A Robot Arm and Image-Guided Navigation Assisted Surgical System for Maxillary Repositioning in Orthognathic Surgery: A Phantom Skull-Based Trial


Abstract
:1. Introduction
2. Materials and Methods
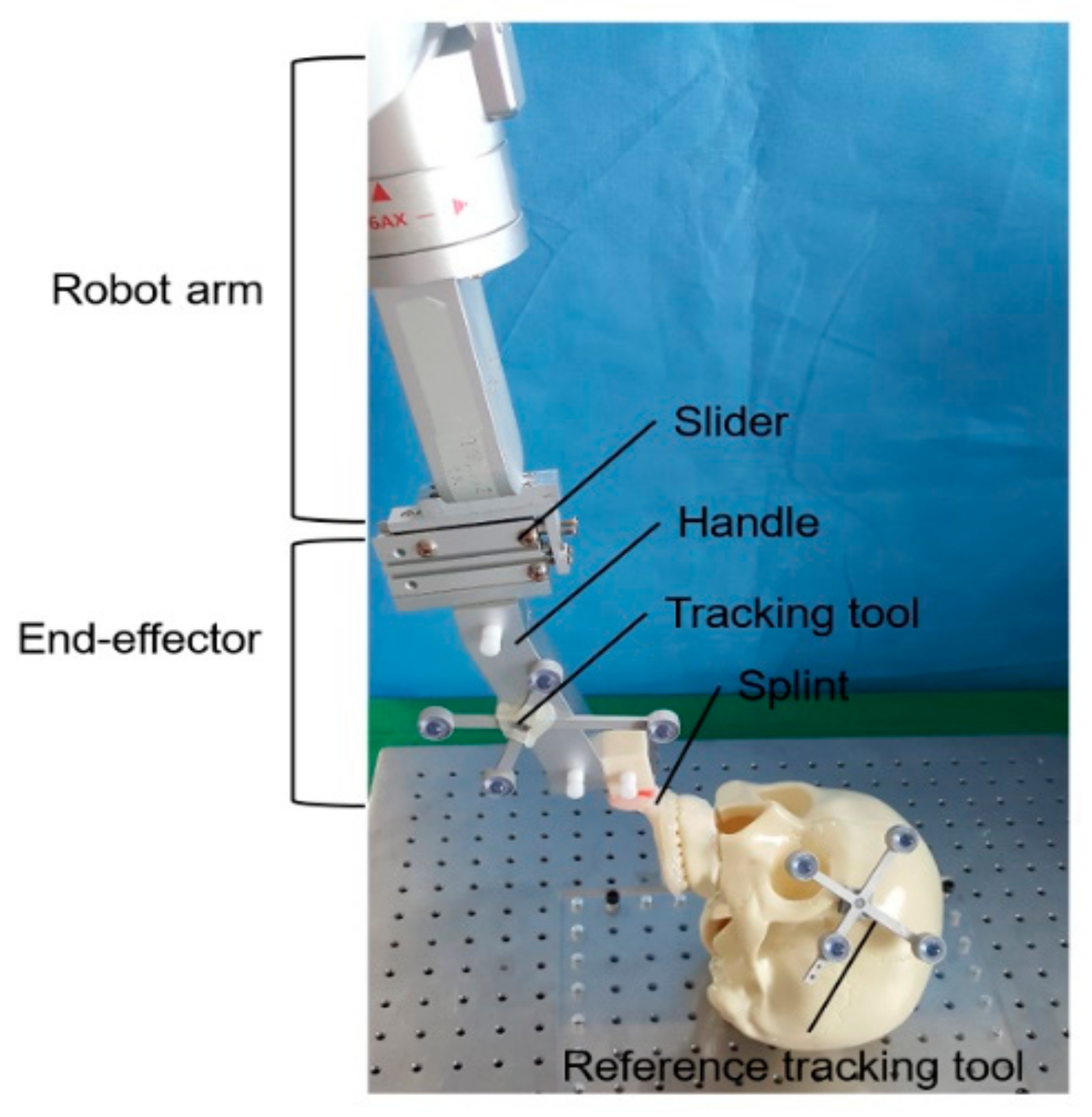
2.1. Robot Arm and Navigation Assisted Orthognathic Vsurgical System
2.2. Workflow
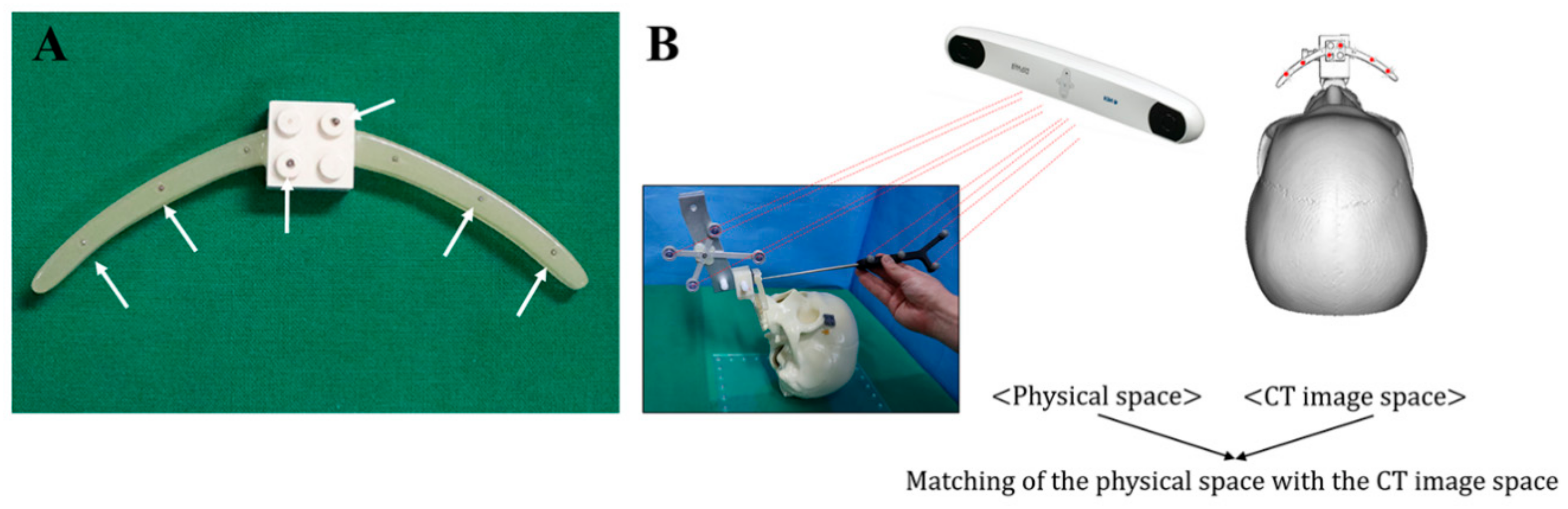
2.2.1. Preoperative Phase
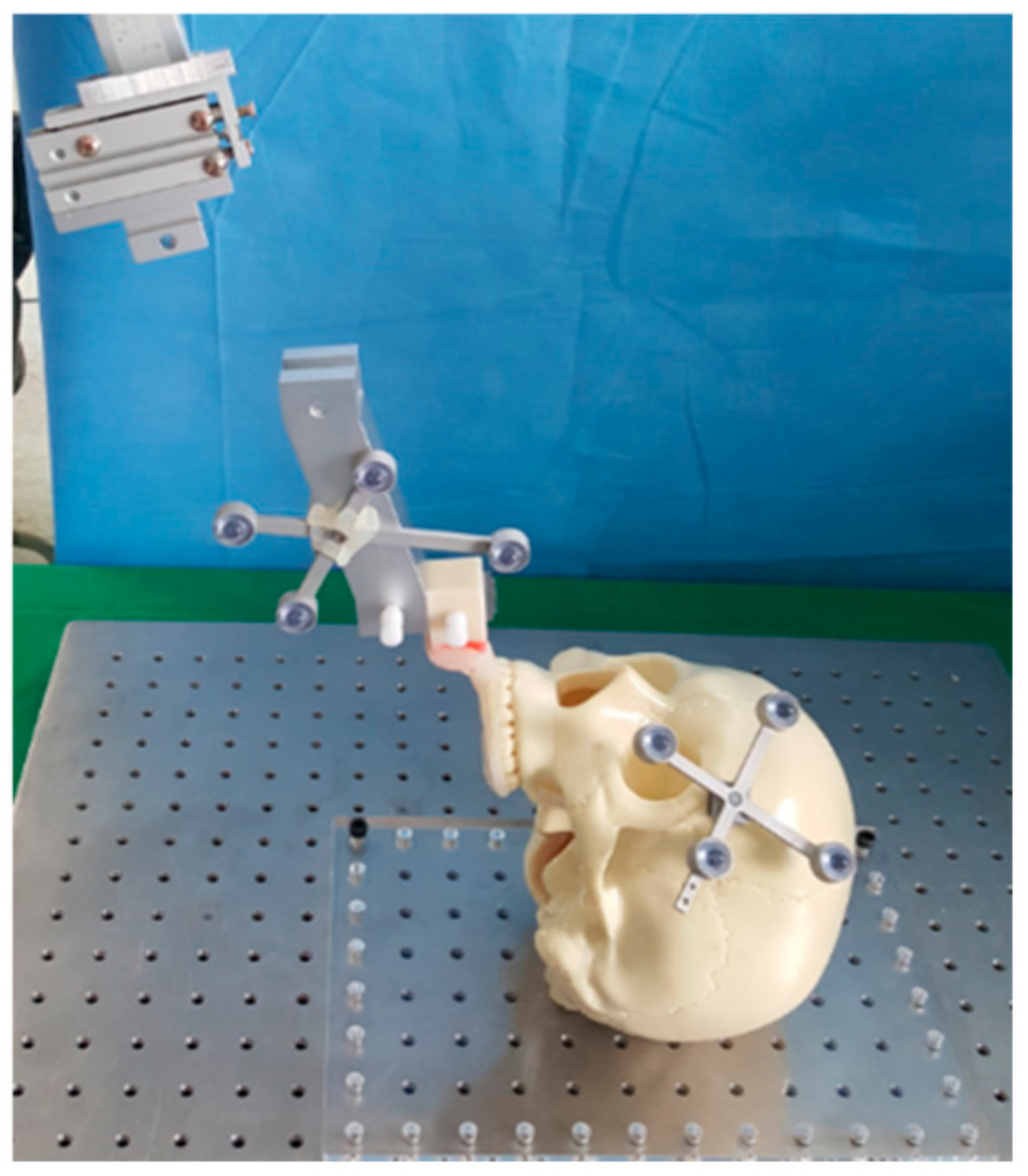
2.2.2. Intraoperative Phase
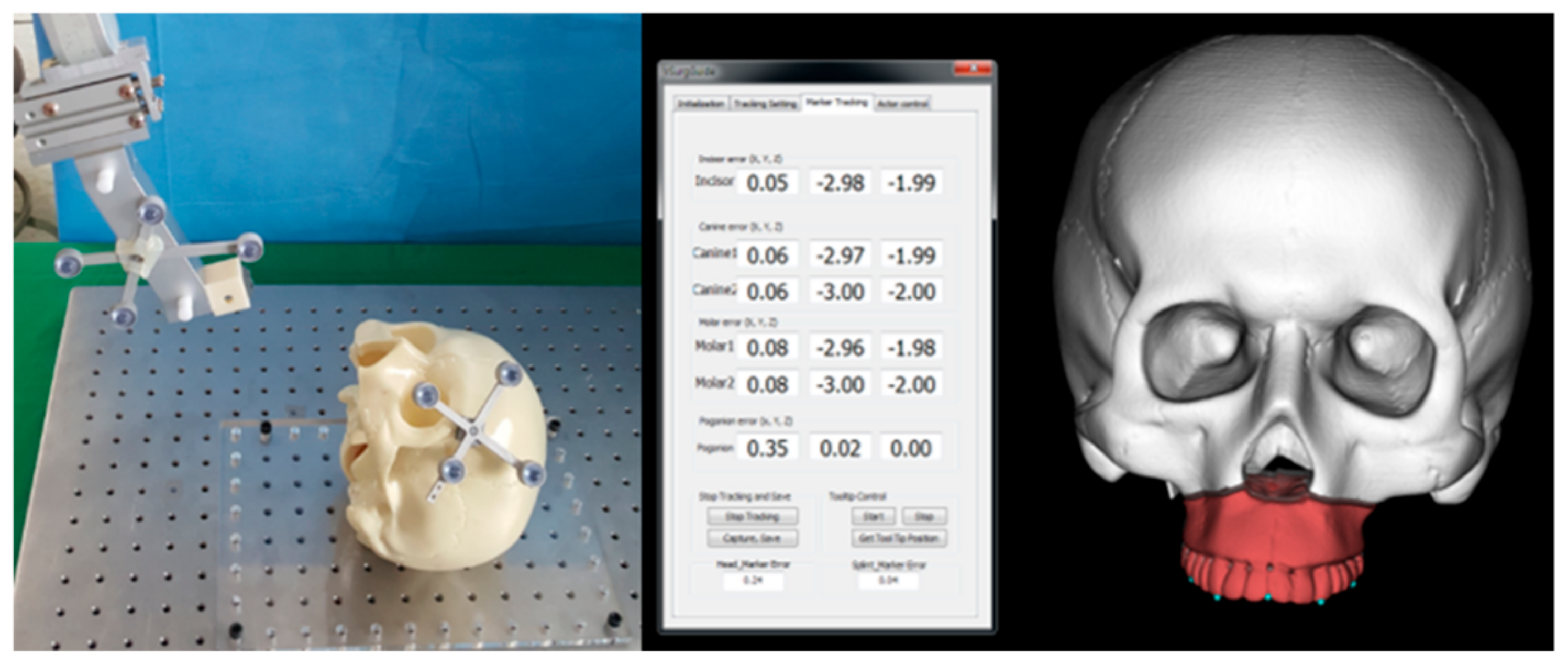
2.3. Accuracy Measurement
3. Results
3.1. Handling of the Robot Arm and Navigation Assisted Orthognathic Surgical System
3.2. Accuracy Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ellis, E. Bimaxillary surgery using an intermediate splint to position the maxilla. J. Oral Maxillofac. Surg. 1999, 57, 53–56. [Google Scholar] [CrossRef]
- Ellis, E. Accuracy of model surgery: Evaluation of an old technique and introduction of a new one. J. Oral Maxillofac. Surg. 1990, 48, 1161–1167. [Google Scholar] [CrossRef]
- Olszewski, R.; Reychler, H. Limitations of orthognathic model surgery: Theoretical and practical implications. Rev. Stomatol. Chir. Maxillofac. 2004, 105, 165–169. [Google Scholar] [CrossRef]
- Gateno, J.; Xia, J.; Teichgraeber, J.F.; Rosen, A.; Hultgren, B.; Vadnais, T. The precision of computer-generated surgical splints. J. Oral Maxillofac. Surg. 2003, 61, 814–817. [Google Scholar] [CrossRef]
- Swennen, G.R.; Mollemans, W.; Schutyser, F. Three-dimensional treatment planning of orthognathic surgery in the era of virtual imaging. J. Oral Maxillofac. Surg. 2009, 67, 2080–2092. [Google Scholar] [CrossRef]
