
Assessment and Brain Training of Patients Experiencing Head and Facial Pain with a Distortion of Orofacial Somatorepresentation: A Narrative Review


Abstract
:1. Introduction
2. Dysfunctional COFP
3. Motor and Somatosensory Disturbances in COFP
4. Orofacial Somatorepresentation Distortion (OFSD)
5. Cognitive and Emotional Disturbances
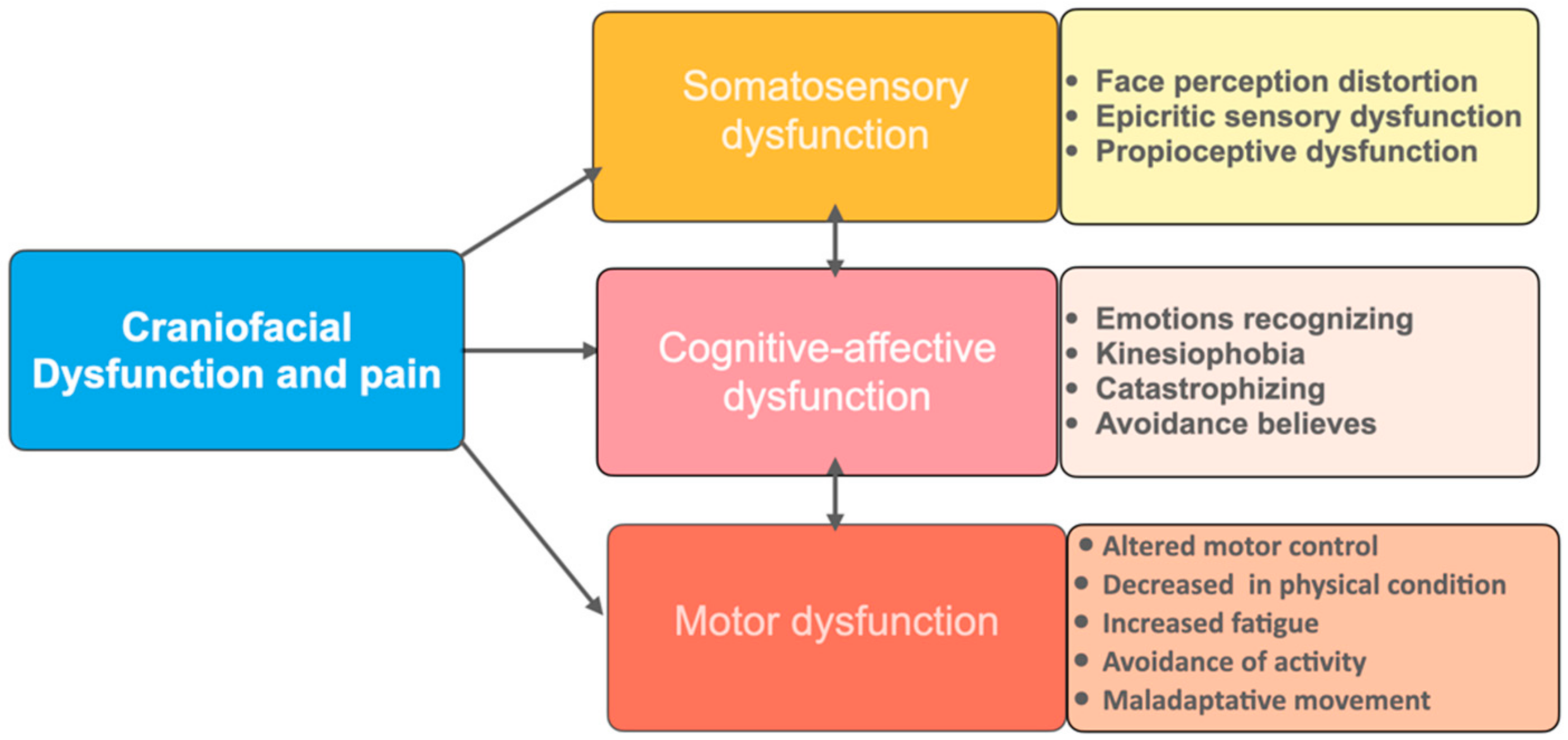
6. Consequences of the Sensorimotor and Emotional Disturbances in COFP
7. Clinical Assessment
7.1. Questionnaires
7.1.1. Craniofacial Pain and Disability Inventory (CF-PDI)
7.1.2. Toronto Alexithymia Scale 26 (TAS-26)
7.1.3. Tampa Scale for Kinesiophobia for Temporomandibular Disorders (TSK-TMD-S)
7.2. Individual Face Perception (IFP)
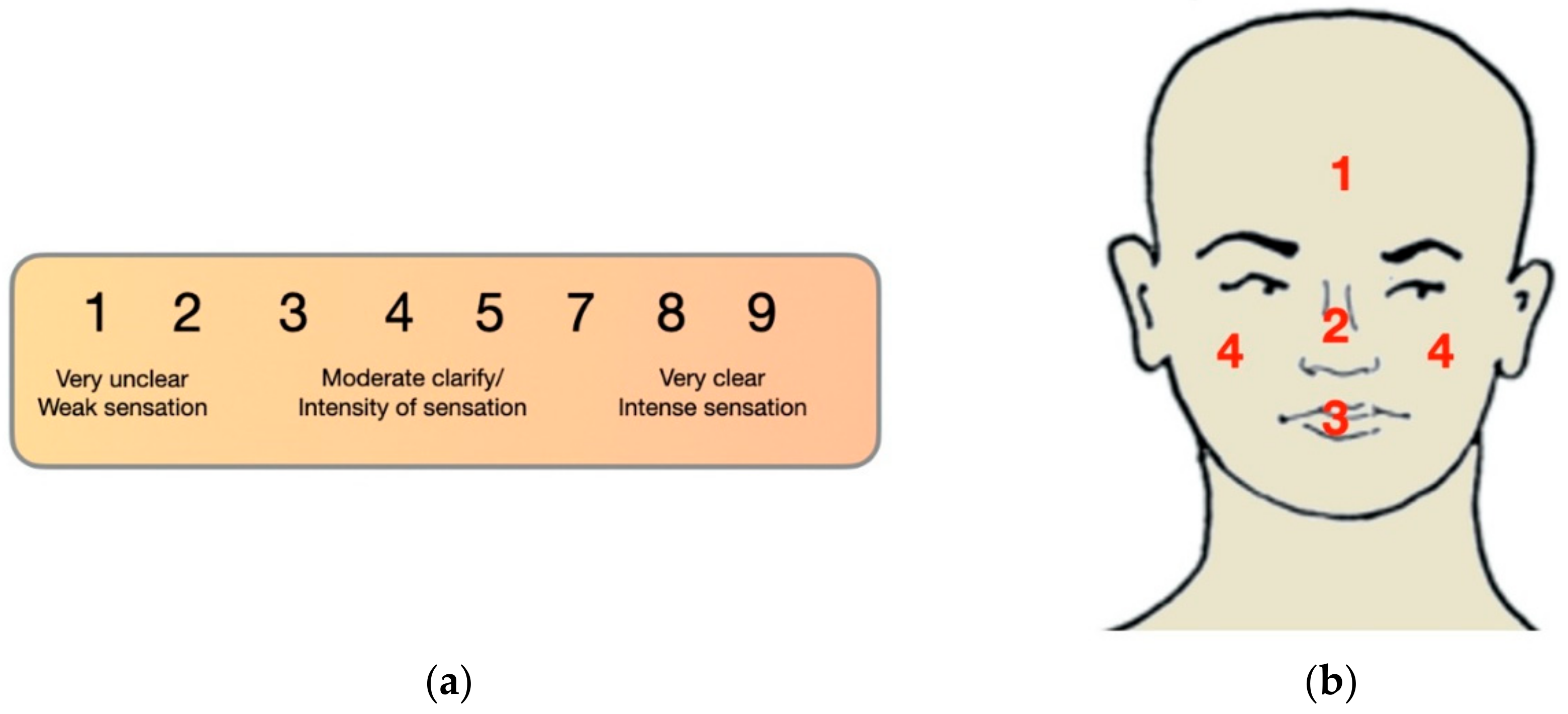
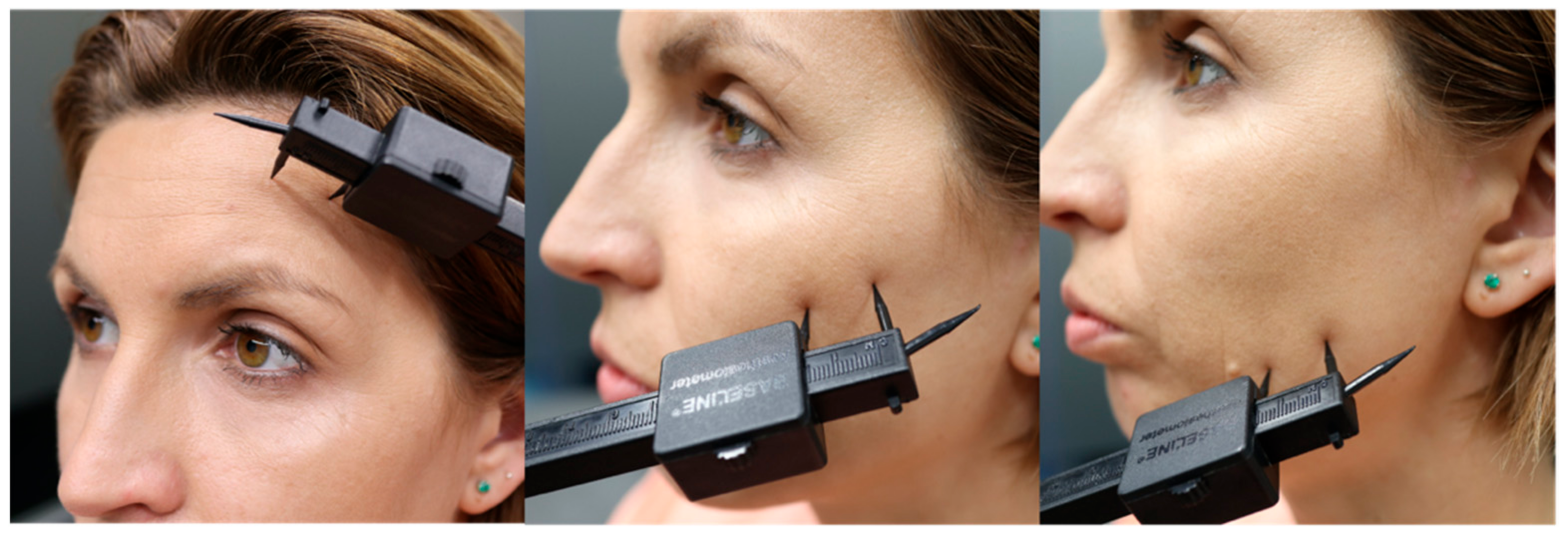
7.3. Two-Point Discrimination
7.4. Laterality Discrimination
7.5. Emotions Recognition
- Reading the Mind in the Eyes Test (RMET) is a test based on facial mimicry that includes 36 photographs of male and female eyes depicting emotional states. For each photograph, participants are asked to choose the emotional state that best describes the eyes, choosing between one of four possible emotions. In the present study, the performance of the participants was calculated as the number of correct responses divided by the total number of trials [131]. The internal consistency for the sample of our study was acceptable (Cronbach’s α = 0.67) [132].
