Study on the Improvement of Electrical Facility System of Automated External Defibrillators by Real-Time Measurement of Thoracic Impedance


Abstract
:1. Introduction
2. Materials and Methods
2.1. Principles of AED
2.2. Measurement Principles of Thoracic Impedance
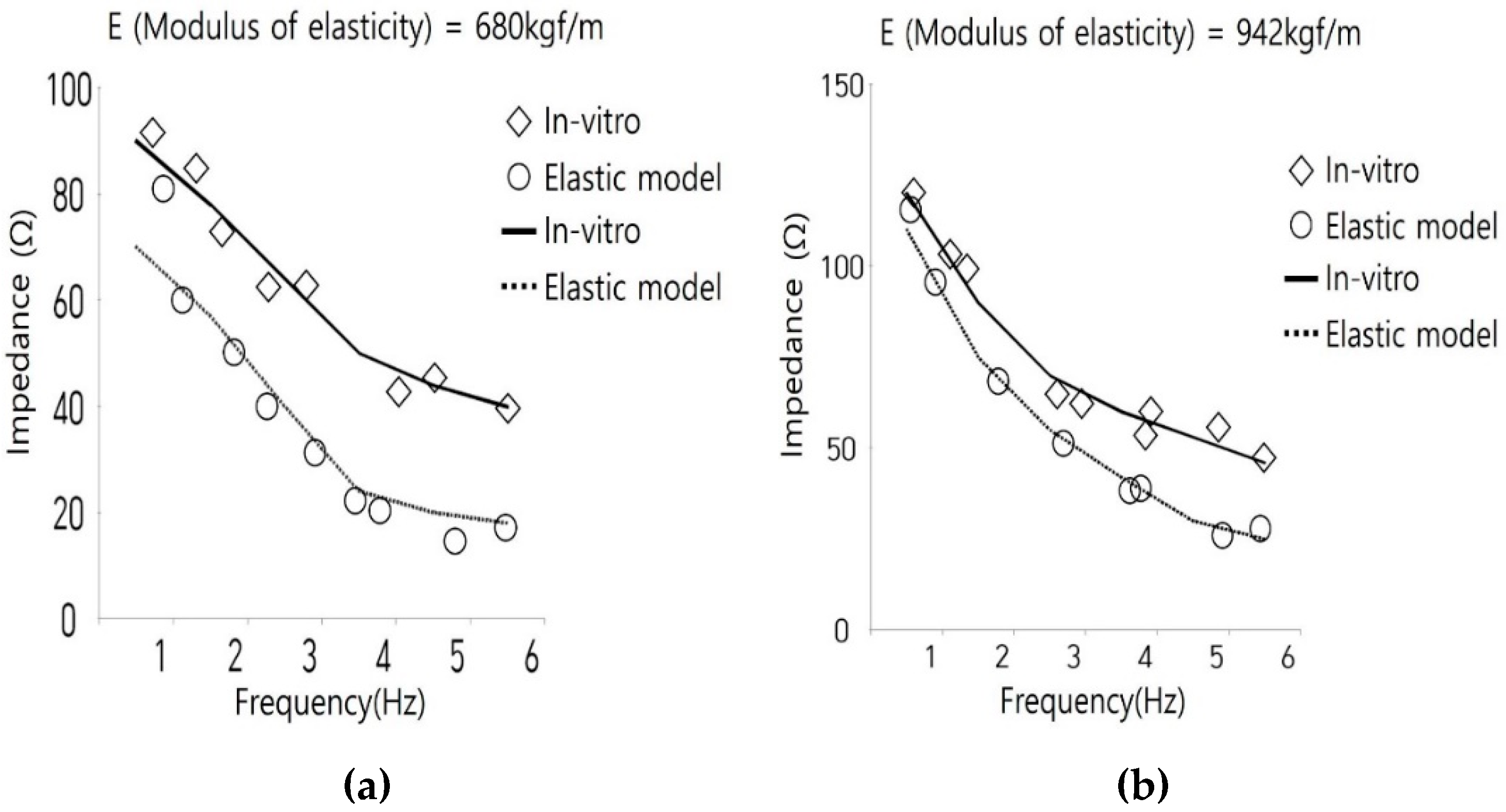
