Patient Profiling Based on Spectral Clustering for an Enhanced Classification of Patients with Tension-Type Headache

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Headache Diary
2.3. Headache Disability Inventory
2.4. Hospital Anxiety and Depression Scale (HADS)
2.5. Health-Related Quality of Life
2.6. Sleep Quality
2.7. Pressure Pain Thresholds
2.8. Dynamic Pressure Thresholds
2.9. Trigger Point Examination
2.10. Data Preprocessing and Imputation
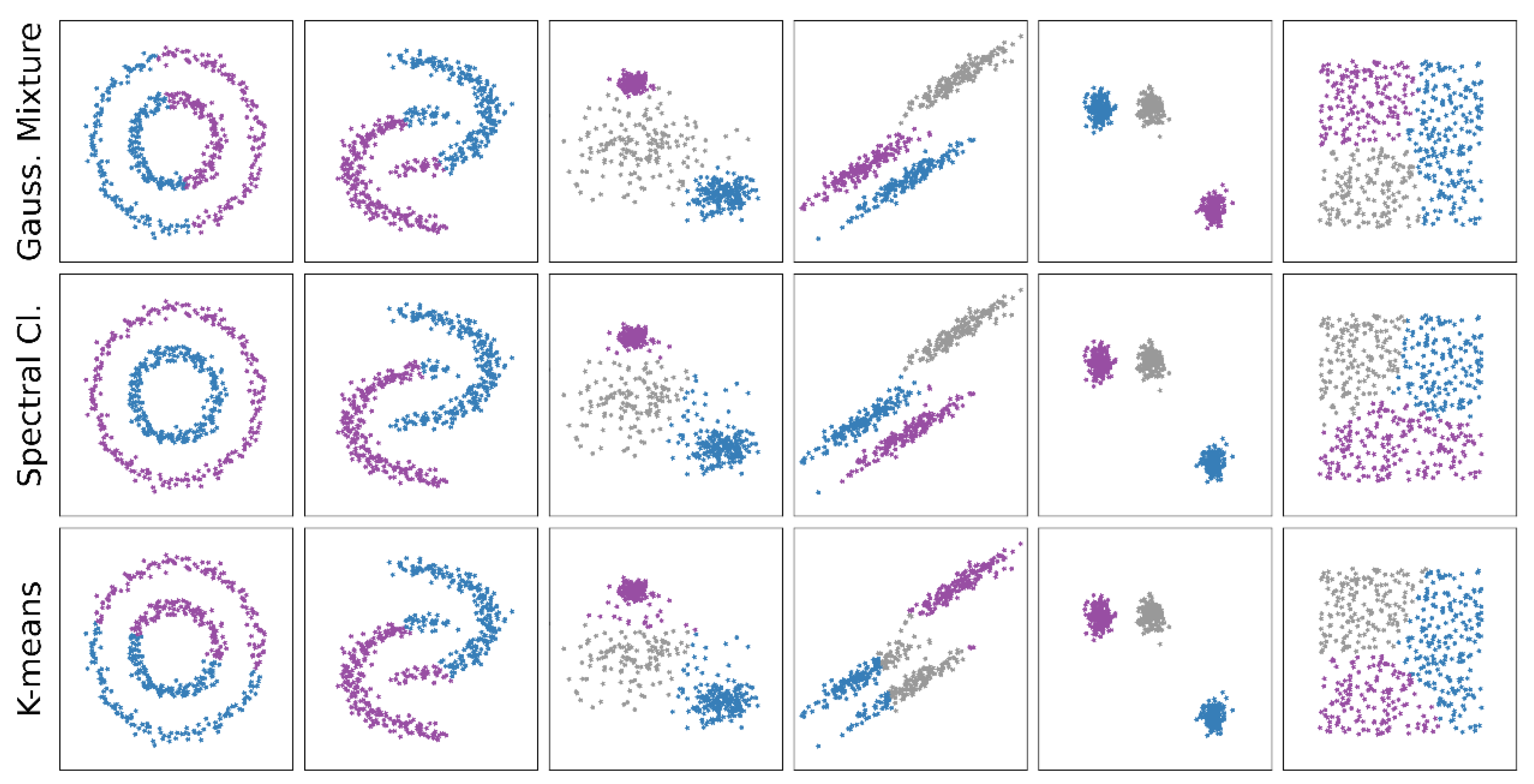
2.11. Clustering Algorithms
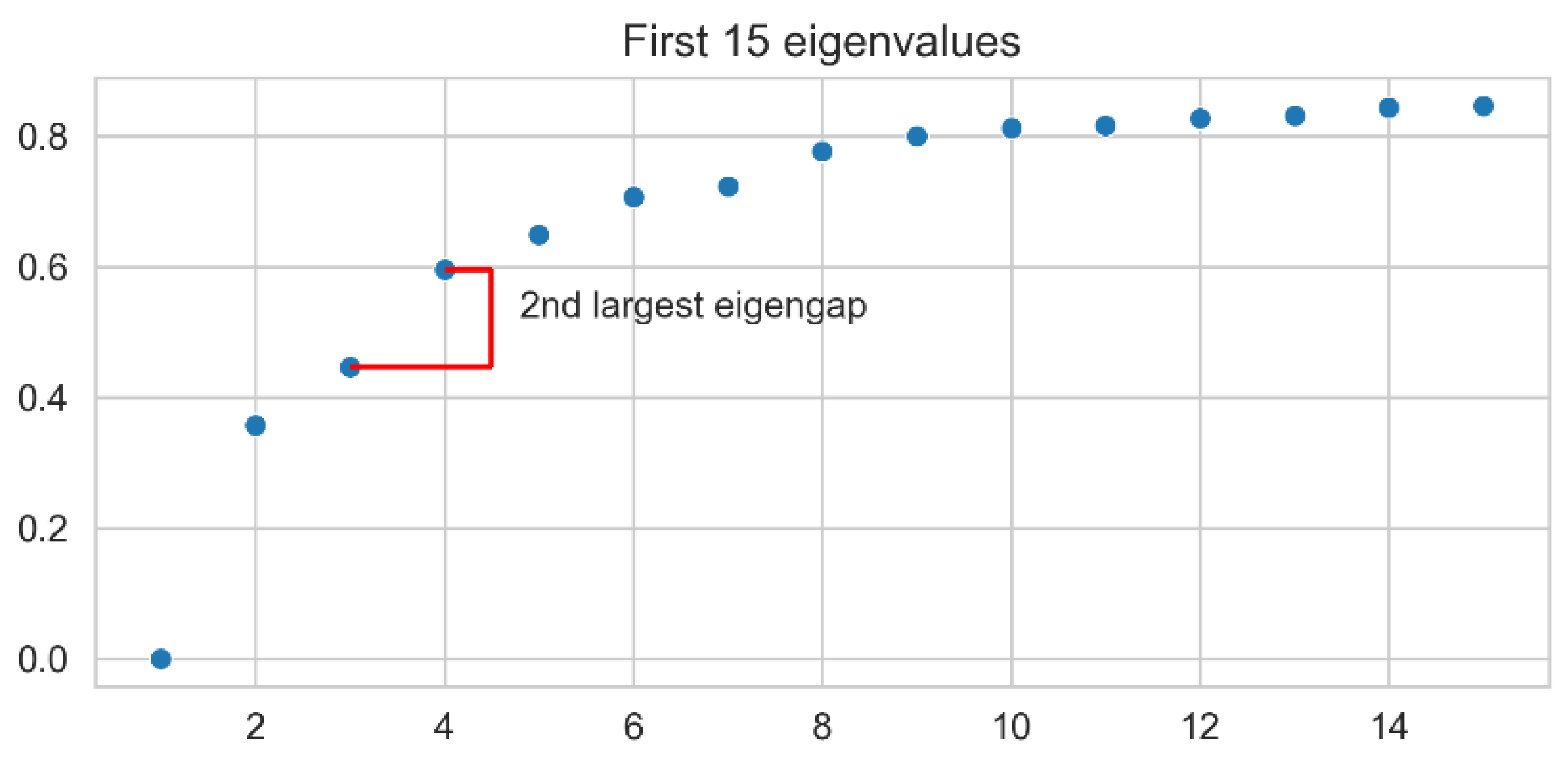
2.12. Spectral Clustering
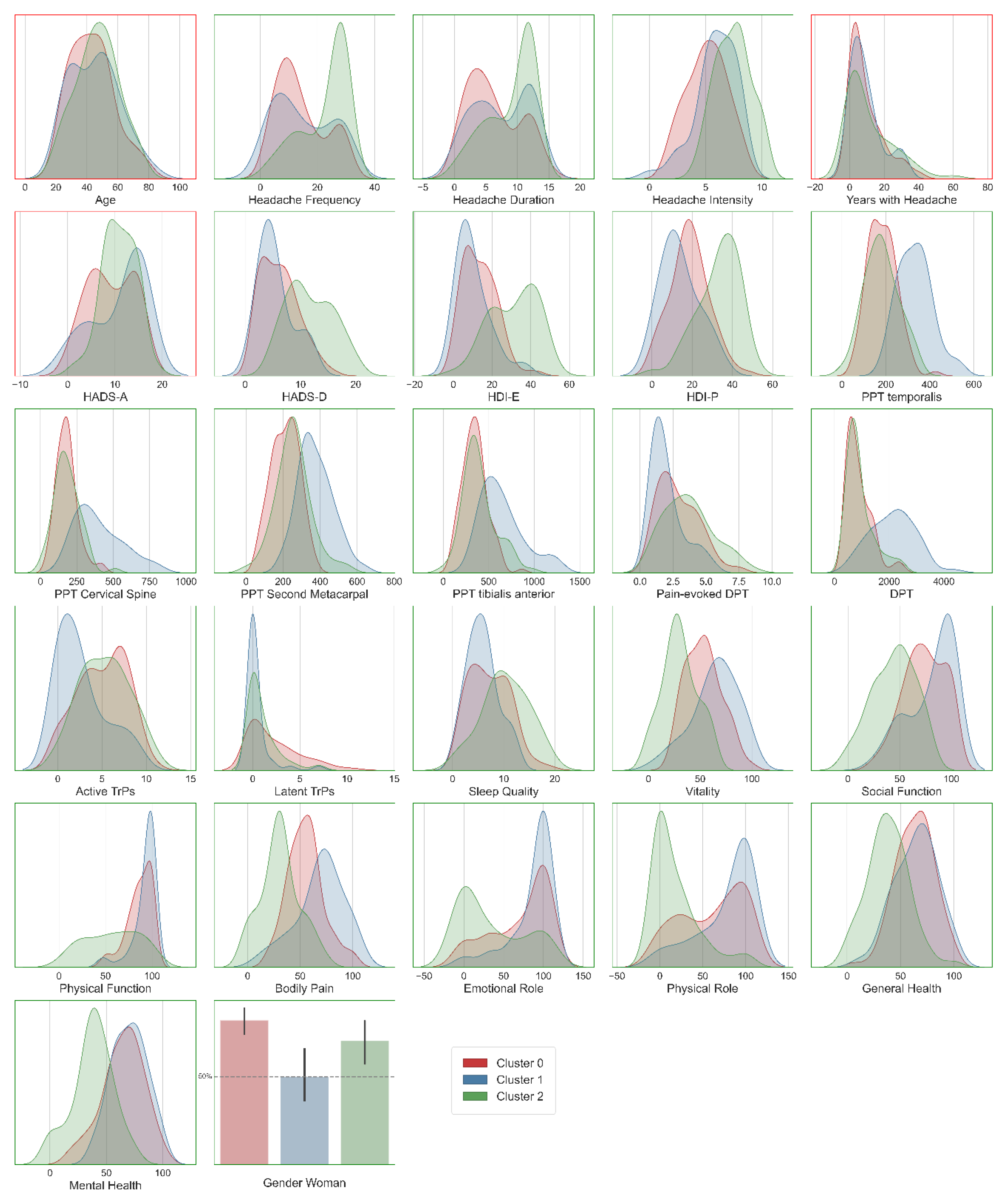
2.13. Statistical Analysis of the Clusters
3. Results
Participants
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- GBD 2016 Neurology Collaborators. Global, regional, and national burden of neurological disorders, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 459–480. [Google Scholar] [CrossRef] [Green Version]
- Ferrante, T.; Manzoni, G.C.; Russo, M.; Camarda, C.; Taga, A.; Veronesi, L.; Pasquarella, C.; Sansebastiano, G.; Torelli, P. Prevalence of tension-type headache in adult general population: The PACE study and review of the literature. Neurol. Sci. 2013, 34, 137–138. [Google Scholar] [CrossRef] [Green Version]
- Hagen, K.; Stovner, L.J.; Zwart, J.-A. Time trends of major headache diagnoses and predictive factors. Data from three Nord-Trøndelag health surveys. J. Headache Pain 2020, 21, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Jensen, R.H. Tension-type headache: The normal and most prevalent headache. Headache 2018, 58, 339–345. [Google Scholar] [CrossRef]
- De Tommaso, M.; Fernández-de-las-Peñas, C. Tension type headache. Curr. Rheumatol. Rev. 2016, 12, 127–139. [Google Scholar] [CrossRef]
- ICHD-III Headache Classification Subcommittee of the International Headache Society: The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [CrossRef]
