
Advances in Biomaterials for Breast Reconstruction


1
SMG-SNU Boramae Medical Center, Department of Plastic and Reconstructive Surgery, Seoul National University College of Medicine, Seoul 07061, Korea
2
Department of Plastic and Reconstructive Surgery, Seoul National University College of Medicine, Seoul National University Hospital, Seoul 03080, Korea
*
Authors to whom correspondence should be addressed.
Appl. Sci. 2021, 11(16), 7493; https://0-doi-org.brum.beds.ac.uk/10.3390/app11167493
Submission received: 7 July 2021
/
Revised: 4 August 2021
/
Accepted: 11 August 2021
/
Published: 15 August 2021
(This article belongs to the Special Issue Current Techniques in Implants for Plastic Surgery)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Breast cancer is one of the most commonly diagnosed malignancies in women. Along with increasing demands for breast reconstruction, the attention given to the psychological and aesthetic benefits of breast reconstruction has also increased. As breast reconstruction and augmentation demands increase, biomaterials for breast reconstruction are being developed, and the related industry is growing quickly worldwide. Among the various biomaterials used for breast enlargement, breast implants have undergone a remarkable evolution since the 1960s. Despite unsatisfactory results and unexpected complications, research dedicated to achieving an ideal breast implant has progressed. In accordance with attention to tissue engineering, a three-dimensional (3D) bioprinting technique for breast tissue regeneration has emerged to overcome the current limitations of breast biomaterials. Along with solid implants, injectable liquid-type fillers are also part of ongoing studies.
1. Introduction
Breast cancer is one of the most commonly diagnosed malignancies in women. In 2018, approximately two million women globally were diagnosed with breast cancer, accounting for almost one in four cancer cases in women [1]. The number of newly diagnosed breast cancer cases has more than doubled, with the portion of cases seen in younger women increasing [2]. Although the five-year survival rate for breast cancer has improved, the disease burden remains high in most countries [3,4]. Therefore, demands for breast reconstruction exist, and the recent increase in the popularity of social media has made evident the attention given to body image. The numbers of bilateral mastectomy and immediate reconstruction procedures have increased, and the psychological and aesthetic benefits of breast reconstruction have also increased. As breast reconstruction and augmentation demands increase, biomaterials for use in breast reconstruction are being developed, and the related industry is growing quickly worldwide.
Among the various biomaterials used for breast enlargement, breast implants have undergone a remarkable evolution since the 1960s. Despite unsatisfactory results and unexpected complications, research dedicated to achieving an ideal breast implant has progressed. In accordance with tissue engineering, a 3D bioprinting technique for breast tissue regeneration has emerged to overcome the current limitations of breast biomaterials. Along with solid implants, injectable liquid-type fillers are also part of ongoing studies.
2. Breast Implant
2.1. Introduction of Saline Implant
The first use of saline-filled breast implants was reported in 1965, and less than a decade later clinical trials were performed to evaluate this implant [5,6,7]. The biggest advantage of the saline implant for augmentation was that it could be inserted through a small incision because the implant could be inserted before inflation. After the implant was inserted, inflation was performed with liquid saline.
However, the saline implant had several limitations [8]. First, the early saline-filled implant had a high deflation rate due to underdeveloped shells and valves. Secondly, the mechanism of post-filling had some pitfalls. Underfilling with saline resulted in increased deflation rates and visible surface wrinkles, and overfilling caused unexpected shape deformities and unnatural firmness. Most importantly, the feel of the implant on palpation after insertion into the breast was not similar to natural breast tissue. These critical limitations of saline implants increased the demand for a more natural and consistent implant material.
2.2. History of Silicone Gel Implant
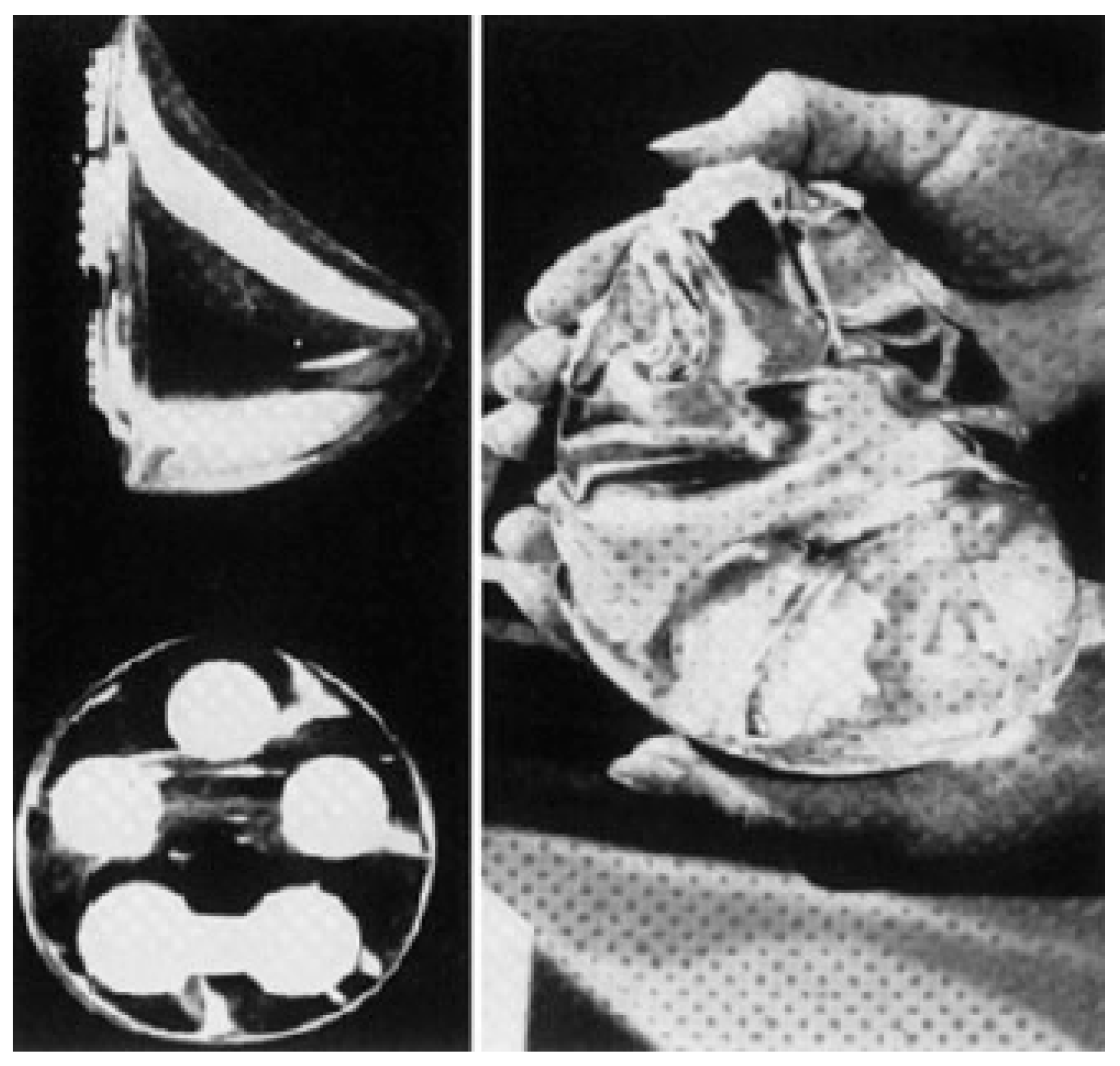
The emergence of the silicone gel implant caused a revolution in breast augmentation. The silicone gel implant was first introduced by Cronin in 1962 and was manufactured by the Dow Corning Corporation between 1963 and 1972 [9]. The implant consisted of a thick, smooth silicone elastomer as two separate envelopes connected along the periphery. The shell (the outer cover of the implant) was filled with a moderately viscous gel, and Dacron patches were attached at the posterior surface of the implant to avoid rotation and induce the proper positioning of the device (Figure 1). However, some women developed very firm breasts less than one year after breast augmentation. As the principle of capsular contracture (the constriction of a capsule of scar tissue around the implant) was not well understood at the time, this breast firmness was attributed to the firmness of the implant. As a result, a new generation of softer breast implants was demanded.
The second-generation silicone gel implant was introduced in 1972 and used for a decade. A thinner shell without Dacron patches and a less viscous gel were used to avoid capsular contracture to overcome previous drawbacks. The gel consisted of 20% highly crosslinked silicone and 80% low molecular weight chains [10]. However, the implants tended to rupture, leading to silicone gel spillage into the periprosthetic space. The oily and sticky component was found within the peri-implant capsule of both ruptured implants and even visually intact implants [11,12,13,14,15,16,17,18].
The third generation of silicone gel implant was introduced with a stronger and thicker shell, as the main goal was to eliminate silicone gel spillage and avoid implant rupture. The newly developed implant had two layers of silicone elastomer and a thin (0.01 mm) layer of fluorosilicone placed between them. Despite a lower capsular contracture rate, there were social concerns about the safety of the silicone gel prosthesis for breasts, given their high complication rates and uncertain effect on soft tissue [19,20,21]. As a result, the Food and Drug Administration (FDA) abandoned the use of third-generation implants in the United States [22,23,24,25,26,27].
