1. Introduction
Laser Assisted In-Situ Keratomileusis (LASIK) has become the most prevalent refractive surgical procedure for myopic and hyperopic corrections (about 1.2 million procedures a year in the US)—over the last two decades. Patient satisfaction is generally found to be very high between 92 and 98 percent [
1,
2]. Modern excimer laser systems can restore 20/20 uncorrected visual acuity (UCVA) in myopic eyes up to—10D and hyperopic up to +6D, feature tissue saving procedures [
3], provide patient-specific, wavefront and/or topography guided ablation patterns, and can treat astigmatism with elliptically shaped patterns.
The concept of multifocal PresbyLASIK is a relatively new yet attractive surgical procedure for the correction of presbyopia. It involves two steps: (1) the correction of the ametropic state for distance vision, and (2) the multifocality addition for near vision. As most commonly reported in literature, multifocality is usually implemented by combining a central corneal curvature addition for near vision correction with a paracentral corneal curvature, adjusted to correct distance vision [
4,
5,
6,
7,
8,
9].
The downside of multifocal LASIK treatments is that they always represent a compromise between distance—and near vision correction, as they create unwanted aberrations—especially spherical aberrations in the central pupillary region. For this reason, modern PresbyLASIK treatment algorithms are wavefront-guided to minimize unwanted aberrations. Compared to treating presbyopia with the well-established multifocal intra ocular lens (IOL) implantation, PresbyLASIK has the advantage of being less invasive because the ocular globe does not need to be opened for treatment. However, the planning of PresbyLASIK procedures is much more demanding and requires experience in the interpretation of the preoperative corneal topography, wavefront analysis and the Zernike coefficients, which all have significant impact on the surgery result. Hence, it is not enough to simply apply the common LASIK indications to PresbyLASIK as well. Presumably, the lack of specific indications—along with missing to consider refraction and wavefront analysis parameters, might well be the reason for the not all encouraging LASIK presbyopia treatment results presented in literature [
10,
11].
In this study we present our PresbyLASIK results and compare them to a control group of regular LASIK myopia correction cases. Further, we propose an updated set of more specific indications for the PresbyLASIK treatment.
2. Materials and Methods
Our study population included two groups of eyes, 40 eyes of 20 study patients (female: 14, male: 6, age: 30 ± 9 years) were treated with regular myopic LASIK correction, and 50 eyes of 25 study patients (female: 14, male: 11, age: 52 ± 3.8 years) were treated for presbyopia with the PresbyLASIK Supracor treatment (B&L Technolas, Munich, Germany). All surgery procedures were performed by an experienced surgeon (BP) at the Eye Clinic ORASIS between January 2014 and February 2015.
The LDV femtosecond laser (Ziemer Ophthalmology, Port, Switzerland) was used to make the LASIK flaps, whereby the hinge was superior in all cases. The flap diameter depended on the corneal curvature and was between 8.5 and 9.0 mm. The Munnerlyn formula [
12] along with the B&L-Technolas proprietary transition zone algorithm was used to calculate the ablation patterns for the regular myopia corrections. In a two-step approach a 2.0 mm laser spot diameter was first used to apply the basic correction, followed by the fine-tuning step with a 1.0 mm laser spot. An eye tracker system was active during all interventions. The cyclorotation is automatically compensated which is especially important for cases where astigmatism correction was included. Whenever the angle kappa was smaller or equal 6° the laser spot was placed in the pupil center, otherwise it was placed at the point of the arithmetic mean between the pupil center and the Purkinje reflex. After the laser correction, the flap was carefully placed back onto the stromal bed, making sure no visible wrinkles are left.
The same approach as for the myopia ablation patterns is also employed to calculate the Supracor PresbyLASIK ablation patterns, however, the target refraction is chosen such that the dominant eye was at 0.0D and the follow-eye was at −0.5D. The goal of a first application phase is to obtain a perfect mono-focal correction, and only in the second phase the central cornea is steepened by the multifocal curvature addition in the 3.0 to 6.0 mm zone. Considering that such an ablation could potentially induced spherical aberration, the Supracor procedure was performed wavefront-guided for all cases.
