Retrospective Case Series Regarding the Advantages of Cortico-Puncture (CP) Therapy in Association with Micro-Implant Assisted Rapid Palatal Expander (MARPE)

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Method
- -
- Patients without craniofacial abnormalities;
- -
- No previous orthodontic treatment;
- -
- Transverse maxillary deficiency;
- -
- Unilateral or bilateral crossbite.
Surgical Protocol
3. Statistical Analysis
4. Results
5. Discussion
6. Conclusions
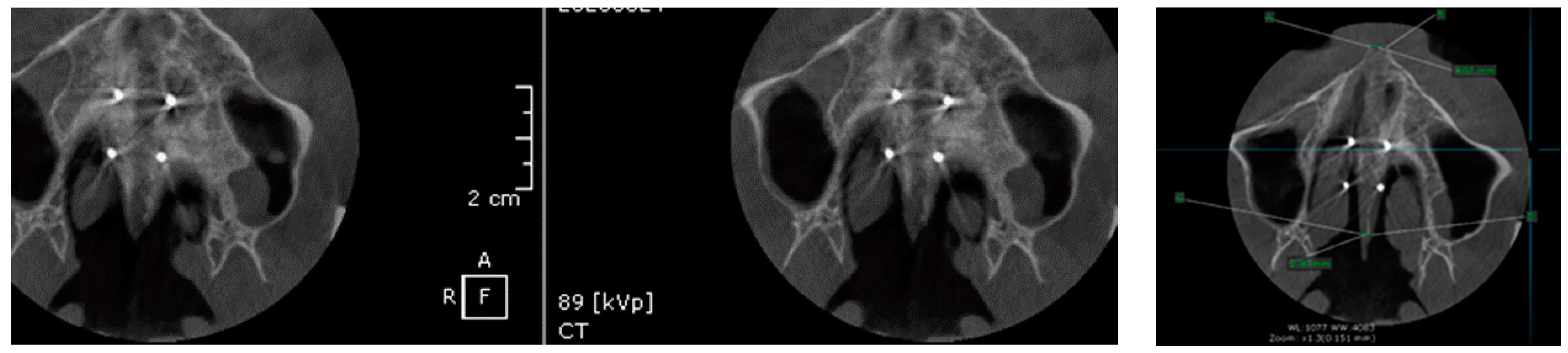
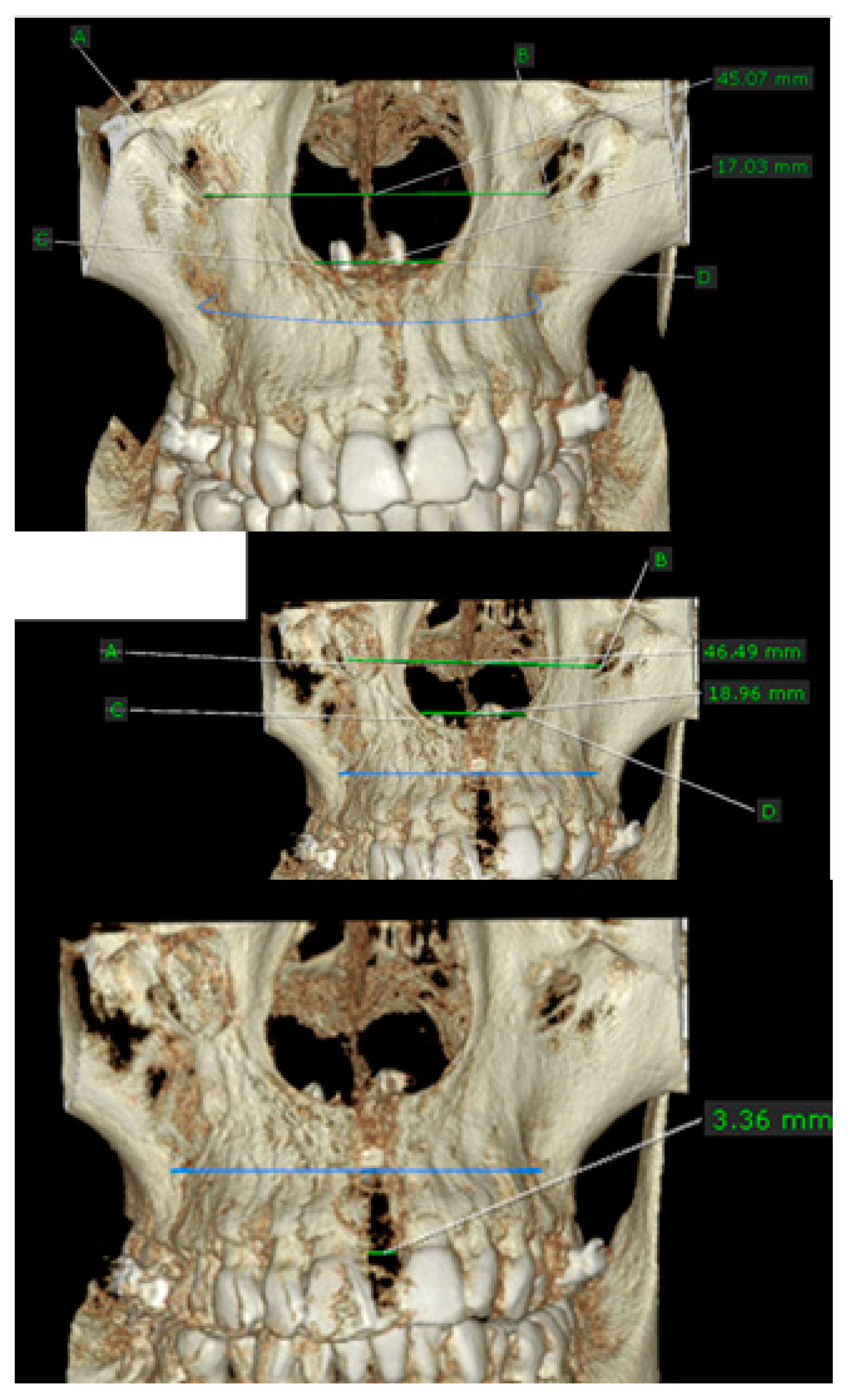
- MARPE associated with cortico-puncture therapy efficiently split the midpalatal suture in adults. The mean split at the anterior nasal spine (ANS) and posterior nasal spine (PNS) was 3.76 and 3.12 mm, respectively. The magnitude of the split at the PNS was smaller than at the ANS (by approximately 85% of the distance), showing that the opening of the midpalatal suture was almost parallel in the anteroposterior direction.
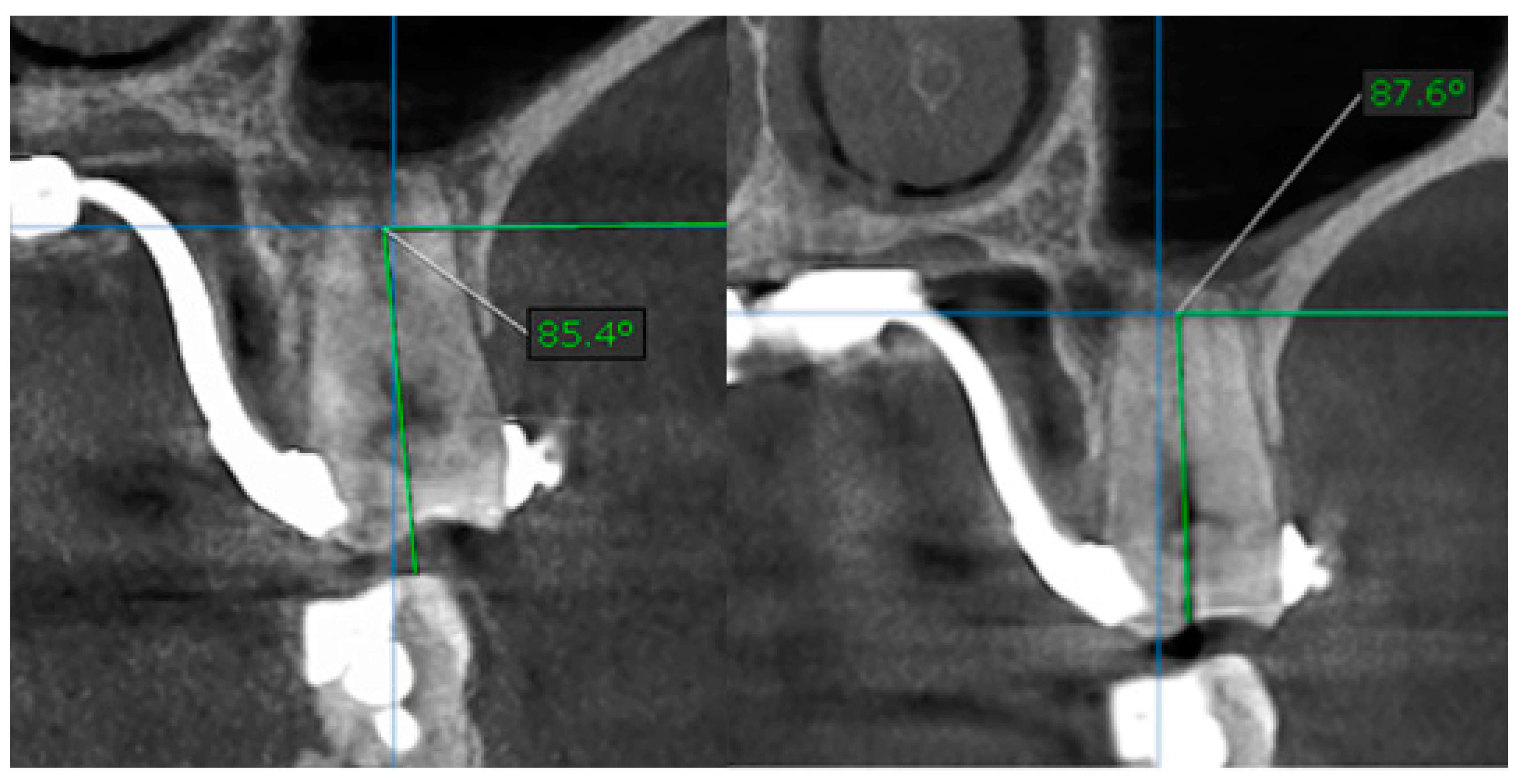
- MARPE therapy associated with cortico-puncture therapy had a positive outcome on midpalatal suture opening and maxillary advancement, but a medium molar inclination of 2.005° was also observed, suggesting that tooth movement cannot be avoided because of the anchorage of the MARPE device at the molar level.
- Our results suggest that non-surgical palatal expansion, assisted by micro-implants and cortico-puncture, is achievable and predictable in young adults. This occurs in safe conditions without the need for more complex surgical treatment.
- The combination of MARPE and the cortico-puncture method proved to be a non-surgical treatment option to correct maxillary transverse deficiency in young adult patients. Cortico-puncture was able to weaken the suture interdigitation, thus facilitating the split.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- MacGinnis, M.; Chu, H.; Youssef, G.; Wu, K.W.; Machado, A.W.; Moon, W. The effects of micro-implant assisted rapid palatal expansion (MARPE) on the nasomaxillary complex—A finite element method (FEM) analysis. Prog. Orthod. 2014, 15, 52. [Google Scholar] [CrossRef] [Green Version]
