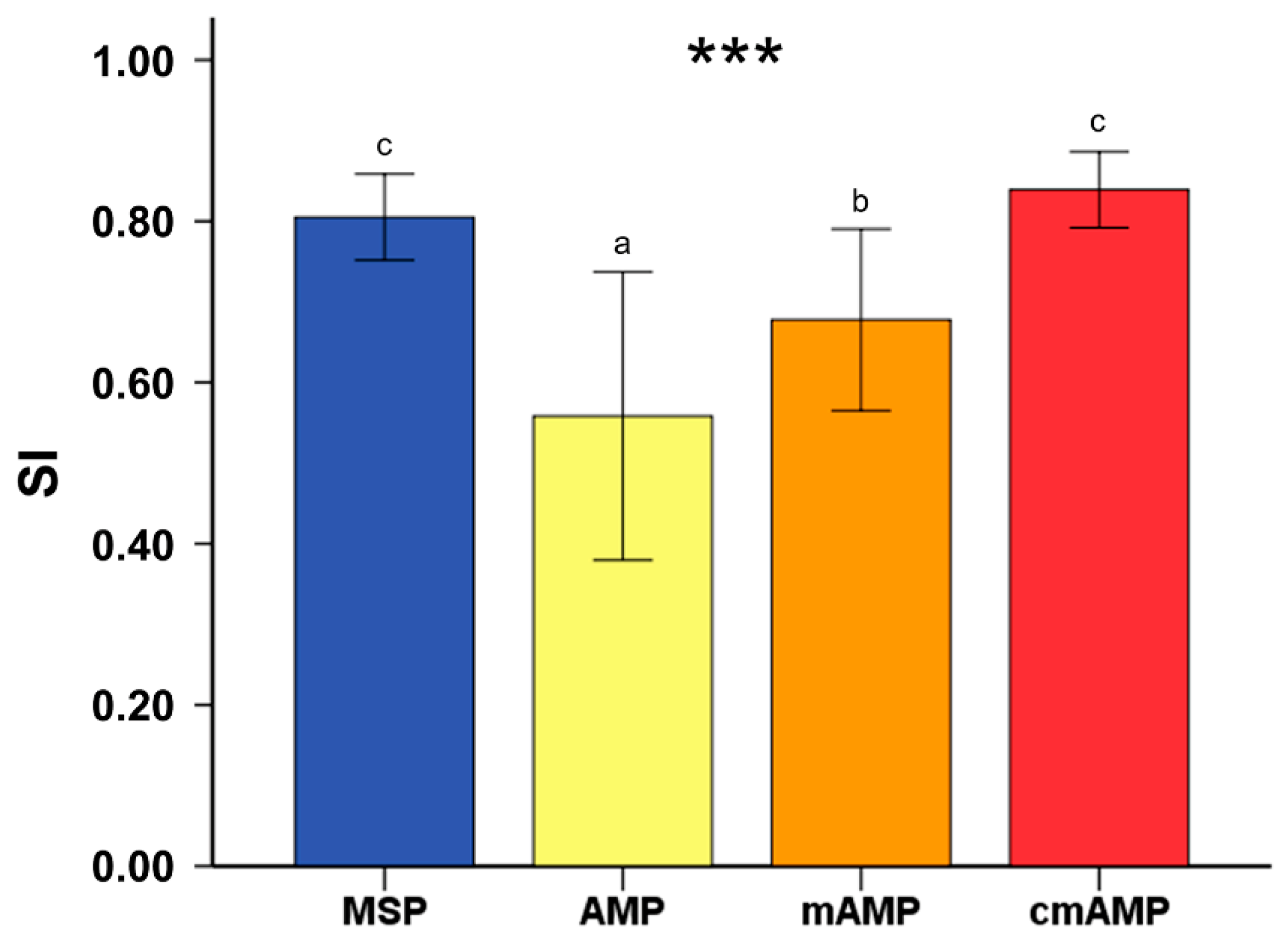
3.1. Non-Overlapping Surface, Volume, and SI Using Mirroring Technique Based on Each Mandibular Midsagittal Plane Prior to Surgery
3.2. Differences in Non-Overlapping Surface, Volume, and SI Based on the MSP before and after Surgery
3.3. Distance and Angle between MSP and Each Mandibular Midsagittal Plane before and after Surgery
3.4. Comparison of SI between MSP 1 Year after Surgery and Each Mandibular Midsagittal Plane before Surgery
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Severt, T.R.; Proffit, W.R. The prevalence of facial asymmetry in the dentofacial deformities population at the University of North Carolina. Int. J. Adult Orthodon. Orthognath. Surg. 1997, 12, 171–176. [Google Scholar] [PubMed]
- Choi, S.H.; Yoo, H.J.; Lee, J.Y.; Jung, Y.S.; Choi, J.W.; Lee, K.J. Stability of pre-orthodontic orthognathic surgery depending on mandibular surgical techniques: SSRO vs IVRO. J. Craniomaxillofac. Surg. 2016, 44, 1209–1215. [Google Scholar] [CrossRef] [PubMed]
- Al-Gunaid, T.; Yamaki, M.; Takagi, R.; Saito, I. Soft and hard tissue changes after bimaxillary surgery in Japanese class III asymmetric patients. J. Orthod. Sci. 2012, 1, 69–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.J.; Lee, K.J.; Yu, H.S.; Jung, Y.S.; Baik, H.S. Three-dimensional effect of pitch, roll, and yaw rotations on maxillomandibular complex movement. J. Craniomaxillofac. Surg. 2015, 43, 264–273. [Google Scholar] [CrossRef] [PubMed]
- Lo, L.J.; Weng, J.L.; Ho, C.T.; Lin, H.H. Three-dimensional region-based study on the relationship between soft and hard tissue changes after orthognathic surgery in patients with prognathism. PLoS ONE 2018, 13, e0200589. [Google Scholar] [CrossRef] [Green Version]
- Ludlow, J.B.; Gubler, M.; Cevidanes, L.; Mol, A. Precision of cephalometric landmark identification: Cone-beam computed tomography vs conventional cephalometric views. Am. J. Orthod. Dentofacial Orthop. 2009, 136, 312. [Google Scholar] [CrossRef]
- Choi, S.H.; Hwang, C.J.; Baik, H.S.; Jung, Y.S.; Lee, K.J. Stability of Pre-Orthodontic Orthognathic Surgery Using Intraoral Vertical Ramus Osteotomy Versus Conventional Treatment. J. Oral Maxillofac. Surg. 2016, 74, 610–619. [Google Scholar] [CrossRef]
- Chen, Y.J.; Yao, C.C.; Chang, Z.C.; Lai, H.H.; Yeh, K.J.; Kok, S.H. Characterization of facial asymmetry in skeletal Class III malocclusion and its implications for treatment. Int. J. Oral Maxillofac. Surg. 2019, 48, 1533–1541. [Google Scholar] [CrossRef]
- Kwon, S.M.; Baik, H.S.; Jung, H.D.; Jang, W.; Choi, Y.J. Diagnosis and Surgical Outcomes of Facial Asymmetry According to the Occlusal Cant and Menton Deviation. J. Oral Maxillofac. Surg. 2019, 77, 1261–1275. [Google Scholar] [CrossRef]
- Davies, J.C.; Chan, H.H.L.; Jozaghi, Y.; Goldstein, D.P.; Irish, J.C. Analysis of simulated mandibular reconstruction using a segmental mirroring technique. J. Craniomaxillofac. Surg. 2019, 47, 468–472. [Google Scholar] [CrossRef]
