
Evaluation of Dental Surface after De-Bonding Orthodontic Bracket Bonded with a Novel Fluorescent Composite: In Vitro Comparative Study

 ,
,  ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
- -
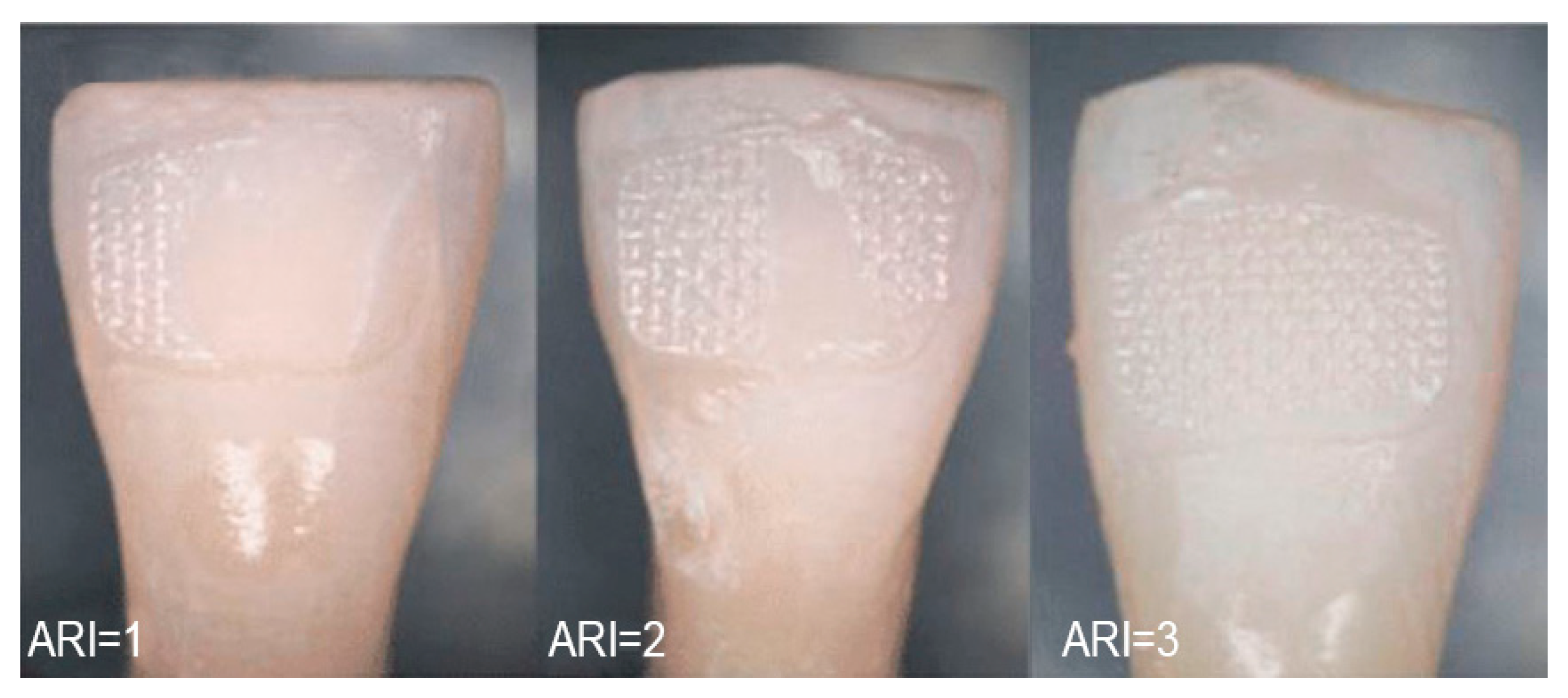
- Grade 0: visible composite residuals OR significant damage to the enamel surface visible without 5× magnification from any view OR any anatomical change to the tooth;
- -
- Grade 1: minor enamel scratching or damage not exposing the dentine, which was partially visible without 5× magnification from some views or/and composite residuals visible using 5× magnification only;
- -
- Grade 2: absence of scratches or presence of minor scratches in the enamel surface, visible only with the use of 5× magnification.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mohebi, S.; Shafiee, H.-A.; Ameli, N. Evaluation of enamel surface roughness after orthodontic bracket debonding with atomic force microscopy. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 521–527. [Google Scholar] [CrossRef]
- Bollen, C.M.; Lambrechts, P.; Quirynen, M. Comparison of surface roughness of oral hard materials to the threshold surface roughness for bacterial plaque retention: A review of the literature. Dent. Mater. 1997, 13, 258–269. [Google Scholar] [CrossRef]
- Goel, A.; Singh, A.; Gupta, T.; Gambhir, R.S. Evaluation of surface roughness of enamel after various bonding and clean-up procedures on enamel bonded with three different bonding agents: An in-vitro study. J. Clin. Exp. Dent. 2017, 9, e608–e616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Attin, R.; Stawarczyk, B.; Kecik, D.; Knosel, M.; Wiechmann, D.; Attin, T. Shear bond strength of brackets to demineralize enamel after different pretreatment methods. Angle Orthod. 2012, 82, 56–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janiszewska-Olszowska, J.; Szatkiewicz, T.; Tomkowski, R.; Tandecka, K.; Grocholewicz, K. Effect of orthodontic debonding and adhesive removal on the enamel–current knowledge and future perspectives—A systematic review. Med. Sci. Monit. Basic Res. 2014, 20, 1991–2001. [Google Scholar]
- Krithikadatta, J.; Gopikrishna, V.; Datta, M. CRIS Guidelines (Checklist for Reporting In-vitro Studies): A concept note on the need for standardized guidelines for improving quality and transparency in reporting in-vitro studies in experimental dental research. J. Conserv. Dent. 2014, 17, 301–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, X.-C.; Chen, L.; Huang, X.-F. Effects of various debonding and adhesive clearance methods on enamel surface: An in vitro study. BMC Oral Health 2017, 17, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.-S.; Park, W.-K.; Son, W.-S.; Ahn, H.-S.; Ro, J.-H.; Kim, Y.-D. Enamel surface evaluation after removal of orthodontic composite remnants by intraoral sandblasting: A 3-dimensional surface profilometry study. Am. J. Orthod. Dentofac. Orthop. 2007, 132, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Maspero, C.; Giannini, L.; Galbiati, G.; Nolet, F.; Esposito, L.; Farronato, G. Titanium orthodontic appliances for allergic patients. Minerva Stomatol. 2014, 63, 403–410. [Google Scholar]
- Dubey, C.; Prakash, A.; Sharma, A.; Jain, U. Enigma of Debonding. Orthod. J. Nepal 2016, 5, 37–41. [Google Scholar] [CrossRef]