- Hartono, N.; Soegiharto, B.M.; Widayati, R. The difference of stress distribution of maxillary expansion using rapid maxillary expander (RME) and maxillary skeletal expander (MSE)—A finite element analysis. Prog. Orthod. 2018, 19, 33. [Google Scholar] [CrossRef] [PubMed]
- Wehrbein, H.; Glatzmaier, J.; Mundwiller, U.; Diedrich, P. The Orthosystem—A new implant system for orthodontic anchorage in the palate. J. Orofac. Orthop. 1996, 57, 142–153. [Google Scholar] [CrossRef] [PubMed]
- Lagravere, M.O.; Carey, J.P.; Heo, G.; Toogood, R.W.; Major, P.W. Transverse, vertical, and anteroposterior changes from bone-anchored maxillary expansion vs traditional rapid maxillary expansion: A randomized clinical trial. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 304–305. [Google Scholar] [CrossRef]
- Liu, S.S.; Kyung, H.; Buschang, P.H. Continuous forces are more effective than intermittent forces in expanding sutures. Eur. J. Orthod. 2010, 32, 371–380. [Google Scholar] [CrossRef] [Green Version]
- Tausche, E.; Hansen, L.; Schneider, M.; Harzer, W. Expansion maxillaire rapide par appui osseux avec une vis Hyrax implanto-portée: Le Dresden Distractor (DD) ou Disjoncteur de Dresde. Orthod. Fr. 2008, 79, 127–135. [Google Scholar] [CrossRef]
- Deeb, W.; Hansen, L.; Hotan, T.; Hietschold, V.; Harzer, W.; Tausche, E. Changes in nasal volume after surgically assisted bone-borne rapid maxillary expansion. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 782–789. [Google Scholar] [CrossRef]
- Angelieri, F.; Cevidanes, L.H.S.; Franchi, L.; Goncalves, J.R.; Benavides, E.; McNamara, J.A., Jr. Midpalatal suture maturation: Classification method for individual assessment before rapid maxillary expansion. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 759–769. [Google Scholar] [CrossRef] [Green Version]
- McNamara, J.A., Jr.; Lione, R.; Franchi, L.; Angelieri, F.; Cevidanes, L.H.; Darendeliler, M.A.; Cozza, P. The role of rapid maxillary expansion in the promotion of oral and general health. Prog. Orthod. 2015, 16, 33. [Google Scholar] [CrossRef] [Green Version]
- Möhlhenrich, S.C.; Modabber, A.; Kniha, K.; Peters, F.; Steiner, T.; Hölzle, F.; Fritz, U.; Raith, S. Simulation of three surgical techniques combined with two different bone-borne forces for surgically assisted rapid palatal expansion of the maxillofacial complex: A finite element analysis. Int. J. Oral Maxillofac. Surg. 2017, 46, 1306–1314. [Google Scholar] [CrossRef]