- Arendt-Nielsen, L.; Egsgaard, L.L.; Petersen, K.K.; Eskehave, T.N.; Graven-Nielsen, T.; Hoeck, H.C.; Simonsen, O. A mechanism-based pain sensitivity index to characterize knee osteoarthritis patients with different disease stages and pain levels. Eur. J. Pain 2015, 19, 1406–1417. [Google Scholar] [CrossRef]
- Pedler, A.; Sterling, M. Patients with chronic whiplash can be subgrouped on the basis of symptoms of sensory hypersensitivity and posttraumatic stress. Pain 2013, 154, 1640–1648. [Google Scholar] [CrossRef]
- Fernández-de-las-Peñas, C.; Benito-González, E.; Palacios-Ceña, M.; Wang, K.; Castaldo, M.; Arendt-Nielsen, L. Identification of subgroups of patients with tension type headache with higher widespread pressure pain hyperalgesia. J. Headache. Pain 2017, 18, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérez-Benito, F.J.; Conejero, J.A.; Sáez, C.; García-Gómez, J.M.; Navarro-Pardo, E.; Florencio, L.L.; Fernández-de-Las-Peñas, C. Subgrouping factors influencing migraine intensity in women: A semi-automatic methodology based on machine learning and information geometry. Pain Pract. 2020, 20, 297–309. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Chen, J. Superpixel segmentation using linear spectral clustering. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Boston, MA, USA, 7–12 June 2015; pp. 1356–1363. [Google Scholar]
- Craddock, R.C.; James, G.A.; Holtzheimer, P.E., 3rd; Hu, X.P.; Mayberg, H.S. A whole brain fMRI atlas generated via spatially constrained spectral clustering. Hum. Brain Mapp. 2012, 33, 1914–1928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Qian, B.; Davidson, I. On constrained spectral clustering and its applications. Data Min. Knowl. Disc. 2014, 28, 1–30. [Google Scholar] [CrossRef] [Green Version]
- Headache Classification Committee of the International Headache Society (IHS). ICHD-III International Classification of Headache Disorders: Headache Classification Subcommittee of the International Headache Society, 3nd edition. Cephalalgia 2013, 33, 629–808. [Google Scholar]