- Ribeiro, A.A.; Almeida, L.F.; Martins, L.P.; Martins, R.P. Assessing adhesive remnant removal and enamel damage with ultraviolet light: An in-vitro study. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 292–296. [Google Scholar] [CrossRef] [Green Version]
- Montasser, M.A.; Drummond, J.L. Reliability of the adhesive remnant index score system with different magnifications. Angle Orthod. 2009, 79, 773–776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Årtun, J.; Bergland, S. Clinical trials with crystal growth conditioning as an alternative to acid-etch enamel pretreatment. Am. J. Orthod. Dentofac. Orthop. 1984, 85, 333–340. [Google Scholar] [CrossRef]
- Bishara, S.E.; Trulove, T.S. Comparisons of different debonding techniques for ceramic brackets: An in vitro study. Am. J. Orthod. Dentofac. Orthop. 1990, 98, 145–153. [Google Scholar] [CrossRef]
- Oz, A.A.; Yazicioglu, S.; Arici, N.; Akdeniz, B.S.; Murat, N.; Arıcı, S. Assessment of the Confidence of the Adhesive Remnant Index Score with Different Methods. Turk. J. Orthod. 2014, 26, 149–153. [Google Scholar] [CrossRef] [Green Version]
- Cehreli, S.B.; Polat-Ozsoy, O.; Sar, C.; Cubukcu, H.E. A comparative study of qualitative and quantitative methods for the assessment of adhesive remnant after bracket debonding. Eur. J. Orthod. 2011, 34, 188–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arima, S.; Namura, Y.; Tamura, T.; Shimizu, N. Easy Debonding of Ceramic Brackets Bonded with a Light-Cured Orthodontic Adhesive Containing Microcapsules with a CO2 Laser. Photomed. Laser Surg. 2018, 36, 162–168. [Google Scholar] [CrossRef]
- Dumbryte, I.; Linkeviciene, L.; Linkevicius, T.; Malinauskas, M. Does orthodontic debonding lead to tooth sensitivity? Comparison of teeth with and without visible enamel microcracks. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 284–291. [Google Scholar] [CrossRef] [PubMed]
- D’Apuzzo, F.; Perillo, L.; Delfino, I.; Portaccio, M. Monitoring early phases of orthodontic treatment by means of Raman spectroscopies. J. Biomed. Opt. 2017, 22, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grassia, V.; Gentile, E.; Di Stasio, D.; Jamilian, A.; Matarese, G.; D’Apuzzo, F.; Lucchese, A. In vivo confocal microscopy analysis of enamel defects after orthodontic treatment: A preliminary study. Ultrastruct. Pathol. 2016, 40, 317–323. [Google Scholar] [CrossRef]
- Farronato, G.; Giannini, L.; Galbiati, G.; Cannalire, P.; Martinelli, G.; Tubertini, I.; Maspero, C. Oral tissues and orthodontic treatment: Common side effects. Minerva Stomatol. 2013, 62, 431–446. [Google Scholar] [PubMed]
- Taha, A.; Hill, R.G.; Fleming, P.S.; Patel, M.P. Development of a novel bioactive glass for air-abrasion to selectively remove orthodontic adhesives. Clin. Oral Investig. 2017, 22, 1839–1849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farronato, M.; Maspero, C.; Lanteri, V.; Fama, A.; Ferrati, F.; Pettenuzzo, A.; Farronato, D. Current state of the art in the use of augmented reality in dentistry: A systematic review of the literature. BMC Oral Health 2019, 19, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, J.T.L.; Borsatto, M.C.; Saraiva, M.C.P.; Matsumoto, M.A.N.; Torres, C.P.; Romano, F.L. Evaluation of Enamel Roughness in Vitro After Orthodontic Bracket Debonding Using Different Methods of Residual Adhesive Removal. Turk. J. Orthod. 2020, 33, 43–51. [Google Scholar] [CrossRef]