- Suri, L.; Taneja, P. Surgically assisted rapid palatal expansion: A literature review. Am. J. Orthod. Dentofac. Orthop. 2008, 133, 290–302. [Google Scholar] [CrossRef] [PubMed]
- Alexander, N.S.; Schroeder, J.W., Jr. Pediatric obstructive sleep apnea syndrome. Pediatr. Clin. N. Am. 2013, 60, 827–840. [Google Scholar] [CrossRef] [PubMed]
- Haas, A.J. The treatment of maxillary deficiency by opening of the midpalatal suture. Angle Orthod. 1965, 35, 200–217. [Google Scholar] [PubMed]
- Lione, R.; Ballanti, F.; Franchi, L.; Baccetti, T.; Cozza, P. Treatment and posttreatment skeletal effects of rapid maxillary expansion studied with low-dose computed tomography in growing subjects. Am. J. Orthod. Dentofac. Orthop. 2008, 134, 389–392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wertz, R.A. Skeletal and dental changes accompanying rapid midpalatal suture opening. Am. J. Orthod. 1970, 58, 41–66. [Google Scholar] [CrossRef]
- Stuart, D.A.; Wiltshire, W.A. Rapid palatal expansion in the young adult: Time for a paradigm shift? J. Can. Dent. Assoc. 2003, 69, 374–377. [Google Scholar]
- Cantarella, D.; Dominguez-Mompell, R.; Moschik, C.; Sfogliano, L.; Elkenawy, I.; Pan, H.; Mallya, S.M.; Moon, W. Zygomaticomaxillary modifications in the horizontal plane induced by micro-implant-supported skeletal expander, analyzed with CBCT images. Prog. Orthod. 2018, 19, 41. [Google Scholar] [CrossRef] [Green Version]
- Cunha, A.C. Expansão Maxilar Assistida por Mini-Implantes: Estudo do Complexo Sutural Craniofacial sob Perspectivas Clínicas e Microestruturais. Ph.D. Thesis, Universidade Federal do Rio de Janeiro, Rio de Janeiro, Brasil, 2017. [Google Scholar]
- Lin, L.; Ahn, H.W.; Kim, S.J.; Moon, S.C.; Kim, S.H.; Nelson, G. Tooth-borne vs boneborne rapid maxillary expanders in late adolescence. Angle Orthod. 2015, 85, 253–262. [Google Scholar] [CrossRef]
- Haas, A.J. Palatal expansion: Just the of dentofacial orthopedics. Am. J. Orthod. 1970, 57, 219–255. [Google Scholar]
- Lione, R.; Franchi, L.; Cozza, P. Does rapid maxillary expansion induce adverse effects in growing subjects? Angle Orthod. 2012, 83, 172–182. [Google Scholar] [CrossRef] [Green Version]
