
Analysis of Body-Slip and Buttock Pressure Characteristics during Operation of a Double-Sliding Reclining Wheelchair in Patients with Spinal Cord Injury


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
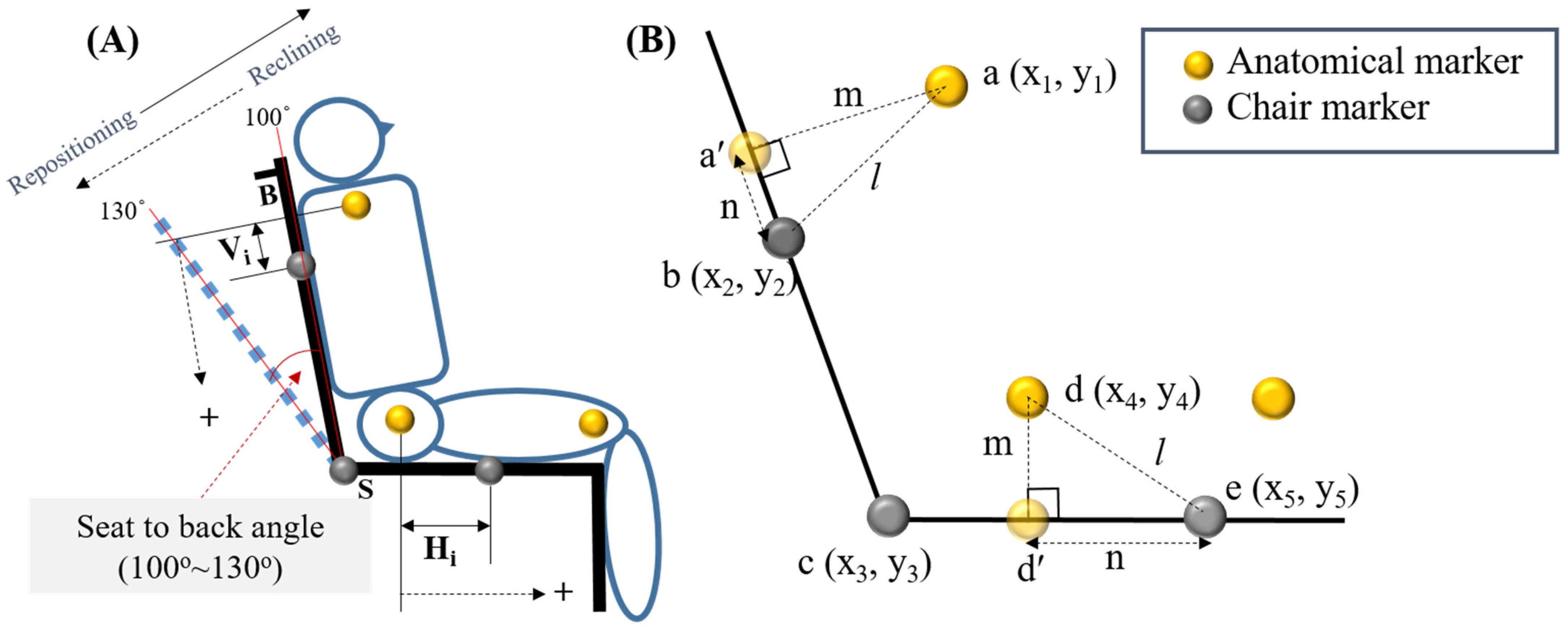
2.2. Measurements
2.3. Experimental Procedure
2.4. Statistical Analysis
3. Results
3.1. Body-Slip
3.2. Buttock Pressure
4. Discussion
4.1. Body-Slip and Buttock Pressure Changes during Wheelchair Reclining
4.2. Body-Slip and Buttock Pressure Changes during Wheelchair Repositioning
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bader, D. The recovery characteristics of soft tissues following repeated loading. J. Rehabil. Res. Dev. 1990, 27, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Colin, D.; Saumet, J. Influence of external pressure on transcutaneous oxygen tension and laser Doppler flowmetry on sacral skin. Clin. Physiol. 1996, 16, 61–72. [Google Scholar] [CrossRef] [PubMed]
- Merbitz, C.; King, R.; Bleiberg, J.; Grip, J. Wheelchair push-ups: Measuring pressure relief frequency. Arch. Phys. Med. Rehabil. 1985, 66, 433–438. [Google Scholar]
- Hobson, D.A. Comparative effects of posture on pressure and shear at the body-seat interface. J. Rehabil. Res. Dev. 1992, 29, 21–31. [Google Scholar] [CrossRef]
- Burns, S.P.; Betz, K.L. Seating pressures with conventional and dynamic wheelchair cushions in tetraplegia. Arch. Phys. Med. Rehabil. 1999, 80, 566–571. [Google Scholar] [CrossRef]
- Lacoste, M.; Weiss-Lambrou, R.; Allard, M.; Dansereau, J. Powered tilt/recline systems: Why and how are they used? Assist. Technol. 2003, 15, 58–68. [Google Scholar] [CrossRef]
- Aissaoui, R.; Lacoste, M.; Dansereau, J. Analysis of sliding and pressure distribution during a repositioning of persons in a simulator chair. IEEE Trans. Neural Syst. Rehabil. Eng. 2001, 9, 215–224. [Google Scholar] [CrossRef]
- Guttmann, L. The Prevention and Treatment of Pressure Sores; Macmillan: London, UK, 1976. [Google Scholar]
- Pfaff, K. Recline and Tilt: Making the Right Match. Team Rehabilitation Report. 1993, pp. 23–27. Available online: https://fdocuments.in/document/when-seated-in-a-wheelchair-how-many-degrees-tilt-is-02092002-prepared.html (accessed on 9 November 2021).
- Kobara, K.; Fujita, D.; Osaka, H.; Ito, T.; Watanabe, S. Influence of distance between the rotation axis of back support and the hip joint on shear force applied to buttocks in a reclining wheelchair’s back support. Prosthet. Orthot. Int. 2013, 37, 459–464. [Google Scholar] [CrossRef] [Green Version]
