
Using FEM to Assess the Effect of Orthodontic Forces on Affected Periodontium

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
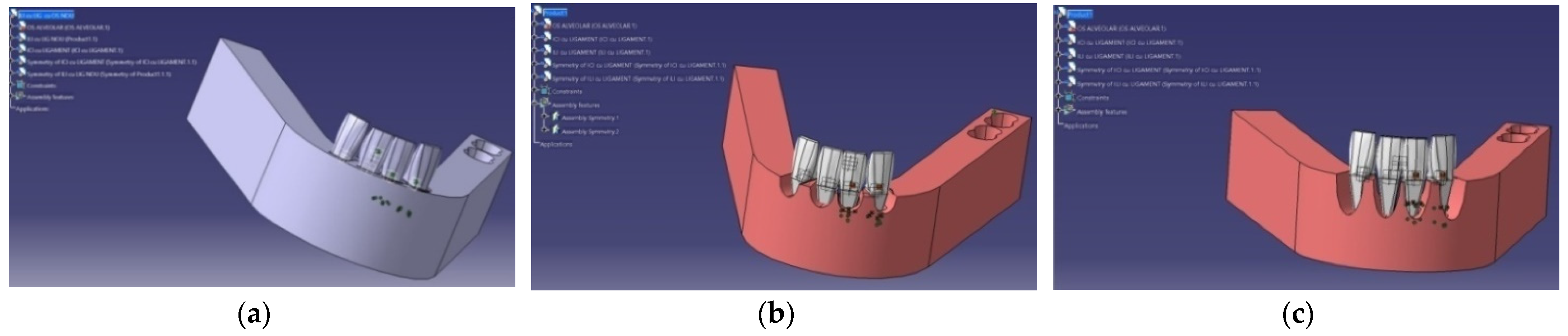
2.1. Analysis Model
2.2. Statistical Analyses
3. Results
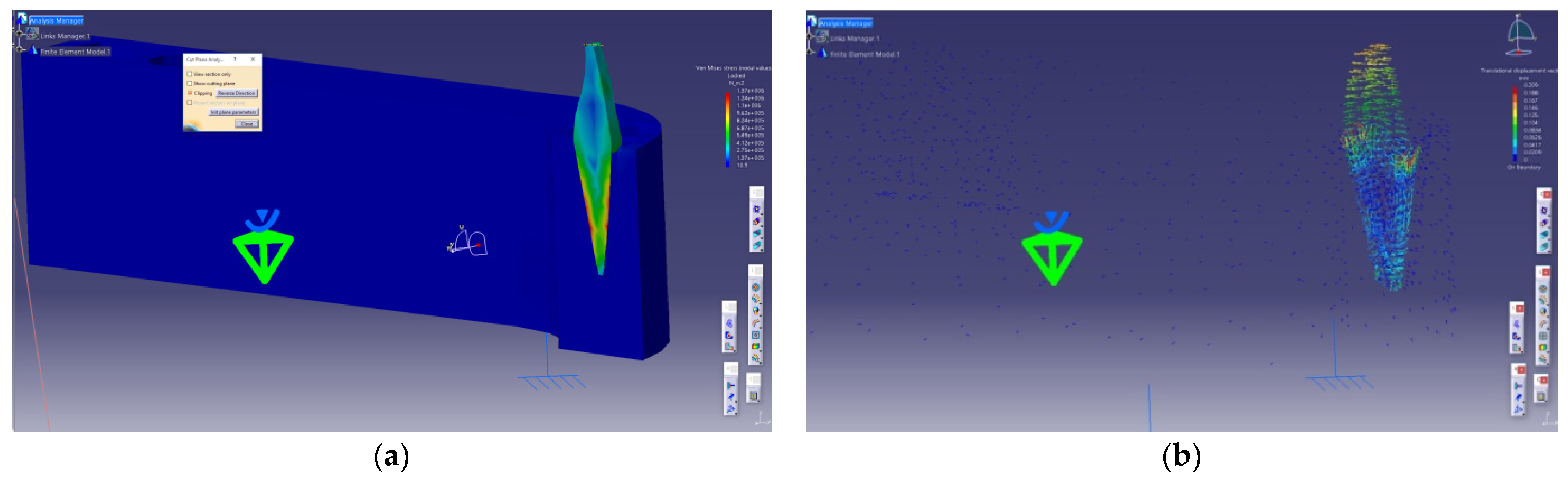
3.1. Lower Central Incisor (LCI)
3.1.1. Predictive Factors in the Modification of the Equivalent Tension Values in the Tooth–Periodontal Ligament–Alveolar Bone Complex (σ ech)
3.1.2. Predictive Factors in the Modification of the Tension Values in the Direction of an Applied Perpendicular Force to the Tooth’s Vestibular Surface (σ c)
3.1.3. Correlation of σ ech, σ c, and f Based on the Value of the Applied Force
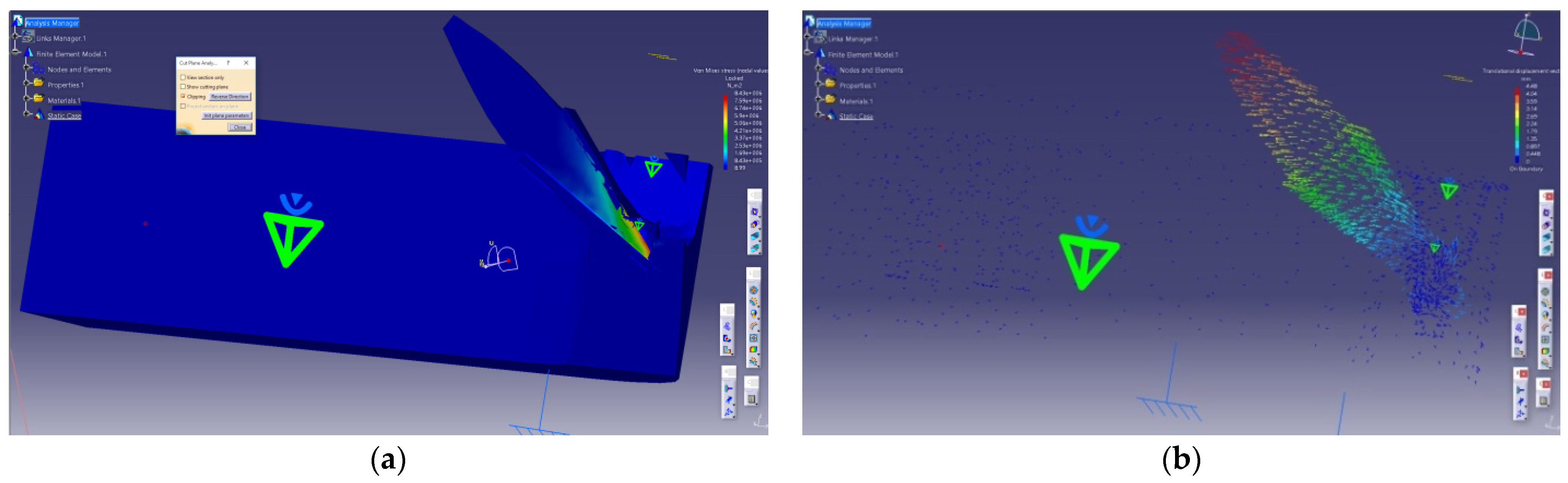
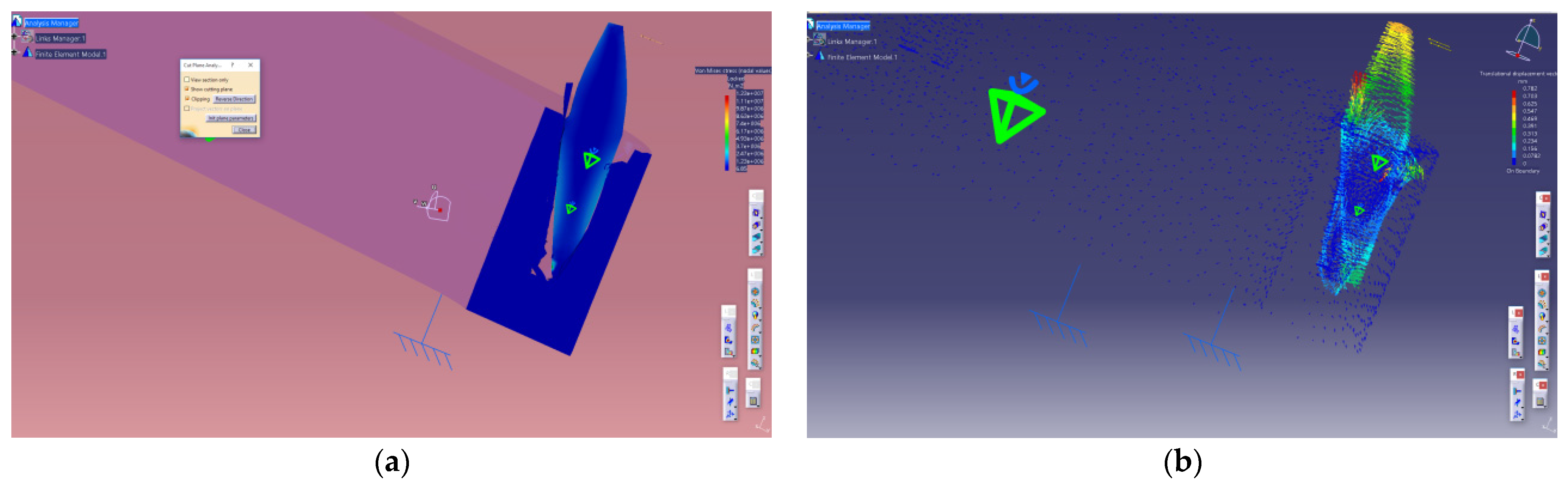
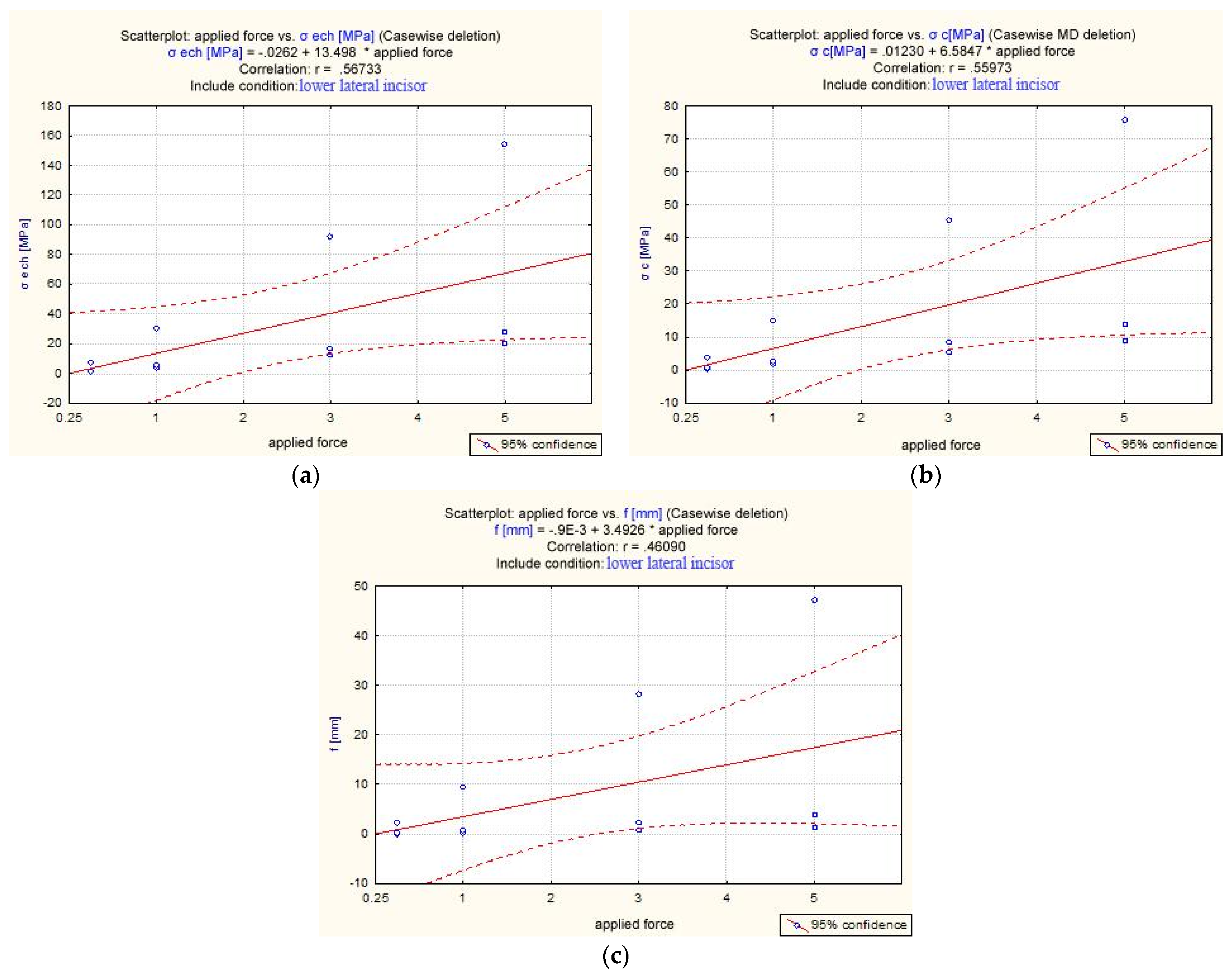
3.2. Lower Lateral Incisor (LLI)
3.2.1. Equivalent Tension in the Tooth–Periodontal Ligament–Alveolar Bone Complex (σ ech)
3.2.2. Tension Registered in the Direction of the Applied Force—Perpendicular to the Tooth’s Vestibular Surface [σ c]
3.2.3. Correlation Analysis of σ ech, σ c, and f Based on the Value of Applied Force
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Antoun, J.S.; Mei, L.; Gibbs, K.; Farella, M. Effect of orthodontic treatment on the periodontal tissues. Periodontology 2000 2017, 74, 140–157. [Google Scholar] [CrossRef] [PubMed]
- Sioustis, I.-A.; Martu, M.-A.; Aminov, L.; Pavel, M.; Cianga, P.; Kappenberg-Nitescu, D.C.; Luchian, I.; Solomon, S.M.; Martu, S. Salivary Metalloproteinase-8 and Metalloproteinase-9 Evaluation in Patients Undergoing Fixed Orthodontic Treatment before and after Periodontal Therapy. Int. J. Environ. Res. Public Health 2021, 18, 1583. [Google Scholar] [CrossRef] [PubMed]
- Pai, S.S.; Panda, S.; Pai, V.; Anandu, M.; Vishwanath, E.; Suhas, A.S. Effects of labial and lingual retraction and intrusion force on maxillary central incisor with varying collum angles: A three-dimensional finite elemental analysis. J. Indian Orthod. Soc. 2017, 51, 28–37. [Google Scholar] [CrossRef] [Green Version]