- Leonardi, R.; Muraglie, S.; Bennici, O.; Cavallini, C.; Spampinato, C. Three-dimensional analysis of mandibular functional units in adult patients with unilateral posterior crossbite: A cone beam study with the use of mirroring and surface-to-surface matching techniques. Angle Orthod. 2019, 89, 590–596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- You, K.H.; Kim, K.H.; Lee, K.J.; Baik, H.S. Three-dimensional computed tomography analysis of mandibular morphology in patients with facial asymmetry and mandibular retrognathism. Am. J. Orthod. Dentofacial. Orthop. 2018, 153, 685–691. [Google Scholar] [CrossRef] [PubMed]
- You, K.H.; Lee, K.J.; Lee, S.H.; Baik, H.S. Three-dimensional computed tomography analysis of mandibular morphology in patients with facial asymmetry and mandibular prognathism. Am. J. Orthod. Dentofacial. Orthop. 2010, 138, 540. [Google Scholar] [CrossRef]
- Fang, J.J.; Tu, Y.H.; Wong, T.Y.; Liu, J.K.; Zhang, Y.X.; Leong, I.F.; Chen, K.C. Evaluation of mandibular contour in patients with significant facial asymmetry. Int. J. Oral Maxillofac. Surg. 2016, 45, 922–931. [Google Scholar] [CrossRef]
- Wong, T.Y.; Liu, J.K.; Fang, J.J.; Wu, T.C.; Tu, Y.H. Use of the matching optimal symmetry plane method in planning surgical correction of facial asymmetry—A preliminary report of 20 patients. J. Oral. Maxillofac. Surg. 2014, 72, 1180.e1–1180.e13. [Google Scholar] [CrossRef]
- Lin, H.; Zhu, P.; Lin, Q.; Huang, X.; Xu, Y.; Yang, X. Comprehensive Analysis of Mandibular Residual Asymmetry after Bilateral Sagittal Split Ramus Osteotomy Correction of Menton Point Deviation. PLoS ONE 2016, 11, e0161601. [Google Scholar] [CrossRef] [PubMed]
- Kwon, S.M.; Hwang, J.J.; Jung, Y.H.; Cho, B.H.; Lee, K.J.; Hwang, C.J.; Choi, S.H. Similarity index for intuitive assessment of three-dimensional facial asymmetry. Sci. Rep. 2019, 9, 10959. [Google Scholar] [CrossRef] [Green Version]
- Jung, H.D.; Jung, Y.S.; Park, J.H.; Park, H.S. Recovery pattern of mandibular movement by active physical therapy after bilateral transoral vertical ramus osteotomy. J. Oral Maxillofac. Surg. 2012, 70, e431–437. [Google Scholar] [CrossRef]
- Sun, L.; Lee, K.M. Three-Dimensional Evaluation of the Postsurgical Stability of Mandibular Setback With the Surgery-First Approach: Comparison Between Patients With Symmetry and Asymmetry. J. Oral Maxillofac. Surg. 2019, 77, 1469-e1. [Google Scholar] [CrossRef]
- Hwang, J.J.; Han, S.S.; Lee, C.; Jung, Y.H. Automatic analysis algorithm for acquiring standard dental and mandibular shape data using cone-beam computed tomography. Sci. Rep. 2018, 8, 13516. [Google Scholar] [CrossRef]
- Haraguchi, S.; Takada, K.; Yasuda, Y. Facial asymmetry in subjects with skeletal Class III deformity. Angle Orthod. 2002, 72, 28–35. [Google Scholar] [PubMed]