- Phillip, D.; Lyngberg, A.C.; Jensen, R. Assessment of headache diagnosis: A comparative population study of a clinical interview with a diagnostic headache diary. Cephalalgia 2007, 27, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.P.; Turner, J.A.; Romano, J.M.; Fisher, L. Comparative reliability and validity of chronic pain intensity measures. Pain 1999, 83, 157–162. [Google Scholar] [CrossRef]
- Jacobson, G.P.; Ramadan, N.M.; Norris, L.; Newman, C.W. The Henry Ford Hospital Headache Disability Inventory. Neurology 1994, 44, 837–842. [Google Scholar] [CrossRef]
- Jacobson, G.P.; Ramadan, N.M.; Norris, L.; Newman, C.W. Headache disability inventory (HDI): Short-term test-retest reliability and spouse perceptions. Headache 1995, 35, 534–539. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Juang, K.D.; Wang, S.J.; Lin, C.H.; Fuh, J.L. Use of the Hospital Anxiety and Depression Scale as a screening tool for patients with headache. Zhonghua Yi Xue Za Zhi 1999, 62, 749–755. [Google Scholar]
- Ware, J.E.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef]
- McHorney, C.A.; Ware, J.E.; Raczek, A.E. The MOS 36-Item Short-Form Health Survey (SF-36): II. Psychometric and clinical tests of validity in measuring physical and mental health constructs. Med. Care 1993, 31, 247–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cole, J.C.; Dubois, D.; Kosinski, M. Use of patient-reported sleep measures in clinical trials of pain treatment: A literature review and synthesis of current sleep measures and a conceptual model of sleep disturbance in pain. Clin. Ther. 2007, 29, 2580–2588. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Carpenter, J.S.; Andrykowski, M.A. Psychometric evaluation of the Pittsburgh Sleep Quality Index. J. Psychosom. Res. 1998, 45, 5–13. [Google Scholar] [CrossRef]
- Palacios-Ceña, M.; Castaldo, M.; Wang, K.; Torelli, P.; Pillastrini, P.; Fernández-de-las-Peñas, C.; Arendt-Nielsen, L. Widespread pressure pain hypersensitivity is similar in women with frequent episodic and chronic tension-type headache: A blinded case-control study. Headache 2017, 57, 217–225. [Google Scholar] [CrossRef]