Fourth-generation and fifth-generation silicone gel implants were manufactured strictly by the American Society for Testing Methodology [28]. Manufacturers provided improved quality control of the breast implant, and various shapes and surface textures were produced. At the same time, the concept of an anatomically shaped implant, composed of a more cohesive gel, was introduced [29,30,31].
2.3. Modification of Implant Surface Topography
A silicone gel implant with a smooth surface was the earliest form and is still being used today. However, the frequency of its use is decreasing because of the relatively high capsular contracture rate. According to previous studies, the rate of capsular contracture is higher for smooth implants than for textured surface implants [32,33,34,35].
Manufacturers presented breast implants with a textured surface to overcome the high capsular contracture rate of implants with a smooth surface [36,37]. Initial textured implants were made with a polyurethane coating, developed in the 1970s [38]. Studies indicated that a polyurethane foam-coated silicone gel implant might reduce capsular contracture [39,40]. After capsular formation around the implant, the 1.5 to 2.0 mm-thick polyurethane coating disintegrated, and it was hypothesized that the tightening that occurred would prevent the alignment of myofibroblasts and eventually interrupt the capsular contracture process [41]. The use of polyurethane implants has spread worldwide since they were introduced. However, as polyurethane foam degraded, it was found to release carcinogenic 2,4-toluene diamine (TDA). This subsequently led to complete prohibition by the FDA in 1991, and this implant was removed from the market. Later, it was revealed that the small amount of 2,4-TDA released would not significantly increase risk [42]. The surgical use of the polyurethane-coated implant continued in countries other than the US. The safety and effectiveness of reducing the capsular contracture rate have been reported on by multiple authors [43,44,45].
As polyurethane foam-covered silicone gel implants are not as biocompatible as silicone, textured implants have been introduced to inhibit capsule formation. Through the “adhesive effect” of the pores on the surface of the textured implant, the stabilization and fixing of the implant in the breast pocket could be achieved. In addition, a textured silicone implant causes less fibrosis, and, as a result, the frequency of capsular contracture is lower than that of a smooth implant [35,46,47]. Still, many textured implants are associated with a significant rate of capsular contracture, and texturization during manufacture has been associated with a collection of serous fluid that develops under the surface in the body (seroma) and double capsule formation.
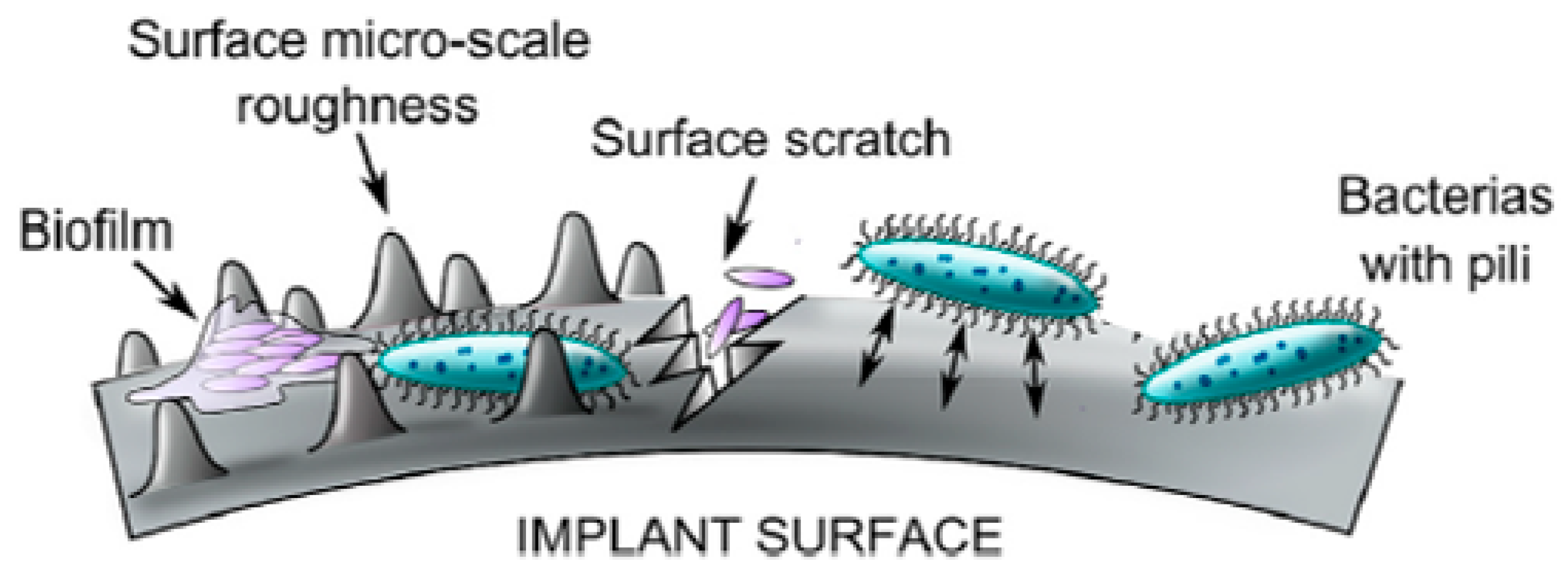
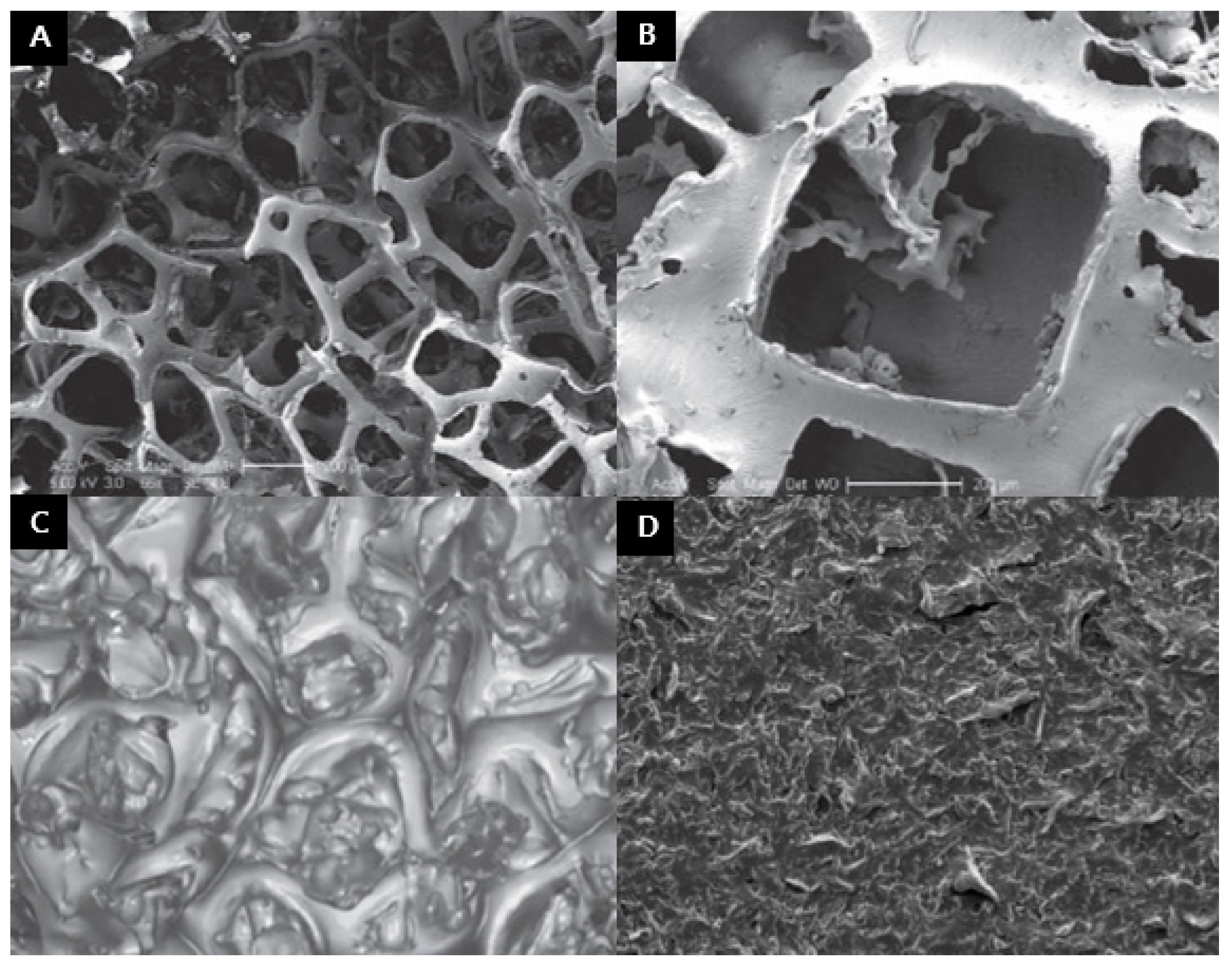
For the next generation of implants, micro- or nanotextured implants were developed by controlling the roughness of the existing surface. The rough surface may induce bacterial colonization by providing space for bacteria and more points of direct contact between the pathogenic cell and the implant surface (Figure 2) [48]. By avoiding aggressive texturing with the projection of sugar crystals and salt onto the implant, reduced roughness has promoted a more natural interaction between the implant and soft tissue, potentially reducing inflammation. For example, Sientra’s Silimed has a web-like organization at the implant’s surface, and Allergan Biocell has a salt-loss pattern on the surface. However, the microtextured implant, such as Mentor Siltex, is manufactured using a pressure imprint-stamping technique (Figure 3A–C) [49]. One of the nanotextured implants, Motiva Silksurface, is manufactured using negative imprinting with three-dimensional (3D) technology. It optimizes biocompatibility by structuring a uniform topography using 3D imprinting on polydimethylsiloxane (PDMS) material to build the outer shell (Figure 3D) [50]. These changes to the surface have minimized inflammation and, in turn, reduced breast implant-related complications such as capsular contracture and late seromas. Moreover, a higher number of contact points could prevent the aggregation of fibroblasts, which might lead to capsular contracture.