- Wu, T.Y.; Denadai, R.; Lin, H.H.; Ho, C.T.; Lo, L.J. The outcome of skeletofacial reconstruction with mandibular rotation for management of asymmetric skeletal class III deformity: A three-dimensional computer-assisted investigation. Sci. Rep. 2019, 9, 13337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vittert, L.; Katina, S.; Ayoub, A.; Khambay, B.; Bowman, A.W. Assessing the outcome of orthognathic surgery by three-dimensional soft tissue analysis. Int. J. Oral. Maxillofac. Surg. 2018, 47, 1587–1595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greyling, L.M.; Le Grange, F.; Meiring, J.H. Mandibular spine: A case report. Clin. Anat. 1997, 10, 416–418. [Google Scholar] [CrossRef]
- Park, W.; Kim, B.C.; Yu, H.S.; Yi, C.K.; Lee, S.H. Architectural characteristics of the normal and deformity mandible revealed by three-dimensional functional unit analysis. Clin. Oral Investig. 2010, 14, 691–698. [Google Scholar] [CrossRef]
- Parnia, F.; Moslehifard, E.; Hafezeqoran, A.; Mahboub, F.; Mojaver-Kahnamoui, H. Characteristics of anatomical landmarks in the mandibular interforaminal region: A cone-beam computed tomography study. Med. Oral Patol. Oral Cir. Bucal. 2012, 17, e420–e425. [Google Scholar] [CrossRef] [Green Version]
- Bruce, R.A.; Hayward, J.R. Condylar hyperplasia and mandibular asymmetry: A review. J. Oral Surg. 1968, 26, 281–290. [Google Scholar]
- Bjork, A. Variations in the growth pattern of the human mandible: Longitudinal radiographic study by the implant method. J. Dent. Res. 1963, 42, 400–411. [Google Scholar] [CrossRef]
- Moss, M.L.; Rankow, R.M. The role of the functional matrix in mandibular growth. Angle Orthod. 1968, 38, 95–103. [Google Scholar]
- Olate, S.; Zaror, C.; Blythe, J.N.; Mommaerts, M.Y. A systematic review of soft-to-hard tissue ratios in orthognathic surgery. Part III: Double jaw surgery procedures. J. Craniomaxillofac. Surg. 2016, 44, 1599–1606. [Google Scholar] [CrossRef]
- Olate, S.; Zaror, C.; Mommaerts, M.Y. A systematic review of soft-to-hard tissue ratios in orthognathic surgery. Part IV: 3D analysis–Is there evidence? J. Craniomaxillofac. Surg. 2017, 45, 1278–1286. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.H.; Lee, H.; Hwang, J.J.; Jung, H.D.; Hwang, C.J.; Cha, J.Y. Differences in soft-tissue thickness changes after bimaxillary surgery between patients with vertically high angle and normal angle. Am. J. Orthod. Dentofacial. Orthop. 2020. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Landmark | Definition |
|---|---|
| N (nasion) | Midpoint of nasofrontal suture |
| S (sella) | Center of sella turcica |
| Or (orbitale) | Most inferior point of the lower margin of the orbit |
| Po (porion) | Most superior point of the external auditory meatus |
| Me (menton) | Most inferior midpoint on the symphysis |
| B (supramental) | Midpoint of greatest concavity on the anterior border of the symphysis |
| G (genial tubercle) | Midpoint on genial tubercle |