- Luchian, I.; Moscalu, M.; Martu, I.; Vata, I.; Stirbu, C.; Olteanu, D.; Pasarin, L.; Martu, M.A.; Solomon, S.; Anton, D.; et al. Perspectives and limits of mandibular lateral incisor intrusion associated with periodontal disease. A FEM study. Rom. J. Oral Rehabil. 2018, 10, 60–70. [Google Scholar]
- Kumar, A.; Konda, P. Patterns of Stress Distribution During Simple Tooth Movements: A Finite Element Study. Indian J. Stomatol. 2012, 3, 226. [Google Scholar]
- Srirekha, A.; Bashetty, K. Infinite to finite: An overview of finite element analysis. Indian J. Dent. Res. 2010, 21, 425. [Google Scholar] [CrossRef]
- Huang, H.-L.; Tsai, M.-T.; Yang, S.-G.; Su, K.-C.; Shen, Y.-W.; Hsu, J.-T. Mandible Integrity and Material Properties of the Periodontal Ligament during Orthodontic Tooth Movement: A Finite-Element Study. Appl. Sci. 2020, 10, 2980. [Google Scholar] [CrossRef]
- Jones, M.L.; Hickman, J.; Middleton, J.; Knox, J.; Volp, C. A validated finite element method study of orthodontic tooth movement in the human subject. J. Orthod. 2014, 16. [Google Scholar] [CrossRef] [PubMed]
- Tatarciuc, M.; Maftei, G.A.; Vitalariu, A.; Luchian, I.; Martu, I.; Diaconu-Popa, D. Inlay-Retained Dental Bridges—A Finite Element Analysis. Appl. Sci. 2021, 11, 3770. [Google Scholar] [CrossRef]
- Luchian, I.; Vata, I.; Martu, I.; Stirbu, C.; Tatarciuc, M.; Martu, S. The periodontal effects of an optimal intrusive force on a maxillary central incisor. A FEM evaluation. Rom. J. Oral Rehabil. 2016, 8, 51–55. [Google Scholar]
- Kanjanaouthai, A.; Mahatumarat, K.; Techalertpaisarn, P.; Versluis, A. Effect of the inclination of a maxillary central incisor on periodontal stress: Finite element analysis. Angle Orthod. 2012, 82, 812–819. [Google Scholar] [CrossRef] [PubMed]
