
Chronic Periodontitis and Acute Respiratory Infections: A Nationwide Cohort Study


Department of Periodontology, Daejeon Dental Hospital, Institute of Wonkwang Dental Research, Wonkwang University College of Dentistry, Daejeon 35233, Korea
*
Author to whom correspondence should be addressed.
Appl. Sci. 2021, 11(20), 9493; https://0-doi-org.brum.beds.ac.uk/10.3390/app11209493
Submission received: 13 September 2021
/
Revised: 30 September 2021
/
Accepted: 11 October 2021
/
Published: 13 October 2021
(This article belongs to the Special Issue Oral and Systemic Implications of Periodontal Disease – an Integrated Approach)
Abstract
:Chronic periodontitis (CP) may increase the risk of exacerbation of and hospitalization for respiratory infections. The aim of the present study was to determine whether CP is associated with acute respiratory infections by analyzing a population-based longitudinal database from the National Health Insurance Service—National Sample Cohort. Univariate and multivariate logistic regression analyses were conducted to assess the association between CP and acute respiratory infections, including acute nasopharyngitis, acute pharyngitis, acute tonsillitis, acute laryngitis and tracheitis, acute bronchitis, and acute bronchiolitis, while adjusting for the confounding effects of sociodemographic variables (sex, age, household income, and smoking status) and comorbidities (diabetes mellitus). Among 545,416 recruited participants, 98,490 (18.1%) had CP. Multivariate analysis, adjusted for sociodemographic variables and comorbidities, showed that except influenza and pneumonia, total acute respiratory infections (odds ratio (OR), 1.33; 95% confidence interval (CI), 1.28–1.38; p < 0.001), acute upper respiratory infections (OR, 1.26; 95% CI, 1.22–1.29; p < 0.001), and acute lower respiratory infections (OR, 1.23; 95% CI, 1.20–1.26; p < 0.001) were significantly associated with CP. The findings of the current cohort study suggest an association between CP and acute respiratory infections. Particularly, CP seems to increase the risk of acute upper and lower respiratory infections.
1. Introduction
Chronic periodontitis (CP) is one of the most common chronic inflammatory diseases. Severe localized or generalized CP affects >10% of the global population and is a major public oral health problem [1,2]. CP progressively and pathologically destroys the tooth-supporting soft and hard tissues, including the cementum, periodontal ligament, and alveolar bone, and may ultimately cause tooth loss [3]. Although previous epidemiologic and cohort studies have suggested that CP is a unidirectional risk factor for lifestyle-related non-communicable diseases, such as cardiovascular disease, hypertension, diabetes mellitus, rheumatoid arthritis, osteoporosis, erectile dysfunction, and cancer, there is increasing evidence indicating that the association between CP and major systemic diseases is bidirectional [4,5,6,7].
Several epidemiologic and etiologic studies have suggested a potential association between CP and acute and chronic respiratory infections such as pneumonia, acute bronchitis, lung abscess, and chronic obstructive pulmonary disease [8,9]. Moreover, previous systematic reviews have confirmed a positive causal association between CP and respiratory infections [10,11].
Accumulation of oral pathogens, especially Fusobacterium nucleatum, associated with CP may increase the risk of exacerbation and hospitalization in patients with respiratory infections [8]. These infections possibly share the direct bacterial-respiratory pathway and the same proinflammatory cytokines or products, such as tumor necrosis factor-α (TNF-α), interleukin (IL)-1, IL-6, and IL-8 [12]. Major immunoinflammatory cells and inflammatory mediators from the mucosal epithelial cells of the upper and lower respiratory tract make the respiratory tract more susceptible to infection and development of severe respiratory disease [12].
While research on the association between CP and chronic respiratory infections, particularly chronic obstructive pulmonary disease, has steadily progressed over recent decades, relevant studies between CP and acute respiratory infections are scarce and scattered [13,14]. Consequently, the epidemiological association between CP and acute respiratory infections remains unclear and requires further research. Therefore, the goal of the present study was to evaluate the associations between CP and acute respiratory infections by analyzing a population-based longitudinal database from the National Health Insurance Service—National Sample Cohort (NHIS-NSC) in South Korea.