- Nie, H.; Arendt-Nielsen, L.; Andersen, H.; Graven-Nielsen, T. Temporal summation of pain evoked by mechanical stimulation in deep and superficial tissue. J. Pain 2005, 6, 348–355. [Google Scholar] [CrossRef]
- Sand, T.; Zwart, J.A.; Helde, G.; Bovim, G. The reproducibility of cephalic pain pressure thresholds in control subjects and headache patients. Cephalalgia 1997, 17, 748–755. [Google Scholar] [CrossRef]
- Palacios-Ceña, M.; Wang, K.; Castaldo, M.; Guerrero-Peral, Á.; Caminero, A.B.; Fernández-de-las-Peñas, C.; Arendt-Nielsen, L. Assessment of deep dynamic mechanical sensitivity in individuals with tension-type headache: The dynamic pressure algometry. Eur. J. Pain 2017, 21, 1451–1460. [Google Scholar] [CrossRef]
- Finocchietti, S.; Graven-Nielsen, T.; Arendt-Nielsen, L. Dynamic mechanical assessment of muscle hyperalgesia in humans: The dynamic algometer. Pain. Res. Manag. 2015, 20, 29–34. [Google Scholar] [CrossRef]
- Simons, D.G.; Travell, J.G.; Simons, L. Myofascial Pain and Dysfunction. The Trigger Point Manual, 3rd ed.; Wolters Kluwer: Philadelphia, PA, USA, 2019. [Google Scholar]
- Fernandez-de-las-Peñas, C.; Dommerholt, J. International consensus on diagnostic criteria and clinical considerations of myofascial trigger points: A Delphi Study. Pain. Med. 2018, 19, 142–150. [Google Scholar] [CrossRef] [Green Version]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-learn: Machine Learning in Python. J. Mach. Learn Res. 2011, 12, 2825–2830. [Google Scholar]
- Luxburg, U.V. A tutorial on spectral clustering. Stat. Comput. 2007, 17, 395–416. [Google Scholar] [CrossRef]
- Arbelaitz, O.; Gurrutxaga, J.; Muguerza, J.; Pérez, J.M.; Perona, I. An extensive comparative study of cluster validity indices. Pattern Recognit. 2013, 46, 243–256. [Google Scholar] [CrossRef]
- Virtanen, P.; Gommers, R.; Oliphant, T.E.; Haberland, M.; Reddy, T.; Cournapeau, D.; Burovski, E.; Peterson, P.; Weckesser, W.; Bright, J.; et al. SciPy 1.0: Fundamental algorithms for scientific computing in Python. Nat. Methods 2020, 17, 261–272. [Google Scholar] [CrossRef] [Green Version]