- Hemanth, M.; Deoli, S.; Raghuveer, H.P.; Rani, M.S.; Hegde, C.; Vedavathi, B. Stress induced in periodontal ligament under orthodontic loading (Part II): A comparison of linear versus non-linear FEM study. J. Int. Oral Health 2015, 7, 114. [Google Scholar]
- Jain, A.; Prasantha, G.S.; Mathew, S.; Sabrish, S. Analysis of stress in periodontium associated with orthodontic tooth movement: A three dimensional finite element analysis. Comput. Methods Biomech. Biomed. Eng. 2021, 1, 1. [Google Scholar] [CrossRef] [PubMed]
- Seo, J.H.; Eghan-Acquah, E.; Kim, M.S.; Lee, J.H.; Jeong, Y.H.; Jung, T.G.; Hong, M.; Kim, W.H.; Kim, B.; Lee, S.J. Comparative Analysis of Stress in the Periodontal Ligament and Center of Rotation in the Tooth after Orthodontic Treatment Depending on Clear Aligner Thickness—Finite Element Analysis Study. Materials 2021, 14, 324. [Google Scholar] [CrossRef]
- Fill, T.S.; Toogood, R.W.; Major, P.W.; Carey, J.P. Analytically determined mechanical properties of, and models for the periodontal ligament: Critical review of literature. J. Biomech. 2012, 45, 9–16. [Google Scholar] [CrossRef]
- Bhalajhi, S.I. Dental Anatomy-Histology and Development; Arya Publishing House: New Dehli, India, 2009; pp. 51–139. [Google Scholar]
- Hohmann, A.; Kober, C.; Young, P.; Dorow, C.; Geiger, M.; Boryor, A.; Sander, F.M.; Sander, C.; Sander, F.G. Influence of different modeling strategies for the periodontal ligament on finite element simulation results. Am. J. Orthod. 2011, 139, 775–783. [Google Scholar] [CrossRef]
- Caballero, G.M.; Carvalho Filho, O.A.; Hargreaves, B.O.; Brito, H.H.; Magalhães Júnior, P.A.; Oliveira, D.D. Mandibular canine intrusion with the segmented arch technique: A finite element method study. Am. J. Orthod. Dentofac. Orthop. 2015, 147, 691–697. [Google Scholar] [CrossRef] [PubMed]
- Kurgan, S.; Terzioglu, H.; Yılmaz, B. Stress distribution in reduced periodontal supporting tissues surrounding splinted teeth. Int. J. Periodontics Restor. Dent. 2014, 34, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Xia, Z.; Jiang, F.; Chen, J. Estimation of periodontal ligament’s equivalent mechanical parameters for finite element modeling. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 486–491. [Google Scholar] [CrossRef] [Green Version]