2. Materials and Methods
2.1. Study Design and Data Source
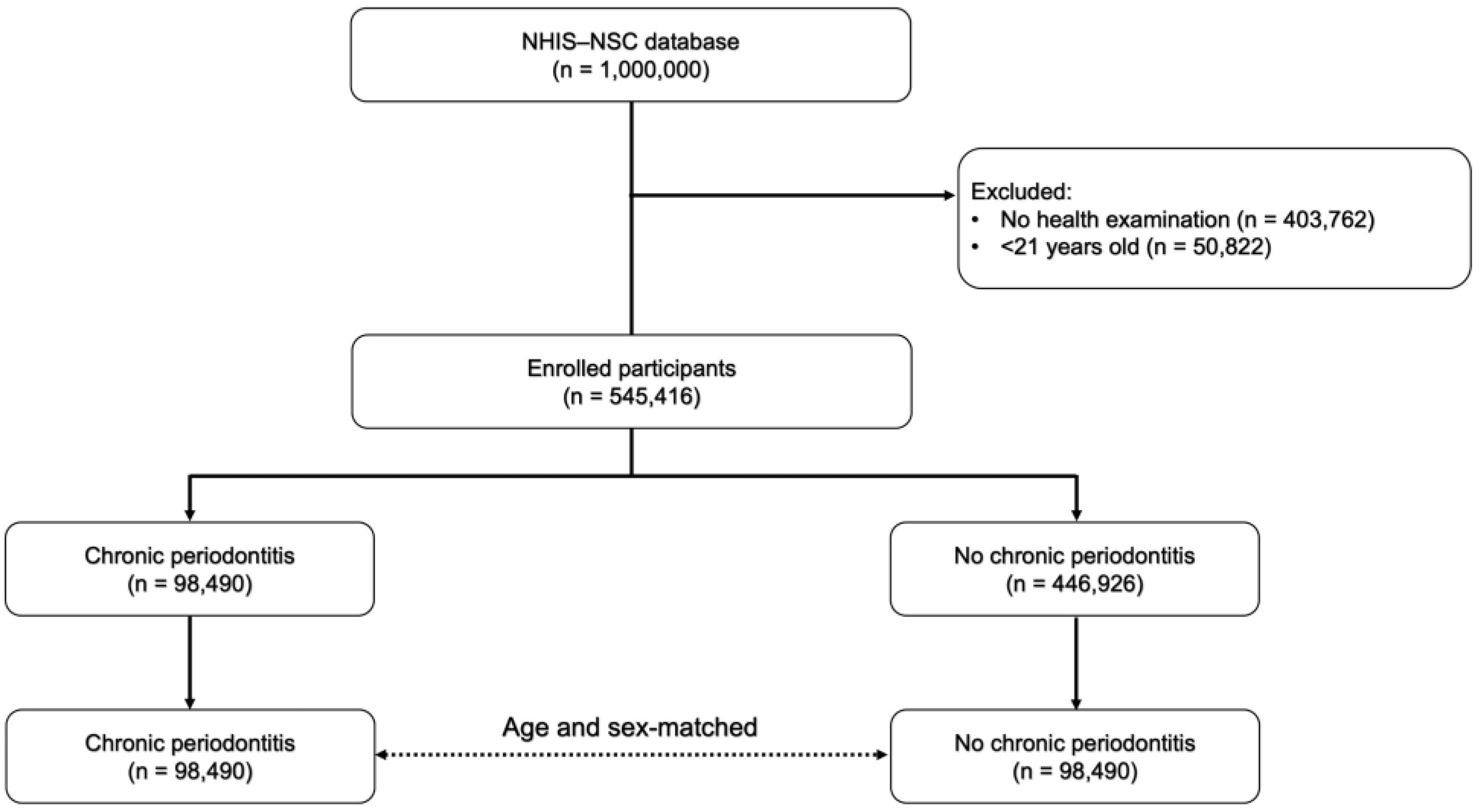
This study used the longitudinal NHIS-NSC database compiled by the National Health Insurance Sharing Service. Data for 1,000,000 individuals, representing 2% of the 48.22 million Korean nationals whose data are maintained in the national health insurance service (NHIS) or medical aid program (MAP) since 2006, were extracted through a multistage stratified sampling method (2142 layers) to ensure similar characteristics in terms of sex (two groups: male and female), age (17 groups: 1–79 years in 5-year intervals and >80 years), region of residence (3 groups: metropolitan, urban, and rural areas), and household income level (21 groups: NHIS in 20 groups and MAP in 1 group). All personal and sensitive information was de-identified prior to the analysis. Among the participants included in the NHIS-NSC database, only adults over 20 years of age who had undergone a routine health examination under the NHIS between 2006 and 2015 were included in this study. A detailed flowchart of the inclusion and exclusion of the participants is shown in Figure 1.
This study conformed to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines and followed the guidelines of the Declaration of Helsinki of 1975, as revised in 2013. The protocol was approved by the Institutional Review Board of Daejeon Dental Hospital, Wonkwang University (Approval No. W2107/001-001), and the requirement for written consent was waived because of the retrospective nature of this study.
2.2. Study Variables and Definitions
Similar to our previous studies, the definition of CP was limited to those who were diagnosed with CP (Korean Classification of Diseases, sixth revision [KCD-6], code K05.3, corresponding to the International Classification of Disease, 10th revision [ICD-10], code K05.3), and received one or more of the following prescription codes for periodontal surgery: U1051-1052, simple or complicated periodontal flap operation; U1071-1072, autograft, allogenic, xenogeneic, or substitute bone graft for alveolar bone defects; U1081-1083, guided tissue regeneration with or without bone graft [15,16].