- Winsauer, H.; Walter, A.; Muchitsch, A.P.; Winsauer, C.; Jaeschke, D.; Katsaros, C.; Scherfler, M.; Ploder, O. Pure bone borne maxillary expansion with 4 mini-implants in adults with and without SARPE: A consecutive study of 35 patients. Presented at the 91st Congress of The European Orthodontic Society, Venice, Italy, 13 June 2015. [Google Scholar]
- Moon, H.-W.; Kim, M.-J.; Ahn, H.-W.; Kim, S.-J.; Kim, S.-H.; Chung, K.-R.; Nelson, G. Molar Inclination and Surrounding Alveolar Bone Change Relative to the Design of Bone-borne Maxillary Expanders: A Cbct study. Angle Orthod. 2020, 90, 13–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Celenk-Koca, T.; Erdinc, A.E.; Hazar, S.; Harris, L.; English, J.D.; Akyalcin, S. Evaluation of miniscrew-supported rapid maxillary expansion in adolescents: A prospective randomized clinical trial. Angle Orthod. 2018, 88, 702–709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garib, D.G.; de Lima Navarro, R. Francischone CE, Oltramari PVP. Expansão rápida da maxila ancorada em implantes: Uma nova proposta para expansão ortopédica na dentadura permanente. Rer. Den. Press Ortod. Ortop. Fac. 2007, 12, 75–81. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.-J.; Park, Y.-C.; Park, J.-Y.; Hwang, W.-S. Miniscrew-assisted nonsurgical palatal expansion before orthognathic surgery for a patient with severe mandibular prognathism. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 830–839. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.-H.; Shi, K.-K.; Cha, J.-Y.; Park, Y.-C.; Lee, K.-J. Nonsurgical miniscrew-assisted rapid maxillary expansion results in acceptable stability in young adults. Angle Orthod. 2016, 86, 713–720. [Google Scholar] [CrossRef] [Green Version]
- Brunetto, D.P.; Sant’Anna, E.F.; Machado, A.W.; Moon, W. Non-surgical treatment of transverse deficiency in adults using microimplant-assisted rapid palatal expansion (MARPE). Den. Press J. Orthod. 2017, 22, 110–125. [Google Scholar] [CrossRef] [Green Version]
- Pulver, R.J.; Campbell, P.M.; Opperman, L.A.; Buschang, P.H. Miniscrew-assisted slow expansion of mature rabbit sutures. Am. J. Orthod. Dentofac. Orthop. 2016, 150, 303–312. [Google Scholar] [CrossRef]