In addition to surface structural modification, modifications using biomaterials are also in progress to minimize capsular contracture. In the porcine model, a 2-methacryloyloxyethyl phosphorylcholine (MPC)-based polymer was grafted on a silicone breast implant and inserted under the skin [51]. MPC-based polymer is known to reduce protein adsorption and inhibit cell adhesion. The results of the study showed a reduction in inflammatory cell recruitment and myoblast markers; consequently, a reduced capsular thickness was observed. Moreover, there are several studies on antibacterial components on breast implant surfaces to lower the incidence of capsular contracture [52,53].
2.4. Modification of Filling Material in Breast Implant
Silicone has been used as a filler since the first implant was introduced in the 1960s. Since the initial development, multiple modifications of filler characteristics have been made to achieve a more durable, consistent, and natural shape. In the past, the property of the silicone filler in breast implants had been thought to be an important factor affecting the capsular contracture rate [54,55]. However, by the evolution of fourth-generation implants, better safety had been explored, and long-term outcomes had been described [56,57].
Silicone is a mixture of semi-inorganic polymeric molecules composed of different length chains of polydimethylsiloxane monomers [30]. The property of the silicone can be varied by the polymer chain length and degree of crosslinking between polymer chains [58]. For example, in liquid silicone the length of the polymer chain is shorter on average, and the degree of crosslinking is minimal. However, in silicone gel, the length of the polymer chain and the degree of crosslinking is increased to maintain the implant’s shape.
The cohesiveness of the breast implant varies by manufacturer. According to a study by Maxwell et al., the Allergan 410 implant had the highest cohesivity when compared with the Mentor CPG implant [56]. Stevens et al. reported that Sientra’s form-stable implant had the least cohesiveness when compared to the Allergan 410 and Mentor CPG implants [59]. However, as there is no standardized grading system for implant cohesiveness, accurate comparison between various implants is difficult. Moreover, as cohesivity is not the only factor that affects implant stiffness, it is not appropriate to interpret high cohesiveness of the implant as high stiffness.
2.5. Breast Implant Associated Anaplastic Large Cell Lymphoma (BIA-ALCL) Issues
As the evolution of the silicone gel implant proceeded, breast implant-associated anaplastic large cell lymphoma (BIA-ALCL) became a significant public concern of women with textured implants. The rising incidence of BIA-ALCL has increased awareness of the use of textured implants. The FDA has received approximately 359 adverse reports of ALCL in women with breast implants, which were reported to the Manufacturer and User Facility Device Experience (MAUDE) database as of February 2017. According to a previous study, BIA-ALCL only occurs in association with textured implants [60]. According to the study carried out by the US FDA, the disease risk of BIA-ALCL was 1:2943 with the Biocell textured implant [61]. The Australian Therapeutic Goods Administration reported that the disease risks were 1:3705 for the Biocell implant, 1:3894 for the Silimed polyurethane implant, and 1:60,631 for the Mentor Siltex implant [62].
In 2019, the FDA issued a recall of the Allergan Biocell textured breast implant, which is classified as a macrotextured implant [63,64]. However, the FDA did not recommend removing or replacing textured implants in asymptomatic patients [65]. Instead, all patients with breast implants were notified of the risk for developing BIA-ALCL, and patients with textured implants were counseled about risk management options. Two thirds of BIA-ALCL patients present with a malignant effusion between the fibrous capsule and the implant. The other one third of patients present with a palpable mass, which may indicate a more aggressive clinical course [66]. The National Comprehensive Cancer Network (NCCN) has suggested several guidelines for management [67].
If BIA-ALCL is localized to the capsule only, it may be treated with surgery; however, in advanced cases, including lymph node involvement, surgery and chemotherapy or radiotherapy are indicated for treatment. To reduce the risk of developing BIA-ALCL, removing textured devices with subsequent closure, exchange for a smooth implant, or conversion to autologous reconstruction could be options [68]. Consequently, in clinics there is a tendency worldwide for surgeons and patients to alter their implant choices from textured to smooth-surface implants [69].
3. Scaffold Guided Breast Tissue Engineering
3.1. Three Dimensional (3D) Bioprinting Technique for Breast Tissue Regeneration
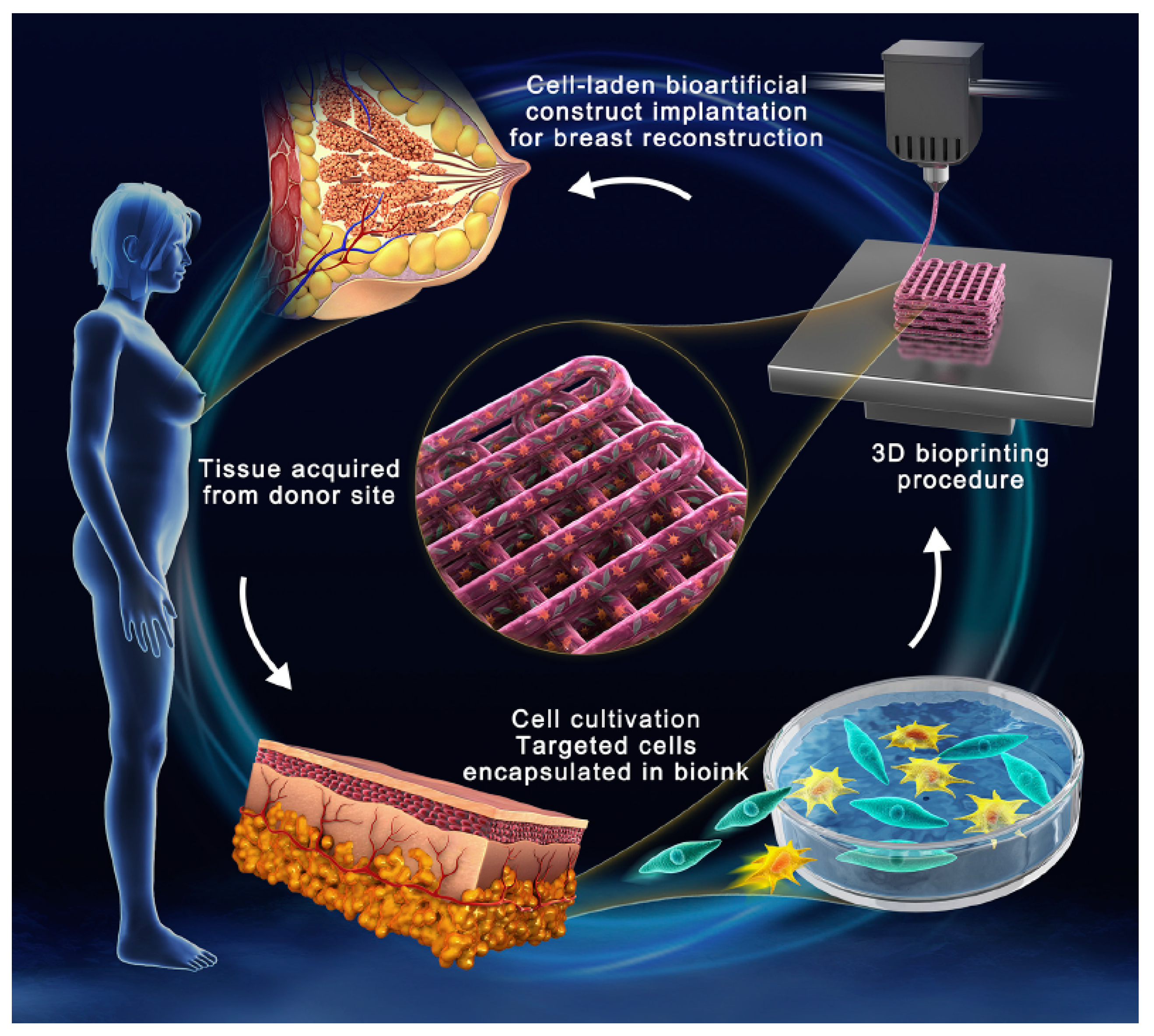
Three dimensional (3D) bioprinting is a valuable tool for regenerative medicine and tissue engineering. It involves fabricating complex bioactive structures with cell-laden bioink under the guidance of computer-aided design (CAD) in a layer-by-layer fashion (Figure 4) [70]. The most frequently used 3D printing techniques for breast tissue regeneration are inkjet printing, extrusion-based bioprinting (EBB), light-mediated stereolithography (SLA), and digital light processing (DLP). Inkjet printing is the most commonly used bioprinting method which provides cell viability via thermal or piezoelectric processes [71]. EBB is capable of handling bioink of a high viscosity using a fluid-dispensing system, which has been mostly utilized in the bioprinting of adipose tissue [72].