Using medical records from 2006 to 2015, participants who were diagnosed with acute respiratory infections by a medical doctor at a private or general hospital using the following diagnostic codes: acute nasopharyngitis (KCD-6/ICD-10 code J01), acute pharyngitis (KCD-6/ICD-10 code J02), acute tonsillitis (KCD-6/ICD-10 code J03), acute laryngitis and tracheitis (KCD-6/ICD-10 code J04), influenza (KCD-6/ICD-10 codes J09–J12), pneumonia (KCD-6/ICD-10 codes J13–18), acute bronchitis (KCD-6/ICD-10 codes J20), and acute bronchiolitis (KCD-6/ICD-10 codes J21), were included in this cohort study.
Patients were categorized into subgroups based on sociodemographic variables and comorbidities, including sex, (2 groups: male and female), age (5 groups: 21–60 years in 5-year intervals and ≥61 years), household income level (5 groups: NHIS in 5 groups, with those in the MAP in the first quintile), smoking status, and diabetes mellitus (KCD-6/ICD-10 codes E10–֪E14).
2.3. Statistical Analysis
Descriptive statistics were used for sociodemographic variables and comorbidities of participants, and categorical parameters were expressed as numbers and percentages. In this retrospective cohort study, we used the chi-square test to compare patients with CP with and without acute respiratory infections. Univariate (model 1) and multivariate (models 2–4) logistic regression analyses were performed to evaluate the crude and adjusted associations between CP and acute respiratory infections. The odds ratios (ORs) are presented with 95% confidence intervals (CIs), and statistical significance was set at p < 0.05. All statistical analyses were performed using SAS version 9.3 (SAS Institute, Cary, NC, USA).
3. Results
3.1. Distribution According to CP
The prevalence of CP in the study participants is shown in Table 1. The percentages of men aged 41–50 years in the CP and non-CP groups were 54.5% and 32.3%, respectively. In the CP group, 28,588 (29.0%) individuals were in the fifth quintile of household income, 33,402 (33.9%) were current smokers, and 25,870 (26.3%) had diabetes mellitus; these values were significantly different from those in the non-CP group (p < 0.001). The prevalence of acute upper and lower respiratory infections in patients with CP was 89.6% and 81.1%, respectively, which was significantly higher than that in patients without CP (p < 0.001).
3.2. Distribution According to Acute Respiratory Infections
The percentages of participants who were male, aged 41–50 years, and in the fifth quintile of household income among all patients with acute respiratory infections were 53.0%, 31.9%, and 28.2%, respectively. Among patients with acute respiratory infections, 58,448 (31.8%) were current smokers, and 46,219 (25.1%) had diabetes mellitus; these values were significantly different from those among patients without acute respiratory infection (p < 0.001). Lastly, among all patients with acute respiratory infection, 92,867 (50.5%) had CP, which was significantly higher than that in patients without acute respiratory infections (p < 0.001). The prevalence of acute respiratory infections among the study participants is shown in Table 2.