- Zemp, R.; Rhiner, J.; Plüss, S.; Togni, R.; Plock, J.A.; Taylor, W.R. Wheelchair tilt-in-space and recline functions: Influence on sitting interface pressure and ischial blood flow in an elderly population. BioMed Res. Int. 2019, 2019, 4027976. [Google Scholar] [CrossRef]
- Jan, Y.-K.; Crane, B.A.; Liao, F.; Woods, J.A.; Ennis, W.J. Comparison of muscle and skin perfusion over the ischial tuberosities in response to wheelchair tilt-in-space and recline angles in people with spinal cord injury. Arch. Phys. Med. Rehabil. 2013, 94, 1990–1996. [Google Scholar] [CrossRef] [Green Version]
- Jan, Y.-K.; Liao, F.; Jones, M.A.; Rice, L.A.; Tisdell, T. Effect of durations of wheelchair tilt-in-space and recline on skin perfusion over the ischial tuberosity in people with spinal cord injury. Arch. Phys. Med. Rehabil. 2013, 94, 667–672. [Google Scholar] [CrossRef] [Green Version]
- Chang, Y.; Kim, Y.C.; Nam, K.T.; Kang, J.S.; Jeong, B.R.; Hong, E.-P. Analysis of body slip and seat pressure in powered wheelchairs with two-slide recline system. Int. J. Precis. Eng. Manuf. 2020, 21, 525–535. [Google Scholar] [CrossRef]
- Brienza, D.M.; Karg, P.E.; Geyer, M.J.; Kelsey, S.; Trefler, E. The relationship between pressure ulcer incidence and buttock-seat cushion interface pressure in at-risk elderly wheelchair users. Arch. Phys. Med. Rehabil. 2001, 82, 529–533. [Google Scholar] [CrossRef] [PubMed]
- Henderson, J.L.; Price, S.H.; Brandstater, M.E.; Mandac, B.R. Efficacy of three measures to relieve pressure in seated persons with spinal cord injury. Arch. Phys. Med. Rehabil. 1994, 75, 535–539. [Google Scholar] [PubMed]
- Warren, C.; Ko, M.; Smith, C.; Imre, J. Reducing back displacement in the powered reclining wheelchair. Arch. Phys. Med. Rehabil. 1982, 63, 447–449. [Google Scholar] [PubMed]
- Bogie, K.; Bader, D. The biomechanics of seating—An initial study. In International Series on Biomechanics; Free University: Amsterdam, The Netherlands, 1987; pp. 498–503. [Google Scholar]
- Shields, R.K.; Cook, T.M. Effect of seat angle and lumbar support on seated buttock pressure. Phys. Ther. 1988, 68, 1682–1686. [Google Scholar] [CrossRef]
- Spijkerman, D.; Terburg, M.; Goossens, R.; Stijnen, T. Effects of inflation pressure and posture on the body-seat interface pressure of spinal cord injured patients seated on an air-filled wheelchair cushion. J. Rehabil. Sci. 1995, 8, 8–12. [Google Scholar]