- Skipper, S.; Perktold, J. Stats models: Econometric and statistical modeling with python. In Proceedings of the 9th Python in Science Conference, Austin, TX, USA, June 28–July 3 2010. [Google Scholar]
- Fernández-de-las-Peñas, C.; Plaza-Manzano, G.; Navarro-Santana, M.J.; Olesen, J.; Jensen, R.H.; Bendtsen, L. Evidence of localized and widespread pressure pain hypersensitivity in patients with tension-type headache: A systematic review and meta-analysis. Cephalalgia 2020, 333102420958384. [Google Scholar] [CrossRef]
- Buchgreitz, L.; Lyngberg, A.C.; Bendtsen, L.; Jensen, R. Frequency of headache is related to sensitization: A population study. Pain 2006, 123, 19–27. [Google Scholar] [CrossRef]
- de Tommaso, M.; Sardaro, M.; Serpino, C.; Costantini, F.; Vecchio, F.; Prudenzano, M.P.; Lamberti, P.; Livrea, P. Fibromyalgia Comorbidity in Primary Headaches. Cephalalgia 2009, 29, 453–464. [Google Scholar] [CrossRef]
- de Tommaso, M.; Federici, A.; Serpino, C.; Vecchio, E.; Franco, G.; Sardaro, M.; Delussi, M.; Livrea, P. Clinical features of headache patients with fibromyalgia comorbidity. J. Headache Pain 2011, 12, 629–638. [Google Scholar] [CrossRef] [Green Version]
- Woolf, C.J. Central sensitization: Implications for the diagnosis and treatment of pain. Pain 2011, 152, S2–S15. [Google Scholar] [CrossRef]
- Fernández-de-las-Peñas, C.; Arendt-Nielsen, L. Improving understanding of trigger points and widespread pressure pain sensitivity in tension-type headache patients: Clinical implications. Expert Rev. Neurother. 2017, 17, 933–939. [Google Scholar] [CrossRef]
- Fernández-de-las-Peñas, C.; Cuadrado, M.L.; Arendt-Nielsen, L.; Simons, D.G.; Pareja, J.A. Myofascial trigger points and sensitization: An updated pain model for tension-type headache. Cephalalgia 2007, 27, 383–393. [Google Scholar] [CrossRef] [PubMed]