2.3. Changes in Impedance According to CPR
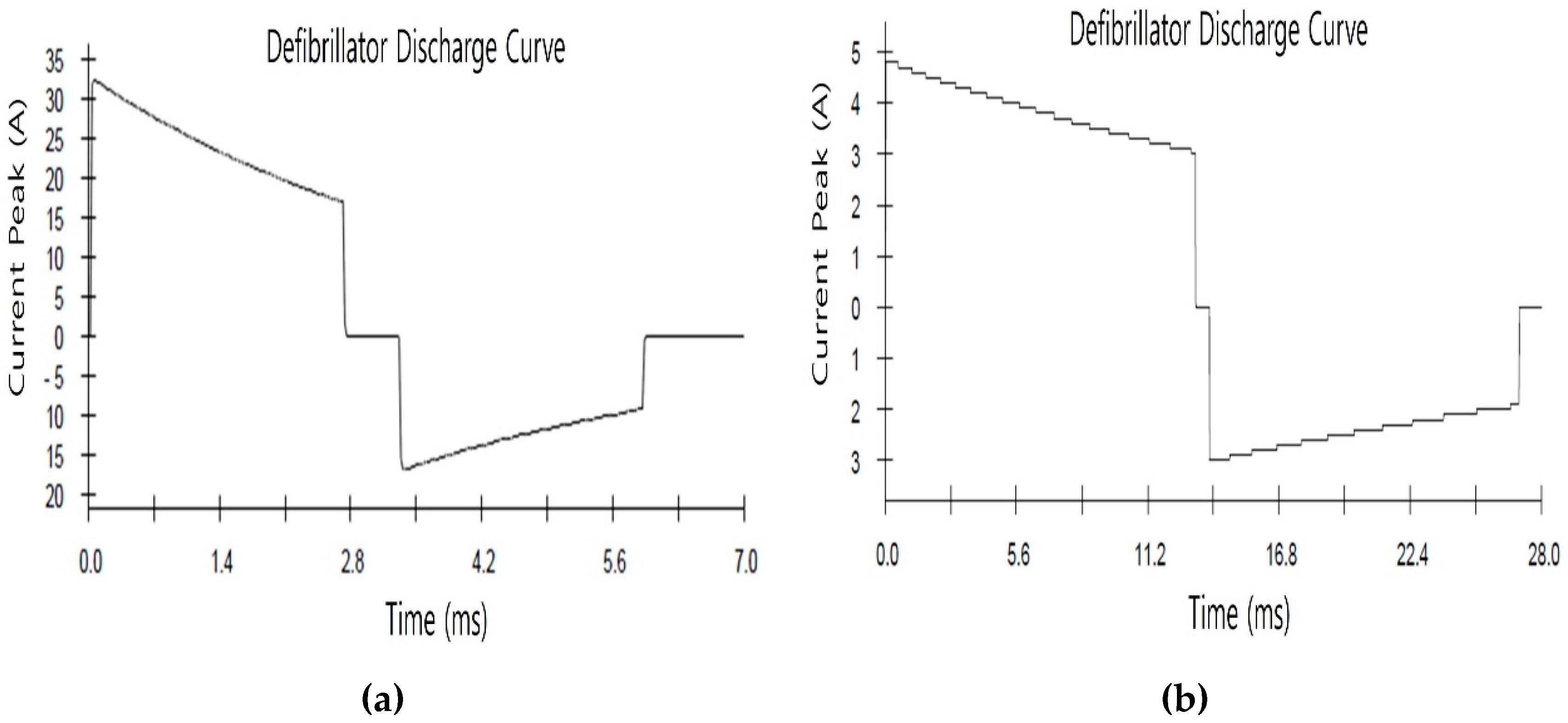
2.4. Experimental Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kim, Y.T. Sudden Cardiac Arrest Survey 2006–2016; Korean Center for Disease Control: Chungcheongbuk-do, Korea, 2017.