- Aissaoui, R. Effect of repositioning on seat and back pressure measurements and posture of able-bodied subjects. In Proceedings of the International Conference on Wheelchairs Seating, Dundee, Scotland, 8–12 September 1997. [Google Scholar]
- Gilsdorf, P.; Patterson, R.; Appel, N. Sitting forces and wheelchair mechanics. J. Rehabil. Res. Dev. 1990, 27, 239–246. [Google Scholar] [CrossRef]
- Huang, H.-C.; Yeh, C.-H.; Chen, C.-M.; Lin, Y.-S.; Chung, K.-C. Sliding and pressure evaluation on conventional and V-shaped seats of reclining wheelchairs for stroke patients with flaccid hemiplegia: A crossover trial. J. Neuroeng. Rehabil. 2011, 8, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goossens, R.; Snijders, C.; Holscher, T.; Heerens, W.C.; Holman, A. Shear stress measured on beds and wheelchairs. Scand. J. Rehabil. Med. 1997, 29, 131–136. [Google Scholar]
- Peterson, M.J.; Adkins, H.V. Measurement and redistribution of excessive pressures during wheelchair sitting: A clinical report. Phys. Ther. 1982, 62, 990–994. [Google Scholar] [CrossRef] [PubMed]
- Makhsous, M.; Lim, D.; Hendrix, R.; Bankard, J.; Rymer, W.Z.; Lin, F. Finite element analysis for evaluation of pressure ulcer on the buttock: Development and validation. IEEE Trans. neural Syst. Rehabil. Eng. 2007, 15, 517–525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Linder-Ganz, E.; Shabshin, N.; Itzchak, Y.; Gefen, A. Assessment of mechanical conditions in sub-dermal tissues during sitting: A combined experimental-MRI and finite element approach. J. Biomech. 2007, 40, 1443–1454. [Google Scholar] [CrossRef]
- Linder-Ganz, E.; Shabshin, N.; Itzchak, Y.; Yizhar, Z.; Siev-Ner, I.; Gefen, A. Strains and stresses in sub-dermal tissues of the buttocks are greater in paraplegics than in healthy during sitting. J. Biomech. 2008, 41, 567–580. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (y) | Height (m) | Weight (kg) | BMI (kg/m2) | Level of Injury | AIS | Total Length of Wheelchair Use (y) | Wheelchair Use Per Day (h) | |
|---|---|---|---|---|---|---|---|---|
| Patient #1 | 55 | 1.65 | 64.2 | 23.6 | L1 | B | 15.2 | >11 |
| Patient #2 | 48 | 1.63 | 65.4 | 24.6 | L1 | B | 15.4 | >11 |
| Patient #3 | 52 | 1.70 | 64.1 | 22.2 | T11 | A | 20.5 | >8 |
| Patient #4 | 52 | 1.75 | 66.0 | 21.6 | T11 | A | 8.2 | >7 |
| Patient #5 | 60 | 1.75 | 85.2 | 29.5 | T7 | A | 14.7 | >8 |