- Arendt-Nielsen, L.; Castaldo, M.; Mechelli, F.; Fernández-de-las-Peñas, C. Muscle triggers as a possible source of pain in a subgroup of tension-type headache patients? Clin. J. Pain 2016, 32, 711–718. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Du, H.; Chen, N.; Guo, J.; Gong, Q.; Zhang, J.; He, L. Regional homogeneity abnormalities in patients with tension-type headache: A resting-state fMRI study. Neurosci. Bull. 2014, 30, 949–955. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández-de-las-Peñas, C.; Cuadrado, M.L. Physical therapy for headaches. Cephalalgia 2016, 36, 1134–1142. [Google Scholar] [CrossRef]
- Cathcart, S.; Petkov, J.; Winefield, A.H.; Lushington, K.; Rolan, P. Central mechanisms of stress-induced headache. Cephalalgia 2010, 30, 285–295. [Google Scholar] [CrossRef]
- Cathcart, S.; Winefield, A.; Lushington, K.; Rolan, P. Stress and tension-type headache mechanisms. Cephalalgia 2010, 30, 1250–1267. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| MEAN | SD | MIN | 25% | 50% | 75% | MAX | MISSING | |
|---|---|---|---|---|---|---|---|---|
| Age (years) | 44.7 | 14.4 | 18.0 | 33.0 | 45.0 | 53.5 | 83.0 | 0.5% |
| Headache frequency (days/month) | 16.8 | 9.45 | 1.0 | 8.0 | 16.0 | 28.0 | 30.0 | 2.4% |
| Headache duration (hours/attack) | 7.4 | 4.35 | 0.5 | 3.5 | 6.85 | 12.0 | 24.0 | 7.7% |
| Headache intensity (nprs 0–10) | 6.1 | 2.65 | 0.0 | 5.0 | 6.0 | 7.6 | 31.0 | 0.0% |
| Years with headache | 10.3 | 11.25 | 0.0 | 2.0 | 5.5 | 15.0 | 60.0 | 3.85% |
| HADS-A (0–21) | 9.9 | 4.7 | 0.0 | 6.0 | 10.0 | 14.0 | 19.0 | 18.75% |
| HADS-D (0–21) | 7.9 | 4.45 | 1.0 | 4.0 | 7.0 | 11.0 | 20.0 | 18.75% |
| HDI-E (0–52) | 19.1 | 13.2 | 0.0 | 8.0 | 16.0 | 26.0 | 52.0 | 18.75% |
| HDI-P (0–48) | 22.8 | 12.3 | 0.0 | 14.0 | 22.0 | 32.0 | 52.0 | 18.75% |
| PPT temporalis (kpa) | 213.3 | 94.5 | 0.0 | 140.9 | 201.75 | 267.0 | 537.0 | 0.0% |
| PPT cervical spine (kpa) | 227.9 | 136.6 | 0.0 | 139.25 | 193.5 | 273.75 | 784.0 | 0.0% |
| PPT second metacarpal (kpa) | 258.7 | 105.9 | 0.0 | 179.9 | 253.0 | 320.0 | 629.5 | 0.0% |
| PPT tibialis anterior (kpa) | 423.65 | 211.3 | 0.0 | 296.9 | 381.75 | 512.6 | 1233.0 | 0.0% |
| Pain-evoked DPT (nprs, 0–10) | 2.95 | 1.7 | 0.5 | 1.5 | 2.5 | 4.0 | 8.5 | 3.85% |