- The Facially Expressed Emotion Labeling (FEEL) test is a computer-based test measures one’s ability to recognize facially expressed basic emotions. The stimuli which the subject has to recognize consist of 42 photographs showing facial displays of six basic emotions which are presented on a computer screen for 300 ms. The test is reliable and has good internal consistency (Cronbach’s coefficient alpha of r = 0.76) [133].
- Myfacetraining (MFT-CRAFTA) software that can be used as assessment and intervention for PC and other devices. The principle is the same as for the FEEL Test (https://www.myfacetraining.com, accessed on 20 June 2021).
7.6. Motor Acuity
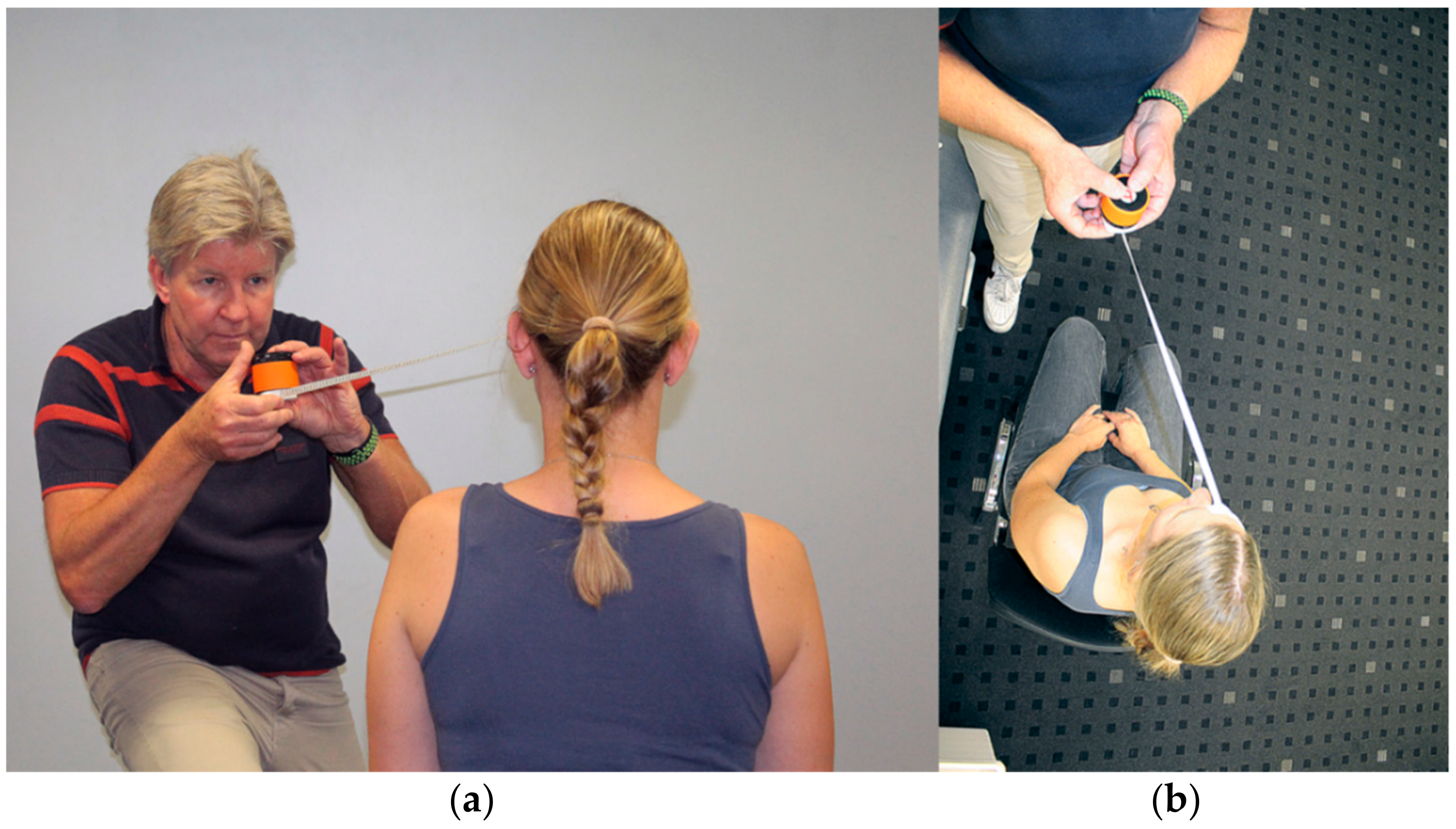
7.6.1. Craniocervical Motor Control
7.6.2. Masticatory Test
7.6.3. Tongue Function
7.7. Auditory Acuity
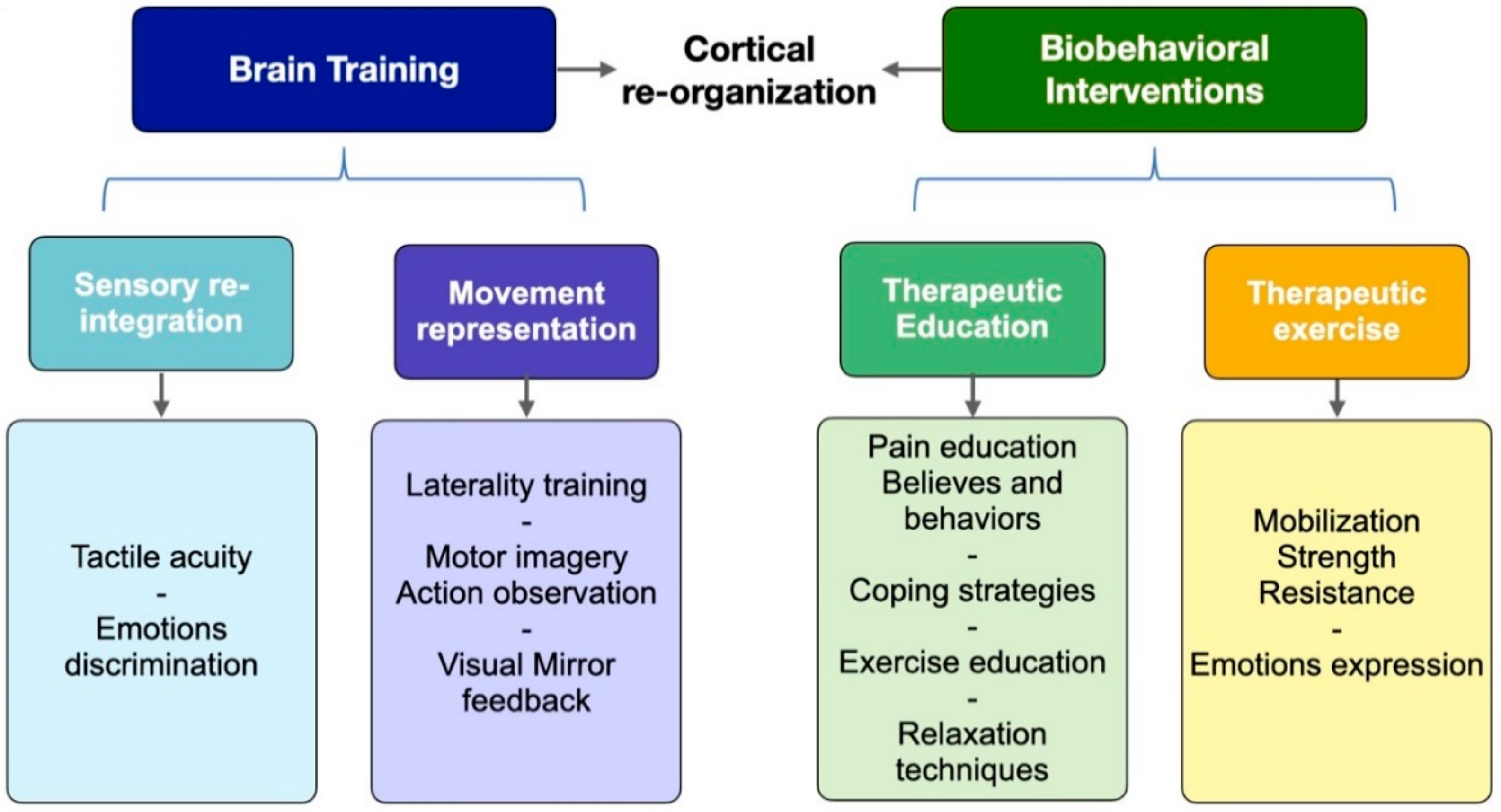
8. Brain-Based Intervention Strategies
8.1. Somatosensory Reintegration
8.2. Emotions Representation
8.3. Movement Representation Techniques
9. Treatment Proposals
9.1. Tactile Acuity Training
9.1.1. Tactile Sensitivity Training
9.1.2. Directional Sensitivity Training
9.1.3. Two-Point Discrimination Training
9.1.4. Enfacement Training
9.2. Movement Representation Techniques
9.2.1. Left/Right Recognition
9.2.2. Motor Imagery and/or Action Observation
9.2.3. Visual Mirror Feedback Therapy
9.3. Emotions Representation
9.3.1. Emotions Recognition
9.3.2. Facial Expression Training
9.4. Face Motor Training through Movement Execution
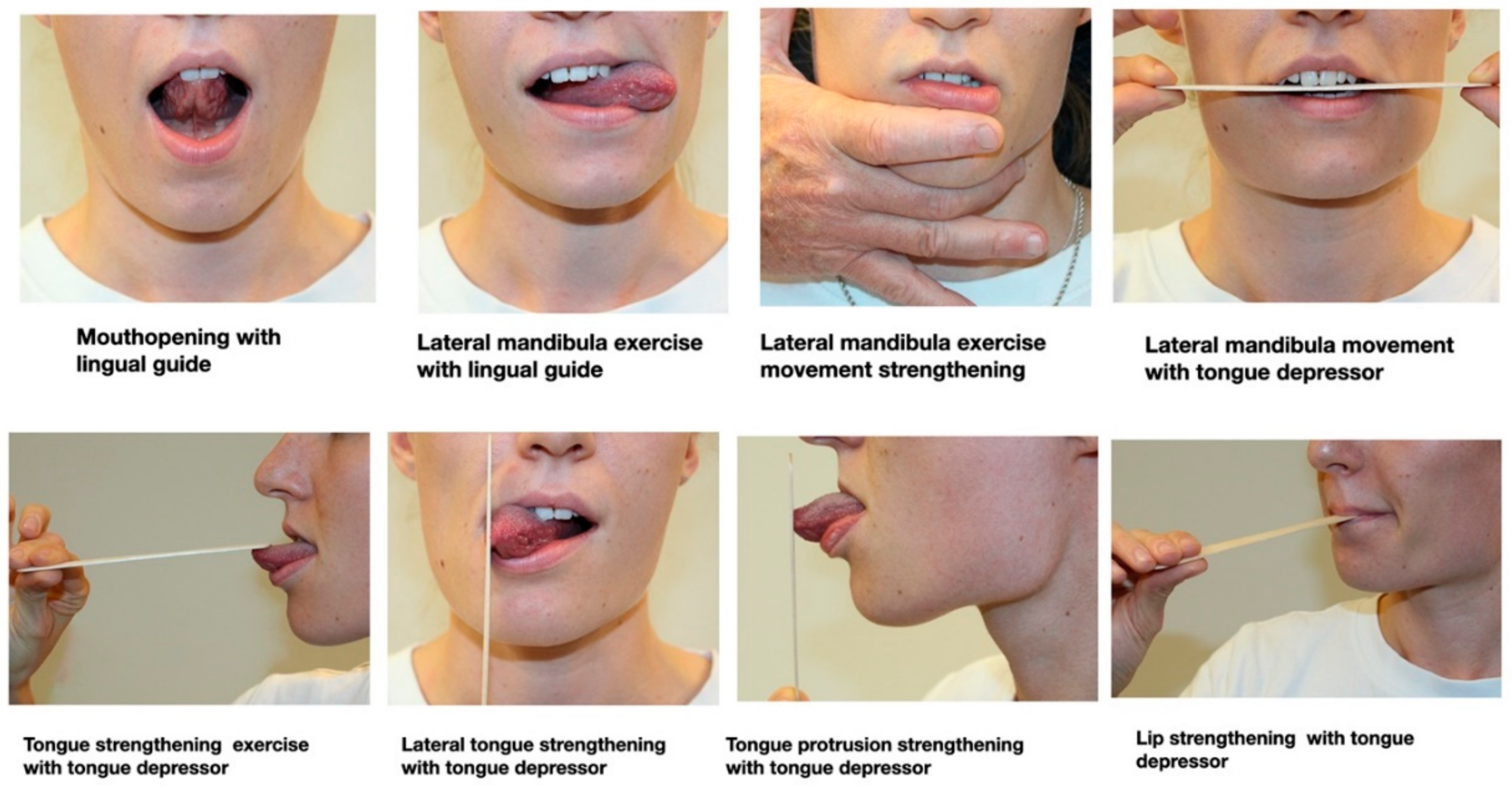
- Mouth opening exercise with lingual guide. Mouth opening movement with the tongue towards the palate. One set/eight repetitions.
- Lateral jaw movement. Lateral jaw movement with a tongue depressor between the incisors to guide the movement. One set/eight repetitions each side.
- Lateral tongue strengthening. Extrabuccal tongue lateral isometric force towards a tongue depressor placed (held vertically). One set/10 repetitions holding 10 s each. Ten-second rest in between.
- Lateral jaw mobilization exercise with lingual guide. Jaw lateral movement with a lateral protrusion of the tongue to guide the movement to the same side. One set/eight repetitions
- Tongue strengthening exercise. With an anterior protrusion of the tongue a depressor placed on the tongue, an isometric force upwards and against the depressor. One set/10 repetitions holding 10 s each. Ten-second rest in between.
- Lateral jaw movement strengthening. Jaw lateral movement with a slight external resistance to permit resisted movement. One set/eight repetitions each side.
- Tongue protrusion strengthening. Isometric force with a tongue protrusion towards a tongue depressor (held vertically). One set/10 repetitions holding 10 s each. Ten-second rest in between.
- Lip strength exercise. Isometric exercise holding the lips in a closed and thigh position with a tongue depressor between them. One set/10 repetitions holding 10 s each. Ten-second rest in between.
9.5. Masticatory Training
9.6. Therapeutic Patient Education
10. Reflection and Conclusions
- In this narrative review, an overview was given of the actual (scarce) external evidence on orofacial somatorepresentation distortion supporting clinical assessment and management.
- The authors have tried to integrate the scarce evidence found regarding the mentioned condition with the theoretical bases of the neuroscience behind the process, together with their clinical experience, in a treatment proposal of therapeutic interventions that might help improve pain, face perceptions and function and therefore quality of life.
- This overview article may challenge clinical research regenerating innovative research questions and its implementation.
- Suggestions which may be implemented in clinical research for Orofacial Somatorepresentation Distortion (OFSD) are as follows:
- ○
- Qualities of OFSD related with DC/TMD classification (Axis I and II) and IASP for example primary and secondary chronic pain, peripheral sensitized and central sensitization dominance conditions.
- ○
- Clinical subclassifications of OFSD.
- ○
- OFSD qualities during unilateral versus bilateral facial symptoms.
- ○
- The mutual degree of change of the acuity (visual, proprioceptive, acoustic and tactile) during the proposed rehabilitation strategy within different syndromes and diagnoses.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- LeResche, L. Epidemiology of Temporomandibular Disorders: Implications for the Investigation of Etiologic Factors. Critical reviews in oral biology and medicine: An official publication of the American Association of Oral Biologists. Crit. Rev. Oral Biol. Med. 1997, 8, 291–305. [Google Scholar] [CrossRef] [PubMed]
- Lipton, J.; Ship, J.; Larach-Robinson, D. Estimated Prevalence and Distribution of Reported Orofacial Pain in the United States. J. Am. Dent. Assoc. 1993, 124, 115–121. [Google Scholar] [CrossRef]
- Breivik, H.; Collett, B.; Ventafridda, V.; Cohen, R.; Gallacher, D. Survey of chronic pain in Europe: Prevalence, impact on daily life, and treatment. Eur. J. Pain 2006, 10, 287. [Google Scholar] [CrossRef]
- Von Korff, M.; Dworkin, S.F.; Le Resche, L.; Kruger, A. An epidemiologic comparison of pain complaints. Pain 1988, 32, 173–183. [Google Scholar] [CrossRef]
- Haggman-Henrikson, B.; Liv, P.; Ilgunas, A.; Visscher, C.M.; Lobbezoo, F.; Durham, J.; Lövgren, A. Increasing gender differences in the prevalence and chronification of orofacial pain in the population. Pain 2020, 161, 1768–1775. [Google Scholar] [CrossRef]
- Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [CrossRef]
- International Classification of Orofacial Pain, 1st edition (ICOP). Cephalalgia 2020, 40, 129–221. [CrossRef] [Green Version]
- Ziegeler, C.; May, A. The ICHD definition of ‘facial pain’ should be revised. Cephalalgia 2020, 40, 1398–1399. [Google Scholar] [CrossRef]
- Ananthan, S.; Benoliel, R. Chronic orofacial pain. J. Neural Transm. 2020, 127, 575–588. [Google Scholar] [CrossRef] [PubMed]
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.-P.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F.; et al. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: Recommendations of the International RDC/TMD Consortium Network * and Orofacial Pain Special Interest Group †. J. Oral Facial Pain Headache 2014, 28, 6–27. [Google Scholar] [CrossRef] [PubMed]
- Dando, W.E.; Branch, M.A.; Maye, J.P. Headache Disability in Orofacial Pain Patients. Headache J. Head Face Pain 2006, 46, 322–326. [Google Scholar] [CrossRef]
- Storm, C.; Wänman, A. Temporomandibular disorders, headaches, and cervical pain among females in a Sami population. Acta Odontol. Scand. 2006, 64, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Tal, M.; Villanueva, L.; Devor, M. Anatomy and neurophysiology of orofacial pain. In Orofacial Pain & Headache; Sharav, Y., Benoliel, R., Eds.; Quintessence Publishing: Chicago, IL, USA, 2015; pp. 31–77. [Google Scholar]
- Shinoda, M.; Kubo, A.; Hayashi, Y.; Iwata, K. Peripheral and Central Mechanisms of Persistent Orofacial Pain. Front. Neurosci. 2019, 13, 1227. [Google Scholar] [CrossRef]