| Patient #6 | 59 | 1.77 | 75.9 | 24.2 | T11 | A | 13.5 | >10 |
| Patient #7 | 52 | 1.72 | 69.9 | 23.6 | T11 | A | 13.2 | >6 |
| Patient #8 | 55 | 1.65 | 74.5 | 27.4 | T11 | A | 11.9 | >6 |
| Patient #9 | 47 | 1.70 | 80.2 | 27.8 | L1 | A | 7.8 | >6 |
| Patient #10 | 66 | 1.63 | 50.2 | 18.9 | T12 | A | 15.0 | >6 |
| Condition | Variable | Double-Sliding | Non-Sliding | Mean Difference | SE | 95% CI | t-Value | |
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| Reclining | BS (mm) | −3.9 ± 7.6 | −25.3 ± 24.3 | 21.42 | 6.95 | 5.69 | 37.15 | 3.081 * |
| SS (mm) | −18.8 ± 10.3 | −10.9 ± 5.6 | −7.86 | 2.49 | −13.49 | −2.24 | −3.164 * | |
| TBS (mm) | 25.9 ± 7.6 | 42.2 ± 14.8 | −16.35 | 5.17 | −28.05 | −4.64 | −3.159 * | |
| Repositioning | BS (mm) | 1.5 ± 11.6 | 18.5 ± 23.2 | −17.00 | 5.39 | −29.20 | −4.80 | −3.153 * |
| SS (mm) | 20.2 ± 8.5 | 14.9 ± 6.4 | 5.28 | 2.45 | −0.26 | 10.83 | 2.155 | |
| TBS (mm) | 30.0 ± 7.6 | 40.8 ± 13.0 | −10.82 | 3.93 | −19.71 | −1.92 | −2.751 * | |
| IUP-RUP | BS (mm) | −2.4 ± 7.7 | −6.8 ± 9.4 | 4.42 | 3.49 | −3.47 | 12.31 | 1.268 |
| SS (mm) | 1.5 ± 3.7 | 4.0 ± 4.6 | −2.58 | 2.33 | −7.84 | 2.68 | −1.109 | |
| TBS (mm) | 8.9 ± 6.8 | 12.9 ± 8.4 | −4.00 | 2.81 | −10.35 | 2.35 | −1.425 | |
| Condition | Variable | Double-Sliding | Non-Sliding | Mean Difference | SE | 95% CI | t-Value | ||
|---|---|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||||
| IUP | Force (%BW) | 17.01 ± 4.44 | 18.45 ± 5.37 | −1.44 | 1.48 | −1.91 | 4.79 | −0.970 | |
| Mean pressure (kPa) | 1.33 ± 0.26 | 1.47 ± 0.38 | −0.14 | 0.14 | −0.18 | 0.45 | −0.978 | ||
| Peak pressure (kPa) | Ischial tuberosity | 25.22 ± 15.73 | 20.37 ± 11.33 | 4.85 | 2.61 | −10.74 | 1.05 | 1.861 | |
| Sacrum | 7.61 ± 2.85 | 13.39 ± 7.68 | −5.79 | 2.01 | 1.23 | 10.34 | −2.875 * | ||
| FRP | Force (N/kg) | 14.94 ± 4.32 | 13.83 ± 1.50 | 1.11 | 1.17 | −3.75 | 1.52 | 0.955 | |
| Mean pressure (kPa) | 1.12 ± 0.27 | 1.23 ± 0.46 | −0.11 | 0.12 | −0.16 | 0.37 | −0.930 | ||
| Peak pressure (kPa) | Ischial tuberosity | 14.20 ± 7.05 | 18.09 ± 8.32 | −3.89 | 2.36 | −1.45 | 9.23 | −1.648 | |
| Sacrum | 14.30 ± 7.03 | 18.05 ± 8.31 | −3.75 | 2.37 | −1.60 | 9.11 | −1.587 | ||
| RUP | Force (N/kg) | 19.90 ± 5.76 | 17.23 ± 4.30 | 2.67 | 1.29 | −5.58 | 0.23 | 2.081 | |
| Mean pressure (kPa) | 1.35 ± 0.25 | 1.57 ± 0.34 | −0.22 | 0.12 | −0.06 | 0.50 | −1.780 | ||
| Peak pressure (kPa) | Ischial tuberosity | 26.07 ± 13.45 | 23.59 ± 15.39 | 2.48 | 1.44 | −5.73 | 0.78 | 1.720 | |