- Zinser, M.J.; Sailer, H.F.; Ritter, L.; Braumann, B.; Maegele, M.; Zoller, J.E. A paradigm shift in orthognathic surgery? A comparison of navigation, computer-aided designed/computer-aided manufactured splints, and “classic” intermaxillary splints to surgical transfer of virtual orthognathic planning. J. Oral Maxillofac. Surg. 2013, 71, e1–e21. [Google Scholar] [CrossRef]
- Van den Bempt, M.; Liebregts, J.; Maal, T.; Berge, S.; Xi, T. Toward a higher accuracy in orthognathic surgery by using intraoperative computer navigation, 3D surgical guides, and/or customized osteosynthesis plates: A systematic review. J. Cranio Maxillofac. Surg. 2018, 46, 2108–2119. [Google Scholar] [CrossRef]
- Gander, T.; Bredell, M.; Eliades, T.; Rucker, M.; Essig, H. Splintless orthognathic surgery: A novel technique using patient-specific implants (PSI). J. Cranio Maxillofac. Surg. 2015, 43, 319–322. [Google Scholar] [CrossRef]
- Han, J.J.; Yang, H.J.; Hwang, S.J. Repositioning of the Maxillomandibular Complex Using Maxillary Template Adjusted Only by Maxillary Surface Configuration Without an Intermediate Splint in Orthognathic Surgery. J. Craniofac. Surg. 2016, 27, 1550–1553. [Google Scholar] [CrossRef]
- Mazzoni, S.; Bianchi, A.; Schiariti, G.; Badiali, G.; Marchetti, C. Computer-aided design and computer-aided manufacturing cutting guides and customized titanium plates are useful in upper maxilla waferless repositioning. J. Oral Maxillofac. Surg. 2015, 73, 701–707. [Google Scholar] [CrossRef]
- Suojanen, J.; Leikola, J.; Stoor, P. The use of patient-specific implants in orthognathic surgery: A series of 32 maxillary osteotomy patients. J. Cranio Maxillofac. Surg. 2016, 44, 1913–1916. [Google Scholar] [CrossRef] [Green Version]