- Park, S.J.; Park, S.M.; Kang, S.M.; Choi, S.W. Real-time monitoring of blood flow using mechanical impedance of chest during CPR. Korean Soc. Mech. Eng. 2017, 11, 2377–2379. [Google Scholar]
- Lwami, T.; Kitamura, T.; Kawamura, T.; Mitamura, H.; Nagao, K.; Takayama, M.; Seino, Y.; Tanaka, H.; Nonogi, H.; Yonemoto, N.; et al. Chest compression-only cardiopulmonary resuscitation for out-of-hospital cardiac arrest with public-access defibrillation. Circulation 2012, 126, 2844–2851. [Google Scholar]
- Adabağ, S.A.; Hodgson, L.; Garcia, S.A.; Anand, V.; Frascone, R.J.; Conterato, M.; Lick, C.J.; Wesley, K.; Mahoney, B.D.; Yannopoulos, D. Outcomes of sudden cardiac arrest in a state-wide integrated resuscitation program: Results from the minnesota resuscitation consortium. Resuscitation 2017, 110, 95–100. [Google Scholar] [CrossRef]
- Fernando, S.; Vaillancourt, C.; Morrow, S.; Stiell, I.G. Analysis of bystander CPR quality during out-of-hospital cardiac arrest using data derived from automated external defibrillators. Resuscitation 2018, 128, 138–143. [Google Scholar] [CrossRef]
- Morrow, W.; Berger, S.; Jenkins, K.; Minich, L.; Rosenthal, G.L.; Snyder, C.S.; Twedell, J.; Beekman, R.H.; Klitzner, T.S.; Manning, P.B.; et al. Pediatric sudden cardiac arrest. Pediatrics 2012, 129, 1094–1102. [Google Scholar]
- Marijon, E.; Uy-Evanado, A.; Dumas, F.; Karam, N.; Reinier, K.; Teodorescu, C.; Narayanan, K.; Gunson, K.; Jui, J.; Jouven, X.; et al. Warning symptoms are associated with survival from sudden cardiac arrest. Ann. Intern. Med. 2016, 164, 9–23. [Google Scholar] [CrossRef] [Green Version]
- Mercier, E.; Laroche, E.; Beck, B.; Sage, N.L.; Cameron, P.A.; Émond, M.; Berthelot, S.; Mitra, B.; Ouellet-Pelletier, J. Defibrillation energy dose during pediatric cardiac arrest: Systematic review of human and animal model studies. Resuscitation 2019, 139, 241–252. [Google Scholar] [CrossRef]
- Cho, H.R.; Jo, H.S.; Kim, D.M.; Ha, T.J.; Baek, M.G.; Park, S.K.; Park, S.G. Study on safety requirements and test methods for automated external defibrillators. Infor. Control Symp. 2018, 18, 213–214. [Google Scholar]
- Ristagno, G.; Yu, T.; Quan, W.; Freeman, G.A.; Locke, E. Comparison of defibrillation efficacy between two pads placements in a pediatric porcine model of cardiac arrest. Resuscitation 2012, 83, 755–759. [Google Scholar] [CrossRef]
- Piuzzi, E.; Pisa, S.; Pittella, E.; Podestà, L.; Sangiovanni, S. Comparison among low-cost portable systems for thoracic impedance plethysmography. In Proceedings of the 2017 IEEE International Instrumentation and Measurement Technology Conference, Torino, Italy, 22–25 May 2017; pp. 1–6. [Google Scholar]
- Cho, Y.C.; Kim, M.S.; Yoon, J.O. A study on the electrical difference for the limbs and thoracic impedance using real-time bio-impedance measurement system. J. Korea Ind. Inf. Syst. Res. 2013, 18, 9–16. [Google Scholar]
- Park, J.Y. Enhancement of Automatic Defibrillator Simulated Algorithm by ECG and Chest Impedance Signal Analysis. Master’s Thesis, Yonsei University, Seoul, Korea, 2015. [Google Scholar]
- Alonso, E.; Aramendi, E.; Daya, M.; Irusta, U.; Chicote, B.; Russell, J.; Tereshchenko, L. Circulation detection using the electrocardiogram and the thoracic impedance acquired by defibrillation pads. Resuscitation 2016, 99, 56–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Losert, H.; Risdal, M.; Sterz, F.; Nysæther, J.B.; Köhler, K.W.; Eftestøl, T.C.; Wandaller, C.; Myklebust, H.; Uray, T.; Aase, S.O.; et al. Thoracic-impedance changes measured via defibrillator pads can monitor signs of circulation. Resuscitation 2007, 73, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Kuang, S.J.; He, B.Q.; Wang, Z.M.; Cheng, X.L. Measurement method and principle for thoracic impedance graph. MATEC Web Conf. 2017, 128, 4. [Google Scholar]
- Kabiri, L.S.; Hernandez, D.; Mitchell, K. Reliability, validity, and diagnostic value of a pediatric bioelectrical impedance analysis scale. Child. Obes. 2015, 11, 650–655. [Google Scholar] [CrossRef]
- González-Otero, D.M.; Gauna, S.R.D.; Ruiz, J.J.; Ayala, U.; Alonso, E. Automatic detection of chest compression pauses using the transthoracic impedance signal. Comput. Cardiol. 2012, 39, 21–24. [Google Scholar]