3.3. CP and Acute Respiratory Infections
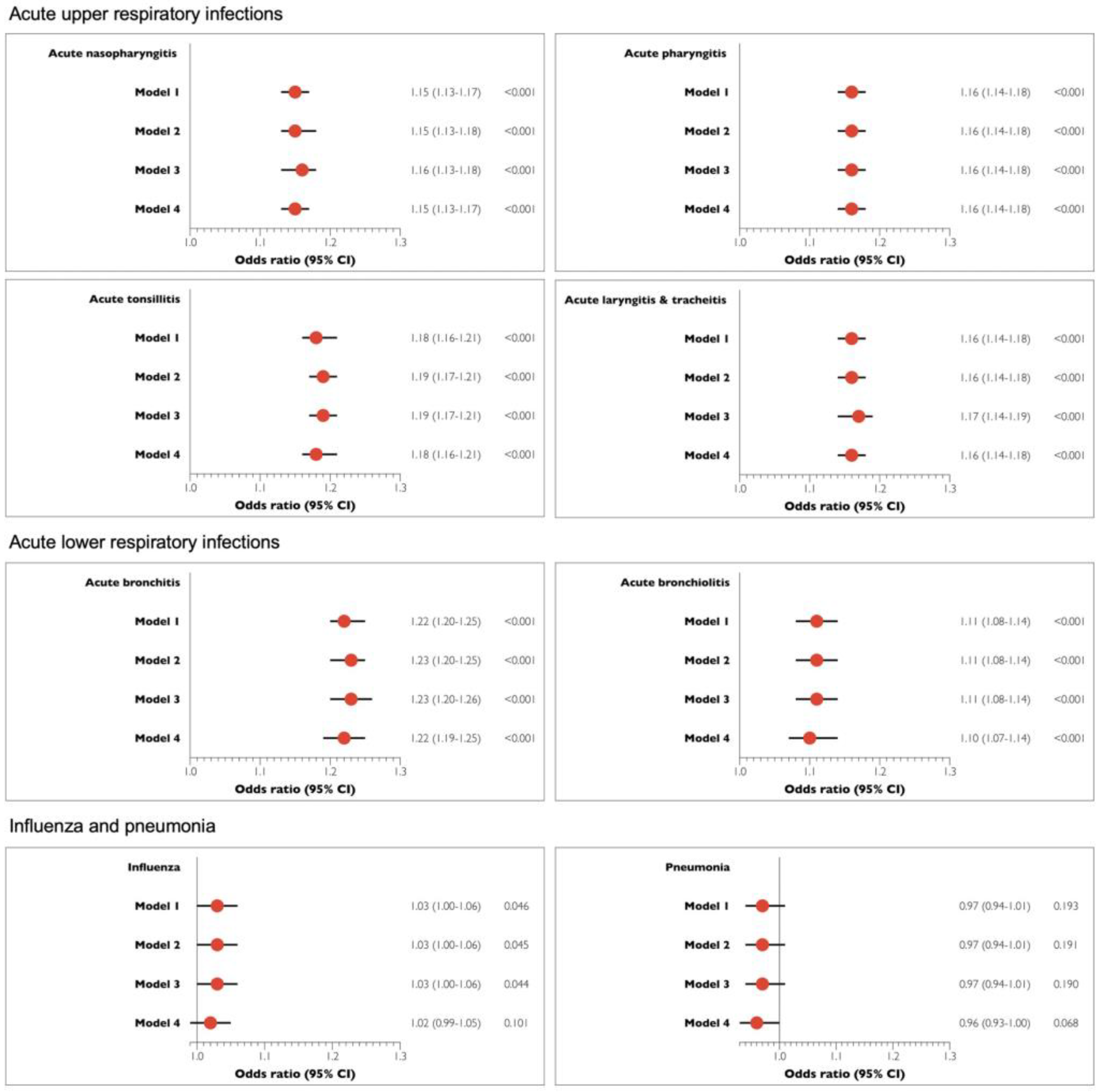
The outcomes of the univariate and multivariate logistic regression analyses performed to investigate the association between the prevalence of CP and acute respiratory infections are shown in Table 3. Univariate analysis showed that total acute respiratory infections (OR, 1.33; 95% CI, 1.29–1.38; p < 0.001), acute upper respiratory infections (OR, 1.26; 95% CI, 1.23–1.30; p < 0.001), and acute lower respiratory infections (OR, 1.23; 95% CI, 1.20–1.26; p < 0.001) were significantly associated with CP. In models 2–4, in which adjustments for sociodemographic variables and comorbidities were performed, participants with CP had a higher chance of having acute respiratory infections, except influenza and pneumonia, compared with participants without CP (p < 0.001). More specifically, in model 4, in which all confounders were adjusted, CP was positively and significantly related to the risk of total acute respiratory infections (OR, 1.33; 95% CI, 1.28–1.38; p < 0.001), acute upper respiratory infections (OR, 1.26; 95% CI, 1.22–1.29; p < 0.001), and acute lower respiratory infections (OR, 1.23; 95% CI, 1.20–1.26; p < 0.001). Figure 2 shows the associations of detailed acute respiratory infectious diseases with chronic periodontitis in the univariate and multivariate analyses.
4. Discussion
Poor oral hygiene associated with local oral infections, especially CP, is known to be a risk factor for acute and chronic respiratory infections. In this study, a significant positive association was found between CP and acute respiratory infections, excluding influenza and acute pneumonia, even after adjusting for sociodemographic variables and comorbidities.
Various possible underlying physiological mechanisms for the role of oral bacteria in the pathogenesis of acute and chronic respiratory infections have been suggested [17,18]. First, dental plaque and calculus can serve as a reservoir for pulmonary pathogens that cause respiratory infection in high-risk elderly people in medical or surgical units. Second, salivary enzymes associated with CP can promote the adhesion of respiratory pathogens to the mucosal tissues of the oral cavity and respiratory tract. In particular, Porphyromonas gingivalis-induced hydrolytic enzymes may destroy the salivary pellicles that resist pathogenic bacteria. Finally, a large variety of cytokines and other biologically active inflammatory mediators induce alteration of respiratory epithelial tissues, which is another potential biological mechanism in the pathogenesis of respiratory infections.