Several studies have investigated structural concepts to obtain the most suitable 3D model for breast tissue engineering. Mohseni et al. researched the ideal additive biomanufacturing of scaffold model for breast reconstruction using a 3D bioprinting technique [73]. In the study, the model was focused on two independent structures. The external structure was designed for the integrity of the scaffold and minimized direct stress transfer to newly formed tissue; the internal structure was designed as tissue guidance that provides an appropriate microenvironment in connection with native tissue by adjusting pore size and channel structure.
3.2. Components of Bioink for Breast Tissue
Bioink is composed of biomolecules, scaffold materials, and encapsulated cells. Bioink maintains cell viability by protecting encapsulated cells during the printing process and provides a proper microenvironment for cell adhesion, proliferation, and differentiation [74]. The appropriate combination of components provides a mechanical and biological environment for successful tissue engineering. The components of biomaterials (bioink) are divided into two categories: nature-derived biomaterials and synthetic biomaterials.
3.2.1. Nature Derived Biomaterials
Nature-derived biomaterials that can be used for breast tissue regeneration consist of collagen, alginate, chitosan, hyaluronic acid (HA), and decellularized extracellular matrix (dECM) [75]. Alginate and chitosan provide an appropriate microenvironment for adipocytes, including adipose-derived stem cells (ADSCs) by means of cell viability and proliferation, leading to adipogenic differentiation [76,77]. DECM is a hydrophilic matrix extracted from tissues via a decellularization process. The components of dECM contain glycosaminoglycans, proteins, polysaccharides, fibronectin, and collagen type I and II. These components provide a biomimetic microenvironment for cell adhesion, proliferation, and differentiation [78]. Although the dECM of adipose tissue has been shown to promote the formation of adipose tissue of the breast, there remains the limitation that the degradation rate of dECM exceeds the rate of new ECM formation [79,80,81]. Nature-derived components have common limitations such as instability and difficulty in modification, but they provide a biological and chemical microenvironment.
3.2.2. Synthetic Components
Synthetic biomaterials have the capacity to be modified in ways that provide mechanical strength, biodegradability, and cell adhesion ability. Some synthetic components have the property of nature-derived biomaterials that can be included as bioink and some other components act as mechanical support of the 3D bioprinting structure.
The most frequently adopted component is poly e-caprolactone (PCL), which provides mechanical strength with sufficient biocompatibility as a characteristic of the additive supportive structure [82]. In a rodent model study, ADSCs seeded to a PCL scaffold increased angiogenesis and minimized the host inflammatory response, resulting in increased tissue growth and biostructure integration [83]. In another study, a 3D-printed PCL device was attached to the surface of a silicone implant and applied to a rodent model to enhance adipogenic differentiation of ADSCs without foreign body reaction [84]. PCL is often researched as a copolymer with other molecular materials. In one study, a copolymer of e-caprolactone and p-dioxanone supported proliferation and differentiation of ADSCs, which is suitable for tissue regeneration [85]. In other study, copolymer of polycaprolactone-co-poly-D,L-lactic acid (PCLLA) was evaluated as a biomaterial for breast tissue reengineering [86]. Although the initial mechanical property of PCLLA has shown potential as an additive during manufacturing, it has limitations in thermal stability and degradation rates [87].
The exact utility of synthetic biomaterials is uncertain, and research is in progress. However, as shown clinical success in bone tissue engineering, they can be regarded as potentially important 3D bioprinting tools for breast tissue regeneration if harmonized with biologic biomaterials.
3.3. Immunomodulation of 3D Bioprinted Scaffold
Recent advances in 3D-bioprinted silicone implants have proven highly accurate anatomical form for individuals. However, immune reaction-derived complications such as capsular contraction and granuloma formation are still unsolved issues. To overcome this immunologic problem, several immunomodulating trials of the 3D scaffold have been attempted. Indolfi et al. applicated matrix-embedded endothelial cells (MEECs) on 3D porous collagen scaffold. In the study, the decreased recruitment of monocytes and the immunosuppressive properties of the MEECs were proven [88]. In another study performed by Barthes et al., coating cytokines composed of interleukin-10 and prostaglandin-E2 on 3D implant, diminished thickness of the inflammatory tissue and the intensity of acute and chronic inflammation were observed. Moreover, overall fibroblastic reaction and the secretion of pro-inflammatory cytokines also have decreased, resulting in lower potential complication rates [89]. Through modulating such microenvironments of implantable 3D biomaterials based on microscale coating to deliver cytokines, reduced adverse immune reactions and promoted tissue regeneration will be accomplished. To sum up, immunomodulation by 3D scaffold cannot be overlooked for ultimate surgical outcome and should be taken into consideration.
4. Breast Fillers
The augmentation of the breast while avoiding burdensome surgery could be an ideal option for reconstructive or aesthetic purposes. For this reason, multiple filler materials for breast augmentation have been introduced for minimally invasive procedures. Breast augmentation using various injectable materials, including paraffin, mineral oil, liquid silicone, and polyacrylamide hydrogel has been performed for several decades. However, all of these fillers have caused the development of severe complications such as infection, unexpected migration, nodular formation, and pain. Due to its simplicity of use, many local clinics worldwide still use filler materials for breast augmentation even though some countries have banned the use of such fillers. The most commonly used fillers are hydrophilic gel and hyaluronic acid.
4.1. Hydrophilic Gel Fillers
Aquafilling (Biomedica, spol, s.r.o., Czech Republic) is a hydrophilic gel composed of 98% sodium chloride solution (0.9%) and 2% polyimide. It was developed for facial contouring in the Czech Republic in 2005 [90]. Along with Aquafilling, there are several similar products that have been sold under the name of Los Deline (Bio Trh, s.r.o., Pargue, Czech Republic) and Aqualift (National Medical Technologies Center Co., Ltd., Kyiv city, Ukraine), which is similar to a formulation that was first copyrighted in 2013 and then renamed to Activegel in 2015. Shin et al. reported Aquafilling/Los Deline injections to correct mild breast deformity after breast augmentation with silicone implants. However, its safety is still controversial. There have been multiple reports of complications such as breast pain, gel migration, inflammation, infection, and nodular lesions [91,92,93,94,95]. These complications may be derived from the copolyimide. The Korean Academic Society of Aesthetic and Reconstructive Breast Surgery stated in 2016 that the copolyimide in Aquafilling/Los Deline is poly (acrylamide-co-N, N’-methylene-bisacrylamide), meaning copolyimide has the same composition as polyacrylamide gel (PAAG) fillers, which have been reported to cause serious adverse complications when used for breast augmentation (localized lump, deformity, infection, gel migration, inability to breastfeed) [96]. The complications of PAAG has been mentioned in previous reports. Unokovych et al. reported 45 Ukrainian women who underwent surgery from 1998 to 2009 to treat PAAG complications, including pain, breast hardening, deformity, lump, fistula. The average duration from injection to developing the complication was 6.1 years [97]. Nomoto et al. reported that 29 patients who received copolymer-filler injection presented with concerns (deformity, gel migration, infection, induration, pain, and fistula) [98]. The mean duration between injection and consultation was 1.8 years. These findings indicate copolyimide filler injections for breast augmentation are associated with similar complications as the PAAG filler injection. In this study, nuclear magnetic resonance (NMR) analysis indicated that copolyimide and PAAG fillers bore all of the characteristic peaks of PAAG, which was previously mentioned by the Korean Society.