Corneal shape was assessed one week before and then 3 months after the LASIK treatment, with the Galilei G4 tomographer (Ziemer Ophthalmic Systems, Port, Switzerland). Thereby, each individual measurement was repeated three times in a row. So, only one measurement with the median astigmatism cylinder value is selected for further data evaluation.
The statistical methods used in this study were straightforward calculations of average and standard deviation, as described in any textbook of statistics. Excel software package (Microsoft, Redmond, WA, USA) was used to import and process data, as well as, to obtain the functional dependence of the selected parameters and their visualization. Two-tailed Student t-test was used for calculating the parametric datas and for the nonparametric test the Wilcoxon signed rank test was used. The level of significance was set at p < 0.05.
3. Results
All study data were carefully analyzed and are presented in the following. Manifest refraction of the whole study population was sph: −1.99D ± 3.48 (SD), cyl: −0.80D ± 0.79 (SD) before, and sph: −0.03D ± 0.27 (SD), cyl: −0.18D ± 0.32 (SD) after the surgery. While the myopia group had a manifest refraction of sph: −3.53D ± 2.48 (SD), cyl: −0.93D ± 0.84 (SD) before, and sph: +0.05D ± 0.19 (SD), cyl: −0.09D ± 0.27 (SD) after the surgery, the presbyopia group had a manifest refraction of sph: −1.02D ± 3.78 (SD), cyl:−0.72D ± 0.75 (SD) before, and sph: −0.09D ± 0.31 (SD), cyl: −0.24D ± 0.34 (SD) after the surgery.
3.1. Uncorrected Visual Acuity
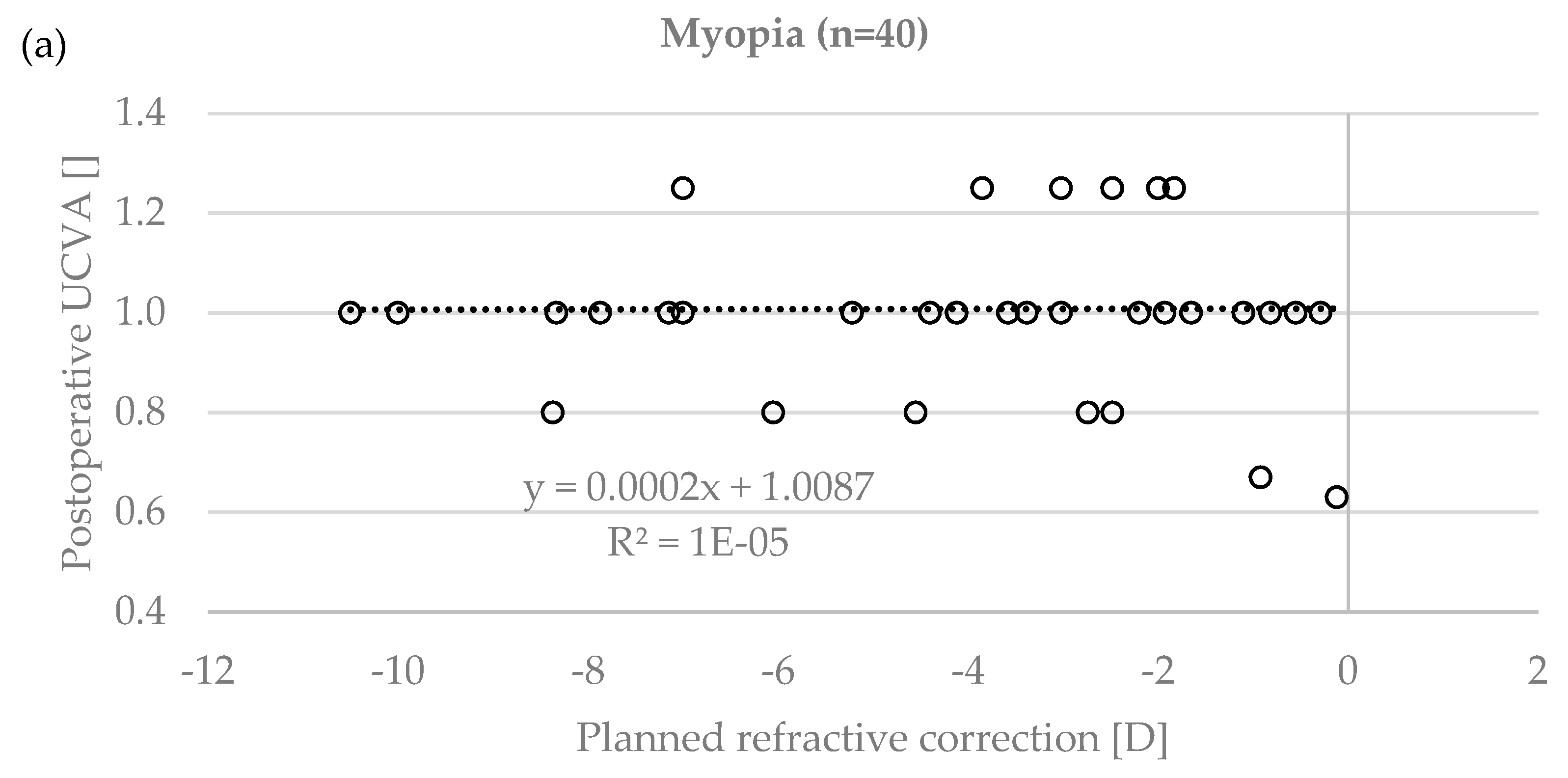
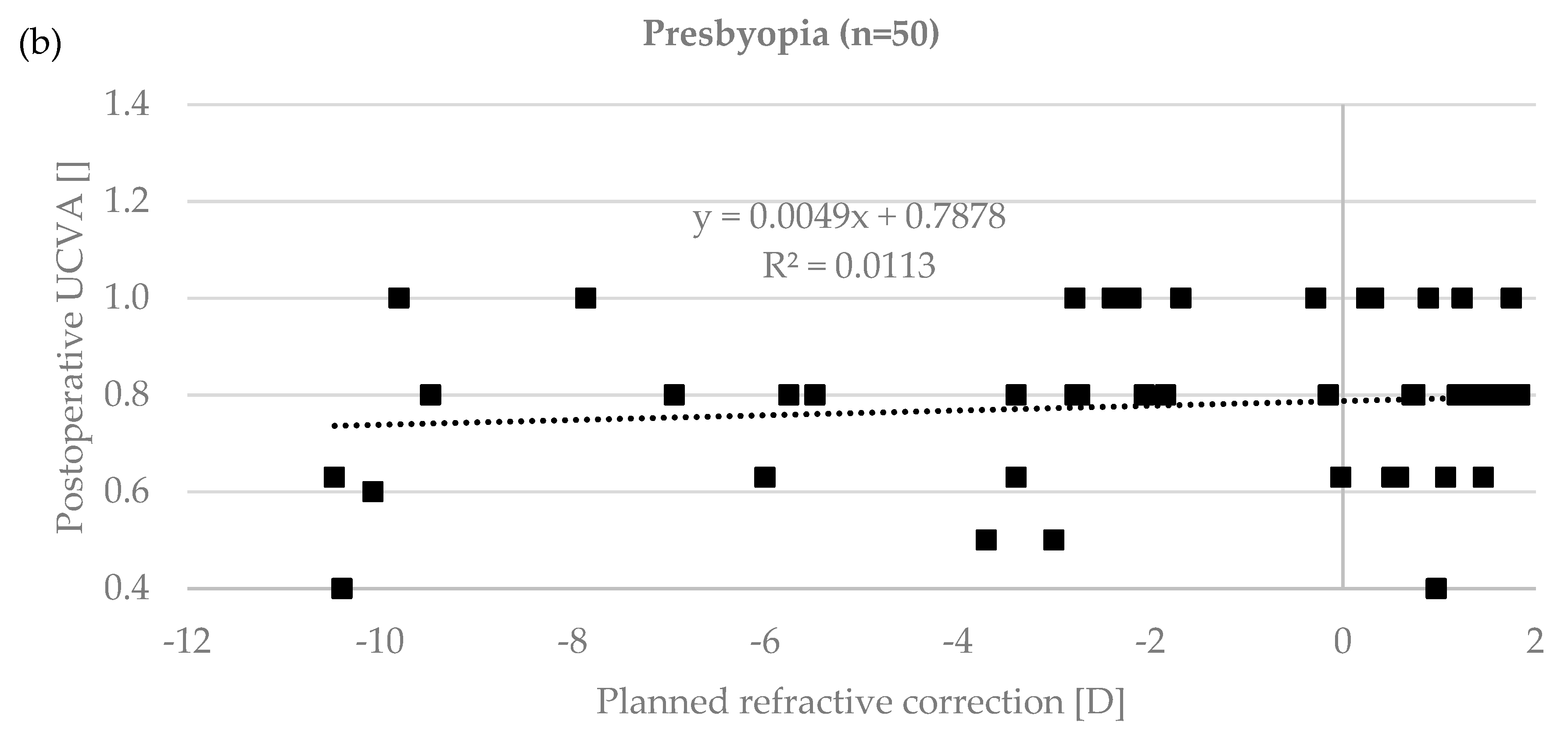
Uncorrected visual acuity (UCVA) was assessed before (decimal scale: 0.31 ± 0.24) and after the treatment (decimal scale: 0.88 ± 0.20) for the whole study population. In the myopia group UCVA was 0.19 ± 0.16 preoperatively, and 1.01 ± 0.15 postoperatively. In the presbyopia group UCVA was 0.38 ± 0.25 preoperatively, and 0.78 ± 0.17 postoperatively. A statistically significant improvement was observed in both groups (