The incidence and severity of chronic respiratory infections are likely to be affected by the severity of CP [19,20,21,22]. A cross-sectional study of the National Health and Nutrition Examination Survey (NHANES) III database reported an increased risk of respiratory infection in patients with clinical attachment loss ≥3 mm compared to those with clinical attachment loss <3 mm (OR, 1.45; 95% CI, 1.02–2.05). Another long-term study found that increased alveolar bone loss is associated with an increased risk of respiratory infection (OR, 1.8; 95% CI, 1.3–2.5). [19,20] Bgyi et al. suggested that the comparative risk of developing postoperative respiratory infection in patients with severe CP was 3.5-fold higher than that in patients with incipient CP (p < 0.0001) [21]. Moreover, a longitudinal retrospective investigation demonstrated that elderly patients (aged > 80 years) with CP may have a higher and increased risk of mortality associated with respiratory infection (Hazard ratio, 3.9; 95% CI, 1.1–3.9; p < 0.05) [22].
However, there are very few studies on the association between CP and acute respiratory infections. This cohort study found that both acute upper and lower respiratory tract infections (including acute nasopharyngitis, acute pharyngitis, acute tonsillitis, acute laryngitis and tracheitis, acute bronchitis, and acute bronchiolitis) were significantly associated with CP; these findings are similar to the corresponding findings with regard to chronic respiratory infections. The results of this study did not show a statistically significant association between CP and influenza and acute pneumonia (p > 0.05). In particular, there was a negative correlation between CP and acute pneumonia, although this was not statistically significant (OR, 0.96; 95% CI, 0.93–1.00; p = 0.068). The relationship between CP and respiratory infections remains unclear because influenza and acute pneumonia are fast-developing respiratory illnesses. Underestimation of the prevalence of influenza and acute pneumonia may weaken the causal relationship and association of CP with influenza and acute pneumonia.
Various clinical and epidemiological studies have demonstrated that self- or professional-driven good oral hygiene practices, such as tooth brushing and professional periodontal treatment, can significantly reduce the incidence or severity of respiratory infections [23,24]. In particular, conventional management of CP, including supragingival and subgingival plaque control using ultrasonic or hand instruments is a very effective routine protocol for the prevention and treatment of respiratory diseases.
In this study, CP was defined based on a combination of diagnostic and prescription codes, but the severity of CP could not be identified because clinical and radiographic periodontal parameters (including plaque index, bleeding on probing, pocket probing depth, clinical attachment loss, marginal bone loss, and number of missing teeth) were not included. This is considered a major fundamental limitation of the NHIS-NSC database. In addition, there are limited clinical data available regarding the potential association between CP and COVID-19. Significant and substantial evidence of an association between CP and COVID-19 is expected to be established in the near future.
5. Conclusions
Within the limitations of this study, the findings of the present cohort study suggest a potential association between CP and acute respiratory infections. Particularly, CP seems to increase the risk of acute upper and lower respiratory infections. Therefore, appropriate management of CP can play a significant role in preventing or reducing the risk of acute respiratory infections. Further prospective and comparative studies are necessary to confirm our findings.
Author Contributions
Conceptualization, J.-H.L. and S.-N.J.; methodology, J.-H.L. and S.-N.J.; software, J.-H.L. and S.-N.J.; validation, J.-H.L. and S.-N.J.; formal analysis, J.-H.L. and S.-N.J.; investigation, J.-H.L. and S.-N.J.; resources, J.-H.L. and S.-N.J.; data curation, J.-H.L. and S.-N.J.; writing—original draft preparation, J.-H.L. and S.-N.J.; writing—review and editing, J.-H.L. and S.-N.J.; visualization, J.-H.L. and S.-N.J.; supervision, J.-H.L. and S.-N.J.; project administration, J.-H.L. and S.-N.J.; funding acquisition, J.-H.L. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by a National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (No. 2019R1A2C1083978).
Institutional Review Board Statement
The study design and protocol were reviewed and authorized by the Institutional Review Board of the Daejeon Dental Hospital, Wonkwang University (approval No. W2107/001-001), and the need for informed or written consent was waived as part of the study approval.
Informed Consent Statement
Patient consent was waived due to retrospective design of the study.
Data Availability Statement
Restrictions apply to the availability of these data. Data was obtained from NHIS and are available https://nhiss.nhis.or.kr (accessed on 10 October 2021) with the permission of NHIS.