| Sacrum | 5.87 ± 2.46 | 12.00 ± 7.54 | −6.13 | 2.57 | 0.31 | 11.95 | −2.384 * | ||
| Condition | Variable | Double-sliding | Non-sliding | Mean difference | SE | 95% CI | t-Value | ||
|---|---|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||||
| Reclining | Force (%BW) | −3.30 ± 4.22 | −3.60 ± 4.38 | 0.30 | 0.93 | −2.41 | 1.81 | 0.322 | |
| Mean pressure (kPa) | −0.21 ± 0.28 | −0.24 ± 0.28 | 0.03 | 0.05 | −0.15 | 0.09 | 0.521 | ||
| Peak pressure (kPa) | Ischial tuberosity | −11.02 ± 10.11 | −2.28 ± 9.71 | −8.74 | 2.61 | 2.83 | 14.65 | −3.344 ** | |
| Sacrum | 6.69 ± 7.59 | 4.66 ± 6.11 | 2.03 | 2.85 | −8.48 | 4.42 | 0.712 | ||
| Repositioning | Force (%BW) | 3.30 ± 4.16 | 5.10 ± 5.30 | −1.80 | 0.81 | −0.04 | 3.64 | −2.212 | |
| Mean pressure (kPa) | 0.23 ± 0.30 | 0.34 ± 0.33 | −0.11 | 0.06 | −0.02 | 0.24 | −1.968 | ||
| Peak pressure (kPa) | Ischial tuberosity | 11.87 ± 8.60 | 5.50 ± 13.71 | 6.37 | 2.66 | −12.38 | −0.35 | 2.394 * | |
| Sacrum | −8.43 ± 7.61 | −6.05 ± 5.73 | −2.38 | 2.81 | −3.98 | 8.74 | −0.846 | ||
| IUP-RUP | Force (%BW) | 0.20 ± 1.62 | 1.40 ± 1.51 | −0.12 | 0.47 | 0.14 | 2.26 | −2.571 * | |
| Mean pressure (kPa) | 0.02 ± 0.11 | 0.10 ± 0.09 | −0.08 | 0.03 | 0.01 | 0.16 | −2.576 * | ||
| Peak pressure (kPa) | Ischial tuberosity | 0.85 ± 5.74 | 3.23 ± 4.91 | −2.38 | 2.74 | −3.82 | 8.57 | −0.868 | |
| Sacrum | −1.74 ± 2.63 | −1.39 ± 4.50 | −0.35 | 1.75 | −3.62 | 4.32 | −0.199 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, Y.; Kang, J.; Jeong, B.; Kim, Y.; Hong, E.-P.; Kim, G. Analysis of Body-Slip and Buttock Pressure Characteristics during Operation of a Double-Sliding Reclining Wheelchair in Patients with Spinal Cord Injury. Appl. Sci. 2021, 11, 10651. https://0-doi-org.brum.beds.ac.uk/10.3390/app112210651
Chang Y, Kang J, Jeong B, Kim Y, Hong E-P, Kim G. Analysis of Body-Slip and Buttock Pressure Characteristics during Operation of a Double-Sliding Reclining Wheelchair in Patients with Spinal Cord Injury. Applied Sciences. 2021; 11(22):10651. https://0-doi-org.brum.beds.ac.uk/10.3390/app112210651
Chicago/Turabian StyleChang, Yunhee, Jungsun Kang, Bora Jeong, Yongcheol Kim, Eung-Pyo Hong, and Gyoosuk Kim. 2021. "Analysis of Body-Slip and Buttock Pressure Characteristics during Operation of a Double-Sliding Reclining Wheelchair in Patients with Spinal Cord Injury" Applied Sciences 11, no. 22: 10651. https://0-doi-org.brum.beds.ac.uk/10.3390/app112210651