- Craddock, C.; Jbabdi, S.; Yan, C.-G.; Vogelstein, J.; Castellanos, F.; Di Martino, A.; Kelly, C.; Heberlein, K.; Colcombe, S.; Milham, M.P. Imaging human connectomes at the macroscale. Nat. Methods 2013, 10, 524–539. [Google Scholar] [CrossRef] [Green Version]
- Shueb, S.; Nixdorf, D.; John, M.; Alonso, B.F.; Durham, J. What is the impact of acute and chronic orofacial pain on quality of life? J. Dent. 2015, 43, 1203–1210. [Google Scholar] [CrossRef]
- Slade, G.; Ohrbach, R.; Greenspan, J.; Fillingim, R.; Bair, E.; Sanders, A.; Dubner, R.; Diatchenko, L.; Meloto, C.; Smith, S.; et al. Painful Temporomandibular Disorder. J. Dent. Res. 2016, 95, 1084–1092. [Google Scholar] [CrossRef] [Green Version]
- Lei, J.; Liu, M.-Q.; Yap, A.U.J.; Fu, K.-Y. Sleep Disturbance and Psychologic Distress: Prevalence and Risk Indicators for Temporomandibular Disorders in a Chinese Population. J. Oral Facial Pain Headache 2015, 29, 24–30. [Google Scholar] [CrossRef]
- Ziegeler, C.; Schulte, L.H.; May, A. Altered trigeminal pain processing on brainstem level in persistent idiopathic facial pain. Pain 2021, 162, 1374–1378. [Google Scholar] [CrossRef]
- Harper, D.; Schrepf, A.; Clauw, D. Pain Mechanisms and Centralized Pain in Temporomandibular Disorders. J. Dent. Res. 2016, 95, 1102–1108. [Google Scholar] [CrossRef] [Green Version]
- Lin, C.-S. Brain Signature of Chronic Orofacial Pain: A Systematic Review and Meta-Analysis on Neuroimaging Research of Trigeminal Neuropathic Pain and Temporomandibular Joint Disorders. PLoS ONE 2014, 9, e94300. [Google Scholar] [CrossRef]
- La Touche, R.; Paris-Alemany, A.; Hidalgo-Pérez, A.; López-De-Uralde-Villanueva, I.; Angulo-Diaz-Parreño, S.; Muñoz-García, D. Evidence for Central Sensitization in Patients with Temporomandibular Disorders: A Systematic Review and Meta-analysis of Observational Studies. Pain Pract. 2018, 18, 388–409. [Google Scholar] [CrossRef] [PubMed]
- Garrigós-Pedrón, M.; La Touche, R.; Desentre, P.N.; Gracia-Naya, M.; Segura-Ortí, E. Widespread mechanical pain hypersensitivity in patients with chronic migraine and temporomandibular disorders: Relationship and correlation between psychological and sensorimotor variables. Acta Odontol. Scand. 2019, 77, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Nasri-Heir, C.; Khan, J.; Benoliel, R.; Feng, C.; Yarnitsky, D.; Kuo, F.; Hirschberg, C.; Hartwell, G.; Huang, C.-Y.; Heir, G.; et al. Altered pain modulation in patients with persistent postendodontic pain. Pain 2015, 156, 2032–2041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gil-Martinez, A.; Paris-Alemany, A.; López-De-Uralde-Villanueva, I.; La Touche, R. Management of pain in patients with temporomandibular disorder (TMD): Challenges and solutions. J. Pain Res. 2018, 11, 571–587. [Google Scholar] [CrossRef] [Green Version]
- Ettlin, D.A.; Napimoga, M.H.; e Cruz, M.M.; Clemente-Napimoga, J.T. Orofacial musculoskeletal pain: An evidence-based bio-psycho-social matrix model. Neurosci. Biobehav. Rev. 2021, 128, 12–20. [Google Scholar] [CrossRef]
- Valmunen, T.; Pertovaara, A.; Taiminen, T.; Virtanen, A.; Parkkola, R.; Jääskeläinen, S.K. Modulation of facial sensitivity by navigated rTMS in healthy subjects. Pain 2009, 142, 149–158. [Google Scholar] [CrossRef]
- Sterling, M.; Jull, G.; Wright, A. The effect of musculoskeletal pain on motor activity and control. J. Pain 2001, 2, 135–145. [Google Scholar] [CrossRef] [PubMed]
- Vallence, A.-M.; Smith, A.; Tabor, A.; Rolan, P.E.; Ridding, M.C. Chronic tension-type headache is associated with impaired motor learning. Cephalalgia 2013, 33, 1048–1054. [Google Scholar] [CrossRef] [Green Version]
- Weissman-Fogel, I.; Moayedi, M.; Tenenbaum, H.C.; Goldberg, M.B.; Freeman, B.V.; Davis, K.D. Abnormal cortical activity in patients with temporomandibular disorder evoked by cognitive and emotional tasks. Pain 2011, 152, 384–396. [Google Scholar] [CrossRef]
- Salomons, T.V.; Moayedi, M.; Weissman-Fogel, I.; Goldberg, M.B.; Freeman, B.V.; Tenenbaum, H.C.; Davis, K.D. Perceived helplessness is associated with individual differences in the central motor output system. Eur. J. Neurosci. 2012, 35, 1481–1487. [Google Scholar] [CrossRef]
- Tucker, K.; Larsson, A.-K.; Oknelid, S.; Hodges, P. Similar alteration of motor unit recruitment strategies during the anticipation and experience of pain. Pain 2012, 153, 636–643. [Google Scholar] [CrossRef] [Green Version]
- Moseley, G.L.; Flor, H. Targeting Cortical Representations in the Treatment of Chronic Pain. Neurorehabilit. Neural Repair 2012, 26, 646–652. [Google Scholar] [CrossRef] [PubMed]
- La Touche, R.; Cuenca-Martínez, F.; Suso-Martí, L.; García-Vicente, A.; Navarro-Morales, B.; Paris-Alemany, A. Tactile trigeminal region acuity in temporomandibular disorders: A reliability and cross-sectional study. J. Oral Rehabil. 2019, 47, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Michelotti, A.; Farella, M.; Stellato, A.; Martina, R.; De Laat, A. Tactile and pain thresholds in patients with myofascial pain of the jaw muscles: A case-control study. J. Orofac. Pain 2008, 22, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Uritani, D.; Nishida, T.; Sakaguchi, N.; Kawakami, T.; Jones, L.; Kirita, T. Difference in Response to a Motor Imagery Task: A Comparison between Individuals with and without Painful Temporomandibular Disorders. Pain Res. Manag. 2018, 2018, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Dagsdóttir, L.K.; Skyt, I.; Vase, L.; Baad-Hansen, L.; Castrillon, E.; Svensson, P. Reports of perceptual distortion of the face are common in patients with different types of chronic oro-facial pain. J. Oral Rehabil. 2016, 43, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Von Piekartz, H.; Wallwork, S.B.; Mohr, G.; Butler, D.S.; Moseley, L. People with chronic facial pain perform worse than controls at a facial emotion recognition task, but it is not all about the emotion. J. Oral Rehabil. 2014, 42, 243–250. [Google Scholar] [CrossRef]
- Chaves, A.C.S.; Reis, F.J.J.; Bandeira, P.M.; Fernandes, O.; Sanchez, T.A. Autonomic dysregulation and impairments in the recognition of facial emotional expressions in patients with chronic musculoskeletal pain. Scand. J. Pain 2021. [Google Scholar] [CrossRef]
- Harvie, D.; Edmond-Hank, G.; Smith, A.D. Tactile acuity is reduced in people with chronic neck pain. Musculoskelet. Sci. Pract. 2018, 33, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Bustan, S.; González-Roldán, A.M.; Schommer, C.; Kamping, S.; Löffler, M.; Brunner, M.; Flor, H.; Anton, F. Psychological, cognitive factors and contextual influences in pain and pain-related suffering as revealed by a combined qualitative and quantitative assessment approach. PLoS ONE 2018, 13, e0199814. [Google Scholar] [CrossRef]
- Juottonen, K.; Gockel, M.; Silén, T.; Hurri, H.; Hari, R.; Forss, N. Altered central sensorimotor processing in patients with complex regional pain syndrome. Pain 2002, 98, 315–323. [Google Scholar] [CrossRef]
- Younger, J.W.; Shen, Y.F.; Goddard, G.; Mackey, S. Chronic myofascial temporomandibular pain is associated with neural abnormalities in the trigeminal and limbic systems. Pain 2010, 149, 222–228. [Google Scholar] [CrossRef] [Green Version]