Acknowledgments
The NHIS-NSC data used in this study were supplied by the NHIS.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Pihlstrom, B.L.; Michalowicz, B.S.; Johnson, N.W. Periodontal diseases. Lancet 2005, 366, 1809–1820. [Google Scholar] [CrossRef] [Green Version]
- Page, R.C.; Eke, P.I. Case definitions for use in population—Based surveillance of periodontitis. J. Periodontol. 2007, 78, 1387–1399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slots, J. Periodontitis: Facts, fallacies and the future. Periodontology 2017, 75, 7–23. [Google Scholar] [CrossRef]
- Seymour, G.J.; Ford, P.J.; Cullinan, M.P.; Leishman, S.; Yamazaki, K. Relationship between periodontal infections and systemic disease. Clin. Microbiol. Infect. 2007, 13, 3–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.H.; Lee, J.S.; Park, J.Y.; Choi, J.K.; Kim, D.W.; Kim, Y.T.; Choi, S.H. Association of lifestyle-related comorbidities with periodontitis: A nationwide cohort study in korea. Medicine 2015, 94, e1567. [Google Scholar] [CrossRef]
- Lee, J.H.; Oh, J.Y.; Youk, T.M.; Jeong, S.N.; Kim, Y.T.; Choi, S.H. Association between periodontal disease and non-communicable diseases: A 12-year longitudinal health-examinee cohort study in south korea. Medicine 2017, 96, e7398. [Google Scholar] [CrossRef] [PubMed]
- Bui, F.Q.; Almeida-da-Silva, C.L.C.; Huynh, B.; Trinh, A.; Liu, J.; Woodward, J.; Asadi, H.; Ojcius, D.M. Association between periodontal pathogens and systemic disease. Biomed. J. 2019, 42, 27–35. [Google Scholar] [CrossRef]
- Sharma, N.; Shamsuddin, H. Association between respiratory disease in hospitalized patients and periodontal disease: A cross-sectional study. J. Periodontol. 2011, 82, 1155–1160. [Google Scholar] [CrossRef]
- Parashar, P.; Parashar, A.; Saraswat, N.; Pani, P.; Pani, N.; Joshi, S. Relationship between respiratory and periodontal health in adults: A case-control study. J. Int. Soc. Prev. Community Dent. 2018, 8, 560–564. [Google Scholar] [CrossRef]
- Azarpazhooh, A.; Leake, J.L. Systematic review of the association between respiratory diseases and oral health. J. Periodontol. 2006, 77, 1465–1482. [Google Scholar] [CrossRef] [Green Version]
- Jeronimo, L.S.; Abreu, L.G.; Cunha, F.A.; Esteves Lima, R.P. Association between periodontitis and nosocomial pneumonia: A systematic review and meta-analysis of observational studies. Oral Health Prev. Dent. 2020, 18, 11–17. [Google Scholar]
- Scannapieco, F.A. Role of oral bacteria in respiratory infection. J. Periodontol. 1999, 70, 793–802. [Google Scholar] [CrossRef]
- Si, Y.; Fan, H.; Song, Y.; Zhou, X.; Zhang, J.; Wang, Z. Association between periodontitis and chronic obstructive pulmonary disease in a chinese population. J. Periodontol. 2012, 83, 1288–1296. [Google Scholar] [CrossRef] [Green Version]
- Usher, A.K.; Stockley, R.A. The link between chronic periodontitis and copd: A common role for the neutrophil? BMC Med. 2013, 11, 241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.H.; Choi, J.K.; Kim, S.H.; Cho, K.H.; Kim, Y.T.; Choi, S.H.; Jung, U.W. Association between periodontal flap surgery for periodontitis and vasculogenic erectile dysfunction in koreans. J. Periodontal. Implant Sci. 2017, 47, 96–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, D.H.; Jeong, S.N.; Lee, J.H. Severe periodontitis with tooth loss as a modifiable risk factor for the development of alzheimer, vascular, and mixed dementia: National health insurance service-national health screening retrospective cohort 2002–2015. J. Periodontal. Implant Sci. 2020, 50, 303–312. [Google Scholar] [CrossRef]
- Gomes-Filho, I.S.; Passos, J.S.; Seixas da Cruz, S. Respiratory disease and the role of oral bacteria. J. Oral Microbiol. 2010, 2, 5811. [Google Scholar] [CrossRef] [PubMed]
- Paju, S.; Scannapieco, F.A. Oral biofilms, periodontitis, and pulmonary infections. Oral Dis. 2007, 13, 508–512. [Google Scholar] [CrossRef] [Green Version]
- Scannapieco, F.A.; Ho, A.W. Potential associations between chronic respiratory disease and periodontal disease: Analysis of national health and nutrition examination survey iii. J. Periodontol. 2001, 72, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Hayes, C.; Sparrow, D.; Cohen, M.; Vokonas, P.S.; Garcia, R.I. The association between alveolar bone loss and pulmonary function: The va dental longitudinal study. Ann. Periodontol. 1998, 3, 257–261. [Google Scholar] [CrossRef] [PubMed]
- Bagyi, K.; Haczku, A.; Marton, I.; Szabo, J.; Gaspar, A.; Andrasi, M.; Varga, I.; Toth, J.; Klekner, A. Role of pathogenic oral flora in postoperative pneumonia following brain surgery. BMC Infect. Dis. 2009, 9, 104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Awano, S.; Ansai, T.; Takata, Y.; Soh, I.; Akifusa, S.; Hamasaki, T.; Yoshida, A.; Sonoki, K.; Fujisawa, K.; Takehara, T. Oral health and mortality risk from pneumonia in the elderly. J. Dent. Res. 2008, 87, 334–339. [Google Scholar] [CrossRef] [PubMed]
- Yoneyama, T.; Yoshida, M.; Matsui, T.; Sasaki, H. Oral care and pneumonia. Oral care working group. Lancet 1999, 354, 515. [Google Scholar] [CrossRef]
- Fourrier, F.; Cau-Pottier, E.; Boutigny, H.; Roussel-Delvallez, M.; Jourdain, M.; Chopin, C. Effects of dental plaque antiseptic decontamination on bacterial colonization and nosocomial infections in critically ill patients. Intensive Care Med. 2000, 26, 1239–1247. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flowchart of the inclusion and exclusion criteria for the study participants, NHIS-NSC, National Health Insurance Service—National Sample Cohort.