4.2. Hyaluronic Acid Fillers
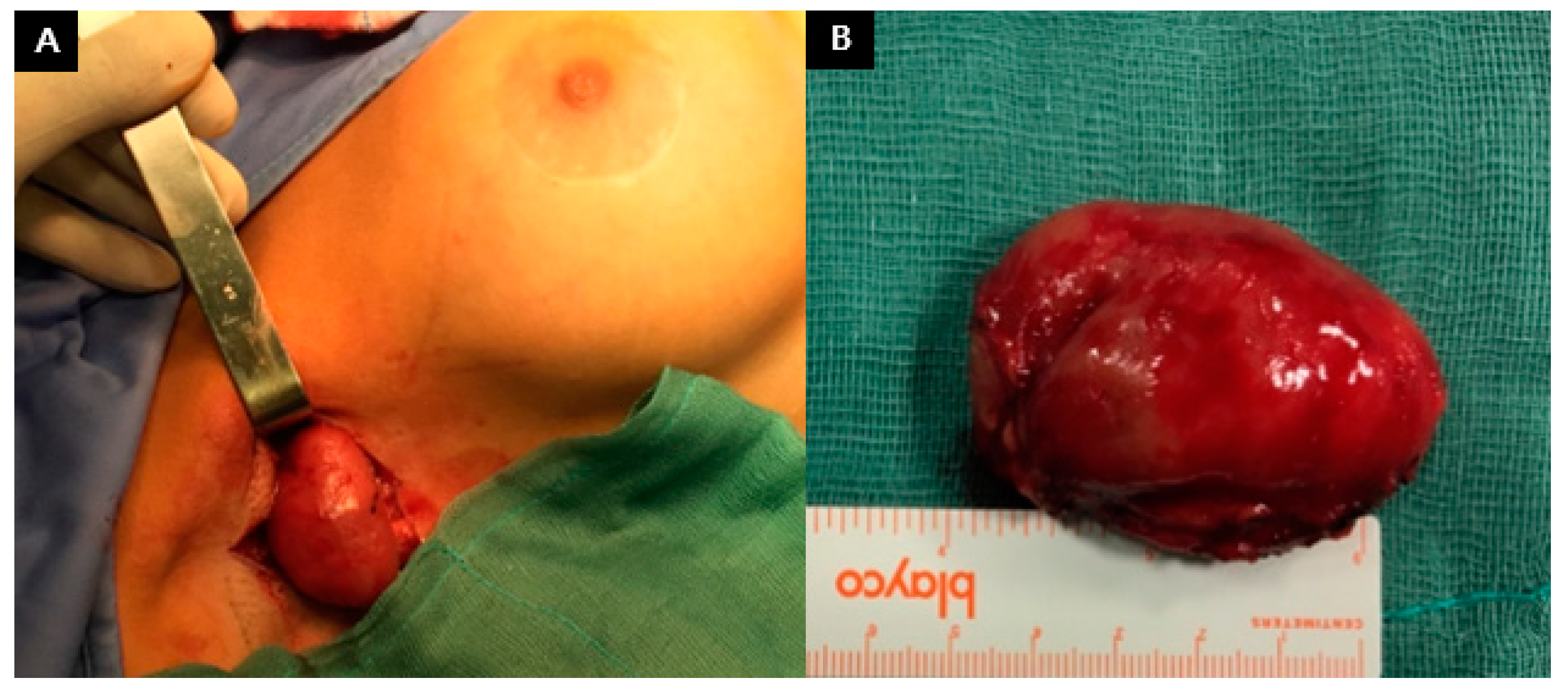
Macrolane (Qmed/Galderma Co) is a NASHA-based (stabilized hyaluronic acid of non-animal origin) medical implant that has been investigated in breast augmentation and buttock augmentation. It plays a role in delivering adipocyte precursor cells and supports adipose tissue formation [99]. Hyaluronic acid has several benefits, such as being noninvasive and reversible, with rapid results. For its simplicity, it attracted much media attention, and many women have undergone this procedure. Untrained aesthetic physicians have spread the HA in the breast instead of placing it deep into the gland, which resulted in mammography errors in the surrounding glandular tissue [100]. Hyaluronic acid filler has the characteristic of high crosslinking, which extends its duration in tissues before its absorption [101]. The degradation of the product is isovolemic, and as the product degrades the remaining hyaluronic acid binds additional water to maintain a constant overall volume [102]. Owing to these characteristics, the duration of the product is limited, and as Macrolane degrades, it can diffuse into the gland and more likely exit the breasts through the lymphatic system [103]. Similar to a previous report, after Macrolane injection into the breast, asymmetrical volume loss with lump formation was noticed. Furthermore, three years after surgery, right axilla lymph node enlargement was noticed, and biopsy showed a high concentration of hyaluronic acid (Figure 5) [104]. Macrolane was finally withdrawn from the market in 2017. After scientific studies of safety and overcoming the cost inefficacy, new hyaluronic fillers may emerge for volume restoration procedures, including breast augmentation.
4.3. Future Perspectives for Breast Fillers
Injectable fillers are widely used in soft tissue augmentation and reconstruction. Injectable materials can be classified as natural or synthetic biomaterials. Natural fillers have the advantage of biocompatibility and degradation over time. However, natural fillers have limitations, such as high absorption rates and a relatively short-lasting filling effect. On the other hand, synthetic fillers tend to have a low biocompatibility with various mechanical strengths. Appropriate filler material could be developed, and current limitations could be eliminated, such as migration, nodule formation, and foreign body reactions through the proper combination of properties of natural and synthetic biomaterials.
5. Conclusions
As the annual number of breast reconstruction and augmentation procedures increases, biomaterials for the breast have overcome multiple clinical obstacles and have gone through an astounding evolution over the last century. Breast implants have undergone a remarkable progression among various biomaterials to achieve more natural, durable, and safe properties for patients. Current promising results in preclinical research reveal that biointegration of the device into the soft tissue is expected to present a solution for unsolved issues such as capsular contracture and foreign body reactions. Moreover, tissue engineering utilizing 3D bioprinting technology will accelerate the emergence of a perfect biomaterial for the breast. Keeping pace with the trend of patients seeking less invasive procedures, safe and long-lasting injection biomaterials are also expected to emerge in the near future.
Author Contributions
J.-H.P.: Writing—original draft and editing; J.-U.P.: Writing—review and editing; H.C.: Supervision. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data sharing not applicable.
Conflicts of Interest
The authors declare no Conflict of Interest.
References
- Saslow, D.; Boetes, C.; Burke, W.; Harms, S.; Leach, M.O.; Lehman, C.D.; Morris, E.; Pisano, E.; Schnall, M.; Sener, S. American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J. Clin. 2007, 57, 75–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Z.; Xu, L.; Shi, W.; Zeng, F.; Zhuo, R.; Hao, X.; Fan, P. Trends of female and male breast cancer incidence at the global, regional, and national levels, 1990–2017. Breast Cancer Res. Treat. 2020, 180, 481–490. [Google Scholar] [CrossRef] [PubMed]
- Allemani, C.; Matsuda, T.; Di Carlo, V.; Harewood, R.; Matz, M.; Nikšić, M.; Bonaventure, A.; Valkov, M.; Johnson, C.J.; Estève, J. Global surveillance of trends in cancer survival 2000–14 (CONCORD-3): Analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet 2018, 391, 1023–1075. [Google Scholar] [CrossRef] [Green Version]
- Fitzmaurice, C.; Abate, D.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdel-Rahman, O.; Abdelalim, A.; Abdoli, A.; Abdollahpour, I.; Abdulle, A.S. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 29 cancer groups, 1990 to 2017: A systematic analysis for the global burden of disease study. JAMA Oncol. 2019, 5, 1749–1768. [Google Scholar] [PubMed] [Green Version]
- Arion, H. Retromammary prosthesis. CR Soc. Fr. Gynecol. 1965, 5, 1–20. [Google Scholar]
- Regnault, P.; Baker, T.J.; Gleason, M.C.; Gordon, H.L.; Grossman, A.R.; Lewis Jr, J.R.; Waters, W.R.; Williams, J.E. Clinical trial and evaluation of a proposed new inflatable mammary prosthesis. Plast. Reconstr. Surg. 1972, 50, 220–226. [Google Scholar] [CrossRef]
- Rees, T.D.; Guy, C.L.; Coburn, R.J.; Rees, T.D. The use of inflatable breast implants. Plast. Reconstr. Surg. 1973, 52, 609–615. [Google Scholar] [CrossRef]
- Young, V.L.; Watson, M.E. Breast implant research: Where we have been, where we are, where we need to go. Clin. Plast. Surg. 2001, 28, 451–483. [Google Scholar] [CrossRef]
- Cronin, T.D.; Brauer, R.O. Augmentation mammaplasty. Surg. Clin. North Am. 1971, 51, 441–452. [Google Scholar] [CrossRef]
- Peters, W.; Smith, D.; Lugowski, S. Failure properties of 352 explanted silicone-gel breast implants. Can. J. Plast. Surg. 1996, 4, 1–8. [Google Scholar] [CrossRef]
- Feng, L.-J.; Amini, S.B. Analysis of risk factors associated with rupture of silicone gel breast implants. Plast. Reconstr. Surg. 1999, 104, 955–963. [Google Scholar] [CrossRef]
- Weum, S.; de Weerd, L.; Kristiansen, B. Form stability of the style 410 anatomically shaped cohesive silicone gel–filled breast implant in subglandular breast augmentation evaluated with magnetic resonance imaging. Plast. Reconstr. Surg. 2011, 127, 409–413. [Google Scholar] [CrossRef]
- Winding, O.; Christensen, L.; Thomsen, J.; Nielsen, M.; Breiting, V.; Brandt, B. Silicon in human breast tissue surrounding silicone gel prostheses: A scanning electron microscopy and energy dispersive X-ray investigation of normal, fibrocystic and peri-prosthetic breast tissue. Scand. J. Plast. Reconstr. Surg. 1988, 22, 127–130. [Google Scholar] [CrossRef]
- Rudolph, R.; Abraham, J.; Vecchione, T.; Guber, S.; Woodward, M. Myofibroblasts and free silicon around breast implants. Plast. Reconstr. Surg. 1978, 62, 185–196. [Google Scholar] [CrossRef] [PubMed]
- Argenta, L.C. Migration of silicone gel into breast parenchyma following mammary prosthesis rupture. Aesthetic Plast. Surg. 1983, 7, 253–254. [Google Scholar] [CrossRef] [PubMed]
- Eisenberg, H.V.; Bartels, R.J. Rupture of a silicone bag-gel breast implant by closed compression capsulotomy: Case report. Plast. Reconstr. Surg. 1977, 59, 849–850. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.; Blackwell, S.J.; Lewis, S.R. Migration of silicone gel after the” squeeze technique” to rupture a contracted breast capsule. Case report. Plast. Reconstr. Surg. 1978, 61, 277–280. [Google Scholar] [CrossRef]
- Thomsen, J.L.; Christensen, L.; Nielsen, M.; Brandt, B.; Breiting, V.B.; Felby, S.; Nielsen, E. Histologic changes and silicone concentrations in human breast tissue surrounding silicone breast prostheses. Plast. Reconstr. Surg. 1990, 85, 38–41. [Google Scholar] [CrossRef]