- Stamper, G.C.; Johnson, T.A. Auditory Function in Normal-Hearing, Noise-Exposed Human Ears. Ear Hear. 2015, 36, 172–184. [Google Scholar] [CrossRef] [Green Version]
- Muhr, P.; Rosenhall, U. Self-assessed auditory symptoms, noise exposure, and measured auditory function among healthy young Swedish men. Int. J. Audiol. 2010, 49, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Suhnan, A.P.; Finch, P.M.; Drummond, P.D. Hyperacusis in chronic pain: Neural interactions between the auditory and nociceptive systems. Int. J. Audiol. 2017, 56, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Moseley, L.; Jones, M. Chronic Facial Pain in a 24-Year-Old University Student. In Clinical Reasoning in Musculoskeletal Practice; Elsevier BV: Edinburgh, Scotland, 2019; pp. 150–163. [Google Scholar]
- Luedtke, K.; Edlhaimb, J. Laterality judgements in patients with frequent episodic migraine. Musculoskelet. Sci. Pract. 2021, 51, 102316. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Saez, M.; Gil-Martínez, A.; González, I.I.; Lee, J.K.; De-Vera, J.D.-C.P.; Carretero, J.C.; Beltran-Alacreu, H. A novel mobile application to determine mandibular and tongue laterality discrimination in women with chronic temporomandibular disorder. Med. Oral Patol. Oral Cir. Bucal 2020, 25, e775–e783. [Google Scholar] [CrossRef]
- Von Piekartz, H.; Mohr, G. Reduction of head and face pain by challenging lateralization and basic emotions: A proposal for future assessment and rehabilitation strategies. J. Man. Manip. Ther. 2014, 22, 24–35. [Google Scholar] [CrossRef] [Green Version]
- Jeannerod, M. Mental imagery in the motor context. Neuropsychologia 1995, 33, 1419–1432. [Google Scholar] [CrossRef]
- Dickstein, R.; Deutsch, J.E. Motor Imagery in Physical Therapist Practice. Phys. Ther. 2007, 87, 942–953. [Google Scholar] [CrossRef] [Green Version]
- Lotze, M.; Halsband, U. Motor imagery. J. Physiol. 2006, 99, 386–395. [Google Scholar] [CrossRef]
- Vannuscorps, G.; Pillon, A.; Andres, M. Effect of biomechanical constraints in the hand laterality judgment task: Where does it come from? Front. Hum. Neurosci. 2012, 6, 299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellan, V.; Wallwork, S.B.; Gallace, A.; Spence, C.; Moseley, G.L. Integrating Self-Localization, Proprioception, Pain, and Performance. J. Danc. Med. Sci. 2017, 21, 24–35. [Google Scholar] [CrossRef] [Green Version]
- Osuagwu, B.A.; Vuckovic, A. Similarities between explicit and implicit motor imagery in mental rotation of hands: An EEG study. Neuropsychologia 2014, 65, 197–210. [Google Scholar] [CrossRef] [Green Version]
- Hanakawa, T.; Immisch, I.; Toma, K.; Dimyan, M.; Van Gelderen, P.; Hallett, M. Functional Properties of Brain Areas Associated with Motor Execution and Imagery. J. Neurophysiol. 2003, 89, 989–1002. [Google Scholar] [CrossRef] [Green Version]
- Avivi-Arber, L.; Martin, R.; Lee, J.-C.; Sessle, B.J. Face sensorimotor cortex and its neuroplasticity related to orofacial sensorimotor functions. Arch. Oral Biol. 2011, 56, 1440–1465. [Google Scholar] [CrossRef]
- Sessle, B.J.; Yao, D.; Nishiura, H.; Yoshino, K.; Lee, J.-C.; Martin, R.E.; Murray, G.M. Properties and plasticity of the primate somatosensory and motor cortex related to orofacial sensorimotor function. Clin. Exp. Pharmacol. Physiol. 2005, 32, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Moreau, D. Unreflective actions? complex motor skill acquisition to enhance spatial cognition. Phenomenol. Cogn. Sci. 2015, 14, 349–359. [Google Scholar] [CrossRef]
- Moseley, G.L.; Gallace, A.; Spence, C. Bodily illusions in health and disease: Physiological and clinical perspectives and the concept of a cortical ‘body matrix’. Neurosci. Biobehav. Rev. 2012, 36, 34–46. [Google Scholar] [CrossRef]
- Sato, S.; Ohta, M.; Sawatari, M.; Kawamura, H.; Motegi, K. Occlusal contact area, occlusal pressure, bite force, and masticatory efficiency in patients with anterior disc displacement of the temporomandibular joint. J. Oral Rehabil. 1999, 26, 906–911. [Google Scholar] [CrossRef] [PubMed]
- Sato, S.; Nasu, F.; Motegi, K. Natural course of nonreducing disc displacement of the temporomandibular joint: Changes in chewing movement and masticatory efficiency. J. Oral Maxillofac. Surg. 2002, 60, 867–872. [Google Scholar] [CrossRef] [PubMed]
- Weber, P.; Corrêa, E.C.R.; Bolzan, G.D.P.; Ferreira, F.D.S.; Soares, J.C.; Da Silva, A.M.T. Mastigação e deglutição em mulheres jovens com desordem temporomandibular. CoDAS 2013, 25, 375–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coelho-Ferraz, M.J.P.; Berzin, F.; Amorim, C.F.; Romano, F.L.; Queluz, D.D.P. Electromyographic and cephalometric correlation with the predominant masticatory movement. Stomatologija 2010, 12, 51–55. [Google Scholar] [PubMed]
- Santana-Mora, U.; López-Cedrún, J.; Mora, M.J.; Otero, X.L.; Santana-Penin, U. Temporomandibular Disorders: The Habitual Chewing Side Syndrome. PLoS ONE 2013, 8, e59980. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Padmaja, B.; Neeharika, S.; Bindu, G.H.; Babu, N.S.; Madhulika, S. Predilection of Chewing Side Preferences and Clinical Assessment of Its Impact on Temporomandibular Joint. J. Dent. Allied Sci. 2018, 7, 65. [Google Scholar] [CrossRef]
- Wiesinger, B.; Haggman-Henrikson, B.; Hellström, F.; Wänman, A. Experimental masseter muscle pain alters jaw-neck motor strategy. Eur. J. Pain 2012, 17, 995–1004. [Google Scholar] [CrossRef]
- Giurgola, S.; Pisoni, A.; Maravita, A.; Vallar, G.; Bolognini, N. Somatosensory cortical representation of the body size. Hum. Brain Mapp. 2019, 40, 3534–3547. [Google Scholar] [CrossRef] [Green Version]
- Mora, L.; Cowie, D.; Banissy, M.J.; Cocchini, G. My true face: Unmasking one’s own face representation. Acta Psychol. 2018, 191, 63–68. [Google Scholar] [CrossRef] [Green Version]
- Skyt, I.; Dagsdóttir, L.; Vase, L.; Baad-Hansen, L.; Castrillon, E.; Roepstorff, A.; Jensen, T.S.; Svensson, P. Painful Stimulation and Transient Blocking of Nerve Transduction Due to Local Anesthesia Evoke Perceptual Distortions of the Face in Healthy Volunteers. J. Pain 2015, 16, 335–345. [Google Scholar] [CrossRef] [Green Version]
- Costa, Y.; Castrillon, E.; Bonjardim, L.; Conti, P.R.; Baad-Hansen, L.; Svensson, P. Effects of Experimental Pain and Lidocaine on Mechanical Somatosensory Profile and Face Perception. J. Oral Facial Pain Headache 2017, 31, 115–123. [Google Scholar] [CrossRef] [Green Version]
- Moseley, L.G. I can’t find it! Distorted body image and tactile dysfunction in patients with chronic back pain. Pain 2008, 140, 239–243. [Google Scholar] [CrossRef]
- Lewis, J.S.; Kersten, P.; McCabe, C.; McPherson, K.; Blake, D.R. Body perception disturbance: A contribution to pain in complex regional pain syndrome (CRPS). Pain 2007, 133, 111–119. [Google Scholar] [CrossRef]
- Flor, H.; Braun, C.; Elbert, T.; Birbaumer, N. Extensive reorganization of primary somatosensory cortex in chronic back pain patients. Neurosci. Lett. 1997, 224, 5–8. [Google Scholar] [CrossRef] [Green Version]
- Ekman, P. Emotions revealed. BMJ 2004, 328, 0405184. [Google Scholar] [CrossRef]