- Heufelder, M.; Wilde, F.; Pietzka, S.; Mascha, F.; Winter, K.; Schramm, A.; Rana, M. Clinical accuracy of waferless maxillary positioning using customized surgical guides and patient specific osteosynthesis in bimaxillary orthognathic surgery. J. Cranio Maxillofac. Surg. 2017, 45, 1578–1585. [Google Scholar] [CrossRef]
- Jakopec, M.; Harris, S.J.; Rodriguez y Baena, F.; Gomes, P.; Cobb, J.; Davies, B.L. The first clinical application of a “hands-on” robotic knee surgery system. Comput. Aided Surg. 2001, 6, 329–339. [Google Scholar] [CrossRef]
- Varma, T.R.; Eldridge, P. Use of the NeuroMate stereotactic robot in a frameless mode for functional neurosurgery. Int. J. Med. Robot. 2006, 2, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Cadiere, G.B.; Himpens, J.; Germay, O.; Izizaw, R.; Degueldre, M.; Vandromme, J.; Capelluto, E.; Bruyns, J. Feasibility of robotic laparoscopic surgery: 146 cases. World J. Surg. 2001, 25, 1467–1477. [Google Scholar] [CrossRef] [PubMed]
- Beasley, R.A. Medical Robots: Current Systems and Research Directions. J. Robot. 2012, 401613. [Google Scholar] [CrossRef]
- Genden, E.M.; Desai, S.; Sung, C.K. Transoral robotic surgery for the management of head and neck cancer: A preliminary experience. Head Neck 2009, 31, 283–289. [Google Scholar] [CrossRef]
- Lin, L.; Shi, Y.; Tan, A.; Bogari, M.; Zhu, M.; Xin, Y.; Xu, H.; Zhang, Y.; Xie, L.; Chai, G. Mandibular angle split osteotomy based on a novel augmented reality navigation using specialized robot-assisted arms--A feasibility study. J. Cranio Maxillofac. Surg. 2016, 44, 215–223. [Google Scholar] [CrossRef]
- Pugin, F.; Bucher, P.; Morel, P. History of robotic surgery: From AESOP(R) and ZEUS(R) to da Vinci(R). J. Visc. Surg. 2011, 148, e3–e8. [Google Scholar] [CrossRef]