- Van Nunen, S.A.; Gatenby, P.A.; Basten, A. Post-mammoplasty connective tissue disease. Arthritis Rheum. Off. J. Am. Coll. Rheumatol. 1982, 25, 694–697. [Google Scholar] [CrossRef]
- Spiera, H. Scleroderma after silicone augmentation mammoplasty. JAMA 1988, 260, 236–238. [Google Scholar] [CrossRef]
- Endo, L.P.; Edwards, N.L.; Longley, S.; Corman, L.C.; Panush, R.S. Silicone and Rheumatic Diseases. Semin. Arthritis Rheum. 1987, 17, 112–118. [Google Scholar] [CrossRef]
- Kessler, D.A. The basis of the FDA’s decision on breast implants. N. Engl. J. Med. 1992, 326, 1713–1715. [Google Scholar] [CrossRef]
- Cohen, I.K. Impact of the FDA ban on silicone breast implants. J. Surg. Oncol. 1994, 56, 1. [Google Scholar] [CrossRef] [PubMed]
- Lundberg, G.D. The breast implant controversy: A clash of ethics and law. JAMA 1993, 270, 2608. [Google Scholar] [CrossRef]
- Handel, N.; Wellisch, D.; Silverstein, M.; Jensen, J.A.; Waisman, E. Knowledge, concern, and satisfaction among augmentation mammaplasty patients. Ann. Plast. Surg. 1993, 30, 13–20; discussion 20. [Google Scholar] [CrossRef] [PubMed]
- Stombler, R.E. Breast implants and the FDA: Past, present, and future. Plast. Surg. Nurs. 1993, 13, 185–187. [Google Scholar] [CrossRef] [PubMed]
- Fisher, J.C. The silicone controversy—when will science prevail? N. Engl. J. Med. 1992, 326, 1696–1698. [Google Scholar] [CrossRef] [PubMed]
- Guidoin, R.; Rolland, C.; Fleury, D.; Charara, J.; Marceau, D.; Bronskill, M.; Cardou, A.; King, M.; Lessard, R. Physical characterization of unimplanted gel filled breast implants. Should old standards be revisited? ASAIO J. Am. Soc. Artif. Intern. Organs 1994, 40, 943–958. [Google Scholar] [CrossRef]
- Cunningham, B. The Mentor study on contour profile gel silicone MemoryGel breast implants. Plast. Reconstr. Surg. 2007, 120, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Maxwell, G.P.; Van Natta, B.W.; Murphy, D.K.; Slicton, A.; Bengtson, B.P. Natrelle style 410 form-stable silicone breast implants: Core study results at 6 years. Aesthet. Surg. J. 2012, 32, 709–717. [Google Scholar] [CrossRef] [Green Version]
- Stevens, W.G.; Harrington, J.; Alizadeh, K.; Berger, L.; Broadway, D.; Hester, T.R.; Kress, D.; d’Incelli, R.; Kuhne, J.; Beckstrand, M. Five-year follow-up data from the US clinical trial for Sientra’s US Food and Drug Administration–approved Silimed® brand round and shaped implants with high-strength silicone gel. Plast. Reconstr. Surg. 2012, 130, 973–981. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coleman, D.J.; Foo, I.T.; Sharpe, D.T. Textured or smooth implants for breast augmentation? A prospective controlled trial. Br. J. Plast. Surg. 1991, 44, 444–448. [Google Scholar] [CrossRef]
- Calobrace, M.B.; Stevens, W.G.; Capizzi, P.J.; Cohen, R.; Godinez, T.; Beckstrand, M. Risk factor analysis for capsular contracture: A 10-year Sientra study using round, smooth, and textured implants for breast augmentation. Plast. Reconstr. Surg. 2018, 141, 20S–28S. [Google Scholar] [CrossRef]
- Wong, C.-H.; Samuel, M.; Tan, B.-K.; Song, C. Capsular contracture in subglandular breast augmentation with textured versus smooth breast implants: A systematic review. Plast. Reconstr. Surg. 2006, 118, 1224–1236. [Google Scholar] [CrossRef]
- Stevens, W.G.; Nahabedian, M.Y.; Calobrace, M.B.; Harrington, J.L.; Capizzi, P.J.; Cohen, R.; d’Incelli, R.C.; Beckstrand, M. Risk factor analysis for capsular contracture: A 5-year Sientra study analysis using round, smooth, and textured implants for breast augmentation. Plast. Reconstr. Surg. 2013, 132, 1115–1123. [Google Scholar] [CrossRef]
- Brohim, R.M.; Foresman, P.A.; Hildebrandt, P.K.; Rodeheaver, G.T. Early tissue reaction to textured breast implant surfaces. Ann. Plast. Surg. 1992, 28, 354–362. [Google Scholar] [CrossRef] [PubMed]
- Abramo, A.C.; De Oliveira, V.R.; Ledo-Silva, M.C.; De Oliveira, E.L. How texture-inducing contraction vectors affect the fibrous capsule shrinkage around breasts implants? Aesthetic Plast. Surg. 2010, 34, 555–560. [Google Scholar] [CrossRef]
- Handel, N.; Jensen, J.A.; Black, Q.; Waisman, J.R.; Silverstein, M.J. The fate of breast implants: A critical analysis of complications and outcomes. Plast. Reconstr. Surg. 1995, 96, 1521–1533. [Google Scholar] [CrossRef] [PubMed]
- Barone, F.E.; Perry, L.; Keller, T.; Maxwell, G.P. The biomechanical and histopathologic effects of surface texturing with silicone and polyurethane in tissue implantation and expansion. Plast. Reconstr. Surg. 1992, 90, 77–86. [Google Scholar] [CrossRef]
- Handel, N.; Silverstein, M.J.; Jensen, J.A.; Collins, A.; Zierk, K. Comparative experience with smooth and polyurethane breast implants using the Kaplan-Meier method of survival analysis. Plast. Reconstr. Surg. 1991, 88, 475–481. [Google Scholar] [CrossRef]
- Vazquez, G.; Pellon, A. Polyurethane-coated silicone gel breast implants used for 18 years. Aesthetic Plast. Surg. 2007, 31, 330–336. [Google Scholar] [CrossRef]
- Handel, N.; Gutierrez, J. Long-term safety and efficacy of polyurethane foam-covered breast implants. Aesthet. Surg. J. 2006, 26, 265–274. [Google Scholar] [CrossRef]
- de la Peña-Salcedo, J.A.; Soto-Miranda, M.A.; Lopez-Salguero, J.F. Back to the future: A 15-year experience with polyurethane foam-covered breast implants using the partial-subfascial technique. Aesthetic Plast. Surg. 2012, 36, 331–338. [Google Scholar] [CrossRef]
- Duxbury, P.J.; Harvey, J.R. Systematic review of the effectiveness of polyurethane-coated compared with textured silicone implants in breast surgery. J. Plast. Reconstr. Aesthetic Surg. 2016, 69, 452–460. [Google Scholar] [CrossRef] [PubMed]
- Hakelius, L.; Ohlsén, L. A clinical comparison of the tendency to capsular contracture between smooth and textured gel-filled silicone mammary implants. Plast. Reconstr. Surg. 1992, 90, 247–254. [Google Scholar] [CrossRef]
- Ersek, R.A. Rate and incidence of capsular contracture: A comparison of smooth and textured silicone double-lumen breast prostheses. Plast. Reconstr. Surg. 1991, 87, 879–884. [Google Scholar] [CrossRef]
- Collis, N.; Coleman, D.; Foo, I.T.; Sharpe, D.T. Ten-year review of a prospective randomized controlled trial of textured versus smooth subglandular silicone gel breast implants. Plast. Reconstr. Surg. 2000, 106, 786–791. [Google Scholar] [CrossRef] [PubMed]
- Gallo, J.; Holinka, M.; Moucha, C.S. Antibacterial Surface Treatment for Orthopaedic Implants. Int. J. Mol. Sci. 2014, 15, 13849–13880. [Google Scholar] [CrossRef] [Green Version]
- Barr, S.; Hill, E.; Bayat, A. Current implant surface technology: An examination of their nanostructure and their influence on fibroblast alignment and biocompatibility. Eplasty 2009, 9, e22. [Google Scholar] [PubMed]
- Sforza, M.; Zaccheddu, R.; Alleruzzo, A.; Seno, A.; Mileto, D.; Paganelli, A.; Sulaiman, H.; Payne, M.; Maurovich-Horvat, L. Preliminary 3-year evaluation of experience with SilkSurface and VelvetSurface motiva silicone breast implants: A single-center experience with 5813 consecutive breast augmentation cases. Aesthet. Surg. J. 2018, 38, S62–S73. [Google Scholar] [CrossRef] [PubMed]
- Ham, J.; Kim, Y.; An, T.; Kang, S.; Ha, C.; Wufue, M.; Kim, Y.; Jeon, B.; Kim, S.; Kim, J.; et al. Covalently grafted 2-methacryloyloxyethyl phosphorylcholine networks inhibit fibrous capsule formation around silicone breast implants in a porcine model. ACS Appl. Mater. Interfaces 2020, 12, 30198–30212. [Google Scholar] [CrossRef]