p < 0.0001). In 4 eyes (4.3%, two in myopia and two in presbyopia group), UCVA remained unchanged, and for two eyes (2.2%, all in the presbyopia group) UCVA was slightly worse than before the treatment. For all other eyes (93.5%), UCVA improved (see
Table 1). The failure to achieve the target refraction and UCVA could be corrected with a re-treatment.
While the multifocal presbyopia treatments showed a small trend (R
2 = 0.01) towards greater corrections having a lower postoperative UCVA, this trend could not be observed (R
2 = 1 × 10
−5) for the myopic corrections (see
Figure 1).
3.2. Residual Stromal Bed and Percentage Tissue Altered
The average residual stromal bed thickness for all cases was 385 μm ± 49 (SD), with a minimum of 285 μm, and a maximum of 510 μm. The recently published and already widely accepted new criterion for LASIK safety, the percentage tissue altered (PTA) value [
13] was 32.0% ± 3.0 (SD), with a minimum of 22% and a maximum of 47%.
3.3. Astigmatism Change
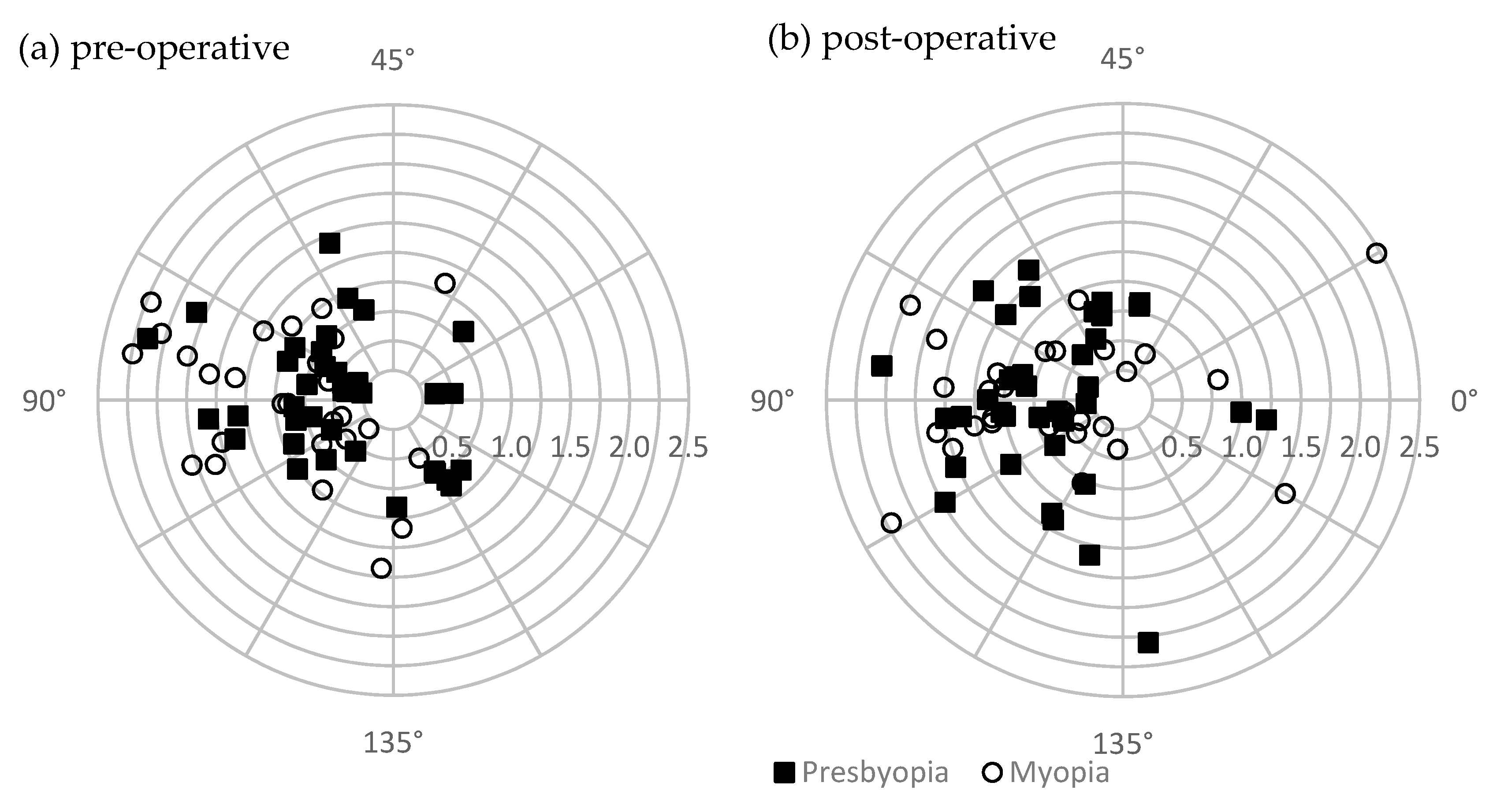
Corneal astigmatism, assessed with the Galilei G4, showed very little difference (
p > 0.6), between preoperative (0.98D ± 0.53 SD) and postoperative measurements (1.01D ± 0.50 SD) over the whole study population. Likewise, the myopia group had preoperative astigmatism of 1.17D ± 0.63 (SD), which changed to postoperative astigmatism of 0.78D ± 0.74 (SD)
p > 0.02. The presbyopia group had preoperative astigmatism of 1.02D ± 0.42 (SD), which changed to postoperative astigmatism of 0.96D ± 0.58 (SD)
p > 0.02. Also,
Figure 2 shows double-angle polar plots of pre-, and post-operative astigmatism measurements for both groups, myopia and presbyopia, and suggests only small changes in astigmatism from pre—to postoperative measurements. However, the Alpins method [
14] vector analysis (including the astigmatism orientation) showed that astigmatism changed significantly, by 0.78D ± 0.74 (SD) for myopia and by 0.96D ± 0.58 (SD) for presbyopia, respectively. The intended astigmatic change (planned astigmatic LASIK ablations) was 0.94D ± 0.84 (SD) for myopia group and 0.65D ± 0.41 (SD) for presbyopia group.