| Mf (mental foramen) | Midpoint of mental foramen |
| MSP | AMP | mAMP | cmAMP | p-Value | |||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | ||
| Right segment | |||||||||
| Non-overlapping surface (mm2) | 4347.03 b | 775.29 | 4786.67 b | 1029.46 | 4423.69 b | 777.71 | 3543.14 a | 734.13 | <0.001 |
| Non-overlapping volume (mm3) | 7942.44 ab | 2790.26 | 14,175.40 c | 6718.91 | 10,382.64 b | 5019.15 | 5088.85 a | 2280.33 | <0.001 |
| Left segment | |||||||||
| Non-overlapping surface (mm2) | 4567.87 a | 1047.01 | 5044.53 b | 1117.22 | 4603.61 a | 949.71 | 4112.34 a | 990.93 | 0.01 |
| Non overlapping volume (mm3) | 8212.43 ab | 3045.53 | 14,093.04 c | 6689.53 | 10,641.74 b | 4926.48 | 5423.47 a | 2467.45 | <0.001 |
| SI | 0.74 b | 0.07 | 0.55 a | 0.17 | 0.67 b | 0.11 | 0.83 c | 0.04 | <0.001 |
| Before Surgery | After Surgery | Difference | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | ||
| Right segment | |||||||
| Non-overlapping surface (mm2) | 4347.03 | 775.29 | 3899.65 | 842.71 | 447.37 | 684.56 | 0.001 |
| Non-overlapping volume (mm3) | 7942.44 | 2790.26 | 6036.33 | 2357.24 | 1906.11 | 2567.01 | <0.001 |
| Left segment | |||||||
| Non-overlapping surface (mm2) | 4567.87 | 1047.01 | 4240.63 | 1008.61 | 327.23 | 623.12 | 0.009 |
| Non-overlapping volume (mm3) | 8212.43 | 3045.53 | 6469.82 | 2703.88 | 1742.60 | 2944.47 | 0.004 |
| SI | 0.74 | 0.07 | 0.80 | 0.05 | −0.05 | 0.07 | <0.001 |
| Between MSP andAMP | Between MSP and mAMP | Between MSP and cmAMP | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | ||
| Before surgery | |||||||
| Distance (mm) | 3.64 b | 2.22 | 3.16 b | 2.07 | 1.77 a | 1.19 | 0.001 |
| Angle (degree) | 5.21 b | 3.61 | 3.98 ab | 2.35 | 2.87 a | 1.49 | 0.005 |
| After surgery | |||||||
| Distance (mm) | 2.46 b | 1.84 | 2.34 b | 1.65 | 1.15 a | 0.74 | 0.002 |
| Angle (degree) | 4.91 b | 3.15 | 2.90 a | 1.63 | 2.02 a | 0.82 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, W.-J.; Hwang, J.J.; Jung, Y.-H.; Cho, B.-H.; Lee, K.-J.; Yu, H.-S.; Choi, S.-H. A New Approach to Set the Absolute Midsagittal Plane of the Mandible Using a Similarity Index in Skeletal Class III Patients with Facial Asymmetry. Appl. Sci. 2020, 10, 8550. https://0-doi-org.brum.beds.ac.uk/10.3390/app10238550
Han W-J, Hwang JJ, Jung Y-H, Cho B-H, Lee K-J, Yu H-S, Choi S-H. A New Approach to Set the Absolute Midsagittal Plane of the Mandible Using a Similarity Index in Skeletal Class III Patients with Facial Asymmetry. Applied Sciences. 2020; 10(23):8550. https://0-doi-org.brum.beds.ac.uk/10.3390/app10238550
Chicago/Turabian StyleHan, Woo-Jin, Jae Joon Hwang, Yun-Hoa Jung, Bong-Hae Cho, Kee-Joon Lee, Hyung-Seog Yu, and Sung-Hwan Choi. 2020. "A New Approach to Set the Absolute Midsagittal Plane of the Mandible Using a Similarity Index in Skeletal Class III Patients with Facial Asymmetry" Applied Sciences 10, no. 23: 8550. https://0-doi-org.brum.beds.ac.uk/10.3390/app10238550