| DPT (grammes) | 1170.4 | 756.8 | 450.0 | 600.0 | 850.0 | 1450.0 | 4325.0 | 3.85% |
| Active TrPs | 4.6 | 3.0 | 0.0 | 2.0 | 5.0 | 7.0 | 11.0 | 1.4% |
| Latent TrPs | 1.5 | 2.3 | 0.0 | 0.0 | 0.0 | 2.0 | 11.0 | 1.4% |
| Sleep quality (0–21) | 8.0 | 4.4 | 0.0 | 4.0 | 8.0 | 11.0 | 20.0 | 10.1% |
| Vitality (0–100) | 48.55 | 22.3 | 0.0 | 30.0 | 50.0 | 65.0 | 100.0 | 1.0% |
| Social function (0–100) | 66.3 | 25.4 | 0.0 | 50.0 | 63.0 | 88.0 | 100.0 | 1.0% |
| Physical function (0–100) | 78.9 | 24.2 | 0.0 | 70.0 | 85.0 | 100.0 | 100.0 | 1.0% |
| Bodily pain (0–100) | 50.6 | 23.3 | 0.0 | 32.0 | 51.0 | 62.0 | 100.0 | 1.0% |
| Emotional role (0–100) | 62.7 | 40.8 | 0.0 | 33.0 | 67.0 | 100.0 | 100.0 | 1.0% |
| Physical role (0–100) | 51.5 | 40.2 | 0.0 | 0.0 | 50.0 | 100.0 | 100.0 | 1.0% |
| General health (0–100) | 56.1 | 22.2 | 0.0 | 40.0 | 57.0 | 72.0 | 100.0 | 1.0% |
| Mental health (0–100) | 57.7 | 22.1 | 0.0 | 40.0 | 60.0 | 76.0 | 100.0 | 1.4% |
| Cluster 0 (n = 102) | Cluster 1 (n = 42) | Cluster 2 (n = 61) | p-Value | |
|---|---|---|---|---|
| Age (years) | 43.4 ± 14.2 | 44.95 ± 15.85 | 46.75 ± 13.8 | 0.6997 |
| Headache frequency (days/month) | 14.2 ± 8.45 | 15.0 ± 10.0 | 22.6 ± 8.2 | <0.001 |
| Headache duration (hours/attack) | 6.3 ± 4.1 | 7.5 ± 4.3 | 9.0 ± 3.7 | <0.01 |
| Headache intensity (NPRS, 0–10) | 5.1 ± 18.8 | 5.9 ± 1.85 | 7.4 ± 1.55 | <0.001 |
| Years with headache | 9.4 ± 9.7 | 9.3 ± 9.1 | 11.6 ± 13.45 | 0.6997 |
| HADS-A (0–21) | 9.1 ± 4.9 | 10.8 ± 5.7 | 10.9 ± 3.6 | 0.161 |
| HADS-D (0–21) | 6.25 ± 3.4 | 5.45 ± 3.1 | 11.7 ± 4.15 | <0.001 |
| HDI-E (0–52) | 13.7 ± 8.75 | 10.2 ± 8.8 | 31.2 ± 12.2 | <0.001 |
| HDI-P (0–48) | 18.7 ± 9.6 | 13.8 ± 9.5 | 33.15 ± 10.5 | <0.001 |
| PPT temporalis (kPa) | 183.9 ± 65.35 | 334.5 ± 77.9 | 180.56 ± 77.1 | <0.001 |
| PPT cervical spine (kPa) | 181.1 ± 74.25 | 406.35 ± 161.7 | 183.1 ± 89.35 | <0.001 |
| PPT second metacarpal (kPa) | 212.65 ± 73.45 | 378.0 ± 92.2 | 255.5 ± 96.85 | <0.001 |
| PPT tibialis anterior (kPa) | 347.7 ± 135.2 | 654.1 ± 238.3 | 395.45 ± 182.1 | <0.001 |