- Liu, H.H.; Li, L.J.; Shi, B.; Xu, C.W.; Luo, E. Robotic surgical systems in maxillofacial surgery: A review. Int. J. Oral Sci. 2017, 9, 63–73. [Google Scholar] [CrossRef]
- Woo, S.Y.; Lee, S.J.; Yoo, J.Y.; Han, J.J.; Hwang, S.J.; Huh, K.H.; Lee, S.S.; Heo, M.S.; Choi, S.C.; Yi, W.J. Autonomous bone reposition around anatomical landmark for robot-assisted orthognathic surgery. J. Cranio Maxillofac. Surg. 2017, 45, 1980–1988. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.S.; Woo, S.Y.; Yang, H.J.; Huh, K.H.; Lee, S.S.; Heo, M.S.; Choi, S.C.; Hwang, S.J.; Yi, W.J. An integrated orthognathic surgery system for virtual planning and image-guided transfer without intermediate splint. J. Cranio Maxillofac. Surg. 2014, 42, 2010–2017. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Woo, S.Y.; Huh, K.H.; Lee, S.S.; Heo, M.S.; Choi, S.C.; Han, J.J.; Yang, H.J.; Hwang, S.J.; Yi, W.J. Virtual skeletal complex model- and landmark-guided orthognathic surgery system. J. Cranio Maxillofac. Surg. 2016, 44, 557–568. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.W.; Lin, H.H.; Chortrakarnkij, P.; Kim, S.G.; Lo, L.J. Intraoperative navigation for single-splint two-jaw orthognathic surgery: From model to actual surgery. J. Cranio Maxillofac. Surg. 2015, 43, 1119–1126. [Google Scholar] [CrossRef] [PubMed]
- Chapuis, J.; Schramm, A.; Pappas, I.; Hallermann, W.; Schwenzer-Zimmerer, K.; Langlotz, F.; Caversaccio, M. A new system for computer-aided preoperative planning and intraoperative navigation during corrective jaw surgery. IEEE Trans. Inf. Technol. Biomed. 2007, 11, 274–287. [Google Scholar] [CrossRef]