- Theodorou, C.I.; Kuijpers-Jagtman, A.M.; Bronkhorst, E.M.; Wagener, F.A. Optimal force magnitude for bodily orthodontic tooth movement with fixed appliances: A systematic review. Am. J. Orthod. Dentofac. Orthop. 2019, 156, 582–592. [Google Scholar] [CrossRef]
- Flores-Mir, C. Forces Between 50 and 100 cN May be Best for Mesiodistal Orthodontic Tooth Movements by Fixed Appliances. J. Evid. Based Dent. Pract. 2020, 20, 101490. [Google Scholar] [CrossRef] [PubMed]
- Romanyk, D.L.; Vafaeian, B.; Addison, O.; Adeeb, S. The use of finite element analysis in dentistry and orthodontics: Critical points for model development and interpreting results. Semin. Orthod. 2020, 26, 162–173. [Google Scholar] [CrossRef]
- Cuoghi, O.A.; Topolski, F.; de Faria, L.P.; Ervolino, E.; Micheletti, K.R.; Miranda-Zamalloa, Y.M.; Moresca, R.; Moro, A.; de Mendonça, M.R. Correlation between pain and hyalinization during tooth movement induced by different types of force. Angle Orthod. 2019, 89, 788–796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rudolph, D.J.; Willes, M.G.; Sameshima, G.T. A finite element model of apical force distribution from orthodontic tooth movement. Angle Orthod. 2001, 71, 127–131. [Google Scholar]
- Gupta, M.; Madhok, K.; Kulshrestha, R.; Chain, S.; Kaur, H.; Yadav, A. Determination of stress distribution on periodontal ligament and alveolar bone by various tooth movements—A 3D FEM study. J. Oral Biol. Craniofac. Res. 2020, 10, 758–763. [Google Scholar] [CrossRef]