| Pain-evoked DPT (NPRS, 0–10) | 2.9 ± 1.55 | 2.0 ± 1.25 | 3.7 ± 1.9 | <0.001 |
| DPT (grammes) | 902.0 ± 467.6 | 2146.4 ± 818.8 | 933.3 ± 504.95 | <0.001 |
| Active TrPs | 5.0 ± 2.8 | 2.7 ± 2.8 | 5.3 ± 2.8 | <0.001 |
| Latent TrPs | 2.2 ± 2.7 | 0.4 ± 1.3 | 1.0 ± 1.65 | <0.001 |
| Sleep Quality (0–100) | 7.2 ± 3.95 | 5.85 ± 3.05 | 10.4 ± 4.6 | <0.001 |
| Vitality (0–100) | 53.6 ± 17.45 | 64.05 ± 22.7 | 30.3 ± 16.7 | <0.001 |
| Social Function (0–100) | 74.15 ± 19.8 | 80.7 ± 22.4 | 44.15 ± 20.85 | <0.001 |
| Physical Function (0–100) | 86.2 ± 13.75 | 93.2 ± 12.35 | 57.0 ± 29.1 | <0.001 |
| Bodily Pain (0–100) | 55.3 ± 16.95 | 69.0 ± 23.1 | 30.8 ± 18.25 | <0.001 |
| Emotional Role (0–100) | 70.6 ± 36.4 | 85.45 ± 27.8 | 35.1 ± 40.6 | <0.001 |
| Physical Role (0–100) | 60.4 ± 36.45 | 78.65 ± 32.4 | 18.45 ± 27.35 | <0.001 |
| General Health (0–100) | 63.6 ± 18.0 | 64.2 ± 20.1 | 38.45 ± 19.55 | <0.001 |
| Mental Health (0–100) | 64.9 ± 18.6 | 70.0 ± 15.4 | 37.9 ± 17.9 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pellicer-Valero, O.J.; Fernández-de-las-Peñas, C.; Martín-Guerrero, J.D.; Navarro-Pardo, E.; Cigarán-Méndez, M.I.; Florencio, L.L. Patient Profiling Based on Spectral Clustering for an Enhanced Classification of Patients with Tension-Type Headache. Appl. Sci. 2020, 10, 9109. https://0-doi-org.brum.beds.ac.uk/10.3390/app10249109
Pellicer-Valero OJ, Fernández-de-las-Peñas C, Martín-Guerrero JD, Navarro-Pardo E, Cigarán-Méndez MI, Florencio LL. Patient Profiling Based on Spectral Clustering for an Enhanced Classification of Patients with Tension-Type Headache. Applied Sciences. 2020; 10(24):9109. https://0-doi-org.brum.beds.ac.uk/10.3390/app10249109
Chicago/Turabian StylePellicer-Valero, Oscar J., César Fernández-de-las-Peñas, José D. Martín-Guerrero, Esperanza Navarro-Pardo, Margarita I. Cigarán-Méndez, and Lidiane L. Florencio. 2020. "Patient Profiling Based on Spectral Clustering for an Enhanced Classification of Patients with Tension-Type Headache" Applied Sciences 10, no. 24: 9109. https://0-doi-org.brum.beds.ac.uk/10.3390/app10249109