- Haas, J.; Eichhammer, P.; Traue, H.C.; Hoffmann, H.; Behr, M.; Crönlein, T.; Pieh, C.; Busch, V. Alexithymic and somatisation scores in patients with temporomandibular pain disorder correlate with deficits in facial emotion recognition. J. Oral Rehabil. 2013, 40, 81–90. [Google Scholar] [CrossRef]
- Von Piekartz, H.; Mohr, G.; Traue, H.C. Recognition of Emotional Facial Expressions and Alexithymia in Patients with Chronic Facial Pain. Ann. Psychiatry Ment. Health 2018, 6, 1134. [Google Scholar]
- Keysers, C.; Gazzola, V. Expanding the mirror: Vicarious activity for actions, emotions, and sensations. Curr. Opin. Neurobiol. 2009, 19, 666–671. [Google Scholar] [CrossRef] [PubMed]
- Van Heukelum, S.; Mars, R.; Guthrie, M.; Buitelaar, J.K.; Beckmann, C.F.; Tiesinga, P.H.; Vogt, B.A.; Glennon, J.; Havenith, M.N. Where is Cingulate Cortex? A Cross-Species View. Trends Neurosci. 2020, 43, 285–299. [Google Scholar] [CrossRef]
- Paradiso, E.; Gazzola, V.; Keysers, C. Neural mechanisms necessary for empathy-related phenomena across species. Curr. Opin. Neurobiol. 2021, 68, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Meffert, H.; Gazzola, V.; Boer, J.A.D.; Bartels, A.A.J.; Keysers, C. Reduced spontaneous but relatively normal deliberate vicarious representations in psychopathy. Brain 2013, 136, 2550–2562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, T.; Kucharska, K.; Wilkos, E.; Sławinska, K. Social cognitive and neurocognitive deficits in inpatients with unilateral thalamic lesions—Pilot study. Neuropsychiatr. Dis. Treat. 2015, 11, 1031–1038. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shamay-Tsoory, S.G.; Aharon-Peretz, J.; Perry, D. Two systems for empathy: A double dissociation between emotional and cognitive empathy in inferior frontal gyrus versus ventromedial prefrontal lesions. Brain 2009, 132, 617–627. [Google Scholar] [CrossRef] [Green Version]
- Perry, A.; Saunders, S.N.; Stiso, J.; Dewar, C.; Lubell, J.; Meling, T.R.; Solbakk, A.-K.; Endestad, T.; Knight, R.T. Effects of prefrontal cortex damage on emotion understanding: EEG and behavioural evidence. Brain 2017, 140, 1086–1099. [Google Scholar] [CrossRef]
- Vaidya, A.R.; Fellows, L.K. Ventromedial frontal lobe damage affects interpretation, not exploration, of emotional facial expressions. Cortex 2019, 113, 312–328. [Google Scholar] [CrossRef]
- Willis, M.L.; Palermo, R.; McGrillen, K.; Miller, L. The nature of facial expression recognition deficits following orbitofrontal cortex damage. Neuropsychologia 2014, 28, 613–623. [Google Scholar] [CrossRef] [PubMed]
- Godin, B.R.; Oishi, K.; Oishi, K.; Davis, C.; Gomez, Y.; Trupe, L.A.; Kim, E.H.; Hillis, A.E.; Tippett, D.C. Impaired Recognition of Emotional Faces after Stroke Involving Right Amygdala or Insula. Semin. Speech Lang. 2018, 39, 87–100. [Google Scholar] [CrossRef]
- Motomura, K.; Terasawa, Y.; Natsume, A.; Iijima, K.; Chalise, L.; Sugiura, J.; Yamamoto, H.; Koyama, K.; Wakabayashi, T.; Umeda, S. Anterior insular cortex stimulation and its effects on emotion recognition. Brain Struct. Funct. 2019, 224, 2167–2181. [Google Scholar] [CrossRef]
- Boucher, O.; Rouleau, I.; Lassonde, M.; Lepore, F.; Bouthillier, A.; Nguyen, D.K. Social information processing following resection of the insular cortex. Neuropsychologia 2015, 71, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Adolphs, R. Neural systems for recognizing emotion. Curr. Opin. Neurobiol. 2002, 12, 169–177. [Google Scholar] [CrossRef]
- Neal, D.T.; Chartrand, T.L. Embodied Emotion Perception. Soc. Psychol. Pers. Sci. 2011, 2, 673–678. [Google Scholar] [CrossRef]
- Sato, W.; Fujimura, T.; Kochiyama, T.; Suzuki, N. Relationships among Facial Mimicry, Emotional Experience, and Emotion Recognition. PLoS ONE 2013, 8, e57889. [Google Scholar] [CrossRef]
- Price, T.F.; Harmon-Jones, E. Embodied emotion: The influence of manipulated facial and bodily states on emotive responses. Wiley Interdiscip. Rev. Cogn. Sci. 2015, 6, 461–473. [Google Scholar] [CrossRef]
- Kircher, T.; Pohl, A.; Krach, S.; Thimm, M.; Schulte-Rüther, M.; Anders, S.; Mathiak, K. Affect-specific activation of shared networks for perception and execution of facial expressions. Soc. Cogn. Affect. Neurosci. 2013, 8, 370–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kajal, D.S.; Fioravanti, C.; Elshahabi, A.; Ruiz, S.; Sitaram, R.; Braun, C. Involvement of top-down networks in the perception of facial emotions: A magnetoencephalographic investigation. NeuroImage 2020, 222, 117075. [Google Scholar] [CrossRef] [PubMed]
- Zhen, Z.; Fang, H.; Liu, J. The Hierarchical Brain Network for Face Recognition. PLoS ONE 2013, 8, e59886. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kraaijenvanger, E.J.; Hofman, D.; Bos, P.A. A neuroendocrine account of facial mimicry and its dynamic modulation. Neurosci. Biobehav. Rev. 2017, 77, 98–106. [Google Scholar] [CrossRef]
- Szily, E.; Kéri, S. Emotion-Related Brain Regions. Ideggyogy. Sz. 2008, 61, 77–86. [Google Scholar]
- Longo, M.R.; Azanon, E.; Haggard, P. More than skin deep: Body representation beyond primary somatosensory cortex. Neuropsychologia 2010, 48, 655–668. [Google Scholar] [CrossRef] [Green Version]
- Kindler, S.; Schwahn, C.; Terock, J.; Mksoud, M.; Bernhardt, O.; Biffar, R.; Völzke, H.; Metelmann, H.R.; Grabe, H.J. Alexithymia and temporomandibular joint and facial pain in the general population. J. Oral Rehabil. 2018, 46, 310–320. [Google Scholar] [CrossRef]
- Pinna, F.; Manchia, M.; Paribello, P.; Carpiniello, B. The Impact of Alexithymia on Treatment Response in Psychiatric Disorders: A Systematic Review. Front. Psychiatry 2020, 11, 311. [Google Scholar] [CrossRef] [Green Version]
- Grabe, H.J.; Frommer, J.; Ankerhold, A.; Ulrich, C.; Gröger, R.; Franke, G.H.; Barnow, S.; Freyberger, H.J.; Spitzer, C. Alexithymia and Outcome in Psychotherapy. Psychother. Psychosom. 2008, 77, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Di Tella, M.; Castelli, L. Alexithymia in Chronic Pain Disorders. Curr. Rheumatol. Rep. 2016, 18, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Gündel, H.; Ceballos-Baumann, A.; Von Rad, M. Aktuelle Perspektiven der Alexithymie. Nervenarzt 2000, 71, 151–163. [Google Scholar] [CrossRef] [PubMed]
- Derryberry, D.; Tucker, D.M. Neural mechanisms of emotion. J. Consult. Clin. Psychol. 1992, 60, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Gil, F.P.; Ridout, N.; Kessler, H.; Neuffer, M.; Schoechlin, C.; Traue, H.C.; Nickel, M. Facial emotion recognition and alexithymia in adults with somatoform disorders. Depress. Anxiety 2009, 26, E26–E33. [Google Scholar] [CrossRef] [Green Version]
- Buhlmann, U.; Winter, A.; Kathmann, N. Emotion recognition in body dysmorphic disorder: Application of the Reading the Mind in the Eyes Task. Body Image 2013, 10, 247–250. [Google Scholar] [CrossRef]
- Yetkin-Ozden, S.; Ekizoglu, E.; Baykan, B. Face Recognition in Patients with Migraine. Pain Pract. 2015, 15, 319–322. [Google Scholar] [CrossRef] [PubMed]
- Flor, H. New developments in the understanding and management of persistent pain. Curr. Opin. Psychiatry 2012, 25, 109–113. [Google Scholar] [CrossRef]