- Vikram, N.R.; Kumar, K.S.; Nagachandran, K.S.; Hashir, Y.M. Apical stress distribution on maxillary central incisor during various orthodontic tooth movements by varying cemental and two different periodontal ligament thicknesses: A FEM study. Indian J. Dent. Res. 2012, 23, 213. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Yu, M.; Jin, S.; Wang, Y.; Luo, R.; Huo, B.; Liu, D.; He, D.; Zhou, Y.; Liu, Y. Stress distribution and collagen remodeling of periodontal ligament during orthodontic tooth movement. Front. Pharmacol. 2019, 10, 1263. [Google Scholar] [CrossRef]
- Cattaneo, P.M.; Dalstra, M.; Melsen, B. Strains in periodontal ligament and alveolar bone associated with orthodontic tooth movement analyzed by finite element. Orthod. Craniofac. Res. 2009, 12, 120–128. [Google Scholar] [CrossRef]
- Zargham, A.; Geramy, A.; Rouhi, G. Evaluation of long-term orthodontic tooth movement considering bone remodeling process and in the presence of alveolar bone loss using finite element method. Orthod. Waves 2016, 75, 85–96. [Google Scholar] [CrossRef]
- Toms, S.R.; Eberhardt, A.W. A nonlinear finite element analysis of the periodontal ligament under orthodontic tooth loading. Am. J. Orthod. Dentofac. Orthop. 2003, 123, 657–665. [Google Scholar] [CrossRef]
- Ma, Y.; Li, S. The optimal orthodontic displacement of clear aligner for mild, moderate and severe periodontal conditions: An in vitro study in a periodontally compromised individual using the finite element model. BMC Oral Health 2021, 21, 109. [Google Scholar] [CrossRef]
- Uhlir, R.; Mayo, V.; Lin, P.H.; Chen, S.; Lee, Y.T.; Hershey, G.; Lin, F.C.; Ko, C.C. Biomechanical characterization of the periodontal ligament: Orthodontic tooth movement. Angle Orthod. 2017, 87, 183–192. [Google Scholar] [CrossRef] [PubMed]
- Mascarenhas, R.; Chatra, L.; Shenoy, S.; Husain, A.; Mathew, J.M.; Parveen, S. A comparative study of forces in labial and lingual orthodontics using finite element method. J. Indian Orthod. Soc. 2015, 49, 15–18. [Google Scholar] [CrossRef] [Green Version]
- Ammar, H.H.; Ngan, P.; Crout, R.J.; Mucino, V.H.; Mukdadi, O.M. Three-dimensional modeling and finite element analysis in treatment planning for orthodontic tooth movement. Am. J. Orthod Dentofac. Orthop. 2011, 139, e59–e71. [Google Scholar] [CrossRef]