- Berger, M.; Nova, I.; Kallus, S.; Ristow, O.; Freudlsperger, C.; Eisenmann, U.; Dickhaus, H.; Engel, M.; Hoffmann, J.; Seeberger, R. Can electromagnetic-navigated maxillary positioning replace occlusional splints in orthognathic surgery? A clinical pilot study. J. Cranio Maxillofac. Surg. 2017, 45, 1593–1599. [Google Scholar] [CrossRef]
- Li, B.; Zhang, L.; Sun, H.; Shen, S.G.; Wang, X. A new method of surgical navigation for orthognathic surgery: Optical tracking guided free-hand repositioning of the maxillomandibular complex. J. Craniofac. Surg. 2014, 25, 406–411. [Google Scholar] [CrossRef]
- Burgner, J.; Toma, M.; Vieira, V.; Eggers, G.; Raczkowsky, J.; Muhling, J.; Marmulla, R.; Worn, H. System for robot assisted orthognathic surgery. Int. J. Comput. Assist. Radiol. Surger. 2007, 2, S419–S421. [Google Scholar]
- Vieira, V.M.M.; Kane, G.J.; Ionesco, H.; Raszkowsky, J.; Boesecke, R.; Eggers, G. Light-weight robot stability for orthognathic surgery. Phantom and animal cadavar trials. In Proceedings of the Deutschen Gesellschaft für Computer-und Roboterassistierte Chirurgie, Dusseldorf, Germany, 18–19 November 2010; pp. 99–101. [Google Scholar]
- Wang, X.; Song, R.; Liu, X.; Li, Q.; Cheng, T.; Xue, Y. System design for orthognathic aided robot. In Proceedings of the 5th annual IEEE International Conference on Cyber Technology in Automation, Control and Intelligent Systems, Shenyang, China, 6–10 June 2015; pp. 612–617. [Google Scholar]
- Kwoh, Y.S.; Hou, J.; Jonckheere, E.A.; Hayati, S. A robot with improved absolute positioning accuracy for CT guided stereotactic brain surgery. IEEE Trans. Biomed. Eng. 1988, 35, 153–160. [Google Scholar] [CrossRef]
- Berger, M.; Kallus, S.; Nova, I.; Ristow, O.; Eisenmann, U.; Dickhaus, H.; Kuhle, R.; Hoffmann, J.; Seeberger, R. Approach to intraoperative electromagnetic navigation in orthognathic surgery: A phantom skull based trial. J. Cranio Maxillofac. Surg. 2015, 43, 1731–1736. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Experiment | Surgical Plan |