- Tsai, C.; Yang, T.-K.; Hsieh, H.-Y.; Yang, L.-Y. Comparison of the effects of micro-osteoperforation and corticision on the rate of orthodontic tooth movement in rats. Angle Orthod. 2015, 86, 558–564. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, S.S.; Braga, L.F.S.; Fujii, D.N.; Moon, W.; Suzuki, H. Corticopuncture Facilitated Microimplant-Assisted Rapid Palatal Expansion. Case Rep. Dent. 2018, 2018, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Hassan, A.H.; Al-Fraidi, A.A.; Al-Saeed, S.H. Corticotomy-assisted orthodontic treatment: Review. Open Den. J. 2010, 4, 159–164. [Google Scholar] [CrossRef] [Green Version]
- Dibart, S.; Surmenian, S.; Sebaoun, J.D.; Montesani, L. Rapid treatment of class II malocclusion with piezocision: Two case reports. Int. J. Periodontics Restor. Den. 2010, 30, 487–493. [Google Scholar]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Anterior Nasal Spine (ANS) Opening after Treatment | Posterior Nasal Spine (PNS) Opening after Treatment | |
|---|---|---|
| Number of values | 20 | 20 |
| Minimum | 2.970 | 2.670 |
| 25% Percentile | 3.250 | 2.780 |
| Median | 3.900 | 2.995 |
| 75% Percentile | 4.165 | 3.385 |
| Maximum | 4.540 | 4.110 |
| Mean | 3.766 | 3.125 |
| SD | 0.4956 | 0.4070 |
| Standard error of mean (SEM) | 0.1108 | 0.09102 |
| Lower 95% CI of mean | 3.534 | 2.934 |
| Upper 95% CI of mean | 3.998 | 3.316 |
| Table Analyzed | Data 2 |
|---|---|
| Column B | Posterior nasal spine (PNS) opening after treatment |
| vs. | vs. |
| Column A | Anterior nasal spine (ANS) opening after treatment |
| Paired t-test | |
| p-value | 0.0008 |
| p-value summary | |
| Significantly different? (p < 0.05) | Yes |
| One- or two-tailed p-value? | Two-tailed |
| t, df | t = 3.964 df = 19 |
| Number of pairs | 20 |
| How big is the difference? | |
| Mean of differences | −0.6410 |
| SD of differences | 0.7232 |
| SEM of differences | 0.1617 |
| 95% confidence interval | −0.9795 to −0.3025 |
| R2 | 0.4526 |
| How effective was the pairing? | |
| Correlation coefficient (r) | −0.2770 |
| p-value (one tailed) | 0.1185 |
| p-value summary | Ns |
| Significant correlation? (p > 0.05) | Yes |
| Parameter | Interincisal Opening at the CEJ Level/Millimeter |
|---|---|
| Minimum | 3.360 |
| 25% percentile | 3.783 |
| Median | 4.210 |