- Moga, R.A.; Buru, S.M.; Chiorean, C.G.; Cosgarea, R. Compressive stress in periodontal ligament under orthodontic movements during periodontal breakdown. Am. J. Orthod. Dentofac. Orthop. 2021, 159, e291–e299. [Google Scholar] [CrossRef] [PubMed]
- Roscoe, M.G.; Cattaneo, P.M.; Dalstra, M.; Ugarte, O.M.; Meira, J.B. Orthodontically induced root resorption: A critical analysis of finite element studies’ input and output. Am. J. Orthod. Dentofac. Orthop. 2021, 159, 779–789. [Google Scholar] [CrossRef] [PubMed]
- Lombardo, L.; Stefanoni, F.; Mollica, F.; Laura, A.; Scuzzo, G.; Siciliani, G. Three-dimensional finite-element analysis of a central lower incisor under labial and lingual loads. Prog. Orthod. 2012, 13, 154–163. [Google Scholar] [CrossRef]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Lower Central Incisor (LCI) | Lower Lateral Incisor (LLI) | |
|---|---|---|
| Crown length | 9 mm | 9.5 mm |
| Root length | 12.5 mm | 14 mm |
| Total length | 21.5 mm | 23.5 mm |
| M-D crown diameter | 5 mm | 5.5 mm |
| M-D crown diameter at cervical level | 3.5 mm | 4 mm |
| F-O crown diameter | 6 mm | 6.5 mm |
| F-O crown diameter at cervical level | 5.3 mm | 5.8 mm |
| Material | Young’s Modulus | Poisson’s Coefficient | References |
|---|---|---|---|
| Tooth | 20 GPa | 0.30 | Caballero et al. 2015 [18] |
| Cortical bone | 13.7 GPa | 0.30 | Kurgan et al. 2014 [19] |
| Spongy bone | 345 MPa | 0.30 | Caballero et al. 2015 [18] |
| Periodontal ligament | 0.71 MPa | 0.40 | Xia et al. 2013 [20] |
| Applied Force | Extent of Periodontal Damage (HBL) | ||
|---|---|---|---|
| No HBL | 33% HBL | 66% HBL | |
| 0.25 N | σ ech = 0.0271 MPa | σ ech = 0.73 MPa | σ ech = 2.1 MPa |
| σ c = 0.0272 MPa | σ c = 0.751 MPa | σ c = 2.16 MPa | |
| f = 0.00468 mm | f = 0.124 mm | f = 1.12 mm | |
| 1 N | σ ech = 1.37 MPa | σ ech = 2.92 MPa | σ ech = 8.43 MPa |
| σ c = 1.38 MPa | σ c = 2.98 MPa | σ c = 8.67 MPa | |