- Simons, L.E.; Elman, I.; Borsook, D. Psychological processing in chronic pain: A neural systems approach. Neurosci. Biobehav. Rev. 2014, 39, 61–78. [Google Scholar] [CrossRef] [Green Version]
- Wolf, E.; Birgerstam, P.; Nilner, M.; Petersson, K. Nonspecific chronic orofacial pain: Studying patient experiences and perspectives with a qualitative approach. J. Orofac. Pain 2008, 22, 349–358. [Google Scholar]
- Hazaveh, M.; Hovey, R. Patient Experience of Living with Orofacial Pain: An Interpretive Phenomenological Study. JDR Clin. Transl. Res. 2018, 3, 264–271. [Google Scholar] [CrossRef] [PubMed]
- Bäck, K.; Hakeberg, M.; Wide, U.; Hange, D.; Dahlström, L. Orofacial pain and its relationship with oral health-related quality of life and psychological distress in middle-aged women. Acta Odontol. Scand. 2019, 78, 74–80. [Google Scholar] [CrossRef] [PubMed]
- La Touche, R.; Pardo-Montero, J.; Gil-Martínez, A.; Paris-Alemany, A.; Angulo-Díaz-Parreño, S.; Suárez-Falcón, J.C.; Lara-Lara, M.; Fernandez-Carnero, J. Craniofacial pain and disability inventory (CF-PDI): Development and psychometric validation of a new questionnaire. Pain Physician 2014, 17, 95–108. [Google Scholar] [CrossRef]
- Monticone, M.; Rocca, B.; Abelli, P.; Tecco, S.; Geri, T.; Gherlone, E.; Luzzi, D.; Testa, M. Cross-cultural adaptation, reliability and validity of the Italian version of the craniofacial pain and disability inventory in patients with chronic temporomandibular joint disorders. BMC Oral Health 2019, 19, 244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greghi, S.M.; Aguiar, A.D.S.; Bataglion, C.; Ferracini, G.N.; La Touche, R.; Chaves, T. Brazilian Portuguese Version of the Craniofacial Pain and Disability Inventory: Cross-Cultural Reliability, Internal Consistency, and Construct and Structural Validity. J. Oral Facial Pain Headache 2018, 32, 389–399. [Google Scholar] [CrossRef] [PubMed]
- Li, X.-L.; He, S.-L.; Wang, J.-H. Validation of a web-based version of the Craniofacial Pain and Disability Inventory. J. Oral Rehabil. 2020, 47, 802–808. [Google Scholar] [CrossRef] [PubMed]
- Von Piekartz, H.; La Touche, R.; Paris-Alemany, A.; Löwen, A.; Ismail, M.; Köhl, R.; Benz, K.; Ballenberger, N. Cross-Cultural Adaption and Psychometric Evaluation of the German Craniofacial Pain and Disability Inventory (CF-PDI). Pain Physician 2020, in press. [Google Scholar]
- Brähler, E.; Brosig, B.; Kupfer, J. Überprüfung und Validierung der 26-Item Toronto Alexithymie-Skala anhand einer repräsentativen Bevölkerungsstichprobe/Testing and validation of the 26-item Toronto Alexithymia Scale in a representative population sample. Z. Psychosom. Med. Psychother. 2000, 46, 368–384. [Google Scholar] [CrossRef] [PubMed]
- La Touche, R.; Pardo-Montero, J.; Cuenca-Martínez, F.; Visscher, C.M.; Paris-Alemany, A.; López-De-Uralde-Villanueva, I. Cross-Cultural Adaptation and Psychometric Properties of the Spanish Version of the Tampa Scale for Kinesiophobia for Temporomandibular Disorders. J. Clin. Med. 2020, 9, 2831. [Google Scholar] [CrossRef] [PubMed]
- He, S.; Wang, J.; Ji, P. Validation of the Tampa Scale for Kinesiophobia for Temporomandibular Disorders (TSK-TMD) in patients with painful TMD. J. Headache Pain 2016, 17, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aguiar, A.S.; Bataglion, C.; Visscher, C.M.; Grossi, D.; Chaves, T.C. Cross-cultural adaptation, reliability and construct validity of the Tampa scale for kinesiophobia for temporomandibular disorders (TSK/TMD-Br) into Brazilian Portuguese. J. Oral Rehabil. 2017, 44, 500–510. [Google Scholar] [CrossRef] [PubMed]
- Visscher, C.M.; Ohrbach, R.; Van Wijk, A.J.; Wilkosz, M.; Naeije, M. The Tampa Scale for Kinesiophobia for Temporomandibular Disorders (TSK-TMD). Pain 2010, 150, 492–500. [Google Scholar] [CrossRef]
- Cameron, O.G. Interoception: The Inside Story—A Model for Psychosomatic Processes. Psychosom. Med. 2001, 63, 697–710. [Google Scholar] [CrossRef]
- Craig, A.D. How do you feel? Interoception: The sense of the physiological condition of the body. Nat. Rev. Neurosci. 2002, 3, 655–666. [Google Scholar] [CrossRef] [PubMed]
- Fox, K.C.R.; Zakarauskas, P.; Dixon, M.; Ellamil, M.; Thompson, E.; Christoff, K. Meditation Experience Predicts Introspective Accuracy. PLoS ONE 2012, 7, e45370. [Google Scholar] [CrossRef]
- Goyal, M.; Singh, S.; Sibinga, E.M.S.; Gould, N.F.; Rowland-Seymour, A.; Sharma, R.; Berger, Z.; Sleicher, D.; Maron, D.D.; Shihab, H.M.; et al. Meditation Programs for Psychological Stress and Well-being. JAMA Intern. Med. 2014, 174, 357–368. [Google Scholar] [CrossRef] [Green Version]
- Barbero, M.; Moresi, F.; Leoni, D.; Gatti, R.; Egloff, M.; Falla, D. Test-retest reliability of pain extent and pain location using a novel method for pain drawing analysis. Eur. J. Pain 2015, 19, 1129–1138. [Google Scholar] [CrossRef] [PubMed]
- Grashoff, M.; Klos, V. Reference Values of Facial Lateralization and Basic Emotions and Its Clinical Implementation in Chronic Facial Pain from the CRAFTA Face Recognition Program; University of Applied Science: Osnabruck, Germany, 2014. [Google Scholar]
- Baron-Cohen, S.; Wheelwright, S.; Hill, J.; Raste, Y.; Plumb, I. The “Reading the Mind in the Eyes” Test revised version: A study with normal adults, and adults with Asperger syndrome or high-functioning autism. J. Child Psychol. Psychiatry 2001, 42, 241–251. [Google Scholar] [CrossRef]
- Oakley, B.F.M.; Brewer, R.; Bird, G.; Catmur, C. Theory of mind is not theory of emotion: A cautionary note on the Reading the Mind in the Eyes Test. J. Abnorm. Psychol. 2016, 125, 818–823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kessler, H.; Bayerl, P.; Deighton, R.M.; Traue, H.C. [Facially Expressed Emotion Labeling (FEEL): A Computer-Based Test for Emotion Recognition. Verhalt. Verhalt. 2002, 23, 297–306. [Google Scholar]
- Von Piekartz, H.; Stotz, E.; Both, A.; Bahn, G.; Armijo-Olivo, S.; Ballenberger, N. Psychometric evaluation of a motor control test battery of the craniofacial region. J. Oral Rehabil. 2017, 44, 964–973. [Google Scholar] [CrossRef]
- Mc Donnell, S.T.; Hector, M.P.; Hannigan, A. Chewing side preferences in children. J. Oral Rehabil. 2004, 31, 855–860. [Google Scholar] [CrossRef]
- La Touche, R.; Losana-Ferrer, A.; Pascual-Vaquerizo, E.; Suso-Martí, L.; Paris-Alemany, A.; Chamorro-Sánchez, J.; Cuenca-Martínez, F. Orofacial sensorimotor behaviour in unilateral chewing: A comparative analysis in asymptomatic population. Physiol. Behav. 2019, 212, 112718. [Google Scholar] [CrossRef] [PubMed]
- Adams, V.; Mathisen, B.; Baines, S.; Lazarus, C.; Callister, R. A Systematic Review and Meta-analysis of Measurements of Tongue and Hand Strength and Endurance Using the Iowa Oral Performance Instrument (IOPI). Dysphagia 2013, 28, 350–369. [Google Scholar] [CrossRef] [PubMed]
- Zanin, M.C.; Garcia, D.M.; Rocha, E.M.; De Felício, C.M. Orofacial Motor Functions and Temporomandibular Disorders in Patients with Sjögren’s Syndrome. Arthritis Rheum. 2019, 72, 1057–1065. [Google Scholar] [CrossRef] [PubMed]