Figure 1.
Flowchart of the inclusion and exclusion criteria for the study participants, NHIS-NSC, National Health Insurance Service—National Sample Cohort.

Figure 2.
Associations of acute respiratory infections with chronic periodontitis in the univariate and multivariate logistic regression analysis. Model 1: unadjusted, Model 2: adjusted for age and sex, Model 3: model 2 plus adjustment for smoking and household income status, and Model 4: model 3 plus adjustment for diabetes mellitus.
Figure 2.
Associations of acute respiratory infections with chronic periodontitis in the univariate and multivariate logistic regression analysis. Model 1: unadjusted, Model 2: adjusted for age and sex, Model 3: model 2 plus adjustment for smoking and household income status, and Model 4: model 3 plus adjustment for diabetes mellitus.


{kind=link}
{kind=link}
Table 1.
Demographic distribution according to chronic periodontitis.
| Variables | Chronic Periodontitis | Non- Chronic Periodontitis | p-Value | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Total | 98,490 | 100.0 | 98,490 | 100.0 | |
| Sex | |||||
| Male | 53,660 | 54.5 | 53,660 | 54.5 | |
| Female | 44,830 | 45.5 | 44,830 | 45.5 | |
| Age group (years) | |||||
| 21–30 | 9963 | 10.1 | 9963 | 10.1 | |
| 31–40 | 23,821 | 24.2 | 23,821 | 24.2 | |
| 41–50 | 31,777 | 32.3 | 31,777 | 32.3 | |
| 51–60 | 19,979 | 20.3 | 19,979 | 20.3 | |
| ≥61 | 12,950 | 13.1 | 12,950 | 13.1 | |
| Household income 1 | |||||
| Low | 13,327 | 13.5 | 13,084 | 13.3 | <0.001 |
| Middle-low | 14,515 | 14.7 | 15,155 | 15.4 | |
| Middle | 18,787 | 19.1 | 19,058 | 19.4 | |
| Middle-high | 23,273 | 23.6 | 23,423 | 23.8 | |
| High | 28,588 | 29.0 | 26,770 | 27.2 | |
| Smoking status | |||||
| Yes | 33,402 | 33.9 | 31,432 | 31.9 | <0.001 |
| No | 65,088 | 66.1 | 67,058 | 68.1 | |
| Comorbid diseases | |||||
| Diabetes mellitus | 25,870 | 26.3 | 22,633 | 23.0 | <0.001 |
| Acute respiratory infections | |||||
| Acute upper respiratory infections | 88,262 | 89.6 | 85,900 | 87.2 | <0.001 |
| Acute lower respiratory infections | 79,828 | 81.1 | 76,434 | 77.6 | <0.001 |
| Influenza and pneumonia | 14,382 | 14.6 | 14,311 | 14.5 | 0.650 |
1 Quintiles based on each household’s insurance status (with a medical aid program in the first quintile)
Table 2.
Demographic distribution according to acute respiratory infections.