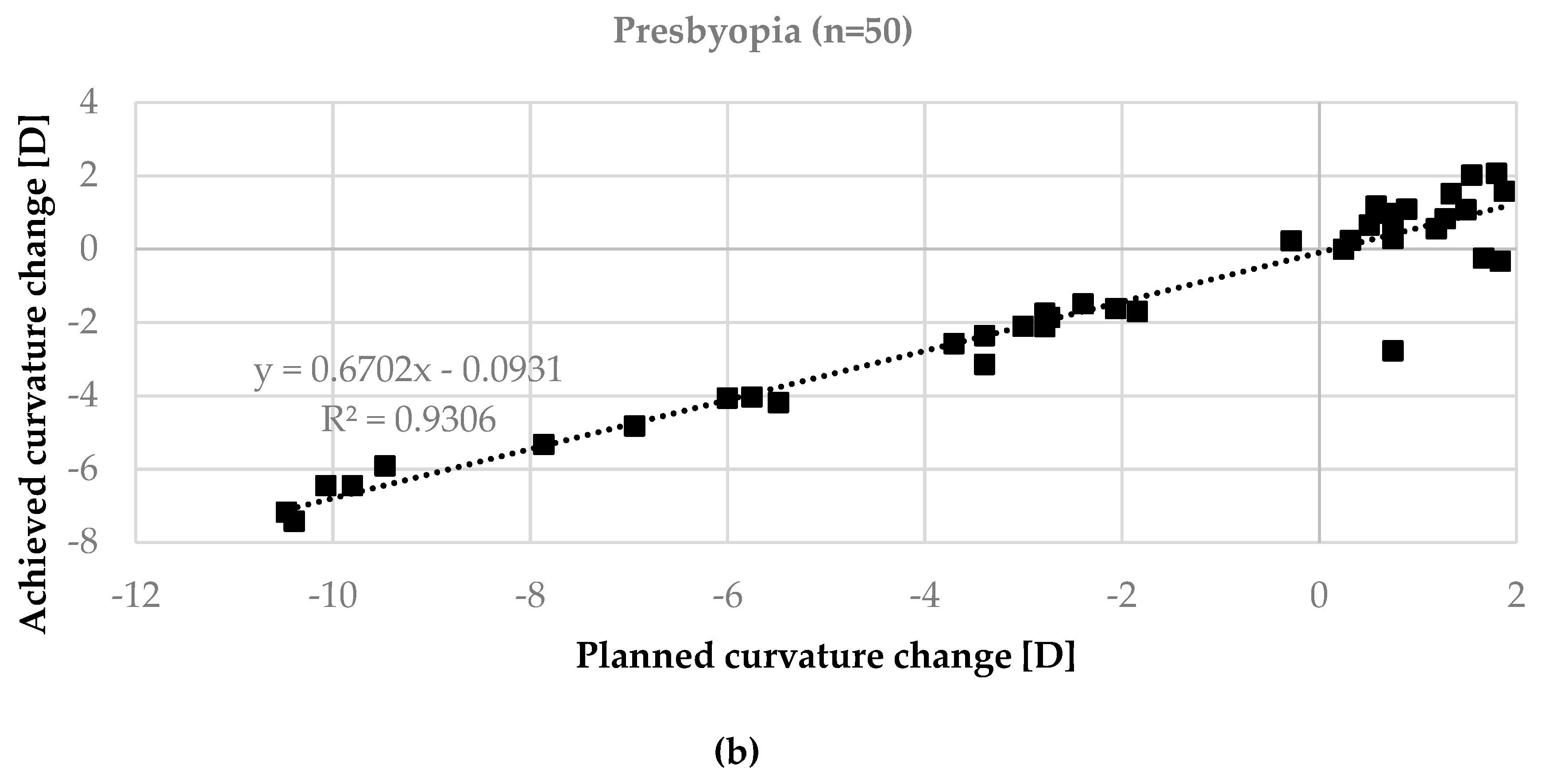
3.4. Corneal Curvature Change
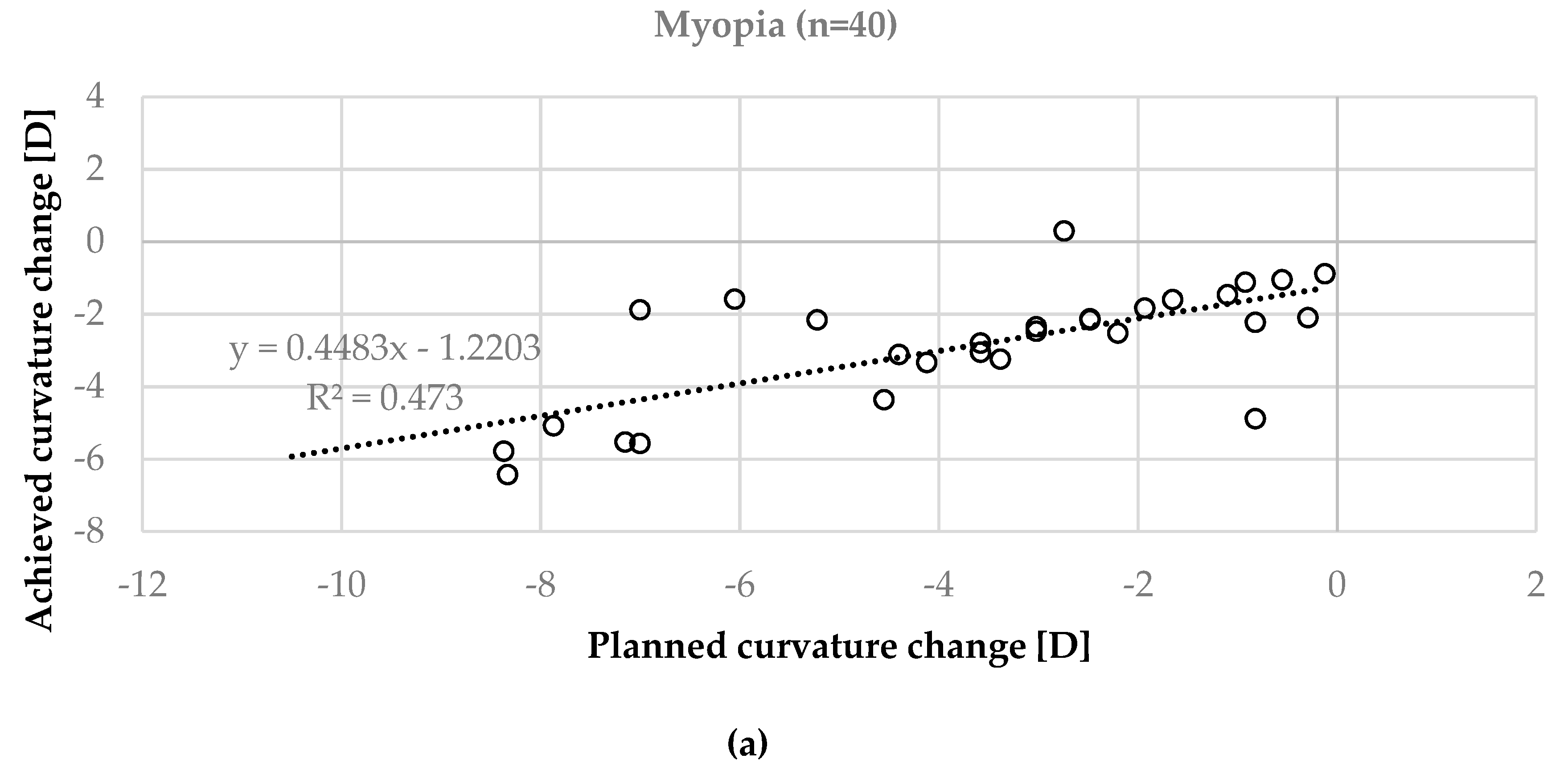
The planned shape change of the anterior corneal surface was compared to the measured corneal surface average corneal curvature–AvgK (postoperative Galilei minus preoperative Galilei). In an ideally case, in
Figure 3, all data points would lie on a diagonal line (y = 1.0x + 0.0, with an R
2 = 1.0). The top plot (b) in
Figure 3 shows that the above graph (b) in
Figure 3 shows that the presbyopia corrections showed a better match between the planned and achieved spherical correction (y = 0.67x − 0.09, R
2 = 0.93) compared to the myopia correction (see graph (a) in
Figure 3) (y = 0.45x − 1.22, R
2 = 0.47).