- Masalski, M.; Grysiński, T.; Kręcicki, T. Hearing Tests Based on Biologically Calibrated Mobile Devices: Comparison with Pure-Tone Audiometry. JMIR Mhealth Uhealth 2018, 6, e10. [Google Scholar] [CrossRef]
- Kawakami, T.; Ishihara, M.; Mihara, M. Distribution Density of Intraepidermal Nerve Fibers in Normal Human Skin. J. Dermatol. 2001, 28, 63–70. [Google Scholar] [CrossRef]
- Nolano, M.; Provitera, V.; Caporaso, G.; Stancanelli, A.; Leandri, M.; Biasiotta, A.; Cruccu, G.; Santoro, L.; Truini, A. Cutaneous innervation of the human face as assessed by skin biopsy. J. Anat. 2013, 222, 161–169. [Google Scholar] [CrossRef]
- Khouri, L.; Nelken, I. Detecting the unexpected. Curr. Opin. Neurobiol. 2015, 35, 142–147. [Google Scholar] [CrossRef]
- Gilbert, S.J.; Burgess, P.W. Executive function. Curr. Biol. 2008, 18, R110–R114. [Google Scholar] [CrossRef] [Green Version]
- Glass, J.M.; Williams, D.A.; Fernandez-Sanchez, M.-L.; Kairys, A.; Barjola, P.; Heitzeg, M.; Clauw, D.J.; Schmidt-Wilcke, T. Executive Function in Chronic Pain Patients and Healthy Controls: Different Cortical Activation During Response Inhibition in Fibromyalgia. J. Pain 2011, 12, 1219–1229. [Google Scholar] [CrossRef] [Green Version]
- Kieliba, P.; Clode, D.; Maimon-Mor, R.O.; Makin, T.R. Robotic hand augmentation drives changes in neural body representation. Sci. Robot. 2021, 6, eabd7935. [Google Scholar] [CrossRef]
- Moseley, L.G.; Wiech, K. The effect of tactile discrimination training is enhanced when patients watch the reflected image of their unaffected limb during training. Pain 2009, 144, 314–319. [Google Scholar] [CrossRef]
- Coelho, L.A.; Gonzalez, C.L. The visual and haptic contributions to hand perception. Psychol. Res. 2017, 82, 866–875. [Google Scholar] [CrossRef]
- Dagsdóttir, L.K.; Bellan, V.; Skyt, I.; Vase, L.; Baad-Hansen, L.; Castrillon, E.; Svensson, P. Multisensory modulation of experimentally evoked perceptual distortion of the face. J. Oral Rehabil. 2017, 45, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Essick, G.; Phillips, C.; Zuniga, J. Effect of Facial Sensory Re-training on Sensory Thresholds. J. Dent. Res. 2007, 86, 571–575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moseley, L.G.; Zalucki, N.M.; Wiech, K. Tactile discrimination, but not tactile stimulation alone, reduces chronic limb pain. Pain 2008, 137, 600–608. [Google Scholar] [CrossRef]
- Phillips, C.; Blakey, G.; Essick, G.K. Sensory Retraining: A Cognitive Behavioral Therapy for Altered Sensation. Atlas Oral Maxillofac. Surg. Clin. 2011, 19, 109–118. [Google Scholar] [CrossRef] [Green Version]
- Galli, F.; Caputi, M.; Sances, G.; Vegni, E.; Bottiroli, S.; Nappi, G.; Tassorelli, C. Alexithymia in chronic and episodic migraine: A comparative study. J. Ment. Health 2016, 26, 192–196. [Google Scholar] [CrossRef] [PubMed]
- Glaros, A.G.; Lumley, M.A. Alexithymia and pain in temporomandibular disorder. J. Psychosom. Res. 2005, 59, 85–88. [Google Scholar] [CrossRef] [PubMed]
- Drimalla, H.; Landwehr, N.; Hess, U.; Dziobek, I. From face to face: The contribution of facial mimicry to cognitive and emotional empathy. Cogn. Emot. 2019, 33, 1672–1686. [Google Scholar] [CrossRef]
- Carr, L.; Iacoboni, M.; Dubeau, M.-C.; Mazziotta, J.C.; Lenzi, G.L. Neural mechanisms of empathy in humans: A relay from neural systems for imitation to limbic areas. Proc. Natl. Acad. Sci. USA 2003, 100, 5497–5502. [Google Scholar] [CrossRef] [Green Version]
- Jeannerod, M.; Decety, J. Mental motor imagery: A window into the representational stages of action. Curr. Opin. Neurobiol. 1995, 5, 727–732. [Google Scholar] [CrossRef]
- Schack, T.; Essig, K.; Frank, C.; Koester, D. Mental representation and motor imagery training. Front. Hum. Neurosci. 2014, 8, 328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buccino, G. Action observation treatment: A novel tool in neurorehabilitation. Philos. Trans. R. Soc. B Biol. Sci. 2014, 369, 20130185. [Google Scholar] [CrossRef] [PubMed]
- Decety, J. The neurophysiological basis of motor imagery. Behav. Brain Res. 1996, 77, 45–52. [Google Scholar] [CrossRef]
- Moseley, L.G. Graded motor imagery is effective for long-standing complex regional pain syndrome: A randomized controlled trial. Pain 2004, 108, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Moseley, G.L. Graded motor imagery for pathologic pain: A randomized controlled trial. Neurology 2006, 67, 2129–2134. [Google Scholar] [CrossRef]
- La Touche, R. Métodos de representación del movimiento en rehabilitación. Construyendo un marco conceptual para la aplicación en clínica. J. MOVE Ther. Sci. 2020, 2, 7. [Google Scholar] [CrossRef]
- Amesz, S.; Tessari, A.; Ottoboni, G.; Marsden, J. An observational study of implicit motor imagery using laterality recognition of the hand after stroke. Brain Inj. 2016, 30, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Hardwick, R.M.; Caspers, S.; Eickhoff, S.B.; Swinnen, S.P. Neural correlates of action: Comparing meta-analyses of imagery, observation, and execution. Neurosci. Biobehav. Rev. 2018, 94, 31–44. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Fritzsch, C.; Bernarding, J.; Holtze, S.; Mauritz, K.; Brunetti, M.; Dohle, C. A comparison of neural mechanisms in mirror therapy and movement observation therapy. J. Rehabil. Med. 2013, 45, 410–413. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Zhang, W.; Xing, B.; Li, J.; Yang, C.; Han, C.; Wang, Q. Mirror Therapy Versus Action Observation Therapy: Effects on Excitability of the Cerebral Cortex in Patients after Strokes. Int. J. Clin. Exp. Med. 2019, 12, 8763–8772. [Google Scholar]
- Suso-Martí, L.; La Touche, R.; Díaz-Parreño, S.A.; Cuenca-Martínez, F. Effectiveness of motor imagery and action observation training on musculoskeletal pain intensity: A systematic review and meta-analysis. Eur. J. Pain 2020, 24, 886–901. [Google Scholar] [CrossRef] [PubMed]
- Thieme, H.; Morkisch, N.; Rietz, C.; Dohle, C.; Borgetto, B. The Efficacy of Movement Representation Techniques for Treatment of Limb Pain—A Systematic Review and Meta-Analysis. J. Pain 2016, 17, 167–180. [Google Scholar] [CrossRef] [PubMed]
- Da Yap, B.W.; Lim, E.C.W. The Effects of Motor Imagery on Pain and Range of Motion in Musculoskeletal Disorders. Clin. J. Pain 2019, 35, 87–99. [Google Scholar] [CrossRef]
- Paravlic, A.H.; Slimani, M.; Tod, D.; Marusic, U.; Milanovic, Z.; Pisot, R. Effects and Dose–Response Relationships of Motor Imagery Practice on Strength Development in Healthy Adult Populations: A Systematic Review and Meta-analysis. Sports Med. 2018, 48, 1165–1187. [Google Scholar] [CrossRef] [PubMed]
- La Touche, R.; Grande-Alonso, M.; Cuenca-Martínez, F.; Gónzález-Ferrero, L.; Suso-Martí, L.; Paris-Alemany, A. Diminished Kinesthetic and Visual Motor Imagery Ability in Adults with Chronic Low Back Pain. PM&R 2019, 11, 227–235. [Google Scholar] [CrossRef]
- Monsma, E.V.; Short, S.E.; Hall, C.R.; Sullivan, P.; Gregg, M. Psychometric Properties of the Revised Movement Imagery Questionnaire (MIQ-R). J. Imag. Res. Sport Phys. Act. 2009, 4, 4. [Google Scholar] [CrossRef]