- Pinho, M.; Manso, M.C.; Almeida, R.F.; Martin, C.; Carvalho, O.; Henriques, B.; Silva, F.; Ferreira, A.P.; Souza, J.C.M. Bond Strength of Metallic or Ceramic Orthodontic Brackets to Enamel, Acrylic, or Porcelain Surfaces. Materials 2020, 13, 5197. [Google Scholar] [CrossRef]
- Tartaglia, G.; Mapelli, A.; Maspero, C.; Santaniello, T.; Serafin, M.; Farronato, M.; Caprioglio, A. Direct 3D Printing of Clear Orthodontic Aligners: Current State and Future Possibilities. Materials 2021, 14, 1799. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| DFC | DSC | |
|---|---|---|
| Operator #1 | 40 s | 234 s |
| Operator #2 | 60 s | 87 s |
| Operator #3 | 36 s | 54 s |
| Operator #4 | 23 s | 56 s |
| Operator #5 | 17 s | 31 s |
| Operator #6 | 37 s | 67 s |
| Operator #7 | 40 s | 80 s |
| Operator #8 | 53 s | 27 s |
| Operator #9 | 37 s | 69 s |
| Operator #10 | 41 s | 66 s |
| SD | 12.4 | 58.3 |
| mean | 38 s | 77 s |
| maximum | 60 s | 234 s |
| minimum | 17 s | 27 s |
| Mann–Whitney | p = 0.015 | |
| 95% C.I. | 19.9 |
| Operator | A.R.I Grade | Grades Description | |
|---|---|---|---|
| DFC | DSC | ||
| Operator #1 | 2 | 1 | 0 grade: visible composite remnants OR significant damage to the enamel surface visible without loupes 5× from any projection of the observer OR any anatomical change to the tooth. |
| Operator #2 | 1 | 1 | 1 grade: minor enamel scratching or damage with no exposition of the dentine partially visible without loupes 5× from a limited number of visible projections of the observer or/and composite remnants visible with loupes 5× only. |
| Operator #3 | 2 | 1 | 2 grade: absence or presence of minor scratches to the enamel surface visible only with the use of head-worn loupe 5×. |
| Operator #4 | 2 | 0 | |
| Operator #5 | 2 | 0 | |
| Operator #6 | 2 | 1 | |
| Operator #7 | 2 | 2 | |
| Operator #8 | 2 | 2 | |
| Operator #9 | 1 | 2 | |
| Operator #10 | 2 | 1 | |
| Operator #11 | 2 | 2 | |
| Operator #12 | 1 | 1 | |
| Operator #13 | 1 | 1 | |
| Operator #14 | 2 | 2 | |
| Operator #15 | 1 | 1 | |
| Operator #16 | 2 | 0 | |
| Operator #17 | 2 | 2 | |
| Operator #18 | 1 | 1 | |
| Operator #19 | 1 | 1 | |
| Operator #20 | 1 | 0 | |
| experienced op | 2 | 1 | |
| experienced op | 2 | 1 | |
| experienced op | 2 | 2 | |
| experienced op | 2 | 2 | |
| st. dev. | 0.48 | 0.70 | |
| average | 1.67 | 1.17 | |
| MAX | 2 | 2 | |
| MIN | 1 | 0 | |
| Pearson | p = 0.006 | ||
| 95% C.I. | 0.182997 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Farronato, M.; Farronato, D.; Inchingolo, F.; Grassi, L.; Lanteri, V.; Maspero, C. Evaluation of Dental Surface after De-Bonding Orthodontic Bracket Bonded with a Novel Fluorescent Composite: In Vitro Comparative Study. Appl. Sci. 2021, 11, 6354. https://0-doi-org.brum.beds.ac.uk/10.3390/app11146354
Farronato M, Farronato D, Inchingolo F, Grassi L, Lanteri V, Maspero C. Evaluation of Dental Surface after De-Bonding Orthodontic Bracket Bonded with a Novel Fluorescent Composite: In Vitro Comparative Study. Applied Sciences. 2021; 11(14):6354. https://0-doi-org.brum.beds.ac.uk/10.3390/app11146354
Chicago/Turabian StyleFarronato, Marco, Davide Farronato, Francesco Inchingolo, Laura Grassi, Valentina Lanteri, and Cinzia Maspero. 2021. "Evaluation of Dental Surface after De-Bonding Orthodontic Bracket Bonded with a Novel Fluorescent Composite: In Vitro Comparative Study" Applied Sciences 11, no. 14: 6354. https://0-doi-org.brum.beds.ac.uk/10.3390/app11146354