| f = 0.208 mm | f = 0.497 mm | f = 4.48 mm | |
| 3 N | σ ech = 4.12 MPa | σ ech = 8.74 MPa | σ ech = 25.3 MPa |
| σ c = 4.15 MPa | σ c = 8.91 MPa | σ c = 26 MPa | |
| f = 0.626 mm | f = 1.49 mm | f = 13.4 mm | |
| 5 N | σ ech = 6.86 MPa | σ ech = 14.6 MPa | σ ech = 42.2 MPa |
| σ c = 6.94 MPa | σ c = 14.9 MPa | σ c = 43.3 MPa | |
| f = 1.04 mm | f = 2.49 mm | f = 22.4 mm | |
| Applied Force | Extent of Periodontal Damage (HBL) | ||
|---|---|---|---|
| No HBL | 33% HBL | 66% HBL | |
| 0.25 N | σ ech = 1.03 MPa | σ ech = 1.4 MPa | σ ech = 7.67 MPa |
| σ c = 0.455 MPa | σ c = 0.697 MPa | σ c = 3.79 MPa | |
| f = 0.065 mm | f = 0.198 mm | f = 2.35 mm | |
| 1 N | σ ech = 4.16 MPa | σ ech = 5.59 MPa | σ ech = 30.7 MPa |
| σ c = 1.86 MPa | σ c = 2.79 MPa | σ c = 15.2 MPa | |
| f = 0.26 mm | f = 0.794 mm | f = 9.41 mm | |
| 3 N | σ ech = 12.3 MPa | σ ech = 16.8 MPa | σ ech = 92.1 MPa |
| σ c = 5.39 MPa | σ c = 8.37 MPa | σ c = 45.5 MPa | |
| f = 0.782 mm | f = 2.38 mm | f = 28.3 mm | |
| 5 N | σ ech = 20.5 MPa | σ ech = 28 MPa | σ ech = 154 MPa |
| σ c = 8.92 MPa | σ c = 14 MPa | σ c = 75.9 MPa | |
| f = 1.3 mm | f = 3.97 mm | f = 47.1 mm | |
| Correlation Coefficient (Beta) | Std. Err. (Beta) | B | Std. Err. B | t | p 95% CI | |
|---|---|---|---|---|---|---|
| Partial correlation σ ech vs. | ||||||
| Intercept | −837.143 | 249.0675 | −3.36111 | 0.008 | ||
| Applied force | 0.659321 | 0.166887 | 4.260 | 1.0783 | 3.95071 | 0.003 |
| Periodontal damage | 0.560924 | 0.166887 | 8.207 | 2.4416 | 3.36111 | 0.008 |
| Partial correlation σ c vs. | ||||||
| Intercept | −862.383 | 256.3378 | −3.36424 | 0.008 | ||
| Applied force | 0.656882 | 0.167272 | 4.358 | 1.1098 | 3.92702 | 0.003 |
| Periodontal damage | 0.562749 | 0.167272 | 8.454 | 2.5129 | 3.36427 | 0.008 |
| Partial correlation f vs. | ||||||
| Intercept | −503.908 | 171.6010 | −2.93651 | 0.016 | ||
| Applied force | 0.485140 | 0.208293 | 1.730 | 0.7429 | 2.32912 | 0.044 |