- Barnea, Y.; Hammond, D.C.; Geffen, Y.; Navon-Venezia, S.; Goldberg, K. Plasma activation of a breast implant shell in conjunction with antibacterial irrigants enhances antibacterial activity. Aesthet. Surg. J. 2018, 38, 1188–1196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruff, E.S.; Hirase, T.; Rude, M.J. Evaluation of antibiotic-impregnated mesh in preventing the recurrence of capsular contracture. Aesthet. Surg. J. 2019, 39, 509–515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asplund, O. Capsular contracture in silicone gel and saline-filled breast implants after reconstruction. Plast. Reconstr. Surg. 1984, 73, 270–275. [Google Scholar] [CrossRef]
- Gylbert, L.; Asplund, O.; Jurell, G. Capsular contracture after breast reconstruction with silicone-gel and saline-filled implants: A 6-year follow-up. Plast. Reconstr. Surg. 1990, 85, 373–377. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, B. The Mentor Core Study on Silicone MemoryGel Breast Implants. Plast. Reconstr. Surg. 2007, 120, 19S–29S. [Google Scholar] [CrossRef]
- Spear, S.L.; Heden, P. Allergan’s silicone gel breast implants. Expert Rev. Med. Devices 2007, 4, 699–708. [Google Scholar] [CrossRef]
- Kaoutzanis, C.; Winocour, J.; Unger, J.; Gabriel, A.; Maxwell, G.P. The evolution of breast implants. Semin. Plast. Surg. 2019, 33, 217–223. [Google Scholar] [CrossRef] [Green Version]
- Brody, G.S. Silicone technology for the plastic surgeon. Clin. Plast. Surg. 1988, 15, 517–520. [Google Scholar] [CrossRef]
- Stevens, W.G.; Pacella, S.J.; Gear, A.J.; Freeman, M.E.; McWhorter, C.; Tenenbaum, M.J.; Stoker, D.A. Clinical experience with a fourth-generation textured silicone gel breast implant: A review of 1012 Mentor MemoryGel breast implants. Aesthet. Surg. J. 2008, 28, 642–647. [Google Scholar] [CrossRef] [Green Version]
- Srinivasa, D.R.; Miranda, R.N.; Kaura, A.; Francis, A.M.; Campanale, A.; Boldrini, R.; Alexander, J.; Deva, A.K.; Gravina, P.R.; Medeiros, L.J.; et al. Global adverse event reports of breast implant-associated ALCL: An international review of 40 government authority databases. Plast. Reconstr. Surg. 2017, 139, 1029–1039. [Google Scholar] [CrossRef]
- McGuire, P.; Reisman, N.R.; Murphy, D.K. Risk Factor Analysis for Capsular Contracture, Malposition, and Late Seroma in Subjects Receiving Natrelle 410 Form-Stable Silicone Breast Implants. Plast. Reconstr. Surg. 2017, 139, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Breast Implants: Update on TGA Monitoring of Anaplastic Large Cell Lymphoma. Available online: https://www.tga.gov.au/alert/breast-implants-update-tga-monitoring-anaplastic-large-cell-lymphoma (accessed on 27 September 2016).
- The FDA Requests Allergan Voluntarily Recall Natrelle BIOCELL Textured Breast Implants and Tissue Expanders from the Market to Protect Patients: FDA Safety Communication. Available online: https://www.fda.gov/medical-devices/safety-communications/fdarequests-allergan-voluntarily-recall-natrelle-biocell-texturedbreast-implants-and-tissue (accessed on 1 July 2021).
- FDA Takes Action to Protect Patients from Risk of Certain Textured Breast Implants; Requests Allergan Voluntarily Recall Certain Breast Implants and Tissue Expanders from Market. Available online: https://www.fda.gov/news-events/press-announcements/fda-takesaction-protect-patients-risk-certain-textured-breast-implantsrequests-allergan (accessed on 1 July 2021).
- Clemens, M.W.; Medeiros, L.J.; Butler, C.E.; Hunt, K.K.; Fanale, M.A.; Horwitz, S.; Weisenburger, D.D.; Liu, J.; Morgan, E.A.; Kanagal-Shamanna, R.; et al. Complete surgical excision is essential for the management of patients with breast implant-associated anaplastic large-cell lymphoma. J. Clin. Oncol. 2016, 34, 160–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Comprehensive Cancer Network (NCCN). Available online: https://www.nccn.org/professionals/physician_gls/pdf/t-cell.pdf (accessed on 1 July 2021).
- Nelson, J.A.; McCarthy, C.; Dabic, S.; Polanco, T.; Chilov, M.; Mehrara, B.J.; Disa, J.J. BIA-ALCL and textured breast implants: A systematic review of evidence supporting surgical risk management strategies. Plast. Reconstr. Surg. 2021, 147, 7S–13S. [Google Scholar] [CrossRef] [PubMed]
- Carr, L.W.; Roberts, J.; Potochny, J.D. How breast implant surface type is influenced by breast implant-associated anaplastic large cell lymphoma: A survey of the American Society of Plastic Surgeons. Ann. Plast. Surg. 2019, 82, S208–S211. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Liu, Y.; Zhang, J.; Liu, H.; Wang, J.; Liu, Q.; Zhang, Y. Three-dimensional bioprinting adipose tissue and mammary Organoids feasible for artificial breast structure regeneration. Mater. Des. 2021, 200, 109467. [Google Scholar] [CrossRef]
- Yilmaz, B.; Tahmasebifar, A.; Baran, E.T. Bioprinting technologies in tissue engineering. Adv. Biochem. Eng. Biotechnol. 2020, 171, 279–319. [Google Scholar]
- Chhaya, M.P.; Balmayor, E.R.; Hutmacher, D.W.; Schantz, J.T. Transformation of breast reconstruction via additive biomanufacturing. Sci. Rep. 2016, 6, 28030. [Google Scholar] [CrossRef] [Green Version]
- Mohseni, M.; Bas, O.; Castro, N.J.; Schmutz, B.; Hutmacher, D.W. Additive biomanufacturing of scaffolds for breast reconstruction. Addit. Manuf. 2019, 30, 100845. [Google Scholar] [CrossRef]
- Hospodiuk, M.; Dey, M.; Sosnoski, D.; Ozbolat, I.T. The bioink: A comprehensive review on bioprintable materials. Biotechnol. Adv. 2017, 35, 217–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Unagolla, J.M.; Jayasuriya, A.C. Hydrogel-based 3D bioprinting: A comprehensive review on cell-laden hydrogels, bioink formulations, and future perspectives. Appl. Mater. Today 2020, 18, 100479. [Google Scholar] [CrossRef] [PubMed]
- Khanmohammadi, M.; Nemati, S.; Ai, J.; Khademi, F. Multipotency expression of human adipose stem cells in filament-like alginate and gelatin derivative hydrogel fabricated through visible light-initiated crosslinking. Mater. Sci. Eng. C Mater. Biol. Appl. 2019, 103, 109808. [Google Scholar] [CrossRef]
- Cheung, H.K.; Han, T.T.; Marecak, D.M.; Watkins, J.F.; Amsden, B.G.; Flynn, L.E. Composite hydrogel scaffolds incorporating decellularized adipose tissue for soft tissue engineering with adipose-derived stem cells. Biomaterials 2014, 35, 1914–1923. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.S.; Das, S.; Jang, J.; Cho, D.W. Decellularized extracellular matrix-based bioinks for engineering tissue- and organ-specific microenvironments. Chem. Rev. 2020, 120, 10608–10661. [Google Scholar] [CrossRef]
- Haddad, S.M.; Omidi, E.; Flynn, L.E.; Samani, A. Comparative biomechanical study of using decellularized human adipose tissues for post-mastectomy and post-lumpectomy breast reconstruction. J. Mech. Behav. Biomed. Mater. 2016, 57, 235–245. [Google Scholar] [CrossRef] [PubMed]
- Eichler, C.; Schulz, C.; Vogt, N.; Warm, M. The use of acellular dermal matrices (ADM) in breast reconstruction: A review. Surg. Technol. Int. 2017, 31, 53–60. [Google Scholar] [PubMed]
- Kabirian, F.; Mozafari, M. Decellularized ECM-derived bioinks: Prospects for the future. Methods 2020, 171, 108–118. [Google Scholar] [CrossRef]
- Chae, M.P.; Hunter-Smith, D.J.; Murphy, S.V.; Findlay, M.W. 3D bioprinting adipose tissue for breast reconstruction. In 3D Bioprinting for Reconstructive Surgery; Thomas, D.J., Jessop, Z.M., Whitaker, I.S., Eds.; Academic Press: London, UK, 2017; pp. 305–353. [Google Scholar]
- Carrow, J.K.; Kerativitayanan, P.; Jaiswal, M.K.; Lokhande, G.; Gaharwar, A. Polymers for Bioprinting. In Essentials of 3D Biofabrication and Translation; Atala, A., Yoo, J.J., Eds.; Academic Press: Boston, MA, USA, 2015; pp. 229–248. [Google Scholar]