| Variables | Total Acute Respiratory Infections | Acute Upper Respiratory Infections | Acute Lower Respiratory Infections | Influenza and Pneumonia | ||||
|---|---|---|---|---|---|---|---|---|
| n (%) | p-Value | n (%) | p-Value | n (%) | p-Value | n (%) | p-Value | |
| Total | 183,972 (100.0%) | 174,162 (100.0%) | 156,262 (100.0%) | 28,693 (100.0%) | ||||
| Sex | ||||||||
| Male | 97,477 (53.0%) | <0.001 | 90,993 (52.2%) | <0.001 | 79,657 (51.0%) | <0.001 | 13,533 (47.2%) | <0.001 |
| Female | 86,495 (47.0%) | 83,169 (47.8%) | 76,605 (49.0%) | 15,160 (52.8%) | ||||
| Age group (years) | ||||||||
| 21–30 | 18,607 (10.1%) | <0.001 | 17,810 (10.2%) | <0.001 | 15,747 (10.1%) | <0.001 | 2779 (9.7%) | 0.099 |
| 31–40 | 44,244 (24.0%) | 42,174 (24.2%) | 37,076 (23.7%) | 5970 (20.8%) | ||||
| 41–50 | 58,737 (31.9%) | 55,324 (31.8%) | 49,366 (31.6%) | 7806 (27.2%) | ||||
| 51–60 | 37,589 (20.4%) | 35,424 (20.3%) | 32,601 (20.9%) | 6304 (22.0%) | ||||
| ≥61 | 24,795 (13.5%) | 23,430 (13.5%) | 21,472 (13.7%) | 5834 (20.3%) | ||||
| Household income a | ||||||||
| Low | 25,413 (13.8%) | <0.001 | 23,843(13.7%) | <0.001 | 21,591 (13.8%) | <0.001 | 3993 (13.9%) | <0.001 |
| Middle-low | 27,594 (15.0%) | 26,121 (15.0%) | 23,463 (15.0%) | 4325 (15.1%) | ||||
| Middle | 35,186 (19.1%) | 33,298 (19.1%) | 29,942 (19.2%) | 5360 (18.7%) | ||||
| Middle-high | 43,819 (23.8%) | 41,554 (23.9%) | 37,342 (23.9%) | 6812 (23.7%) | ||||
| High | 51,960 (28.2%) | 49,346 (28.3%) | 43,924 (28.1%) | 8203 (28.6%) | ||||
| Smoking status | ||||||||
| Yes | 58,448 (31.8%) | <0.001 | 54,350 (31.2%) | <0.001 | 47,610 (30.5%) | <0.001 | 7904 (27.5%) | <0.001 |
| No | 125,524 (68.2%) | 119,812 (68.8%) | 108,652 (69.5%) | 20,789 (72.5%) | ||||
| Comorbid diseases | ||||||||
| Diabetes mellitus | 46,219 (25.1%) | <0.001 | 43,885 (25.2%) | <0.001 | 40,312 (25.8%) | <0.001 | 8629 (30.1%) | <0.001 |
| Chronic periodontitis | 92,867 (50.5%) | <0.001 | 88,262 (50.7%) | <0.001 | 79,828 (51.1%) | <0.001 | 14,382 (50.1%) | 0.652 |
a Quintiles based on each household’s insurance status (with a medical aid program in the first quintile).
Table 3.
ORs and 95% CIs for chronic periodontitis in participants with acute respiratory infections in univariate and multivariate logistic regression models.
Table 3.
ORs and 95% CIs for chronic periodontitis in participants with acute respiratory infections in univariate and multivariate logistic regression models.
| Variables | Model 1 | Model 2 | Model 3 | Model 4 | ||||
|---|---|---|---|---|---|---|---|---|
| Crude OR (95% CI) | p-Value | Adjusted OR (95% CI) | p-Value | Adjusted OR (95% CI) | p-Value | Adjusted OR (95% CI) | p-Value | |
| Total acute respiratory infections | 1.33 (1.29–1.38) | <0.001 | 1.34 (1.29–1.39) | <0.001 | 1.35 (1.30–1.40) | <0.001 | 1.33 (1.28–1.38) | <0.001 |
| Acute upper respiratory infections | 1.26 (1.23–1.30) | <0.001 | 1.27 (1.23–1.30) | <0.001 | 1.27 (1.23–1.31) | <0.001 | 1.26 (1.22–1.29) | <0.001 |
| Acute lower respiratory infections | 1.23 (1.20–1.26) | <0.001 | 1.24 (1.21–1.26) | <0.001 | 1.24 (1.21–1.27) | <0.001 | 1.23 (1.20–1.26) | <0.001 |
| Influenza and pneumonia | 1.00 (0.98–1.03) | 0.650 | 1.00 (0.98–1.03) | 0.648 | 1.00 (0.98–1.03) | 0.643 | 0.99 (0.97–1.02) | 0.902 |
Model 1: unadjusted. Model 2: adjusted for age and sex. Model 3: model 2 plus adjustment for smoking and household income status. Model 4: model 3 plus adjustment for diabetes mellitus. OR, odds ratio; CI, confidence interval.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Lee, J.-H.; Jeong, S.-N. Chronic Periodontitis and Acute Respiratory Infections: A Nationwide Cohort Study. Appl. Sci. 2021, 11, 9493. https://0-doi-org.brum.beds.ac.uk/10.3390/app11209493
AMA Style
Lee J-H, Jeong S-N. Chronic Periodontitis and Acute Respiratory Infections: A Nationwide Cohort Study. Applied Sciences. 2021; 11(20):9493. https://0-doi-org.brum.beds.ac.uk/10.3390/app11209493
Chicago/Turabian StyleLee, Jae-Hong, and Seong-Nyum Jeong. 2021. "Chronic Periodontitis and Acute Respiratory Infections: A Nationwide Cohort Study" Applied Sciences 11, no. 20: 9493. https://0-doi-org.brum.beds.ac.uk/10.3390/app11209493
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.