| Periodontal damage | 0.611691 | 0.208293 | 4.940 | 1.6822 | 2.93669 | 0.016 |
| Correlation Coefficient (Beta) | Std. Err. (Beta) | B | Std. Err. B | t | p 95% CI | |
|---|---|---|---|---|---|---|
| Partial correlation σ ech vs. | ||||||
| Intercept | −3142.65 | 1085.324 | −2.89558 | 0.017 | ||
| Applied force | 0.567328 | 0.197499 | 13.50 | 4.699 | 2.87256 | 0.018 |
| Periodontal damage | 0.571916 | 0.197499 | 30.81 | 10.640 | 2.89580 | 0.017 |
| Partial correlation σ c vs. | ||||||
| Intercept | −1577.99 | 535.3633 | −2.94752 | 0.016 | ||
| Applied force | 0.559729 | 0.197028 | 6.58 | 2.3178 | 2.84086 | 0.019 |
| Periodontal damage | 0.580795 | 0.197028 | 15.47 | 5.2482 | 2.94778 | 0.016 |
| Partial correlation f vs. | ||||||
| Intercept | −1080.60 | 371.9040 | −2.90559 | 0.017 | ||
| Applied force | 0.460901 | 0.212483 | 3.49 | 1.6101 | 2.16912 | 0.058 |
| Periodontal damage | 0.617439 | 0.212483 | 10.59 | 3.6458 | 2.90583 | 0.017 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luchian, I.; Martu, M.-A.; Tatarciuc, M.; Scutariu, M.M.; Ioanid, N.; Pasarin, L.; Kappenberg-Nitescu, D.C.; Sioustis, I.-A.; Solomon, S.M. Using FEM to Assess the Effect of Orthodontic Forces on Affected Periodontium. Appl. Sci. 2021, 11, 7183. https://0-doi-org.brum.beds.ac.uk/10.3390/app11167183
Luchian I, Martu M-A, Tatarciuc M, Scutariu MM, Ioanid N, Pasarin L, Kappenberg-Nitescu DC, Sioustis I-A, Solomon SM. Using FEM to Assess the Effect of Orthodontic Forces on Affected Periodontium. Applied Sciences. 2021; 11(16):7183. https://0-doi-org.brum.beds.ac.uk/10.3390/app11167183
Chicago/Turabian StyleLuchian, Ionut, Maria-Alexandra Martu, Monica Tatarciuc, Mihaela Monica Scutariu, Nicoleta Ioanid, Liliana Pasarin, Diana Cristala Kappenberg-Nitescu, Ioana-Andreea Sioustis, and Sorina Mihaela Solomon. 2021. "Using FEM to Assess the Effect of Orthodontic Forces on Affected Periodontium" Applied Sciences 11, no. 16: 7183. https://0-doi-org.brum.beds.ac.uk/10.3390/app11167183