|---|---|
| #1 | Advancement by 3 mm and downward by 2 mm |
| #2 | Advancement by 3 mm and downward by 2 mm |
| #3 | Cant correction by 4 mm (Right, 2 mm upward; Left, 2 mm downward) |
| #4 | Cant correction by 4 mm (Right, 2 mm upward; Left, 2 mm downward) |
| #5 | Posterior impaction at the upper first molar by 3 mm |
| #6 | Posterior impaction at the upper first molar by 3 mm |
| #7 | Bodily shift to right side by 3 mm |
| #8 | Bodily shift to right side by 3 mm |
| #9 | Advancement by 3 mm and downward by 2 mm |
| #10 | Cant correction by 4 mm (Right, 2 mm upward; Left, 2 mm downward) |
| Upper Incisor Point | Right Upper Canine | Left Upper Canine | Right Upper 1st Molar | Left Upper 1st Molar | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Experiment | x | y | z | x | y | z | x | y | z | x | y | z | x | y | z |
| #1 | 0.51 | 0.03 | 0.41 | 0.43 | 0.14 | 0.31 | 0.42 | 0.18 | 0.14 | 0.27 | 0.07 | 0.12 | 0.25 | 0.43 | 0.39 |
| #2 | 0.19 | 0.21 | 0.36 | 0.14 | 0.31 | 0.16 | 0.14 | 0.10 | 0.34 | 0.00 | 0.25 | 0.13 | 0.00 | 0.07 | 0.13 |
| #3 | 0.14 | 0.14 | 0.22 | 0.18 | 0.24 | 0.15 | 0.19 | 0.04 | 0.18 | 0.26 | 0.33 | 0.03 | 0.28 | 0.04 | 0.07 |
| #4 | 0.05 | 0.02 | 0.04 | 0.06 | 0.04 | 0.01 | 0.06 | 0.00 | 0.02 | 0.08 | 0.03 | 0.08 | 0.09 | 0.02 | 0.04 |
| #5 | 0.00 | 0.00 | 0.00 | 0.02 | 0.04 | 0.02 | 0.02 | 0.05 | 0.01 | 0.05 | 0.07 | 0.04 | 0.05 | 0.05 | 0.01 |
| #6 | 0.02 | 0.02 | 0.05 | 0.02 | 0.01 | 0.05 | 0.03 | 0.04 | 0.09 | 0.03 | 0.02 | 0.07 | 0.03 | 0.07 | 0.13 |
| #7 | 0.06 | 0.07 | 0.03 | 0.07 | 0.08 | 0.02 | 0.07 | 0.06 | 0.05 | 0.07 | 0.08 | 0.03 | 0.07 | 0.05 | 0.06 |