- Hidalgo-Peréz, A.; Fernández-García, Á.; López-De-Uralde-Villanueva, I.; Gil-Martínez, A.; Paris-Alemany, A.; Fernandez-Carnero, J.; La Touche, R. Effectiveness of A Motor Control Therapeutic Exercise Program Combined with Motor Imagery on the Sensorimotor Function of the Cervical Spine: A Randomized Controlled Trial. Int. J. Sports Phys. Ther. 2015, 10, 877–892. [Google Scholar] [PubMed]
- Daly, A.E.; Bialocerkowski, A.E. Does evidence support physiotherapy management of adult Complex Regional Pain Syndrome Type One? A systematic review. Eur. J. Pain 2009, 13, 339–353. [Google Scholar] [CrossRef] [PubMed]
- La Touche, R.; Herranz-Gómez, A.; Destenay, L.; Gey-Seedorf, I.; Cuenca-Martínez, F.; Paris-Alemany, A.; Suso-Martí, L. Effect of brain training through visual mirror feedback, action observation and motor imagery on orofacial sensorimotor variables: A single-blind randomized controlled trial. J. Oral Rehabil. 2020, 47, 620–635. [Google Scholar] [CrossRef] [PubMed]
- Krämer, H.H.; Seddigh, S.; Moseley, G.L.; Birklein, F.; Moseley, L. Dysynchiria is not a common feature of neuropathic pain. Eur. J. Pain 2008, 12, 128–131. [Google Scholar] [CrossRef]
- Breckenridge, J.D.; Ginn, K.A.; Wallwork, S.B.; McAuley, J.H. Do People with Chronic Musculoskeletal Pain Have Impaired Motor Imagery? A Meta-analytical Systematic Review of the Left/Right Judgment Task. J. Pain 2019, 20, 119–132. [Google Scholar] [CrossRef]
- Essick, G.; Afferica, T.; Aldershof, B.; Nestor, J.; Kelly, D.; Whitsel, B. Human perioral directional sensitivity. Exp. Neurol. 1988, 100, 506–523. [Google Scholar] [CrossRef]
- Gülbetekin, E.; Altun, E.; Er, M.N.; Fidancı, A.; Keskin, P.; Steenken, D. Effects of right or left face stimulation on self and other perception in enfacement illusion. Soc. Neurosci. 2021, 16, 1–17. [Google Scholar] [CrossRef]
- Wittkopf, P.; Lloyd, D.; Johnson, M. The effect of visual feedback of body parts on pain perception: A systematic review of clinical and experimental studies. Eur. J. Pain 2018, 22, 647–662. [Google Scholar] [CrossRef] [Green Version]
- Sessle, B.; Adachi, K.; Avivi-Arber, L.; Lee, J.; Nishiura, H.; Yao, D.; Yoshino, K. Neuroplasticity of face primary motor cortex control of orofacial movements. Arch. Oral Biol. 2007, 52, 334–337. [Google Scholar] [CrossRef]
- Brunsdon, V.E.A.; Bradford, E.E.F.; Smith, L.; Ferguson, H.J. Short-term physical training enhances mirror system activation to action observation. Soc. Neurosci. 2019, 15, 98–107. [Google Scholar] [CrossRef]
- Kawai, N.; Shibata, M.; Watanabe, M.; Horiuchi, S.; Fushima, K.; Tanaka, E. Effects of functional training after orthognathic surgery on masticatory function in patients with mandibular prognathism. J. Dent. Sci. 2020, 15, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Greene, D.L.; Appel, A.J.; Reinert, S.E.; Palumbo, M.A. Lumbar Disc Herniation. Spine 2005, 30, 826–829. [Google Scholar] [CrossRef]
- Nijs, J.; Roussel, N.; van Wilgen, C.P.; Köke, A.; Smeets, R. Thinking beyond muscles and joints: Therapists’ and patients’ attitudes and beliefs regarding chronic musculoskeletal pain are key to applying effective treatment. Man. Ther. 2013, 18, 96–102. [Google Scholar] [CrossRef]
- Moseley, G.L.; Nicholas, M.K.; Hodges, P. Does anticipation of back pain predispose to back trouble? Brain 2004, 127, 2339–2347. [Google Scholar] [CrossRef] [Green Version]
- Nijs, J.; van Wilgen, C.P.; Van Oosterwijck, J.; van Ittersum, M.; Meeus, M. How to explain central sensitization to patients with ‘unexplained’ chronic musculoskeletal pain: Practice guidelines. Man. Ther. 2011, 16, 413–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Louw, A.; Zimney, K.; Puentedura, E.J.; Diener, I. The efficacy of pain neuroscience education on musculoskeletal pain: A systematic review of the literature. Physiother. Theory Pract. 2016, 32, 332–355. [Google Scholar] [CrossRef]
- Marcos-Martín, F.; González-Ferrero, L.; Martín-Alcocer, N.; Paris-Alemany, A.; La Touche, R. Multimodal physiotherapy treatment based on a biobehavioral approach for patients with chronic cervico-craniofacial pain: A prospective case series. Physiother. Theory Pract. 2018, 34, 671–681. [Google Scholar] [CrossRef] [PubMed]
- Turk, D.C.; Wilson, H.D. Fear of Pain as a Prognostic Factor in Chronic Pain: Conceptual Models, Assessment, and Treatment Implications. Curr. Pain Headache Rep. 2010, 14, 88–95. [Google Scholar] [CrossRef] [Green Version]
- Bromberg, J.; Wood, M.E.; Black, R.A.; Ba, D.A.S.; Zacharoff, K.L.; Chiauzzi, E.J. A Randomized Trial of a Web-Based Intervention to Improve Migraine Self-Management and Coping. Headache J. Head Face Pain 2012, 52, 244–261. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sequence of Training (Task Levels) | Baseline | Progression When No Pain or Discomfort | What If…? |
|---|---|---|---|
| 1. Tactile acuity training |
|
| Pain experience?
Next, Step 2 |
| 2. Watching face activity left/right of picture |
|
| Pain experience?
Next, Step 3 |
| 3. Left/Right discrimination training (implicit) |
|
| Pain experience?
|
| 4. Left/Right discrimination training (explicit) |
|
| Pain experience?
|
| 5. Emotion recognition (implicit) |
|
| Pain experience?
|
| 6. Emotion expression imagination |
|
| Pain experience?
progression:
|
| 7. Emotion expression Movement (explicit) |
|
| Pain experience?
the pain and fear is increasing during the tasks. |
| 8. Face mirroring |
|
| Pain experience and or dysynchiria
|
| 9. Combinations | Randomization of task levels 2–7. Task: Start with maximum of 3 tasks levels, about 3–5 min |
| Pain experience and or dysynchiria
|
| 10. Orofacial exercises | Mouth opening with lingual guide, lateral jaw movement, lateral jaw mobilization with lingual guide. 1 set/8 repetitions of each exercise | Include the following exercises to the previous: lateral tongue strengthening, tongue strengthening exercise, lateral jaw movement strengthening, tongue protrusion strengthening, lip strength exercise. 1 set/10 repetitions holding 10 s each, and 10 s rest in between. | Pain experience?
Include a second set of all the exercises. |
| 11. Integrating of other behavioral Methods | Drawing up a list of fear/threat facial activity (top 5 list). Task: Start with the activity which causes less fear /pain with visual control with the mirror. |
| Pain or fear experience?
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
von Piekartz, H.; Paris-Alemany, A. Assessment and Brain Training of Patients Experiencing Head and Facial Pain with a Distortion of Orofacial Somatorepresentation: A Narrative Review. Appl. Sci. 2021, 11, 6857. https://0-doi-org.brum.beds.ac.uk/10.3390/app11156857
von Piekartz H, Paris-Alemany A. Assessment and Brain Training of Patients Experiencing Head and Facial Pain with a Distortion of Orofacial Somatorepresentation: A Narrative Review. Applied Sciences. 2021; 11(15):6857. https://0-doi-org.brum.beds.ac.uk/10.3390/app11156857
Chicago/Turabian Stylevon Piekartz, Harry, and Alba Paris-Alemany. 2021. "Assessment and Brain Training of Patients Experiencing Head and Facial Pain with a Distortion of Orofacial Somatorepresentation: A Narrative Review" Applied Sciences 11, no. 15: 6857. https://0-doi-org.brum.beds.ac.uk/10.3390/app11156857