- Ruiz, J.M.; Alonso, E.; Aramendi, E.; Kramer-Johansen, J.; Eftestøl, T.C.; Ayala, U.; Gonzalez-Otero, D. Reliable extraction of the circulation component in the thoracic impedance measured by defibrillation pads. Resuscitation 2013, 84, 1345–1352. [Google Scholar] [CrossRef]
- Meredith-Jones, K.; Williams, S.; Taylor, R. Bioelectrical impedance as a measure of change in body composition in young children. Pediatr. Obes. 2015, 10, 252–259. [Google Scholar] [CrossRef]
- Ruiz, J.M.; Gauna, S.R.D.; Gonzalez-Otero, D.; Saiz, P.; Gutiérrez, J.J.; Veintemillas, J.F.; Bastida, J.M.; Alonso, D. Circulation assessment by automated external defibrillators during cardiopulmonary resuscitation. Resuscitation 2018, 128, 158–163. [Google Scholar] [CrossRef]
- Kwok, H.; Coult, J.; Liu, C.; Blackwood, J.; Kudenchuk, P.J.; Rea, T.D.; Sherman, L.D. An accurate method for real-time chest compression detection from the impedance signal. Resuscitation 2016, 105, 22–28. [Google Scholar] [CrossRef]
- Gruber, J.; Stumpf, D.; Zapletal, B.; Neuhold, S.; Fischer, H. Real-time feedback systems in CPR. Trends Anaesth. Crit. Care 2012, 2, 287–297. [Google Scholar] [CrossRef]
- Lee, D.Y.; Kang, S.M.; Choi, S.W. Mechanical impedance monitoring system of the patient’s chest during cardiopulmonary resuscitation. Korean Soc. Mech. Eng. 2018, 42, 583–587. [Google Scholar] [CrossRef]
- Berve, P.O.; Irusta, U.; Kramer-Johansen, J.; Skålhegg, T.; Kongsgård, H.W.; Brunborg, C.; Aramendi, E.; Wik, L. Transthoracic impedance measured with defibrillator pads—New interpretations of signal change induced by ventilations. Clin. Med. 2019, 8, 724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, S.M.; Choi, S.W. Monitoring mechanical impedance of the thorax with compression and decompression cardiopulmonary resuscitation device. J. Mech. Sci. Technol. 2019, 33, 981–988. [Google Scholar] [CrossRef]
- Arbogast, K.B.; Maltese, M.; Nadkarni, V.; Steen, P.A.; Nysæther, J. Anterior-posterior thoracic force-deflection characteristics measured during cardiopulmonary resuscitation: Comparison to post-mortem human subject data. Stapp Car Crash J. 2006, 50, 131–145. [Google Scholar] [PubMed]
- Medical Device Performance Test Guidance 2010; Korean Food and Drug Administration: Seoul, Korea, 2010.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name | Description |
|---|---|
| IEC 60601-2-4:2010 | Medical electrical equipment-part 2-4: Particular requirements for the basic safety and essential performance of cardiac defibrillators. |
| Impedance (Ω) | First Peak Voltage (v) | First Peak Current (A) | Second Peak Voltage (V) | Second Peak Current (A) | Amount of Energy (J) |
|---|---|---|---|---|---|
| 25 | 1411 | 56.4 | 1044 | 29.8 | 156.0 |
| 50 | 1423 | 28.5 | 848 | 17.0 | 148.4 |
| 75 | 1467 | 19.6 | 906 | 12.1 | 153.5 |
| 100 | 1462 | 14.6 | 914 | 9.1 | 150.8 |
| 125 | 1468 | 11.7 | 925 | 7.4 | 151.3 |
| 150 | 1471 | 9.8 | 930 | 6.2 | 150.7 |
| 175 | 1474 | 8.4 | 935 | 5.3 | 150.9 |
| Impedance (Ω) | First Peak Voltage (v) | First Peak Current (A) | Second Peak Voltage (V) | Second Peak Current (A) | Amount of Energy (J) |
|---|---|---|---|---|---|
| 25 | 807 | 32.2 | 420 | 16.8 | 50.4 |
| 50 | 829 | 16.5 | 489 | 9.8 | 49.6 |
| 75 | 840 | 11.2 | 513 | 6.8 | 49.4 |
| 100 | 844 | 8.4 | 522 | 5.2 | 49.6 |
| 125 | 843 | 6.7 | 525 | 4.2 | 49.0 |
| 150 | 846 | 5.6 | 528 | 3.5 | 49.2 |
| 175 | 847 | 4.8 | 532 | 3.0 | 49.0 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ha, T.-J.; Park, H.-G.; Park, S.-K.; Park, S.-G. Study on the Improvement of Electrical Facility System of Automated External Defibrillators by Real-Time Measurement of Thoracic Impedance. Appl. Sci. 2020, 10, 3323. https://0-doi-org.brum.beds.ac.uk/10.3390/app10093323
Ha T-J, Park H-G, Park S-K, Park S-G. Study on the Improvement of Electrical Facility System of Automated External Defibrillators by Real-Time Measurement of Thoracic Impedance. Applied Sciences. 2020; 10(9):3323. https://0-doi-org.brum.beds.ac.uk/10.3390/app10093323
Chicago/Turabian StyleHa, Tae-Jin, Hong-Gyu Park, Su-Kang Park, and Sang-Geon Park. 2020. "Study on the Improvement of Electrical Facility System of Automated External Defibrillators by Real-Time Measurement of Thoracic Impedance" Applied Sciences 10, no. 9: 3323. https://0-doi-org.brum.beds.ac.uk/10.3390/app10093323