| #8 | 0.01 | 0.03 | 0.02 | 0.01 | 0.03 | 0.00 | 0.01 | 0.04 | 0.01 | 0.01 | 0.05 | 0.03 | 0.01 | 0.07 | 0.05 |
| #9 | 0.00 | 0.00 | 0.05 | 0.02 | 0.04 | 0.07 | 0.02 | 0.05 | 0.05 | 0.06 | 0.06 | 0.09 | 0.06 | 0.06 | 0.07 |
| #10 | 0.04 | 0.02 | 0.01 | 0.05 | 0.01 | 0.01 | 0.05 | 0.02 | 0.02 | 0.05 | 0.01 | 0.01 | 0.05 | 0.03 | 0.03 |
| Mean | 0.10 | 0.05 | 0.12 | 0.10 | 0.09 | 0.08 | 0.10 | 0.06 | 0.09 | 0.09 | 0.10 | 0.06 | 0.09 | 0.09 | 0.10 |
| SD | 0.16 | 0.07 | 0.15 | 0.13 | 0.10 | 0.10 | 0.13 | 0.05 | 0.10 | 0.10 | 0.11 | 0.04 | 0.10 | 0.12 | 0.11 |
| Experiment | #1 | #2 | #3 | #4 | #5 | #6 | #7 | #8 | #9 | #10 | Mean ± SD |
|---|---|---|---|---|---|---|---|---|---|---|---|
| RMSD | 0.54 | 0.35 | 0.33 | 0.09 | 0.06 | 0.10 | 0.11 | 0.06 | 0.09 | 0.05 | 0.18 ± 0.16 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, J.J.; Woo, S.-Y.; Yi, W.-J.; Hwang, S.J. A Robot Arm and Image-Guided Navigation Assisted Surgical System for Maxillary Repositioning in Orthognathic Surgery: A Phantom Skull-Based Trial. Appl. Sci. 2020, 10, 1549. https://0-doi-org.brum.beds.ac.uk/10.3390/app10041549
Han JJ, Woo S-Y, Yi W-J, Hwang SJ. A Robot Arm and Image-Guided Navigation Assisted Surgical System for Maxillary Repositioning in Orthognathic Surgery: A Phantom Skull-Based Trial. Applied Sciences. 2020; 10(4):1549. https://0-doi-org.brum.beds.ac.uk/10.3390/app10041549
Chicago/Turabian StyleHan, Jeong Joon, Sang-Yoon Woo, Won-Jin Yi, and Soon Jung Hwang. 2020. "A Robot Arm and Image-Guided Navigation Assisted Surgical System for Maxillary Repositioning in Orthognathic Surgery: A Phantom Skull-Based Trial" Applied Sciences 10, no. 4: 1549. https://0-doi-org.brum.beds.ac.uk/10.3390/app10041549