| 75% percentile | 4.365 |
| Maximum | 4.770 |
| Mean | 4.103 |
| SD | 0.3881 |
| SEM | 0.08679 |
| Lower 95% CI of mean | 3.921 |
| Upper 95% CI of mean | 4.284 |
| D’Agnostino & Pearson Omnibus Normality Test | 1st Molar Tilt after Treatment | 1st Molar Tilt before Treatment |
|---|---|---|
| Number of vales | 40 | 40 |
| Minimum | 85.60 | 84.00 |
| 25% Percentile | 87.60 | 85.23 |
| Median | 88.00 | 85.65 |
| 75% Percentile | 88.65 | 86.70 |
| Maximum | 89.30 | 87.90 |
| Mean | 87.88 | 85.87 |
| Std. Deviation | 1.001 | 1.057 |
| Std. Error of Mean | 0.2238 | 0.2363 |
| Lower 95 % CI of mean | 87.41 | 85.38 |
| Upper 95 % CI of mean | 88.34 | 86.36 |
| Table Analyzed | Data 1 |
|---|---|
| Column B | 1st Molar tilt before treatment |
| Vs. | Vs. |
| Column A | 1st Molat tilt after treatment |
| Paired t test | |
| p value | < 0.0001 |
| p value summary | |
| Significantly different? (p < 0.05) | yes |
| One- or two-tailed P value | Two-tailed |
| t, df | t = 12.33 df = 19 |
| Number of pairs | 40 |
| How big is the difference | −2.005 |
| SD of differences | 0.7273 |
| SEM of differences | 0.1626 |
| 95% confidence interval | −2.345 to −1.665 |
| R square | 0.8889 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bud, E.-S.; Păcurar, M.; Vlasa, A.; Lazăr, A.P.; Lazăr, L.; Vaida, P.; Bud, A. Retrospective Case Series Regarding the Advantages of Cortico-Puncture (CP) Therapy in Association with Micro-Implant Assisted Rapid Palatal Expander (MARPE). Appl. Sci. 2021, 11, 1306. https://0-doi-org.brum.beds.ac.uk/10.3390/app11031306
Bud E-S, Păcurar M, Vlasa A, Lazăr AP, Lazăr L, Vaida P, Bud A. Retrospective Case Series Regarding the Advantages of Cortico-Puncture (CP) Therapy in Association with Micro-Implant Assisted Rapid Palatal Expander (MARPE). Applied Sciences. 2021; 11(3):1306. https://0-doi-org.brum.beds.ac.uk/10.3390/app11031306
Chicago/Turabian StyleBud, Eugen-Silviu, Mariana Păcurar, Alexandru Vlasa, Ana Petra Lazăr, Luminița Lazăr, Petru Vaida, and Anamaria Bud. 2021. "Retrospective Case Series Regarding the Advantages of Cortico-Puncture (CP) Therapy in Association with Micro-Implant Assisted Rapid Palatal Expander (MARPE)" Applied Sciences 11, no. 3: 1306. https://0-doi-org.brum.beds.ac.uk/10.3390/app11031306