- Naderi, N.; Griffin, M.F.; Mosahebi, A.; Butler, P.E.; Seifalian, A.M. Adipose derived stem cells and platelet rich plasma improve the tissue integration and angiogenesis of biodegradable scaffolds for soft tissue regeneration. Mol. Biol. Rep. 2020, 47, 2005–2013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baek, W.; Kim, M.S.; Park, D.B.; Joo, O.Y.; Lee, W.J.; Roh, T.S.; Sung, H.J. Three-dimensionally printed breast reconstruction devices facilitate nanostructure surface-guided healthy lipogenesis. ACS Biomater. Sci. Eng. 2019, 5, 4962–4969. [Google Scholar] [CrossRef]
- Fuoco, T.; Ahlinder, A.; Jain, S.; Mustafa, K.; Finne-Wistrand, A. Poly(ε-caprolactone-co-p-dioxanone): A degradable and printable copolymer for pliable 3d scaffolds fabrication toward adipose tissue regeneration. Biomacromolecules 2020, 21, 188–198. [Google Scholar] [CrossRef]
- Poh, P.S.; Hege, C.; Chhaya, M.P.; Balmayor, E.R.; Foehr, P.; Burgkart, R.H.; Schantz, J.-T.; Schiller, S.M.; Schilling, A.F.; Hutmacher, D.W. Evaluation of polycaprolactone − poly-D, L-lactide copolymer as biomaterial for breast tissue engineering. Polym. Int. 2017, 66, 77–84. [Google Scholar] [CrossRef]
- Indolfi, L.; Baker, A.B.; Edelman, E.R. The role of scaffold microarchitecture in engineering endothelial cell immunomodulation. Biomaterials 2012, 33, 7019–7027. [Google Scholar] [CrossRef] [PubMed]
- Barthes, J.; Lagarrigue, P.; Riabov, V.; Lutzweiler, G.; Kirsch, J.; Muller, C.; Courtial, E.-J.; Marquette, C.; Projetti, F.; Kzhyskowska, J. Biofunctionalization of 3D-printed silicone implants with immunomodulatory hydrogels for controlling the innate immune response: An in vivo model of tracheal defect repair. Biomaterials 2021, 268, 120549. [Google Scholar] [CrossRef]
- Ozcan, U.A.; Ulus, S.; Kucukcelebi, A. Breast augmentation with Aquafilling: Complications and radiologic features of two cases. Eur. J. Plast. Surg. 2019, 42, 405–408. [Google Scholar] [CrossRef]
- Son, M.J.; Ko, K.H.; Jung, H.K.; Koh, J.E.; Park, A.Y. Complications and radiologic features of breast augmentation via injection of aquafilling gel. J. Ultrasound Med. 2018, 37, 1835–1839. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Chang, H.; Park, J.U. Complication of ruptured poly implant prothèse breast implants combined with aquafilling gel injection: A case report and literature review. Aesthetic Plast. Surg. 2019, 43, 46–52. [Google Scholar] [CrossRef]
- Jung, B.K.; Yun, I.S.; Kim, Y.S.; Roh, T.S. Complication of AQUAfilling gel injection for breast augmentation: Case report of one case and review of literature. Aesthetic Plast. Surg. 2018, 42, 1252–1256. [Google Scholar] [CrossRef] [PubMed]
- Hee Ko, K.; Kyoung Jung, H.; Young Park, A. Radiologic features of distant filler migration with inflammatory reaction following augmentation mammoplasty using aquafilling® filler. Iran J. Radiol. 2017, 14, e63468. [Google Scholar] [CrossRef] [Green Version]
- Ikizceli, T.; Cindemir, E.; Gulsen, G.; Bijan, B. Imaging findings of aquafilling gel injection for breast augmentation. Breast J. 2020, 26, 278–280. [Google Scholar] [CrossRef]
- Roh, T.S. Letter: Position Statement of Korean Academic Society of Aesthetic and Reconstructive Breast Surgery: Concerning the Use of Aquafilling(R) for Breast Augmentation. Arch. Aesthetic Plast. Surg. 2016, 22, 45–46. [Google Scholar] [CrossRef]
- Unukovych, D.; Khrapach, V.; Wickman, M.; Liljegren, A.; Mishalov, V.; Patlazhan, G.; Sandelin, K. Polyacrylamide gel injections for breast augmentation: Management of complications in 106 patients, a multicenter study. World J. Surg. 2012, 36, 695–701. [Google Scholar] [CrossRef]
- Nomoto, S.; Hirakawa, K.; Ogawa, R. Safety of copolyamide filler injection for breast augmentation. Plast. Reconstr. Surg. Glob. Open 2021, 9, e3296. [Google Scholar] [CrossRef]
- Von Heimburg, D.; Zachariah, S.; Low, A.; Pallua, N. Influence of different biodegradable carriers on the in vivo behavior of human adipose precursor cells. Plast. Reconstr. Surg. 2001, 108, 411–420; discussion 421–422. [Google Scholar] [CrossRef] [PubMed]
- Hedén, P. Update on body shaping and volume restoration: The role of hyaluronic acid. Aesthetic Plast. Surg. 2020, 44, 1295–1299. [Google Scholar] [CrossRef] [PubMed]
- Chaput, B.; De Bonnecaze, G.; Chavoin, J.P.; Gangloff, D.; Garrido, I. France prohibits the use of macrolane in aesthetic breast augmentation for reasons similar to criticisms of autologous fat grafting to the breast. Aesthetic Plast. Surg. 2012, 36, 1000–1001. [Google Scholar] [CrossRef] [PubMed]
- Sue, G.R.; Seither, J.G.; Nguyen, D.H. Use of hyaluronic acid filler for enhancement of nipple projection following breast reconstruction: An easy and effective technique. JPRAS Open 2020, 23, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Hedén, P.; Olenius, M.; Tengvar, M. Macrolane for breast enhancement: 12-month follow-up. Plast. Reconstr. Surg. 2011, 127, 850–860. [Google Scholar] [CrossRef]
- Trignano, E.; Baccari, M.; Pili, N.; Serra, P.L.; Rubino, C. Complications after breast augmentation with hyaluronic acid: A case report. Gland Surg. 2020, 9, 2193–2197. [Google Scholar] [CrossRef]
Figure 1.
The Cronin–Gerow silicone implant had anatomic shape, smooth surface, and posteriorly placed Dacron patches to maintain position. Based on [9].
Figure 1.
The Cronin–Gerow silicone implant had anatomic shape, smooth surface, and posteriorly placed Dacron patches to maintain position. Based on [9].

Figure 2.
The mechanism of bacterial attachment to the implant surface. Based on [48].
Figure 2.
The mechanism of bacterial attachment to the implant surface. Based on [48].

Figure 3.
Scanning electron microscopy (SEM) images of implant surface. (A) Sientra Silimed foam textured implant surface (66× magnification); (B) Allergan Biocell salt-loss textured implant surface (104× magnification); (C) Mentor Siltex imprinted textured implant surface (100× magnification); (D) Motiva SilkSurface textured implant surface (300 µm scale). Based on [49,50].
Figure 3.
Scanning electron microscopy (SEM) images of implant surface. (A) Sientra Silimed foam textured implant surface (66× magnification); (B) Allergan Biocell salt-loss textured implant surface (104× magnification); (C) Mentor Siltex imprinted textured implant surface (100× magnification); (D) Motiva SilkSurface textured implant surface (300 µm scale). Based on [49,50].

Figure 4.
Reconstruction of breast with a personalized three-dimensional (3D) bioprinted adipose tissue construct using stem cells derived from autologous tissue. Based on [70].
Figure 4.
Reconstruction of breast with a personalized three-dimensional (3D) bioprinted adipose tissue construct using stem cells derived from autologous tissue. Based on [70].

Figure 5.
A case of hyaluronic acid filler migration: (A) migration of Macrolane filler from breast to axilla, 3 years after injection; (B) axillary Macrolane lump. Based on [102].
Figure 5.
A case of hyaluronic acid filler migration: (A) migration of Macrolane filler from breast to axilla, 3 years after injection; (B) axillary Macrolane lump. Based on [102].

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Park, J.-H.; Park, J.-U.; Chang, H. Advances in Biomaterials for Breast Reconstruction. Appl. Sci. 2021, 11, 7493. https://0-doi-org.brum.beds.ac.uk/10.3390/app11167493
AMA Style
Park J-H, Park J-U, Chang H. Advances in Biomaterials for Breast Reconstruction. Applied Sciences. 2021; 11(16):7493. https://0-doi-org.brum.beds.ac.uk/10.3390/app11167493
Chicago/Turabian StylePark, Jun-Ho, Ji-Ung Park, and Hak Chang. 2021. "Advances in Biomaterials for Breast Reconstruction" Applied Sciences 11, no. 16: 7493. https://0-doi-org.brum.beds.ac.uk/10.3390/app11167493
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.