4. Discussion
In this study, femto-LASIK refractive surgical treatments were performed in two groups of study populations. While one of the groups received a standard myopia treatment, the second group was treated with a specific multifocal presbyLASIK algorithm to treat presbyopia. Study data, such as uncorrected visual acuity (UCVA), were carefully analyzed and presented as study results.
In almost all the cases (>93%), UCVA was improved after the surgery, with respect to the baseline assessment before the treatment. Thereby, the standard femto-LASIK myopia treatment showed slightly better results than the presbyLASIK treatment, where outcome UCVA was lower. This most likely arises from the fact that the subjective tolerance to eye surgical treatments including multifocal optics is greater than in monofocal treatments. Even a small deviation of 0.5D from the target value can be disturbing for the patient. Accordingly, there was a small but significant trend in recent results, where higher correction of presbyLASIK lead to lower postoperative UCVA. No similar trend was observed in the standard myopia treatment cases, where even high corrections of up to −10.5D had perfect vision with UCVA result of decimal 1.0.
The completely positive UCVA outcome was achieved, although the results suggest that astigmatism was drastically undertreated. Even though the laser was programmed with astigmatism correcting ablation patterns for all cases with treatable preoperative astigmatism, significant postoperative corneal astigmatism was observed in the topography measurements of both study groups. This observation is not supported by estimates of apparent refraction, where the cylinder of astigmatism decreased from −0.80D ± 0.79 (SD) to −0.18 D ± 0.33 (SD) (p < 0.00001). Thus, it could be assumed that the topography measurements were not accurate enough, but we did not have additional data to examine this in more details.
After surgical treatment, the mechanical strength of the cornea depends only on the residual stroma. It is well known that when the residual stroma is too thin to handle IOP, both its anterior and posterior surface will bulge forward as in ectasia. Nowadays, residual stroma thickness (RST) is accepted to be at least 250 µm. Conventionally, thickness less than 480 is considered abnormal, while some surgeons consider preoperative corneal thickness less than 500 µm unsuitable for LASIK. While planning the treatments, 250 µm of the RST was suggested as it accounts for 50% of 500 µm, which is the minimum corneal thickness recommended for LASIK. Also, high percentage of tissue altered (PTA) is the most common cause of ectasia after LASIK in patients with normal preoperative corneal topography. According to Santiago et al. [
13], high values of PTA, especially higher than 40% is important factor in the development post-Lasik ectasia with normal preoperative corneal topography. For that reasonPTA should be taken as one of the screening parameter for refractive surgery candidates. In addition to this criterion, we have aimed at a postoperative thickness of 300 µm residual cornea stroma or more for all cases to allow re-treatment if necessary. None of the eyes in this study developed postoperative ectasia.
The observation, that postoperative central corneal curvature was steeper than planned comes from the fact that the algorithm used for the multifocality add-on causes a central steepening within the 3.0 mm zone. This is because the central zone is intended to be used for near vision. The 3.0 to 6.0 mm zone is adjusted to correct intermediate and distance vision. Both eyes thereby are treated the same way, except that the non-dominant eye is targeted at −0.5D from plano.
The results in this study suggest that the used procedure for presbyLASIK improves vision of presbyopia patients. Hence, we propose to include subjects for the presbyopia treatment older than 48 years, with a mesopic pupil of 3.5–6.5 mm diameter, and with a postoperative Kmean between 35.0D and 47.0D. The central near vision add-ons should be chosen >2.0D. We further suggest that cases where eye surgery was previously performed should not be included, especially cases where corneal refractive surgery was performed. Also, those cases with irregular corneal morphology, lens opacification, natural preoperative multifocality in the cornea, or a central corneal thickness CCT < 500 µm microns should not be included.

 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}